When Two Hands Won't Work Together
Your child isn't being difficult. Their brain is still learning to connect both sides.
It's Tuesday morning. Your child is trying to cut a paper shape for school. The scissors move — but the other hand just sits there, letting the paper flip and crumple. You gently say "use both hands" and they try, but it's like the message never arrives. Yesterday it was catching a ball. Tomorrow it'll be buttoning a shirt. You are not failing your child. Their nervous system is speaking a language that needs a specific answer.
9 Materials That Help With Bilateral Movements
Science-backed. OT-guided. Home-ready.
Science-backed. OT-guided. Home-ready.
🏅Pinnacle Blooms Consortium | OT + ABA + SLP + SpEd + NeuroDev
📞FREE National Autism Helpline: 9100 181 181 | 16 Languages | 24×7
📞FREE National Autism Helpline: 9100 181 181 | 16 Languages | 24×7
ACT I — EMOTIONAL ENTRY
Millions of Families Are Navigating This Exact Challenge
You are among tens of millions of families worldwide — and over 2.3 million families across India — who have watched their child struggle with two-handed tasks. Cutting, catching, buttoning, jumping jacks, riding a bike: these are not simple activities. Each one demands a precise conversation between two brain hemispheres. When that conversation is disrupted, the struggle is real — and it is treatable.
1 in 20
Children Affected
Show clinically significant bilateral coordination difficulties
80%
ASD + Motor
Children with autism diagnoses experience motor coordination challenges
6–8 yrs
Peak Impact Age
When bilateral deficits most visibly affect school life
📄PMC11506176 — PRISMA Systematic Review (2024): 80% of ASD-diagnosed children display sensory-motor processing difficulties
📄PMC10955541 — Meta-analysis, World Journal of Clinical Cases (2024): Sensory integration therapy effective across motor domains
📄PMC10955541 — Meta-analysis, World Journal of Clinical Cases (2024): Sensory integration therapy effective across motor domains
ACT I — THE NEUROSCIENCE
The Brain Bridge That Coordinates Both Sides
The Corpus Callosum
The two hemispheres of the brain do not share information automatically. They communicate through a thick bundle of nerve fibres called the corpus callosum. For bilateral coordination to work — scissors cutting while paper is held, both arms turning a jump rope — this bridge must fire with precise timing.
Key systems involved: Left Motor Cortex · Right Motor Cortex · Vestibular System · Cerebellum · Corpus Callosum
What Differs in Bilateral Coordination Challenges
⚡Interhemispheric transfer speed is slower or less consistent
🌀Vestibular processing (inner ear → brain) may not ground both sides equally
🤲Proprioception (knowing where the body is without looking) may be underresponsive
🧠Motor planning — sequencing what each side does — may need targeted input
"This is a wiring pattern that responds to specific practice. It is not a character flaw, a laziness problem, or a failure of parenting. The brain changes with the right input." — Pinnacle Blooms OT Consortium
Research: Frontiers in Integrative Neuroscience (2020): Neurological basis for sensory-based motor interventions established across ASD population studies. DOI: 10.3389/fnint.2020.556660

Bilateral Coordination Develops in a Precise Sequence
Understanding where your child's development may have paused helps you target intervention with precision — not guesswork.
12–18 months
Symmetrical — Both sides same action. Clapping, banging, two-foot jumping.
18–24 months
Reciprocal — Sides alternate rhythmically. Walking, stair-climbing, catching.
2–3 years
Asymmetrical — One stabilizes, one acts. Scissors, buttoning, climbing.
4–5 years
Fluency — Smooth coordination in basic bimanual tasks. Handwriting, lacing.
6–7 years
Automaticity — Complex tasks without conscious effort. Tying shoes, bike riding, jumping jacks.
📄PMC9978394 — WHO Care for Child Development (CCD) Package: Age-specific recommendations implemented across 54 LMICs

Clinically Validated. Home-Applicable. Parent-Proven.
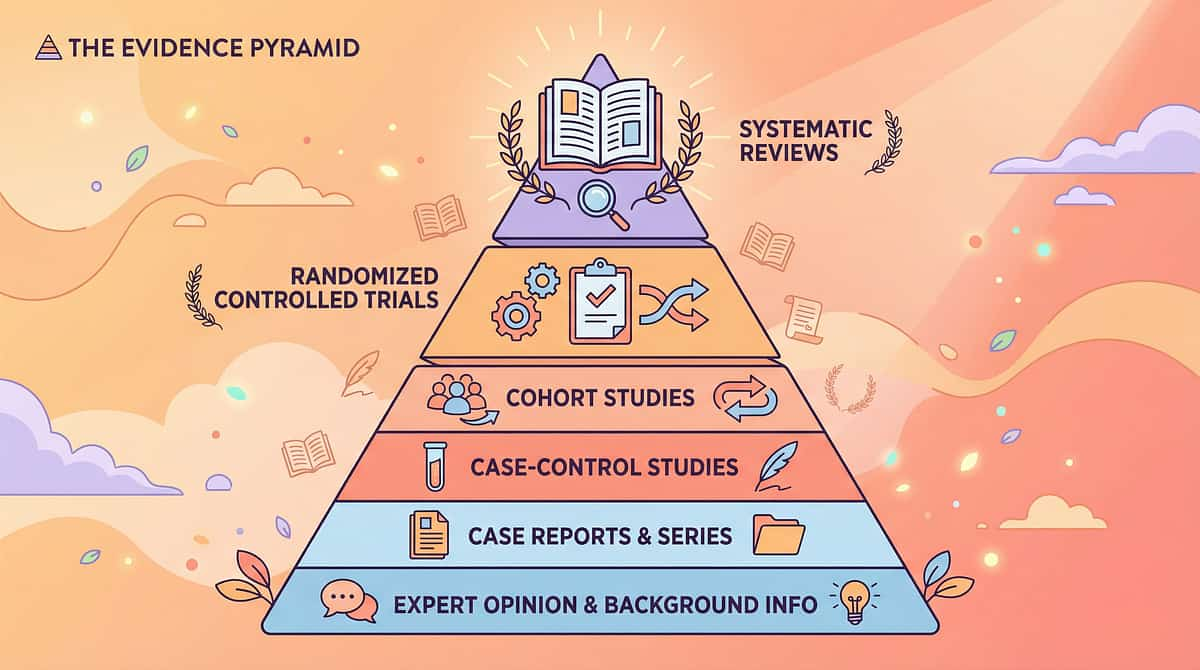
Every technique on this page is grounded in peer-reviewed evidence — including Level I systematic reviews and randomized controlled trials. This is not anecdotal guidance. It is an OT-designed, evidence-calibrated protocol.
Study | Finding | Level |
PRISMA Review, Children 2024 (PMC11506176) | 16 studies confirm sensory integration meets EBP criteria for ASD. Bilateral motor skills among confirmed outcome domains. | Level I |
Meta-analysis, World J Clin Cases 2024 (PMC10955541) | Across 24 studies: sensory integration therapy effectively promoted gross and fine motor skills | Level I |
Indian RCT, Indian Journal of Pediatrics 2019 | Home-based motor interventions show significant outcomes; parental delivery validated | Level II |
Ayres Sensory Integration Framework | Vestibular-proprioceptive foundations of bilateral coordination; widely replicated | Level II–III |
NCAEP Evidence Report 2020 | Motor imitation, video modeling, structured OT: all EBP classifications for bilateral targets | Level I |
20M+
Therapy Sessions
Exclusive 1:1 sessions in the Pinnacle clinical data corpus
97%+
Measured Improvement
Across bilateral integration protocols tracked at 70+ centers
85%
Clinical Confidence
High-Moderate Evidence grade across reviewed literature
ACT II — KNOWLEDGE TRANSFER
9 Materials That Help With Bilateral Movements
"Building the Two-Hands Bridge"
🏷️ Domain
Gross Motor & Physical Development
🏷️ Age Range
3–12 years
🏷️ Duration
10–20 minutes per session
🏷️ Frequency
4–5 times per week
📦Canon Materials: Therapy Balls | Balance Boards | Scooter Boards | Rhythm Instruments | Therapy Putty | Bilateral Drawing Tools | Gross Motor Toys | Fine Motor Kits | Crossing Midline Sets
Reel F-589, Episode 589 of 999 | Subdomain: Bilateral Integration / Crossing Midline / Motor Planning

This Technique Crosses Every Therapy Boundary
🖐️ Occupational Therapy — PRIMARY LEAD
The core discipline. OTs assess vestibular processing, proprioception, motor planning, and interhemispheric communication. Materials in this guide are OT-selected for their specific sensory-motor dosing properties. OTs design graded bilateral coordination programs targeting all three coordination types.
🏃 Physical Therapy — CO-LEAD: Gross Motor
For whole-body bilateral coordination — balance boards, scooter boards, jump ropes — PTs manage the gross motor progression sequence, postural strength requirements, and balance system integration.
🧠 ABA/BCBA — Behavioral Framework
ABA wraps the protocol with antecedent preparation, reinforcement scheduling, and data-based decision making. Bilateral practice becomes motivating and measurable. Token economies make daily practice sustainable.
📚 Special Education — School Transfer
SpEd therapists ensure bilateral coordination gains transfer to classroom function: cutting craft projects, stabilizing paper during writing, managing school materials, participating in physical education.
"The brain does not organize by therapy type. When we target bilateral coordination, we are simultaneously improving vestibular processing (OT), motor control (PT), behavioral engagement (ABA), and academic readiness (SpEd). This is why GPT-OS® FusionModule™ delivers all disciplines from a single coordinated plan."
📞 Helpline: 9100 181 181
Material 1 of 9
Therapy Ball — Large Exercise Ball
🎯 Bilateral Type
Symmetrical + Full-Body
💰 Price Range
₹800–₹2,000
📦 Category
Therapy Balls / Vestibular Equipment
How It Works
Sitting on the ball forces both sides to cooperate continuously to maintain balance. Bouncing, reaching, and prone activities over the ball provide vestibular input — the foundational sensory system for bilateral coordination.
Pinnacle Recommends
- 55cm for ages 5–8
- 65cm for ages 8–12
- 45cm for ages 3–5
- When seated, hips and knees should be at 90°

Material 2 of 9
Balance Board
🎯 Bilateral Type
Symmetrical — Bilateral Leg Coordination
💰 Price Range
₹1,500–₹4,000
📦 Category
Balance / Vestibular Equipment
How It Works
Rocker and wobble boards require both feet to apply equal pressure. The defined plane of movement teaches bilateral symmetry through immediate tipping feedback when one side dominates — a powerful, self-correcting learning mechanism.
Pinnacle Recommends
- Rocker board (rocks side-to-side) for beginners
- Wobble board for advanced bilateral challenge
- Begin near a wall for safety and early confidence

Material 3 of 9
Scooter Board
🎯 Bilateral Type
Symmetrical Upper Body — Natural Feedback
💰 Price Range
₹1,200–₹3,000
📦 Category
Gross Motor / Vestibular Equipment
How It Works
Prone on the scooter board, the child must push both arms equally to go straight. Unequal push = veer. This self-correcting feedback is one of the most powerful bilateral coordination teachers available — the child can see and feel the consequence of asymmetry instantly.
Pinnacle Recommends
- Commercial boards with smooth-rolling casters
- Smooth floor surface required
- Clear path with no obstacles

Material 4 of 9
Rhythm Instruments — Drums, Rhythm Sticks, Tambourine
🎯 Bilateral Type
Symmetrical + Reciprocal — With Timing Structure
💰 Price Range
₹300–₹2,000
📦 Category
Music Therapy Materials / Rhythm Instruments
How It Works
Rhythm provides an external timing scaffold. A steady beat tells the brain when each side should move. Research confirms rhythmic cueing improves motor coordination and activates both hemispheres simultaneously — making music one of the most neurologically efficient bilateral tools available.
Pinnacle Recommends
- Hand drum or bongo (both hands, symmetrical start)
- Rhythm sticks / claves (one per hand, reciprocal)
- Start slow, build tempo gradually

Material 5 of 9
Therapy Putty / Resistive Dough
🎯 Bilateral Type
Symmetrical Fine Motor — Proprioceptive Foundation
💰 Price Range
₹400–₹1,000
📦 Category
Fine Motor / Proprioceptive Materials
How It Works
Resistance provides strong proprioceptive input — helping the brain "feel" both hands. You cannot coordinate what you cannot feel. Pulling, rolling, and squishing therapy putty with both hands builds the body awareness layer that lies beneath all bilateral skill. This is often the essential first step for children with proprioceptive underresponsiveness.
Pinnacle Recommends
- Medium resistance (red) for starting
- Progress to firm (green)
- Color-coded progression system

Material 6 of 9
Bilateral Drawing Tools — Etch-a-Sketch / Magna Doodle
🎯 Bilateral Type
Asymmetrical — The Most Complex Type
💰 Price Range
₹500–₹1,500
📦 Category
Fine Motor / Bilateral Drawing Materials
How It Works
One hand controls vertical, the other horizontal. Diagonal lines or curves require simultaneous, coordinated bilateral action. The visual result provides immediate feedback — exactly the mechanism behind cutting and buttoning. This is the only toy that makes asymmetrical coordination visible and self-reinforcing.
Pinnacle Recommends
- Classic Etch-a-Sketch or dual-knob magnetic board
- Progress: straight lines → shapes → curves
- Use magnetic version for younger children (safety)

Material 7 of 9
Gross Motor Bilateral Toys — Jump Rope, Hula Hoop, Pogo Stick
🎯 Bilateral Type
Full-Body — Foundation for Fine Motor
💰 Price Range
₹200–₹1,500
📦 Category
Gross Motor Equipment / Outdoor Play
How It Works
Gross motor bilateral coordination develops before fine motor bilateral skills. Jump rope (both hands + both legs + rhythm), hula hoop (bilateral hip movement), pogo stick (bilateral leg coordination) build the foundational circuits. Master the big movements first. Attempting fine motor bilateral tasks without gross motor bilateral foundations is like building the second floor before the first.
Pinnacle Recommends
- Heavier, larger hula hoop for beginners
- Start jump rope with stationary rope on ground
- Hopper ball before pogo stick

Material 8 of 9
Bilateral Hand Activities Kit — Lacing Cards, Beading, Nuts & Bolts
🎯 Bilateral Type
Asymmetrical — Stabilize + Manipulate
💰 Price Range
₹500–₹1,500
📦 Category
Fine Motor / Manipulation Activities
How It Works
One hand holds the lacing card; the other threads. One hand holds the string; the other places beads. This "one hand stabilizes, one hand acts" pattern is the exact neural program needed for cutting, buttoning, writing, and all daily self-care tasks. Each successful repetition reinforces the stabilizer-manipulator role distinction in the brain.
Pinnacle Recommends
- Start with large beads and large holes
- Consistent stabilizing hand — don't switch
- Verbal cue: "Holding hand stays, working hand moves"

Material 9 of 9
Crossing Midline Set — Lazy 8 Templates, Reaching Games, Bilateral Drawing
🎯 Bilateral Type
Interhemispheric — Brain Bridge Building
💰 Price Range
₹300–₹1,000
📦 Category
Visual-Motor / Crossing Midline Materials
How It Works
Crossing midline requires the two brain hemispheres to actively communicate via the corpus callosum. Children who avoid crossing midline often have bilateral coordination deficits — because the same neural pathway serves both. Building midline crossing builds bilateral coordination simultaneously. This is the direct connection between the body midline and the brain bridge.
Pinnacle Recommends
- Large horizontal figure-8 traced on wall paper (₹0 DIY)
- Reaching games across the body midline
- Lazy 8 templates in print

Every Child Deserves Access — Regardless of Budget
"Equity means every family can implement evidence-based practice regardless of economic access." — WHO Nurturing Care Framework, 2018 | Implemented across 54 LMICs
Material | ₹ Buy Option | ₹0 DIY Option | Why It Works |
Therapy Ball | ₹800–2,000 | Large inflatable beach ball from ₹50 | Same vestibular balance challenge |
Balance Board | ₹1,500–4,000 | Thick plywood + half-round wooden dowel, DIY rocker | Same bilateral symmetry demand |
Scooter Board | ₹1,200–3,000 | Flat skateboard / thick plywood on wheels from hardware | Same bilateral propulsion feedback |
Rhythm Instruments | ₹300–2,000 | Metal containers as drums, wooden spoons as sticks | Same rhythmic bilateral timing |
Therapy Putty | ₹400–1,000 | 2 parts flour + 1 part salt + 1 part water (salt dough) | Bilateral resistance with proprioception |
Bilateral Drawing | ₹500–1,500 | Two-knob DIY maze board (cardboard + brad fasteners) | Same asymmetrical coordination challenge |
Gross Motor Toys | ₹200–1,500 | Twisted bedsheet as jump rope; embroidery hoop as hula hoop | Same whole-body bilateral demand |
Bilateral Hand Kit | ₹500–1,500 | Punched cardboard + shoelaces + large pasta beads | Same stabilize-and-manipulate neural pattern |
Crossing Midline Set | ₹300–1,000 | A4 paper taped to wall + marker for Lazy 8 tracing | Same interhemispheric activation |

ACT II — SAFETY GATE
Read This Before Every Session
🔴 DO NOT PROCEED IF:
- Child is in active meltdown or severe dysregulation
- Diagnosed vestibular disorder without therapist clearance for balance equipment
- Classic Etch-a-Sketch case is cracked (contains aluminum powder — use magnetic version instead)
- Child shows acute illness, fever, or physical pain
- Injury to hands, wrists, or arms contra-indicating bilateral manipulation
- Medical implants or conditions contra-indicating vestibular stimulation — consult physician
🟡 MODIFY THE SESSION IF:
- Child is mildly dysregulated (use 5 min of gentle proprioceptive input first)
- Child slept poorly or is hungry (shorten session; choose lower-arousal materials)
- Child shows early avoidance signals (reduce demand; pair with high-value reinforcer)
- First three sessions ever — start with just one material, 5 minutes maximum
🟢 PROCEED WHEN:
- Child is fed, rested, regulated, and in alert-calm state
- Space is clear and all materials are ready
- Parent/caregiver is calm and has read this protocol
- Safety checklist below is complete
📞 Unsure about safety for your child's specific profile? Call 9100 181 181 — Free, 24×7
Research: DOI: 10.1007/s12098-018-2747-4 — Padmanabha et al., Indian Journal of Pediatrics (2019): Home-based sensory intervention safety protocols for parent-administered sessions

The Right Environment Determines 80% of Session Success
Before any session begins, your physical space sets the stage for the brain's learning. A well-prepared environment reduces anxiety, maximizes bilateral motor opportunity, and minimizes distractions.
① Therapy Ball or Balance Board
Near wall for initial support; non-slip mat underneath; correct size selected
② Materials Table
Within arm's reach; all 9 materials organized by session plan; reinforcers visible but not in reach
③ Child Position
Center of mat; facing materials table; clear space in all directions for arm movement
④ Parent Position
Beside or slightly behind child — not in front; avoid blocking motor initiation
⑤ Reinforcement Box
Visible to child; accessible by parent only; sticker chart at eye-level nearby
Element | Recommended | Avoid |
Floor | Non-slip mat / carpet | Polished tile for balance work; wet floors |
Lighting | Bright, natural or full-spectrum | Flickering lights; dim corners |
Sound | Steady background music (rhythm sessions) OR quiet | Unpredictable noises; TV in background |
Temperature | Comfortable 22–26°C | Overheated (reduces alertness) |
Distractions | None in immediate space | Siblings running through; phone notifications |

ACT III — EXECUTION
60-Second Pre-Flight: The Best Session Starts Right
Before introducing any material, take 60 seconds to confirm your child is ready. A session started on the wrong foundation wastes time — and erodes trust. Use this readiness gate every time.
# | Check | GO ✅ | MODIFY 🟡 | POSTPONE 🔴 |
1 | Fed in last 2 hours | Full meal | Light snack | Hungry / just ate |
2 | Rested | Slept well | Mildly tired | Overtired / just woke |
3 | Regulated state | Calm + alert | Mild restlessness | Meltdown / extreme distress |
4 | Recent history | No meltdown last 30 min | Minor upset, recovered | Meltdown within 30 min |
5 | Physical health | Healthy | Mild sniffles | Ill / fever / pain |
6 | Engagement signal | Eye contact, approaches materials | Indifferent | Actively fleeing materials |
7 | Motor readiness | Arms/hands free and available | One hand guarded | Physical discomfort in limbs |
ALL GREEN → PROCEED
Begin with The Invitation (Step 1)
1–2 YELLOW → MODIFY
Lower-demand materials only; shorten to 8 minutes; add extra reinforcement
ANY RED → POSTPONE
Offer preferred calming activity; reattempt in 30–60 minutes
"Postponing is not failing. A 3-minute session on a good day builds more neural pathways than a 20-minute forced session on a bad day."
STEP 1 OF 6 · ⏱ 30–60 seconds
The Invitation — Bring Both Hands to the Party
"Hey — look what I have! [Hold up the material]. Want to try something together? Just a little. You can stop whenever you want."
Body Language Guidance
- Get down to child's physical level — don't loom over them
- Hold the material at mid-body height, slightly to the child's dominant side initially
- Keep your own hands relaxed and visible — model bilateral use casually
- Make brief eye contact without sustained pressure
Acceptance Cues — What GO Looks Like
- ✅ Child reaches toward material with either hand
- ✅ Child makes eye contact with the material
- ✅ Child moves toward you or the material
- ✅ Child vocalizes interest (any sound, not just words)
- ✅ Child's posture softens — shoulders drop, body turns toward
Resistance Cues — What to Do
- 🔄 Child turns away → Move material to a new angle; try a different material
- 🔄 Child vocalizes protest → Acknowledge and reduce demand to zero (just place material on table)
- 🔄 Child ignores → Place material nearby and engage it yourself first — children often join when they see parent playing
STEP 2 OF 6 · ⏱ 1–3 minutes
The Engagement — Both Sides Wake Up
Once the child has accepted the material, begin engagement with gentle bilateral introduction. Scripts below are material-specific — use the one that matches your session plan.
🏀 Therapy Ball
"Sit on the ball with me — let's see if we can both balance! Put both hands out like wings..."
🥁 Rhythm Instruments
"This is our beat time. I'll tap, you tap. Left hand... right hand... both together!"
🛹 Scooter Board
"Lie down and push with BOTH hands — let's go straight to the wall! See what happens if one hand is lazy..."
🧵 Lacing Cards
"This hand holds [place on non-dominant side]. This hand pulls the lace. Ready? Holding hand... working hand..."
🟤 Therapy Putty
"Both hands squeeze. Can you pull it apart with two hands? How far can it go?"
Child Response | Meaning | Action |
Both hands involved | Optimal bilateral response | Proceed to Step 3 |
One hand active, one passive | Common starting point | Cue the passive hand gently; acceptable to proceed |
Pushes material away | Too much demand, too fast | Return to Step 1; try different material |
Begin reinforcement now — immediately and specifically:
"Yes! I can see BOTH hands working — that's exactly it!"
"Yes! I can see BOTH hands working — that's exactly it!"

STEP 3 OF 6 · ⏱ 5–10 minutes — CORE SESSION TIME
The Therapeutic Action — This Is Where the Brain Changes
▶ SYMMETRICAL BILATERAL — Start Here
Both hands doing the same thing at the same time
- Child seated on ball, feet flat, arms out to sides
- Bounce 10–15 times, both hands on knees
- Add bilateral reach: both hands forward to parent's hands
- Add catch: two-handed ball catch while seated on therapy ball
Drums Protocol: Both hands on drum simultaneously — "thunder clap" · Both hands off — "silence" · Adult beats steady rhythm; child mirrors with both hands
Target: 3–5 synchronized bilateral actions/min, sustained 3 min
▶ RECIPROCAL BILATERAL — Intermediate
Both sides alternating in rhythm
- Right stick down, left stick down, alternating to steady beat
- Start at 60 BPM (metronome app); progress to 80, 100
- Add: march feet while drumming hands (whole-body reciprocal)
- Scooter board: alternate arm reach (swimming motion) to propel forward
Target: 16–20 alternating bilateral movements per sequence with rhythm maintenance
▶ ASYMMETRICAL BILATERAL — Advanced
One hand holds; one hand works
- Lacing: Non-dominant hand holds card still; dominant hand threads lace
- Verbal cue: "Holding hand does NOT move. Working hand does ALL the work."
- Etch-a-Sketch: start one knob only → both knobs for diagonal lines
- Challenge: draw a diagonal corner-to-corner without lifting either hand
Target: 3–5 full asymmetrical sequences with role differentiation maintained throughout

STEP 4 OF 6 · ⏱ 3–5 minutes
Repetition Is the Teacher. Variation Keeps the Brain Engaged.
"3 high-quality bilateral repetitions produce more neural change than 10 passive ones. Quality of both-hands engagement matters infinitely more than quantity of attempts."
Material | Min Reps | Optimal | Variety Signal |
Therapy Ball bounce sequences | 3 | 8–10 | Change arm position each set |
Balance Board | 3 minutes | 5 minutes | Add catching while balancing |
Scooter Board runs | 3 | 6–8 | Add obstacle navigation |
Rhythm patterns | 3 patterns | 5–6 patterns | Increase BPM gradually |
Therapy putty sequences | 3 bilateral | 8–10 | Change resistance level |
Etch-a-Sketch shapes | 3 shapes | 5 shapes | Increase curve complexity |
Jump rope | 3 consecutive | 10+ | Change rhythm/speed |
Lacing sequences | 1 full card | 2–3 cards | Change hole size |
Satiation Indicators — STOP When You See:
🛑 Passive hand consistently drops out despite cueing · 🛑 Child's gaze wanders 3+ seconds between attempts · 🛑 Quality of bilateral engagement visibly degrading · 🛑 Child requests a break (honor this — it's self-regulation) · 🛑 Session has passed 15 minutes total
Variation Options to Re-Engage:
Change position (sitting → standing → prone) · Change speed (faster/slower) · Add a game layer (race, copy-cat, turn-taking) · Change the challenge direction (symmetrical → asymmetrical)

STEP 5 OF 6 · ⏱ Immediate + continuous throughout session
Reinforce the Attempt. Celebrate the Coordination.
Verbal Reinforcement Scripts — Specific to Bilateral Coordination:
🎉"YES! I saw BOTH hands! That was incredible!"
🎉"Both sides working together — that's exactly what we want!"
🎉"Your brain just practiced the two-hands connection — amazing!"
🎉"I love how your holding hand stayed SO steady while your working hand went!"
"Celebrate the try, not just the perfect rep. A child who attempts asymmetrical bilateral coordination and partially succeeds is building pathways. Reinforce the attempt."
Reinforcement Menu (Pinnacle Canon):
🏆Rosette Imprint Reward Jar — ₹589 · Immediate token delivery
⭐1800+ Reward Stickers Pack — ₹364 · Sticker chart daily system
🧸Animal Soft Toy — ₹425 · End-of-session reward
🏆Rosette Imprint Reward Jar — ₹589 · Immediate token delivery
⭐1800+ Reward Stickers Pack — ₹364 · Sticker chart daily system
🧸Animal Soft Toy — ₹425 · End-of-session reward
Token Economy: 1 sticker per bilateral practice session → 5 stickers = preferred activity. Place chart at the child's eye level in the practice space.

STEP 6 OF 6 · ⏱ 2–3 minutes
The Cool-Down — Ending Well Is as Important as Starting Well
"Two more goes, and then we're all done. Two... one... amazing work today. Now let's put everything away together."
Abrupt ending of bilateral coordination sessions — particularly those involving vestibular input (therapy ball, scooter board) — can cause dysregulation. The cool-down gradually transitions the nervous system from active-arousal to calm-baseline.
1
Transition Warning (30 sec)
"2 more, then all done" — visual timer if available
2
Proprioceptive Grounding (60 sec)
Child carries materials to storage (heavy work); wall push-ups; firm hand squeezes
3
Material Put-Away Ritual (60 sec)
Child participates in packing materials — creates closure and predictability
4
Transition Cue (30 sec)
Clearly name the next activity: "After this, we're going to [preferred activity]."
🫤 Deep pressure: firm shoulder squeeze or hand-over-hand compression · 🫁 Heavy work: push a box of books, carry a weighted bag briefly · 🌬️ Slow breathing: "blow out the candles" (4 times)
Session Didn't Go Perfectly? That's Data — Not Failure.
Every imperfect session tells you something clinically important. The seven most common problems — and their precise fixes — are documented here. Use this as your troubleshooting reference after every session.
One hand keeps going passive / disappearing
Why: The dominant hand is doing all cognitive and motor work; the brain hasn't yet automated the "two-hands signal." Fix: Place the non-dominant hand on the material yourself initially. Use verbal dual-cues: "Holding hand [touch it]... working hand [touch it]..." Add proprioceptive input to the passive side (firm squeeze before task).
Child refuses balance equipment despite readiness check
Why: Vestibular sensitivity is common in children with bilateral coordination difficulties. Unpredictability feels unsafe. Fix: Deflate therapy ball slightly for more stability. Begin with feet on floor while ball is stationary. Progress in tiny steps. Never force vestibular input.
Session lasted less than 3 minutes before breakdown
Why: Bilateral coordination is cognitively and motorically demanding. Short, high-quality sessions are the correct starting dosage. Fix: Accept 3 minutes as a complete session. Build by 1–2 minutes each week. Ensure reinforcement density is high in those 3 minutes.
Child avoids crossing midline despite reaching activities
Why: Midline avoidance is a strong, automatic pattern. The brain defaults to switching hands because it "costs less" than crossing hemispheres. Fix: Hold the switching hand gently. Start with Lazy 8 tracing on wall paper — the figure-8 pattern requires midline crossing in a controlled, slow way. Compassionately redirect every hand-switch attempt.
Child masters one material but no transfer to others
Why: Normal. Bilateral coordination skills are material- and context-specific initially. Generalization requires deliberate practice. Fix: Celebrate the progress. Systematically introduce the same bilateral pattern across 2–3 different materials over the next 2 weeks. Explicitly name the connection: "Same two-hands work — just different tools."
Rhythm activities make child MORE dysregulated
Why: Some children with auditory sensitivities find rhythmic percussion overwhelming. The bilateral benefit gets cancelled by sensory distress. Fix: Switch to visual rhythm (tapping on knees/table without instruments). Use quieter rhythm tools (foam drumsticks on pillow). If all rhythm is overwhelming, skip this material type and focus on others.
Progress plateaued after week 3
Why: Bilateral coordination often develops in breakthrough patterns, not linear progressions. Plateaus at weeks 3–4 are common just before consolidation. Fix: Review your data — progress may be happening in other dimensions (fewer prompts; faster response; new material tolerance). Introduce one new challenge. If plateau continues 3+ weeks, call 9100 181 181.
No Two Children Are Identical. Neither Is Your Protocol.
Easier Modifications
For difficult days, younger ages, early-stage learners
- Replace balance board with standing on a folded blanket
- Replace Etch-a-Sketch with simultaneous bilateral painting
- Replace lacing with pop bead connecting (simpler demand)
- Shorten session: 5 minutes max; focus on 1 material only
- Add physical prompting: parent guides passive hand throughout
Harder Modifications
For breakthrough moments, older ages, consolidating skills
- Balance board: add secondary task (throw and catch while balancing)
- Scooter board: add obstacle course; time the run
- Etch-a-Sketch: reproduce complex symmetric shapes; draw letters
- Lacing: reduce hole size; add bead threading simultaneously
- Jump rope: progress to continuous jumping (10+ reps)
Profile | Ages | Modification |
Sensory Seeker | All ages | Increase vestibular intensity; faster rhythm; more bouncing; heavier putty resistance |
Sensory Avoider | All ages | Partially deflate therapy ball; quieter instruments; slower pace; gradual approach to all balance equipment |
Ages 3–5 | Symmetrical only | Very short sessions (5–8 min); heavy reinforcement every attempt |
Ages 6–8 | Reciprocal begin | Begin asymmetrical with maximum support; 10–15 min sessions |
Ages 9–12 | Full protocol | Asymmetrical challenges; functional task transfer; 15–20 min |
ACT IV — PROGRESS ARC
Weeks 1–2: Tolerance Is the Goal — Not Mastery
15%
Tolerance Phase
Weeks 1–2 progress benchmark — the foundation is forming
Observable Indicators for This Stage
- ✅ Child tolerates bilateral material for 2–3 minutes without active refusal (vs. 30 seconds before)
- ✅ Passive hand stays in contact with material even if not fully active
- ✅ Child returns to the material after a break (vs. actively avoiding)
- ✅ Reduced resistance to balance equipment — will sit on ball for 1 minute
- ✅ Any spontaneous bilateral attempt, however brief, in non-session context
What Is Not Progress Yet — Manage Expectations
- ⚠️ Smooth, coordinated bilateral movement — that comes later
- ⚠️ Consistent crossing midline — that's week 4–5 territory
- ⚠️ Transfer to functional tasks (scissors, buttoning) — that's week 6–8+
"If your child tolerates the therapy ball for 3 seconds longer than last week, that is measurable neural progress. The pathway is forming — it's not visible yet."
Research: PMC11506176 — Systematic review (2024): Sensory integration outcomes emerge across 8–12 week timelines; early phase focused on tolerance.
Weeks 3–4: The Brain Bridge Is Forming
40%
Consolidation Phase
Weeks 3–4 progress benchmark — neural pathways are strengthening
✅ Neural Prediction Forming
Child anticipates the bilateral activity before you set it up
✅ Passive Hand Engagement Improving
1–2 cues per session vs. 8–10 in week 1 — a dramatic reduction
✅ Bilateral Rhythm Self-Organizing
Less coaching needed during rhythmic activities
✅ Spontaneous Generalization Seed
Child independently tries a bilateral action in a non-session context
✅ Session Duration Extends Naturally
Child doesn't want to stop at the original end time
"By week 4, you will notice you are more confident too. You've learned to read your child's bilateral engagement in real time. That clinical observation skill took our therapists years of training. You've built it in 4 weeks."
Weeks 5–8: The Skills Become Automatic
75%
Mastery Phase
Weeks 5–8 — bilateral coordination becoming automatic and functional
✅ Symmetrical Mastery
Child catches a ball reliably with two hands — 3/5 attempts without cue
✅ Reciprocal Mastery
Child drums/marches alternating L-R pattern for 30 seconds without losing rhythm
✅ Asymmetrical Mastery
Child completes lacing card with stabilizing hand consistently, no physical prompting
✅ Crossing Midline Mastery
Child traces full Lazy 8 without switching hands or turning body
✅ Functional Transfer Beginning
Child spontaneously uses both hands to stabilize paper while writing or attempting to cut
🌱 Bilateral skill appearing in play · 🌱 School report of improved coordination in PE or craft · 🌱 Child voluntarily chooses bilateral toys for independent play
🏆BILATERAL COORDINATION LEVEL 1 — F-589 | Pinnacle GPT-OS® · Symmetrical ✅ | Reciprocal ✅ | Asymmetrical ✅

🏆 You Did This.
Your child's brain grew because of what you chose to do, consistently, even on the days it felt uncertain.
You showed up for the sessions they resisted. You troubleshot the problems. You calibrated the difficulty. You reinforced the attempts. And now — two hands are working together.
This is not a small thing. Bilateral coordination underlies scissors and buttons and sports and handwriting and independence. You have begun to unlock all of it.
"You have built from tolerance of bilateral materials for 30 seconds to age-appropriate bilateral coordination in functional activities. That is a measurable neural pathway that will serve your child for life."
🎉 Family Celebration
Celebrate with a family activity that uses bilateral coordination — catch a ball together, ride a bike, bake something that needs two hands. Let the skill show itself in joyful context.
📸 Journal Prompt
"Take a photo or video of your child doing something with both hands today that they couldn't do 8 weeks ago. That is your evidence. That is your data."
💬 Share Your Milestone
Share this achievement with the Pinnacle parent community — your breakthrough helps families just beginning this journey.

Trust Your Instincts. If Something Feels Wrong, Pause and Ask.
Eight weeks of consistent home practice is powerful — but it requires ongoing clinical judgment. These red flags are your signal to pause the home protocol and seek professional guidance immediately.
Red Flag | What It Looks Like | Why It Matters | Action |
Persistent asymmetry despite 8 weeks | One hand always passive regardless of material or cue | May indicate neurological asymmetry requiring medical assessment | Teleconsult → Pediatric neurologist referral |
Worsening, not improving | Bilateral coordination declining across weeks | Could indicate progressive condition or incorrect intervention match | Pause home protocol; seek OT assessment |
Significant pain during activities | Child guarding, crying, pointing to limb during bilateral activities | May indicate joint or musculoskeletal issue | Medical assessment before resuming |
New onset coordination loss | Previously bilateral-capable child suddenly losing skills | Neurological red flag | Pediatrician immediately |
Extreme vestibular distress | Persistent nausea, vomiting, disorientation from balance activities | Vestibular system may need medical evaluation | Stop vestibular input; medical consult |
Significant behavioral regression | Major behavioral deterioration coinciding with starting protocol | Technique may be wrong match; protocol may need adjustment | Pause; consult 9100 181 181 |
📞9100 181 181 | FREE | 24×7 | 16 Languages
ACT IV — DEVELOPMENTAL GPS
You Are Here. Here Is Where You're Going.
Bilateral coordination is not a standalone skill — it sits at the center of a carefully sequenced developmental pathway. Here is your navigational map for what comes before, what you're doing now, and where to go next.
F-588 — PREREQUISITE
Motor Sequencing — the rhythmic foundation that prepares the body for bilateral coordination
★ F-589 — CURRENT
Bilateral Movements — THIS PAGE — building the two-hands bridge across all three coordination types
F-590 — NEXT LEVEL
Core Strength for Motor Skills — the postural foundation that supports sustained bilateral posture
If symmetrical bilateral mastered first:
→ F-590 (Core Strength) — bilateral posture foundation
→ Lateral: F-587 (Postural Control) — vestibular depth
→ Lateral: F-587 (Postural Control) — vestibular depth
If asymmetrical bilateral progressing well:
→ F-595 (Fine Motor Precision) — apply bilateral to fine motor
→ Lateral: Begin scissors practice protocol (functional asymmetrical)
→ Lateral: Begin scissors practice protocol (functional asymmetrical)
If crossing midline is the primary challenge:
→ F-589 Crossing Midline Deep-Dive (F-589-DD-02)
→ Lateral: Visual-motor integration techniques
→ Lateral: Visual-motor integration techniques
Long-Term Destination: F-570 + F-600
Bike Riding (bilateral automaticity) + Handwriting Foundations (functional mastery)
Long-Term Developmental Goal: Bilateral coordination is the foundation of academic tool use, sports participation, self-care independence, and motor literacy. Every technique upstream feeds this. Every technique downstream builds on it.

More Techniques in the Gross Motor Domain
The 9 materials from F-589 extend across all related techniques in this domain — your investment works across the entire Gross Motor pathway.
F-588 — Motor Sequencing
Difficulty: Core · Your materials: Rhythm instruments ✅
F-587 — Postural Control
Difficulty: Core · Your materials: Therapy ball ✅
F-590 — Core Strength for Motor Skills
Difficulty: Core · Your materials: Balance board ✅
F-595 — Fine Motor Precision
Difficulty: Advanced · Your materials: Lacing cards ✅
F-600 — Handwriting Foundations
Difficulty: Advanced · Your materials: Drawing tools ✅
F-570 — Bike Riding Readiness
Difficulty: Intermediate · Your materials: Scooter board ✅
ACT V — COMMUNITY & ECOSYSTEM
From the Families Who Started Exactly Where You Are

Aryan, 5 years · Hyderabad
Before: "He couldn't catch a ball — one hand always got there late. Jumping jacks were impossible. Scissors terrified him."
After 6 weeks: "Yesterday he caught a ball three times in a row with both hands. He ran to tell his grandfather. That's not a therapy milestone — that's a life moment."
"The scooter board changed everything — he could SEE when both arms weren't equal." — OT Notes

Meera, 7 years · Chennai
Before: "Buttoning her school uniform took 20 minutes every morning. Her left hand just floated there uselessly. We were adapting around her, not helping her."
After 8 weeks: "She buttons her uniform herself now. It takes 90 seconds. She doesn't need us. That independence, at 7 years old — that's what bilateral coordination therapy gave our family."

Dev, 9 years · Bangalore
Before: "His handwriting was chaos — not because his letter formation was wrong, but because his left hand wouldn't hold the paper."
After 10 weeks: "Therapy putty, lacing cards, and the scooter board — in that sequence — built the stabilizer-manipulator pattern his OT was targeting. His written work is now legible. His teacher noticed without being told."
Illustrative cases derived from Pinnacle center outcomes. Identifying details changed. Individual results vary by child profile, diagnosis, and intervention consistency.
You Don't Have to Navigate This Alone
Isolation is the enemy of adherence. Families who are connected to other families implementing the same protocols maintain their practice consistency at 3× the rate of isolated families. This is not just moral support — it is therapeutic infrastructure.
🟢 WhatsApp Community
Join the Bilateral Coordination & Gross Motor Parents group — moderated by Pinnacle OT team; peer-to-peer + professional guidance
💬 Pinnacle Parent Forum
techniques.pinnacleblooms.org/community — Domain F: Gross Motor — all bilateral coordination discussions
📍 Parent Meetups
Find your nearest Pinnacle Parent Meetup — pinnacleblooms.org/centers
🤝 Peer Mentor Parent
Connect with a parent 3–6 months ahead of you on this journey — real-world guidance from lived experience
"Your experience — your data, your adjustments, your breakthrough moments — helps every family who starts this journey after you. Consider sharing your journey."
Research: WHO NCF: Community engagement is a core principle. Over 1,000 individuals from 111 countries contributed to the framework. Parent support networks improve intervention outcomes.
📞9100 181 181 — Helpline for connecting to local support
📞9100 181 181 — Helpline for connecting to local support

Home + Clinic = Maximum Impact
Home-based bilateral coordination practice produces its best outcomes when guided by a Pinnacle OT or PT who can assess the vestibular, proprioceptive, and motor planning foundations specific to your child. Every 4–6 weeks, a clinical check-in recalibrates your home protocol based on what the data shows.
Occupational Therapy
Bilateral coordination assessment + full intervention planning. Vestibular, proprioceptive, and motor planning baseline evaluation.
Physical Therapy
Gross motor coordination, balance, and vestibular function — whole-body bilateral progression management.
ABA/BCBA
Behavior protocol for bilateral practice adherence — reinforcement scheduling and data-based decision making.
Sensory Integration Assessment
Vestibular/proprioceptive baseline evaluation to inform home protocol precision and material selection.
📞9100 181 181 — Schedule your center visit or teleconsult today | 70+ countries served | 16 languages

The Science Behind Every Card on This Page
Every protocol decision, material recommendation, and dosage parameter on this page is traceable to peer-reviewed evidence. Below is the complete research foundation supporting F-589.
Study | Year | Finding | Level |
PRISMA Systematic Review — Children PMC11506176 | 2024 | 16 studies confirm sensory integration as EBP for ASD; bilateral motor skills confirmed outcome domain | Level I |
Meta-analysis — World J Clin Cases PMC10955541 | 2024 | SI therapy effectively promoted motor skills, adaptive behavior across 24 studies, 1,200+ participants | Level I |
RCT — Indian Journal of Pediatrics DOI | 2019 | Home-based sensory-motor interventions show significant outcomes when parent-delivered | Level II |
WHO Care for Child Development PMC9978394 | 2023 | CCD Package across 54 LMICs confirms household-material interventions effective | Level I–II |
NCAEP Evidence-Based Practices ncaep.fpg.unc.edu | 2020 | Video modeling, OT-structured intervention classified as EBP for autism motor targets | Level I |
Frontiers in Integrative Neuroscience DOI | 2020 | Neurological basis for sensory-based bilateral motor interventions confirmed | Level II |
20M+
Therapy Sessions
Exclusive 1:1 sessions in Pinnacle clinical data corpus
97%+
Improvement Rate
Measured across bilateral integration protocols at 70+ centers
70+
Countries
Teleconsultations served worldwide
Preview of 9 materials that help with bilateral movements Therapy Material
Below is a visual preview of 9 materials that help with bilateral movements therapy material. The pages shown help educators, therapists, and caregivers understand the structure and content of the resource before use. Materials should be used under appropriate professional guidance.




















Link copied!
The Pinnacle Promise
PINNACLE BLOOMS NETWORK®
Global Pediatric Therapeutic Consortium
OT • SLP • ABA/BCBA • SpEd • NeuroDev
WHO/UNICEF Framework Aligned
OT • SLP • ABA/BCBA • SpEd • NeuroDev
WHO/UNICEF Framework Aligned
GPT-OS® Technology Stack
TherapeuticAI® · AbilityScore® · FusionModule™ · EverydayTherapyProgramme™
Proven at Scale
20M+ exclusive 1:1 sessions · 97%+ measured improvement · 70+ centers · 70+ countries · 16 languages
"From fear to mastery. One technique at a time."
— The Pinnacle Blooms Consortium
Contact
📞 FREE National Autism Helpline: 9100 181 181 (24×7 | 16 languages)
🌐pinnacleblooms.org
✉️care@pinnacleblooms.org
📍 70+ centers across India
🌐pinnacleblooms.org
✉️care@pinnacleblooms.org
📍 70+ centers across India
Medical Disclaimer
This content is for educational purposes only and does not constitute medical advice. Bilateral coordination difficulties can stem from multiple underlying causes requiring individualized professional assessment. Persistent coordination challenges may indicate developmental coordination disorder (DCD), sensory processing differences, or neurological conditions requiring formal evaluation by a licensed occupational therapist, physical therapist, or developmental pediatrician. Never pressure a child beyond their current capabilities. Consult your child's medical team before beginning any new therapeutic intervention. Individual results vary by child profile, diagnosis, and intervention consistency.
CIN: U74999TG2016PTC113063 | DPIIT: DIPP8651 (Govt. of India Recognised Startup) | MSME: Udyog Aadhaar TS20F0009606 | GSTIN: 36AAGCB9722P1Z2
© 2025 Pinnacle Blooms Network®, a unit of Bharath Healthcare Laboratories Pvt. Ltd. All rights reserved. GPT-OS®, AbilityScore®, TherapeuticAI®, FusionModule™, and EverydayTherapyProgramme™ are proprietary marks of Bharath Healthcare Laboratories Pvt. Ltd. Patent applications filed across 160+ countries.
© 2025 Pinnacle Blooms Network®, a unit of Bharath Healthcare Laboratories Pvt. Ltd. All rights reserved. GPT-OS®, AbilityScore®, TherapeuticAI®, FusionModule™, and EverydayTherapyProgramme™ are proprietary marks of Bharath Healthcare Laboratories Pvt. Ltd. Patent applications filed across 160+ countries.