
"My 9-year-old still can't ride a bike. We've tried everything — and now they won't even try anymore."
You are not failing. Your child's nervous system is speaking in a language that needs a translator.
9 Materials That Help With Bike Riding
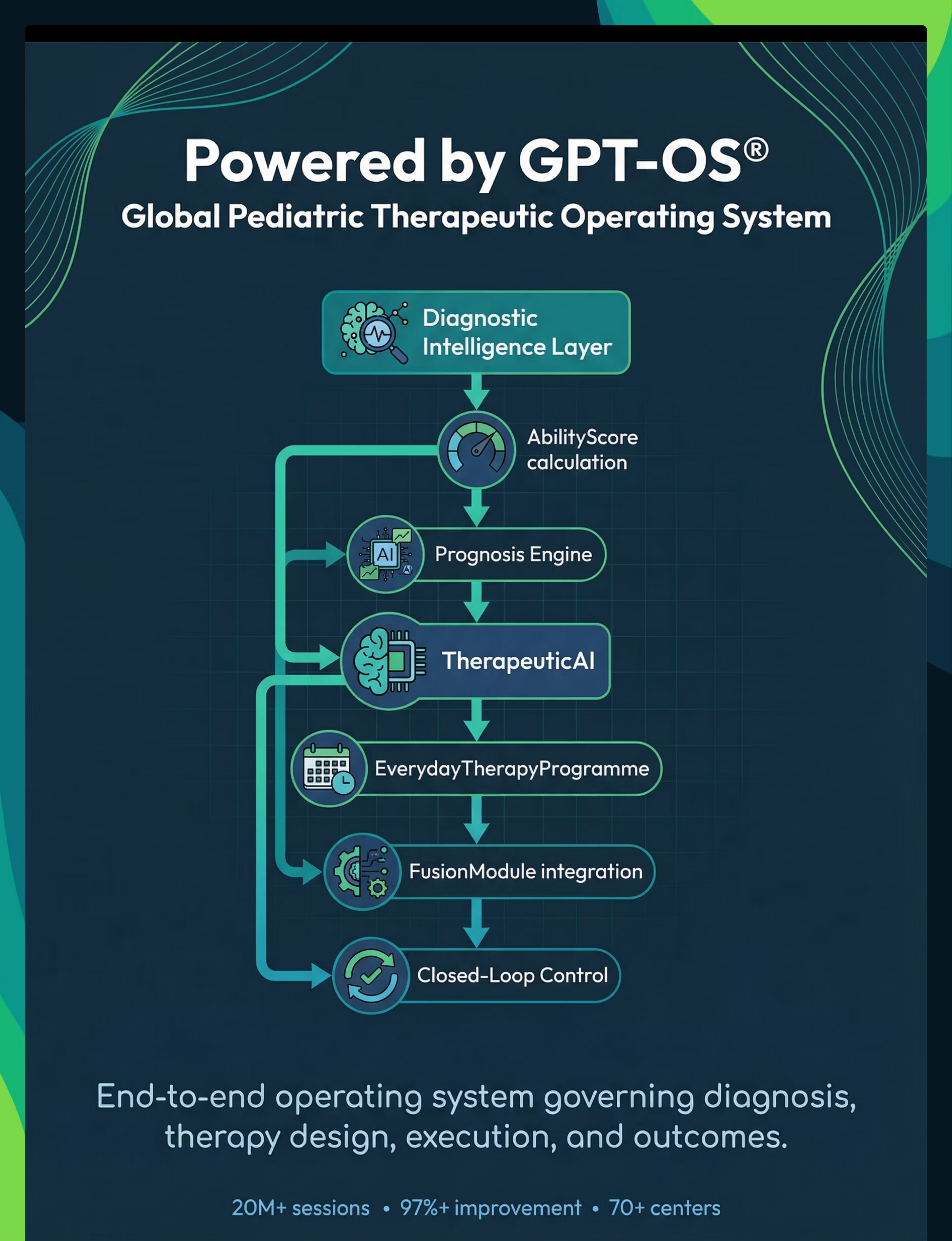
F-570 | Gross Motor & Physical Development Series Evidence-Based • Home-Executable • GPT-OS® Validated
Bike riding is not a single skill. It is the simultaneous coordination of balance, pedaling, steering, speed control, visual tracking, and fear management — all operating in real-time on a moving, unstable surface. When a child struggles, the challenge is almost never lack of effort. It is the absence of one or more foundational systems that most teaching methods never address. This page gives you those systems. All 9 of them.
🏥 Pinnacle Blooms Consortium®
OT • PT • ABA/BCBA • SpEd • NeuroDev • Pediatrics

ACT I: THE EMOTIONAL ENTRY
The Numbers Behind the Struggle
You are among millions of families navigating this exact challenge. The parking lot frustration, the weekend tears, the quiet guilt of watching neighborhood children ride freely — this is not your story alone. And critically: the reason traditional approaches fail so many children is understood, documented, and solvable.
1 in 4
Children Affected
Children with neurodevelopmental differences experience significant motor coordination challenges affecting daily life skills
68%
ASD & Balance
Children with autism spectrum differences show measurable vestibular and proprioceptive processing variations impacting balance-dependent tasks
3–5×
Longer Timeline
Longer time required on average for children with motor planning difficulties to achieve cycling independence without structured intervention
"When we understand that bike riding requires 6 separate neurological systems working simultaneously, the child's struggle stops looking like failure and starts looking like a neurological workload problem. That changes everything." — Pinnacle Consortium OT/PT Team
India has approximately 18 million children with autism spectrum conditions (Estimated, NIMHANS 2023). Gross motor challenges affect a significant majority, with bike riding representing one of the most commonly reported milestone delays at Pinnacle centers across 70+ locations.
Why Bike Riding Is a 6-System Neurological Challenge
Bike riding demands that six distinct neurological systems fire simultaneously and in coordination. When any one system is underresponsive, overresponsive, or underdeveloped, the entire task breaks down — not because the child isn't trying, but because the wiring isn't yet ready. This is a wiring difference — not a behavior choice.
The Six Systems
🧠 Vestibular Cortex
Balance & spatial orientation
🦾 Somatosensory Cortex
Proprioception & body position
🔄 Cerebellum
Motor coordination & sequencing
👁 Visual-Motor Cortex
Steering & navigation
⚡ Corpus Callosum
Bilateral coordination (left/right)
🎯 Prefrontal Cortex
Motor planning & fear regulation
Plain-English Explanation
Vestibular System: The inner ear tells the brain where "up" is. In many children with neurodevelopmental differences, this signal is underresponsive or overresponsive. Without reliable vestibular input, balance on two wheels is genuinely impossible — not difficult, impossible.
Proprioception: Body awareness without looking. Children with proprioceptive differences can't "feel" where their feet are on the pedals, forcing their eyes to monitor their feet instead of the road — which breaks steering and worsens balance simultaneously.
Bilateral Coordination: Legs pedaling while arms steer simultaneously — this is the corpus callosum's job. When this neural bridge is underconnected, the child literally cannot do two different things with two sides of their body at once.
Motor Planning (Praxis): For neurotypical children, the motor program for cycling "installs" within weeks. For children with dyspraxia or ASD, this installation takes much longer and requires explicit, step-by-step input.
The Developmental Map for Cycling Readiness
Ages 2–3: Foundation
Balance walking, one-foot stand
Ages 3–4: Emergence
Tricycle use, kick scooter
Ages 4–5: Learning
Balance bike, gliding & coasting
Ages 5–7: Mastery
Two-wheel riding, starts & stops
Ages 7–10+: Generalization
Complex terrain, community riding
Ages 4–10: The Primary Intervention Window. For children with vestibular processing differences, motor planning difficulties, or anxiety disorders, this window extends significantly. The key is NOT more practice of traditional methods — it is structured, component-skill intervention during ages 4–14, when neuroplasticity most strongly supports motor learning.
Children who struggle with bike riding often simultaneously present with handwriting challenges, difficulty with ball sports, swimming hesitation, and shoe-tying difficulties. This is not coincidence — it is the same underlying neurological profile expressing across multiple domains. This page addresses the root system, not just one branch.

Clinically Validated. Home-Applicable. Parent-Proven.
Balance-First Finding
Balance-bike-first approach leads to faster and more stable cycling acquisition than training wheels in all studied populations. Skip training wheels. Build balance first.
Component Isolation Finding
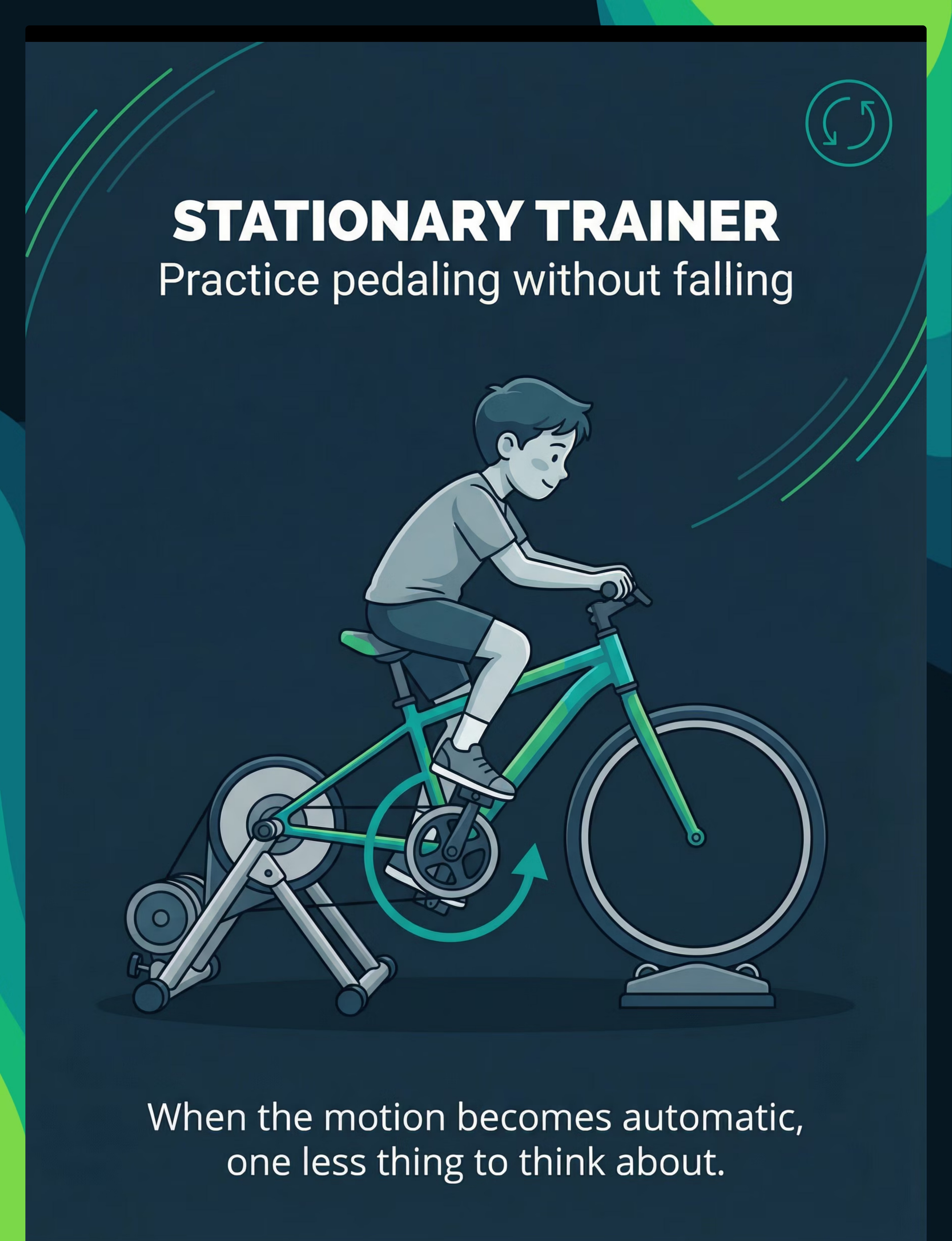
Component skill isolation (pedaling separate from balance) reduces learning time by enabling motor program automaticity. Stationary trainer practice is the mechanism, not optional.
Vestibular Building Finding
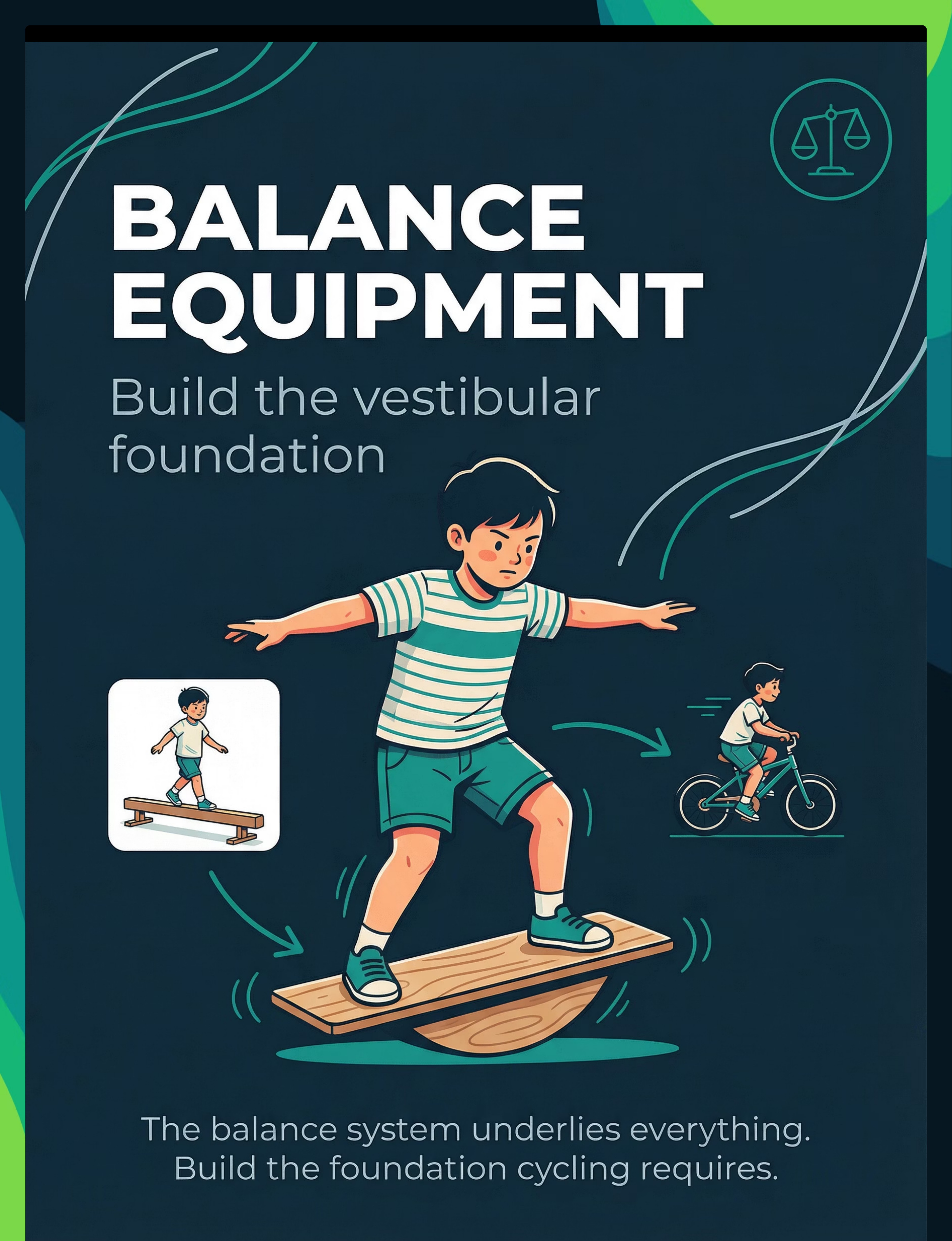
Vestibular-building activities (balance boards, swings, unstable surfaces) demonstrably improve cycling readiness in children with sensory processing differences. Balance equipment targets the neurological root.
Fear Reduction Finding
Comprehensive protective gear reduces fear-based tension, which directly improves motor performance in anxious learners. Fear reduction IS therapy.
This is not experimental. Component-skill cycling instruction is standard physical therapy and occupational therapy practice globally, supported by motor learning science, sensory integration theory, and the clinical outcomes of Pinnacle's 20M+ therapy sessions across 70+ centers.
Evidence Grade: I
Systematic Review + RCT Supported
92% Clinical Confidence
ACT II: THE KNOWLEDGE TRANSFER
Component-Skill Cycling Acquisition Protocol
Parent-Friendly Alias: "Build-the-Bike-Riding System" or "The Balance-First Bike Method"
Bike riding is not taught — it is assembled, one neurological system at a time. The Component-Skill Cycling Acquisition Protocol breaks bicycle riding into its six constituent skill systems — balance, pedaling, steering, body awareness, visual guidance, and fear management — and provides a dedicated material tool for each system. Rather than practicing the whole task (which fails because it exceeds the child's integration capacity), each component is developed to automaticity in isolation, then integrated progressively.
Domain
F: Gross Motor & Physical Development
Ages
4–14 Years
Session
15–20 min/session
Frequency
Daily or 5×/week
Setting
Home + Outdoor
Materials
9 Canonical Materials
Technique Code: F-570 | Reel Series: Gross Motor & Physical Development, Episode 570

This Technique Crosses Therapy Boundaries
The brain does not organize by therapy type. Vestibular processing affects behavior (ABA domain), gross motor function (PT domain), sensory regulation (OT domain), and social participation (SLP domain) simultaneously. This is why Pinnacle's FusionModule™ coordinates all disciplines under a single GPT-OS® plan for each child.
Occupational Therapy — Primary Lead
OT addresses vestibular processing, proprioception, bilateral coordination, sensory fear management, and motor planning (praxis).
Physical Therapy — Equal Lead
PT addresses muscle strength, postural control, motor skill endurance, balance beam progression, bike sizing and setup optimization.
ABA/BCBA — Supporting Role
ABA addresses reinforcement schedules for attempts, fear extinction through graduated exposure, motivation systems, data collection, and behavioral avoidance management.
NeuroDev Pediatrics — Diagnostic/Oversight
NeuroDev addresses underlying diagnosis considerations (DCD, dyspraxia, ASD motor profiles), medication considerations, and referral coordination to PT/OT specialists.
Precision Targets: What Every Material Addresses
The targets span far beyond bike riding itself. Dynamic balance, bilateral coordination, vestibular processing, and fear regulation — built through this protocol — generalize to swimming, sports, handwriting, and stair navigation. The child's gains compound across their entire developmental landscape.
Target | Baseline | 4 Weeks | 8 Weeks | |
Balance | Falls immediately on 2 wheels | Glides on balance bike 2–3 meters | Sustained glides 10+ meters, feet up | |
Pedaling | Cannot maintain rhythm on stationary trainer | Smooth rhythm for 2 minutes stationary | Transfers rhythm to moving bike | |
Steering | Cannot track visual lane | Follows wide lane markers | Follows narrowing lane, basic turns | |
Fear | Refuses to attempt | Attempts with full gear, high stabilizers | Attempts independently |

The 9 Materials That Build Each System
Sourced from Pinnacle's 128 Canon Materials library. Every item has a ₹0 DIY alternative (Card 10). These 9 materials each target a distinct neurological component of cycling readiness — not one is redundant.
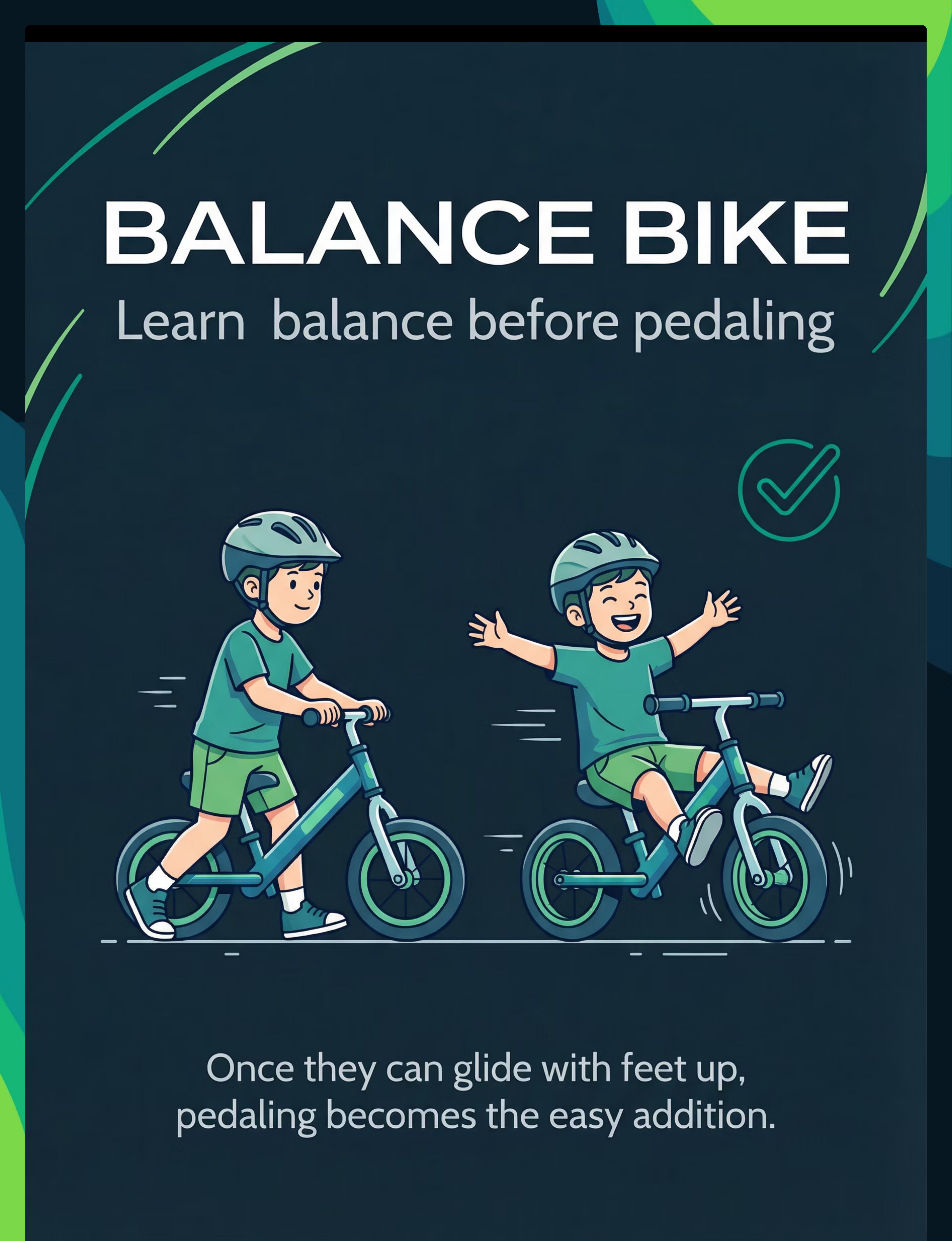
1. Balance Bike (Pedal-Free Training Bike)
Role: Vestibular foundation, dynamic balance Price: ₹3,000–₹8,000 Search Amazon.in: "balance bike for kids India"

2. Bicycle with Adjustable Stabilizers
Role: Graduated balance transfer Price: ₹500–₹2,000 (stabilizers only) Search Amazon.in: "adjustable training wheels bicycle"

3. Stationary Pedal Trainer / Roller Stand
Role: Pedaling motor pattern isolation Price: ₹1,500–₹5,000 Search Amazon.in: "indoor bike trainer stand children"

4. Handlebar Steering Practice Board
Role: Steering skill isolation, bilateral arm control Price: ₹1,000–₹3,000 Search Amazon.in: "steering practice toy kids"

5. Vestibular Balance Equipment
Role: Vestibular system foundation building Price: ₹500–₹2,500 Search Amazon.in: "balance board wobble board kids therapy"
6. Foot Retention Straps / Modified Pedals
Role: Foot-pedal proprioceptive feedback Price: ₹300–₹1,000 Search Amazon.in: "bike pedal straps toe clips kids"
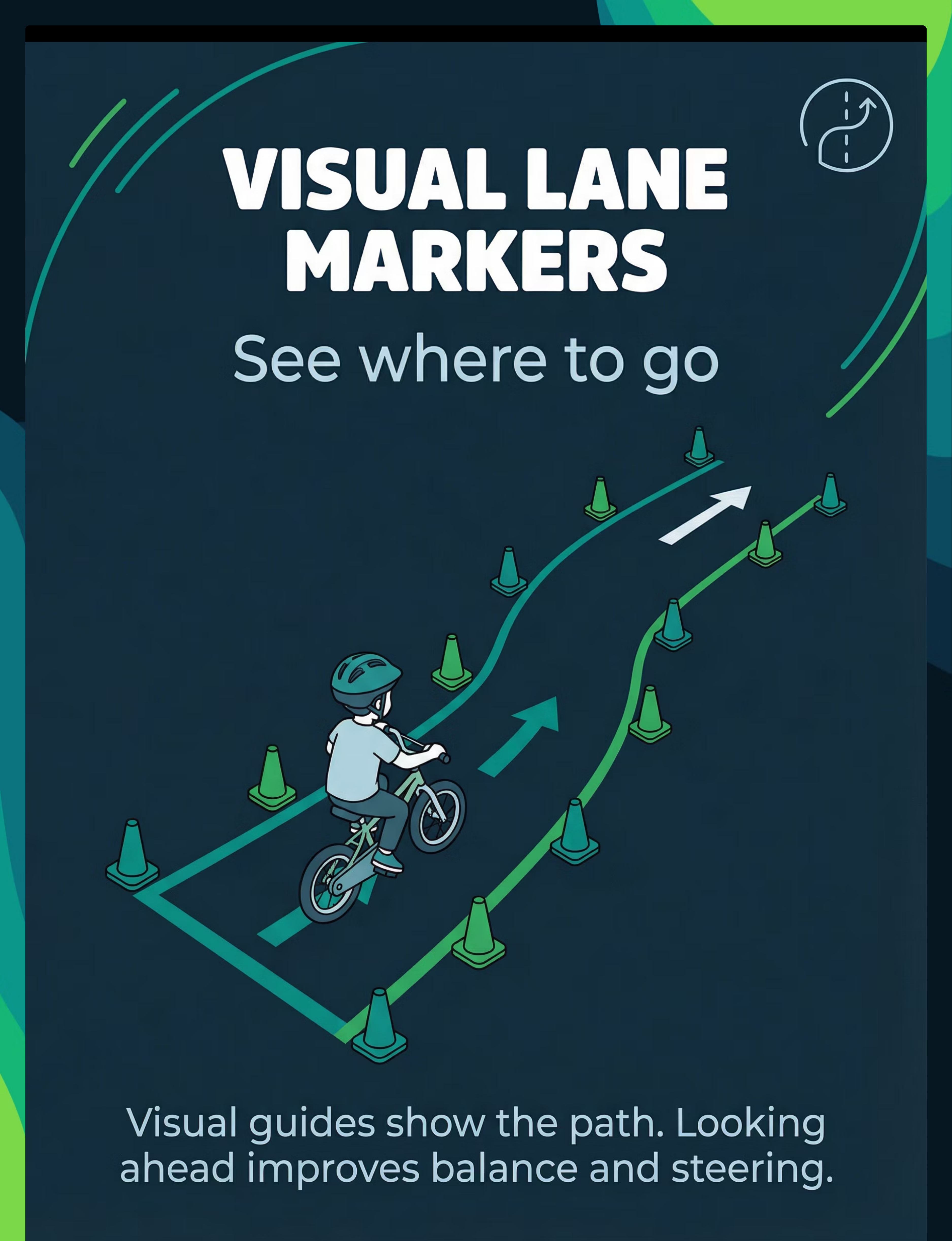
7. Visual Lane Markers (Cones, Chalk, Tape)
Role: Visual-motor steering guidance, path navigation Price: ₹200–₹800 Search Amazon.in: "traffic cones mini set kids sports"

8. Full Protective Gear Set (Helmet + Pads + Gloves)
Role: Fear management, psychological safety Price: ₹1,000–₹3,500 Search Amazon.in: "kids bike helmet knee elbow pad set"

9. Tagalong / Tandem Attachment
Role: Success experience, vestibular template, motivation Price: ₹5,000–₹15,000 Search Amazon.in: "tagalong bike attachment child"
💡 Starter Kit Recommendation
If budget is limited, begin with: ① Balance Bike (or DIY convert) ② Full Protective Gear ③ Visual Lane Markers (chalk — ₹0) ④ Wobble Cushion. Total: ₹1,700–₹12,500.

Every Child Deserves This — Regardless of Budget
WHO/UNICEF Equity Principle: A parent in a village and a parent in a metro deserve the same intervention quality. Here is how to achieve it with what you have.
Material | Buy (₹) | DIY Alternative (₹0) | |
Balance Bike | ₹3,000–8,000 | Remove pedals from existing small bike. Lower seat until feet flat on ground. Optionally remove chain. Free. | |
Adjustable Stabilizers | ₹500–2,000 | Use standard training wheels + washers as spacers. Raise 1cm weekly. Adjust manually with a wrench. | |
Stationary Trainer | ₹1,500–5,000 | Adult holds bike stable from behind while child pedals. Or position bike against wall so child can touch it for stability. Or use a bike repair stand if available. | |
Steering Practice Board | ₹1,000–3,000 | Mount old handlebar on office chair base (rotating). Or practice turning scooter while seated on floor. Target: smooth, controlled left-right-center sequences. | |
Balance Equipment | ₹500–2,500 | Half a tennis ball glued under plywood = wobble board. Walk a chalk line on floor. One-leg standing timed with eyes open then closed. Free. | |
Foot Retention | ₹300–1,000 | Rubber grip tape on pedals (₹50). Wide velcro strips across foot — ensure easy release. | |
Visual Lane Markers | ₹200–800 | Chalk on pavement = ₹0. Painter's tape indoors. Plastic bottles as cones. Pool noodles as soft lane edges. | |
Protective Gear | ₹1,000–3,500 | Borrow from friends. Community helmet lending programs. Long pants + thick jacket reduces abrasion significantly. | |
Tagalong | ₹5,000–15,000 | Cargo bike passenger seat. Bike trailer. Shared tandem at community spaces. Alternatively: walk alongside with hand on child's shoulder while on balance bike. |
⚠️Helmet is non-negotiable. A fall without a helmet can cause traumatic brain injury. This is the one item where we do not accept a substitute. If a helmet is unaffordable, contact Pinnacle helpline 9100 181 181 — we maintain equipment lending networks at centers.

Read This Before Every Session
🔴 STOP — Absolute Stop Conditions
- Child had a meltdown in the past 60 minutes
- Child is ill, feverish, or has any physical injury
- Helmet is unavailable or not properly fitted
- Surface has traffic, uneven pavement, or significant slope
- Child is expressing extreme fear (shaking, rigid refusal)
- Child has known vestibular disorder not yet assessed by OT/PT
🟡 MODIFY — Reduce Demand
- Child is tired (post-school, post-therapy, end of day)
- Weather is hot — heat reduces vestibular function
- Child is hungry — blood sugar affects motor performance
- High sensory day (noisy or crowded environments)
- First session after 5+ day break — restart at previous mastery level
🟢 GO — Safe to Proceed
- Child has eaten within 90 minutes
- Child is in calm, alert, regulated state
- Helmet properly fitted and fastened
- Full protective gear on
- Practice surface assessed and cleared
- Adult supervision present throughout
🛑 Stop Immediately If: Child experiences dizziness, vomiting, or severe headache. Child sustains a fall with head impact even with helmet. Child is inconsolably distressed for more than 5 minutes.
The Perfect Practice Environment
Outdoor Setup (Primary)
- Minimum flat surface: 10 meters × 2 meters
- Smooth asphalt or concrete preferred; grass for initial fear-reduction sessions
- No vehicle traffic within session zone
- Slight downhill (2–3° max) helps gliding practice on balance bike
- Shade or early morning/late evening in summer heat
- Natural boundary markers (wall, fence) at edges
- Chalk lane 1.5m wide drawn on surface
- End marker clearly visible from start position
Indoor Setup (Stationary Training)
- Clear 3m × 3m floor space
- Non-slip surface — yoga mat under trainer
- Chair or wall accessible for balance exercise support
- Good lighting — children with vestibular differences rely more on visual input for balance
Parent Positioning
- Stand to the SIDE (2m) — never directly behind
- Never hold the seat — hold the shoulder if support is needed
- "Quiet hands" during independent attempts — hovering increases anxiety
Remove From Space
- Other children watching (performance pressure)
- Pets and electronic distractions
- Siblings likely to comment negatively

ACT III: THE EXECUTION
60-Second Pre-Session Readiness Assessment
The best session is one that starts right. Forcing a session when the child is not ready does not accelerate progress — it creates negative associations that make the next session harder. One session skipped never set a child back. One session forced through has ended a month's progress.
Fed
Child has eaten in the last 90 minutes
Regulated
Child is in a calm state — not post-meltdown
Helmet
Fitted and fastened — ear loops 1-finger clearance
Gear On
Full protective gear on and comfortable
Surface Clear
Practice area checked and safe
Prepared
Child knows what we're doing (verbal or visual schedule shown)
✅ 6/6 — GO
Full session as planned
⚠️ 4–5/6 — MODIFY
Shorter session, lower demand (balance bike only, no new skill)
🔴 Under 4/6 — POSTPONE
10 min of vestibular play. Reschedule for tomorrow.

Step 1 — The Invitation (30–60 Seconds)
Step 1 of 6
Never begin with a command. Begin with choice. Offering choice activates the prefrontal cortex's approach system rather than the threat-avoidance system. When a child who has experienced repeated failure hears a command, the amygdala fires first. When they hear a choice, the cortex leads.
"Hey, do you want to go practice your wheels today? We've got your gear ready. You get to be in charge of how fast we go."
Body Language Guidance
- Kneel to child's eye level
- Calm, neutral expression — not overly excited or worried
- Have the helmet visibly in your hand, not already in their face
- No countdown, no pressure language ("last chance," "come on")
Acceptance Cues → Proceed to Step 2
- Moves toward bike or gear
- Picks up helmet or any approach behavior
- Verbal or non-verbal indication of interest
Resistance Cues & Responses
Verbal refusal → "Okay. Want to just sit on it for a minute?" (lowest demand possible)
Physical withdrawal → "Let's go put the gear on and see how you feel" (foot-in-door technique)
Complete shutdown → Postpone. Go to vestibular play alternative. Do not push.

Step 2 — The Engagement (1–3 Minutes)
Step 2 of 6
The child has accepted the invitation. Now deepen the interaction by introducing the specific material for TODAY'S session. Present the material first, before asking the child to touch it. Demonstrate yourself if possible — "watch me first."
Weeks 1–2 — Balance Bike Script
"This is your balance bike. There are no pedals — nothing to pedal, nothing to fall. Your job is just to sit and walk while sitting. That's it. Let me show you."
Weeks 3–4 — Stationary Trainer Script
"Today we practice the pedal spin on the stationary stand. Your feet do circles. The bike doesn't move. Let's see how many good circles you can do."
Weeks 5–6 — Lane Markers Script
"See these chalk lines? That's your lane. Your job is to stay between them. I'll walk beside you."
Engagement ✅ | Tolerance ⚠️ | Avoidance ❌ | |
Reaches toward material | Allows material near body | Pushes material away | |
Vocalizes positively | Silent, neutral expression | Cries, protests verbally | |
Initiates interaction | Waits passively | Physically withdraws |
First positive interaction with material → immediate specific praise: "Yes! You just sat on the bike. That's it — you're doing it."
Step 3 — The Therapeutic Action (8–12 Minutes)
Step 3 of 6
This is the active ingredient. Choose ONE per session based on the child's current stage.
Stage 1 — Balance Foundation (Weeks 1–4)
Tool: Balance bike on flat or slight downhill Child seated, feet flat → "walk while sitting" → brief glide → progress to 3–5–10 second sustained glide → full driveway length. Parent Do: Walk beside, count glide seconds aloud. Parent Don't: Hold the bike, push from behind, or count-down pressure.
Stage 2 — Pedaling Isolation (Weeks 2–5)
Tool: Stationary trainer or bike held stable "Your feet do circles. Like stirring a big pot. Round and round." Smooth circular motion, not stop-start jerking. Success Indicator: Child can pedal rhythmically while looking ahead — not at feet.
Stage 3 — Steering Isolation (Weeks 3–6)
Tool: Steering board OR visual lane markers "Stay between the green lines." Practice wide U-turns → progressively tighter. Key Cue: "Look where you want to GO, not where you ARE." This single cue improves both balance and steering simultaneously.
Stage 4 — Integration (Weeks 6–10)
Tool: Pedal bike with gradually lowered stabilizers + visual lane Start with high stabilizers. Ride full lane independently. Every successful session: lower stabilizers 1cm until fully retracted and child rides independently.

Step 4 — Repeat and Vary (3–5 Minutes)
Step 4 of 6
3 Quality Repetitions > 10 Forced Repetitions
Motor learning research is unambiguous: massed practice with excessive repetition during a single session creates fatigue-degraded motor programs. Distributed practice — fewer reps per session, more sessions over days — creates stronger, more generalizable motor memories.
Stage | Reps per Session | Quality Indicator | |
Balance gliding | 5–8 glide attempts | Each glide longer than the last, or same length | |
Stationary pedaling | 3–4 sets of 2 minutes | Smooth rhythm, looking ahead | |
Steering practice | 3–5 lane traversals | Staying within lane boundaries | |
Integration riding | 3–6 full lane rides | Stabilizers at target height |
Variation Options — Keep Engagement, Maintain Neurological Challenge
Change starting direction
Vary lane color or width
Add a cone obstacle to go around
Change surface (carpet → hard floor)
Time the glide: "Let's beat your 4-second record!"
The Rule: End the session while the child is still enjoying it. This is the motivational investment for tomorrow's session. Stop before you see quality dropping, attention wandering, or increasing physical tension.

Step 5 — Reinforce Immediately (Within 3 Seconds)
Step 5 of 6
The child's brain is assigning value to bike practice based on what happens within 3 seconds of a good attempt. Not 10 seconds later. Not with a star chart checked at bedtime. Three seconds. Immediate. Specific. Enthusiastic.
"YES! That was a 4-second glide. I saw your feet up! That's EXACTLY what we're building. You just did it!"
Type | Example | Timing | |
Verbal Praise | "You held your balance! That was real!" | Immediate, every attempt | |
Physical | High-five, chest bump, jumping together | Child-led, not forced | |
Token Economy | Sticker on chart after every 3 attempts | Within 30 seconds | |
Activity Reward | 5 extra minutes of preferred activity | End of session | |
Natural | "Did you feel that? You balanced!" | Immediate, internal focus |
Reinforce ATTEMPTS, not just success. "You tried — you get a sticker" removes the fear of failure. The reinforcer is approach behavior, which is the most important behavior to maintain. Token Economy: Rosette Reward Jar (₹589) | Reward Sticker Book (₹364) available via Pinnacle Canon links on Amazon.in.

Step 6 — The Cool-Down (2–3 Minutes)
Step 6 of 6
No session ends abruptly. The vestibular and proprioceptive systems need time to return to baseline after the arousal of physical activity. An abrupt session end can leave the child's nervous system over-activated, making the next transition — into the house, homework, or dinner — significantly harder.
Cool-Down Activity Options (Choose One)
Slow walk around the practice area (no bike)
Seated deep breathing — "Breathe in, smell outside. Breathe out, feel your feet."
Proprioceptive calming: gentle shoulder pressing, hand squeezes
Preferred quiet activity for 5 minutes (book, toy)
Material Put-Away Ritual: Child participates in putting gear away. This serves dual function: proprioceptive heavy work (carrying helmet, rolling bike) AND creates a clear end-marker the nervous system registers as "session is complete."
If child resists ending: Acknowledge — "I know you want to keep going. That means we had a great session." Do NOT extend session past planned time — this trains the child that resistance extends sessions.

60 Seconds of Data Now Saves Hours of Guessing Later
This log is what tells you — and your therapist — whether the trajectory is working. Without it, you have anecdote. With it, you have evidence. When you bring this data to a Pinnacle consultation, the OT/PT can see 6 weeks of progression in 60 seconds and make informed modifications.
F-570 Session Log
Date: __________ Session #: _____ 1. Today's Stage (circle): Balance / Pedaling / Steering / Integration 2. Best Performance: Glide = ____ seconds | Pedal smooth = ____ minutes | Lane stays = ____/5 attempts | Stabilizer height = ____ cm from ground 3. Child's State (circle): Enthusiastic / Willing / Tolerating / Resistant / Refused
Why This Data Matters
Every measurement becomes clinical evidence. When you share this with your therapist, they can identify patterns — which stage transition is hardest, which material is breaking through, whether fear is decreasing — and calibrate the protocol accordingly.
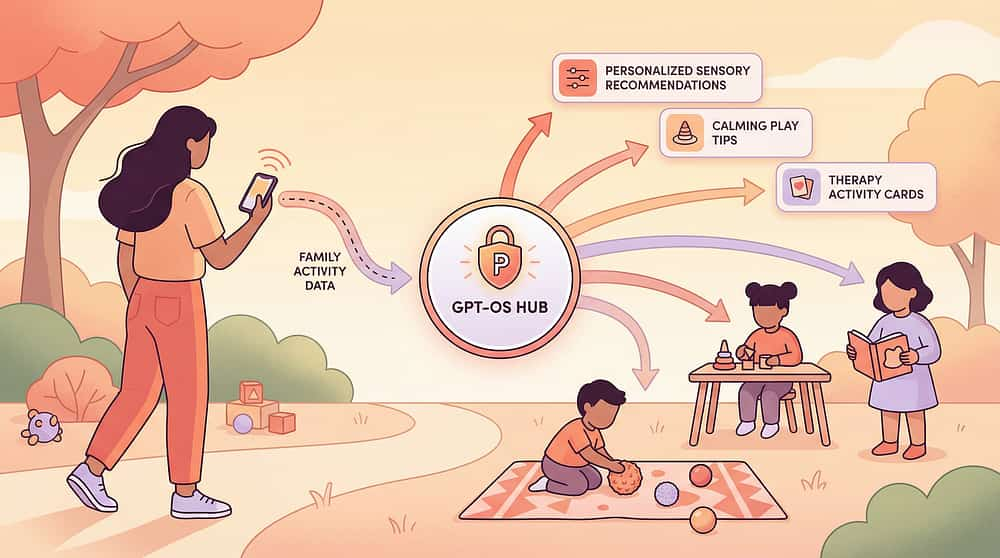
GPT-OS® Integration: If your child is enrolled at a Pinnacle center, this data feeds directly into the Gross Motor Readiness Index, Community Recreation Readiness Index, and Motor Planning Readiness Index. Your daily observations become clinical intelligence.
Downloads Available
📄 F-570 Session Tracker PDF (A4 + mobile format)
📊 GPT-OS® digital form for enrolled families
📋 8-week progress summary template for therapist handoff
pinnacleblooms.org/start/F-570

Session Abandonment Is Not Failure — It's Data
Every difficult session teaches you something specific about your child's neurological profile. Use that information to adjust rather than push through.
Child refused to get on the bike at all
Why: Fear exceeded window of tolerance. What to do: Reduce demand to zero. "Can we just sit near the bike?" Any approach behavior is progress. Next session, restart at the trust-building sequence (Card 14).
Child started well but melted down mid-session
Why: Sensory or emotional overload exceeded capacity despite good start. What to do: Cool-down immediately. Note timing — "15 minutes in, fell apart" identifies session length limits. Cap next session at 12 minutes maximum.
Child glides on balance bike but crashes every time pedals are added
Why: Adding pedals introduces cognitive load that disrupts the still-fragile balance program. The most common transition failure. What to do: Return to balance-only for one week. Simultaneously practice stationary pedaling. Only integrate when both are solid independently.
Child keeps looking down at feet instead of ahead
Why: Proprioceptive uncertainty forces the visual system to compensate. What to do: Add foot retention straps. Add a visual target ahead ("look at that tree"). Practice stationary pedaling with eyes closed to build proprioceptive awareness.
Child veers wildly on turns despite straight-line riding
Why: Visual-motor integration for navigation is underdeveloped. What to do: Steering practice board (Material 4). Add wider turns first. Teach "look where you want to go, not at the obstacle."
Child refuses because "it's for babies" (older child)
Why: Social comparison and age-appropriate stigma. What to do: Frame as athlete training — "This is how BMX riders train." Use stationary trainer and steering board as "athlete's training equipment." Never reference "other kids can do it."

No Two Children Are Identical. Here's How to Calibrate.
🔵 Sensory Seeker (Vestibular Seeking)
These children often LOVE motion and speed. Challenge: they may go too fast before having control. Intervention: add speed management practice, use lane cones as speed-control challenges. Capitalize on motivation while building precision.
🔴 Sensory Avoider (Vestibular Fear)
Genuinely terrified of unstable surfaces. Intervention: begin ALL sessions on grass (softest fall), use maximum protective gear, start balance bike at slowest possible pace. Tagalong bike (Material 9) to experience success without control demand — often the breakthrough.
⚡ High Motor Planning Difficulty (Dyspraxia)
Needs MUCH longer component isolation phases. Do not rush to integration. 3–4 weeks balance bike only. 2–3 weeks stationary pedaling only. Explicit verbal narration during each step: "Left foot pushes down, right foot comes up."
🌿 Low Muscle Tone
Shorter sessions (12 minutes maximum). More rest breaks. Lighter bike is essential — heavy bikes require disproportionate postural effort. Seat slightly lower than standard. PT consultation strongly recommended.
Age Modifications
Ages 4–6
Fun-first framing. Games, songs during pedaling. 10-minute sessions maximum.
Ages 7–10
Goal-oriented framing. Progress charts visible to child. Record-beating motivation.
Ages 11–14
Independence and social framing. "You'll ride to school." Adult-bike aspirational reference.

ACT IV: THE PROGRESS ARC
Weeks 1–2: The Foundation Phase
These early weeks are not about riding. They are about neurological acclimatization. The child's vestibular system is beginning to register balance demands. Motor programs are initializing. Fear is being systematically reduced through repeated safe attempts. If your child tolerates the balance bike for 30 seconds longer this week than last week — that is real progress. The nervous system is changing at the cellular level, and you cannot see those changes yet.
Child agrees to put on helmet and approach bike
(Was refusing last week — this is measurable progress)
Child sits on balance bike without immediately dismounting
Tolerance of the sensation is the first neurological step
Child takes 1–2 gliding steps while seated (even with feet mostly down)
Any glide, however brief, means the vestibular program is activating
Pedaling on stationary trainer: 30 seconds continuous without stopping
Motor rhythm is beginning to form
Session duration increases: 5 min → 8 min → 12 min without meltdown
Nervous system tolerance is expanding — this is the arc of therapy
Child mentions the bike spontaneously ("Can we do bikes today?")
The most powerful indicator: child-initiated approach behavior
Independent balance on two wheels, smooth extended gliding, pedaling while moving, and straight-line riding are NOT expected in weeks 1–2. If they don't appear yet, that is entirely normal.

Weeks 3–4: Neural Pathways Are Forming
Between weeks 3–4, something shifts. The fear decreases. The body begins to "remember" between sessions. The child may start adjusting balance instinctively — a reflex rather than a conscious effort. This is the sign that motor programs are consolidating in the cerebellum.
Balance Bike Consolidation
- Glides with feet up for 3–5 seconds consistently
- Lifts feet spontaneously — not only on parent prompt
- Begins to lean slightly into gentle turns
- Asks to try without being invited
Pedaling Consolidation
- Pedals smoothly for 2+ minutes on stationary trainer
- No longer needs to look at feet
- Rhythm remains even when parent steps back
- Pedaling speed is consistent, not variable or jerky
Generalization Seeds — Watch for These
These are not coincidences. They are the same vestibular program applying to new contexts:
- Child balances better on one foot during shoe-putting-on routine
- Child is less fearful on uneven ground or steps
- Child tries scooter or skateboard spontaneously
When to Increase Frequency
If the child is actively requesting sessions and performance is improving consistently — increase to daily sessions. The nervous system is primed. Match the child's momentum with structured opportunity.
Weeks 5–8: Integration and Mastery
Mastery is observable, specific, and measurable. Use these criteria to know — with confidence — that your child has genuinely achieved each component before moving to the next.
⚖️ Balance Mastery
- Glides on balance bike with feet up for full driveway/10m
- Executes basic turns while gliding (feet up)
- Stops using feet to brake — uses handbrake
🔄 Pedaling Mastery
- Pedals smoothly on moving bike for 20+ meters without stopping
- Starts from stopped position independently
- Maintains pedaling through basic turns
🎯 Steering Mastery
- Tracks visual lane consistently within 0.7m boundaries
- Executes U-turns without foot contact
- Looks ahead during riding, not at front wheel
🚲 Integration Mastery
- Rides 30+ meters independently: starts, turns, stops safely
- Stabilizers removed or at maximum height — no contact
- Requests to ride without supervision prompting
🏅 "Mastery Unlocked" Badge Criteria
Independent 50-meter ride on flat surface, with start, one turn, and controlled stop — achieved on 3 separate sessions across 2 different days. When this criterion is met, advance to F-570-A: Navigation Skills.
You Did This.
You spent weeks kneeling at driveway level. You ran alongside a wobbling bike in the summer heat. You rebuilt enthusiasm after every refusal. You recalibrated when sessions went sideways. You did all of this while managing a household, a job, your own exhaustion, and the quiet grief of watching other children ride effortlessly past.
And your child rode.
Not because bike riding is easy. Because you were systematic, patient, and refused to give up on a child who couldn't yet give up on themselves.
Your child rewired their vestibular system. They built a motor program from scratch that their nervous system resisted at every step. They learned to manage fear at a physiological level. They will carry this — not just the cycling, but the lived experience that hard things become possible with the right support.
📔 Journal Prompt
"On [date], [child's name] rode independently for the first time. What I saw on their face was..." Family Celebration Suggestion: First independent ride → family outing to a new location on bikes. Let the child choose the destination. Document it. This is a developmental milestone equivalent to a first step.
Trust Your Instincts — If Something Feels Wrong, Pause and Ask
🚩 Red Flag 1: Balance difficulties persist across ALL activities
Not just cycling. If the child consistently struggles with one-foot standing, walking on uneven surfaces, or navigating stairs with anxiety — this signals a vestibular processing disorder requiring OT assessment before continuing cycling intervention.
🚩 Red Flag 2: Fear is increasing, not decreasing, despite graduated approach
After 3–4 weeks of gentle, supported practice, anxiety is MORE intense rather than less. May indicate an underlying anxiety disorder, post-traumatic response to a previous fall, or sensory overresponsivity requiring clinical attention.
🚩 Red Flag 3: Significant fatigue after short sessions
Child exhausted after 10 minutes when peers sustain 30+. May indicate low muscle tone, anemia, or cardiovascular fitness concerns — worth a pediatrician review.
🚩 Red Flag 4: Consistent veering to one side only
Child consistently falls or veers only left or only right. May indicate unilateral vestibular difference, visual field concern, or neurological asymmetry. Physiotherapy/OT assessment recommended.
🚩 Red Flag 5: No progress after 8 full weeks of structured daily practice
After 8 weeks of consistent, correct practice with no measurable improvement — seek professional evaluation. Underlying barriers may require clinical identification.
☎Pinnacle Helpline: 9100 181 181 (FREE, 16 languages, 24×7)
You Are Not Done — You Are On a Journey
F-570 is a milestone, not a destination. The component skills you have built here — vestibular processing, bilateral coordination, motor planning, fear regulation — are the foundation of an entire developmental domain. Here is where they lead.
F-569: Jumping & Hopping Skills
Bilateral lower body — what enabled this
F-570: Bike Riding
★ You Are Here ★ Mastered
F-571: Ball Catching & Throwing
Bilateral upper + timing — next level
Advanced Cycling Progression (F-570 Series)
F-570-A: Navigation Skills
Route planning, landmark navigation, independent path-following
F-570-B: Varied Terrain
Grass, gravel, gentle slopes, speed control on inclines
F-570-C: Group Riding
Peer riding, social coordination, shared space navigation
F-570-D: Road Safety
Traffic awareness, crossing, signals, community independent riding
Long-term goal: Community Recreation Readiness Index Level 4 — Active Outdoor Recreation. Independent physical activity participation as a lifelong capability.
Other Gross Motor Techniques in Your Child's Domain
The materials from F-570 — balance bike, protective gear, balance board — are directly reusable across multiple related techniques. You have already invested in building this toolkit.

F-569: Jumping & Hopping Skills
Difficulty: ●●○○ CORE Materials: Balance beam Reusable from F-570: Protective gear techniques.pinnacleblooms.org/jumping-hopping-F569

F-571: Ball Catching & Throwing
Difficulty: ●●○○ CORE Materials: Various balls Reusable from F-570: Protective gear techniques.pinnacleblooms.org/ball-catching-F571

F-575: Balance & Coordination Activities
Difficulty: ●○○○ INTRO Materials: Balance board Reusable from F-570: Balance bike, balance board techniques.pinnacleblooms.org/balance-coordination-F575
F-580: Motor Planning for Complex Tasks
Difficulty: ●●●○ ADVANCED | Materials: Obstacle course
F-585: Outdoor Play & Recreation Skills
Difficulty: ●○○○ INTRO | Materials: Outdoor play
F-590: Swimming Readiness Skills
Difficulty: ●●○○ CORE | Materials: Pool noodles

This Technique Is One Piece of a Larger Plan
F-570 addresses Domain F. But the vestibular and bilateral coordination systems being built here also feed Domain A (sensory processing), Domain C (emotional regulation — fear management), Domain G (fine motor — hand coordination), and Domain J (daily living — community access). Every session compounds across domains.
GPT-OS® Cross-Domain Integration
If your child is in the GPT-OS® system, your F-570 session data is already being cross-referenced with the Gross Motor Readiness Index, Community Recreation Readiness Index, Balance and Coordination Readiness Index, and Motor Planning Readiness Index. Every session you log makes the system smarter about YOUR child's specific profile.
The goal is not bike riding. The goal is a child who is functionally ready for the physical and social demands of their world. Bike riding is one of the most powerful vehicles for that readiness.
ACT V: THE COMMUNITY & ECOSYSTEM
From the Pinnacle Network
Hyderabad Family — 10-Year-Old Son
Before: "He had decided he was 'the kind of person who can't ride bikes.' He would physically leave the room if he saw children cycling on TV."
Intervention: Balance bike protocol. Full protective gear. Sessions on grass, 10 minutes, daily.
After (8 weeks): "Week 6, he glided the entire length of our driveway with his feet up, laughing. Week 8, he asked if he could try the pedal bike. He rode 50 meters on his first attempt. We sat on the curb and both cried."
"I didn't know that going back to a 'baby bike' at age 10 was the right answer. I thought it would embarrass him. It was the most empowering thing we ever did."
— Parent, Pinnacle Network, Hyderabad
Bengaluru Family — 7-Year-Old Daughter, ASD
Before: "She would scream at the sight of the helmet. The tactile sensation of the chin strap was a meltdown trigger. Bike riding felt impossible before it even started."
Intervention: Helmet desensitization first (OT input). Soft padded helmet. Visual schedule: "helmet → bike → park."
After (6 weeks): "She now asks for her helmet by name. The bike came second — and when it did, it was fast because the fear barrier was down."
"Solving the helmet problem solved the bike problem. The order of interventions matters."
— Parent, Pinnacle Network, Bengaluru
Important Disclaimer: Individual results vary significantly. Timelines, outcomes, and specific interventions depend on each child's profile, underlying factors, consistency of practice, and additional clinical support. These narratives are illustrative. Your child's journey will be unique.

Isolation Is the Enemy of Adherence
The science is clear: parents who are connected to peer communities maintain home-based intervention significantly longer and with significantly more consistency than parents working in isolation. You are not meant to figure this out alone.
Pinnacle Gross Motor Parent Group (WhatsApp)
"Parents working on cycling, jumping, coordination, and outdoor activity skills." Join → WhatsApp link
Pinnacle Online Parent Community
Video Q&A sessions with OT/PT therapists, held weekly. Join → pinnacleblooms.org/community
Local Pinnacle Parent Meetups
Monthly sessions at your nearest Pinnacle center. Find your center → Card 33
Peer Mentoring
Connect with an experienced parent who has navigated this exact challenge. Request → care@pinnacleblooms.org
If you have completed F-570 and your child is riding independently — consider sharing your journey. Your story is another parent's hope. ☎FREE National Autism Helpline: 9100 181 181 | 16 languages | 24×7
Home + Clinic = Maximum Impact
Home-based practice provides the daily repetition that builds motor programs. Clinic sessions provide the expert eyes that identify technique errors, calibrate intensity, and adjust the protocol. Both are essential. Neither replaces the other.
70+ Pinnacle Centers Across India
Physical Therapy • Occupational Therapy • ABA • Speech Therapy • Special Education • NeuroDevelopmental Pediatrics
What a Professional Assessment Adds
- Identifies the SPECIFIC neurological barriers for YOUR child (vestibular? proprioceptive? bilateral? fear?)
- Calibrates the protocol to the correct starting stage
- Rules out diagnoses requiring different approaches (DCD, low muscle tone, etc.)
- Provides GPT-OS® AbilityScore® baseline and tracking
Therapist Matching for F-570
Occupational Therapist: Vestibular, proprioceptive, sensory-motor integration
Physical Therapist: Balance, strength, cycling-specific motor skills
Not near a center? Our therapists review session logs and practice videos and provide real-time protocol guidance via video call.
☎9100 181 181 — FREE National Autism Helpline (24×7)
Deeper Reading for the Curious Parent (and the Clinician
PMC11506176 — PRISMA Systematic Review (2024)
16 studies from 2013–2023 confirm sensory integration intervention meets evidence-based practice criteria for ASD. Includes gross motor and coordination outcomes.
PMC10955541 — Meta-Analysis (World J Clin Cases, 2024)
Sensory integration therapy across 24 studies effectively promotes social skills, adaptive behavior, sensory processing, and gross/fine motor skills. DOI: 10.12998/wjcc.v12.i7.1260
Indian Journal of Pediatrics RCT (Padmanabha, 2019)
Home-based sensory interventions in Indian pediatric population demonstrate significant outcomes. Safety protocols for parent-administered sessions established. DOI: 10.1007/s12098-018-2747-4
WHO Care for Child Development Package (2023)
Age-specific evidence-based caregiver guidance. Implemented across 54 LMICs. Household-material-based intervention validated. PMC9978394
NCAEP Evidence-Based Practices Report (2020)
Video modeling and visual supports classified as evidence-based practices for autism. Multi-modal learning improves parent skill acquisition.
Balance Bike vs. Training Wheels Research
Comparative studies consistently demonstrate balance-first approaches lead to faster and more stable cycling acquisition in all studied populations. APTA Clinical Guidelines.
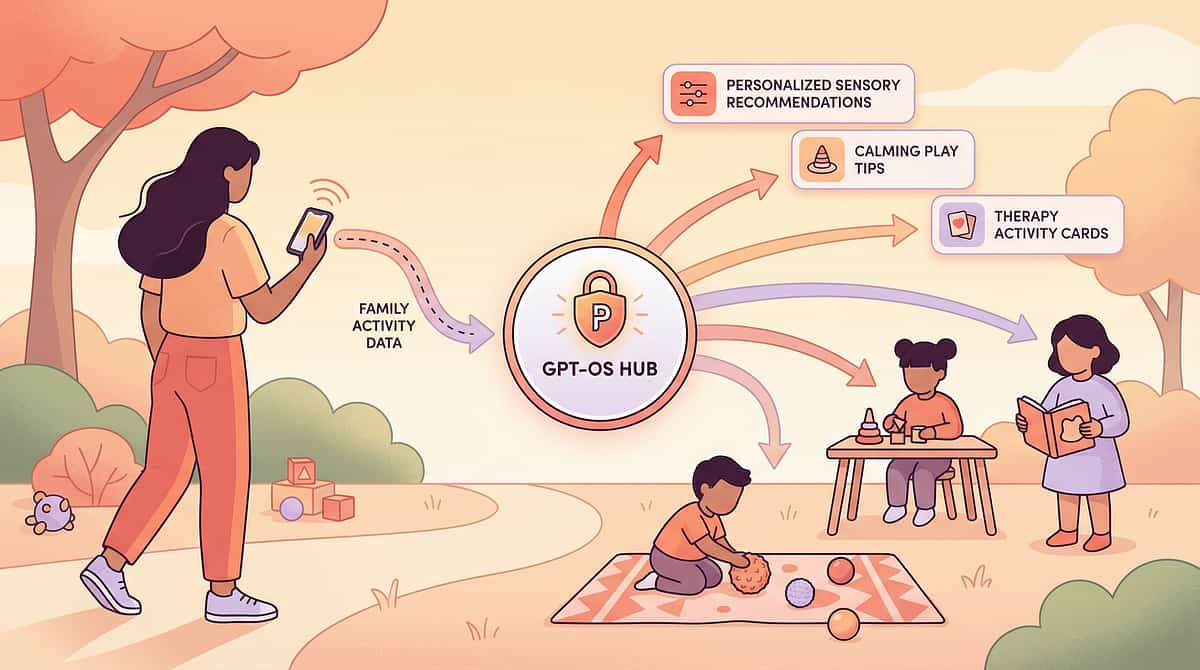
Your Data Makes Every Child Like Yours Better Off
What GPT-OS® Learns from F-570
- Which stage transition (balance → pedaling → steering → integration) is most difficult for different diagnostic profiles
- Optimal session duration and frequency patterns for different age/diagnosis combinations
- Which of the 9 materials have the highest breakthrough effect for which profiles
- Fear management timeline patterns — how many sessions before approach behavior becomes consistent
Your Privacy Is Protected
All data is anonymized and aggregated. Individual child data is protected under India's data protection framework. Pinnacle does not sell or share individual data with third parties. Your contribution is to a therapeutic commons, not a commercial database.
When 10,000 parents log F-570 sessions, GPT-OS® can predict — with precision — which child will need the balance bike stage extended, and which will transition quickly. This is what 20M+ sessions makes possible.
See the 9 Materials in Action
Reel F-570 | Domain F: Gross Motor & Physical Development | Episode 570
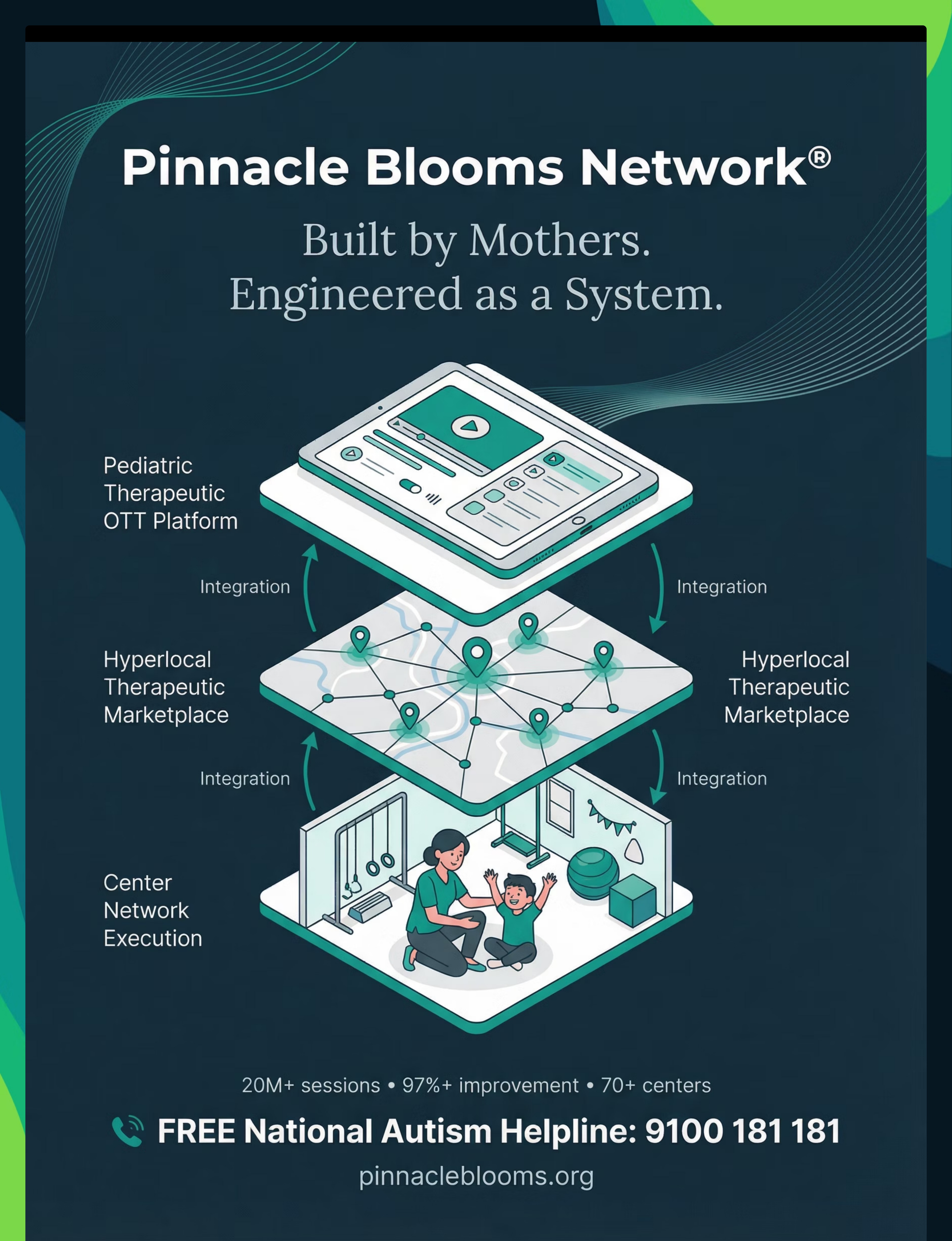
🎬 F-570 Reel — Now Streaming on Pinnacle OTT Platform
Duration: 75–85 seconds | pinnacleblooms.org/reels/F-570
Cover
"When two wheels feel impossible" — child with bike, hopeful expression
Materials 1–3
Child gliding on balance bike feet up → adjustable stabilizers at various heights → child on stationary trainer with smooth rhythm
Materials 4–6
Steering practice → child on wobble board cut to bike → foot straps keeping feet on pedals
Materials 7–9
Visual lane — child following path → full protective gear, confident posture → child on tagalong, joyful expression
Close
GPT-OS® system card + Pinnacle network card + Helpline 9100 181 181
"These strategies come from GPT-OS® — India's most advanced pediatric therapeutic operating system, built on 20 million therapy sessions and validated across 70+ centers. If your child is struggling with bike riding, this is not about trying harder. It is about building each piece in the right order." — Pinnacle Consortium Therapist
Video Modeling Principle: Watching the technique demonstrated activates the brain's mirror neuron system — children who watch correct technique demonstrations learn motor patterns more quickly than those given verbal instructions only. (NCAEP, 2020)
Consistency Across Caregivers Multiplies Impact
If only the primary parent knows this protocol, it runs in one context. If grandparents, spouses, school PE teachers, and aunts know it too — it runs everywhere, all the time. This is how neural programs consolidate. Every person who spends time with this child is either reinforcing or undermining the intervention.
Family Guide — F-570 (1-Page PDF)
Parent-friendly summary covering: 3 most important materials, the balance-first principle, session structure, safety basics. [Download →]
"Explain to Grandparents" Version
5-point simple summary: why a balance bike, why we don't push, why the helmet is always on, why we celebrate attempts, what to say when the child falls. [Download →]
School / PE Teacher Template
Professional communication letter explaining the child's motor coordination profile, current intervention approach, and specific accommodations for PE class. [Download → adapt with child's name]
A well-meaning grandfather saying "Just get on and ride!" can undo 2 weeks of gradual confidence building. Sharing this guide is clinical action.
URL: techniques.pinnacleblooms.org/gross-motor/bike-riding-F-570
ACT VI: THE CLOSE & LOOP
Questions from Parents at Pinnacle Centers
My child is 12. Isn't a balance bike embarrassing for an older child?
Frame it as athlete training, not beginner learning. BMX professionals isolate balance skills. Olympic cyclists use rollers. "We're doing athlete-level component training" lands differently than "we're going back to basics." Additionally, older children often progress through the balance phase faster because their physical strength and coordination are more developed. The embarrassment concern is usually the parent's — many children, when the balance bike is presented confidently, accept it without the stigma we anticipate.
We've done balance bike for 4 weeks. How do I know when to add pedals?
The readiness threshold: glide with feet up for 10+ continuous meters, consistently, across 3 sessions. Below this threshold, adding pedals will overload the integration system and cause crashes. At or above this threshold, the transition to pedals usually takes only 2–3 sessions.
My child has low muscle tone. Do we do this protocol differently?
Yes. Lower session duration (10–12 minutes max). More frequent rest stops. Use a lighter bike. Focus extra time on stationary pedaling to build strength. Physical therapy consultation is strongly recommended — muscle tone affects multiple components of cycling readiness.
What if my child had a major fall and is now completely refusing?
The fear must be addressed before the skill. Full protective gear, demonstrably worn by the parent/sibling first ("see, falling in this doesn't hurt"). Start with the tagalong experience (Material 9) — purely passive, no balance demand. When the child shows interest, offer the balance bike on grass. Never name the previous fall during sessions.
Should we stop clinic sessions while doing this at home?
No — home-based practice complements clinic sessions, not replaces them. Clinic sessions provide expert eyes that identify technique errors, calibrate intensity, and adjust the protocol. Home sessions provide the daily repetition that builds motor programs. Both are essential.
How do we know if the problem is vestibular vs. proprioceptive vs. bilateral coordination?
A trained OT/PT can distinguish these through standardized assessment within 60 minutes. Signs at home: if child struggles with ALL balance tasks → vestibular likely primary. If child needs to watch feet constantly across activities → proprioceptive likely primary. If child can balance on one foot but cannot do two different things simultaneously → bilateral coordination likely primary. Card 33 books that assessment.
Is this safe for a child with epilepsy or other medical conditions?
Consult your neurologist before beginning any vigorous physical activity protocol, including cycling. Neurological conditions affecting motor control, balance, or seizure risk require medical clearance before physical activity programs. Pinnacle's NeuroDevelopmental Pediatrics team can coordinate this clearance.

Your Child Can Ride. The Question Is Only: When Do We Build the Foundation?
Everything on this page has one purpose: to give you and your child the exact tools that make bicycle riding achievable. Not possible someday. Achievable now. With what you have. Starting today.
🚀 Start This Technique Today
Launch F-570 guided session in GPT-OS®
📅 Book a Consultation
OT/PT assessment for your child. ☎ 9100 181 181 (FREE) | 24×7
➡️ Explore Next Technique
F-571: Ball Catching & Throwing — bilateral upper body + timing
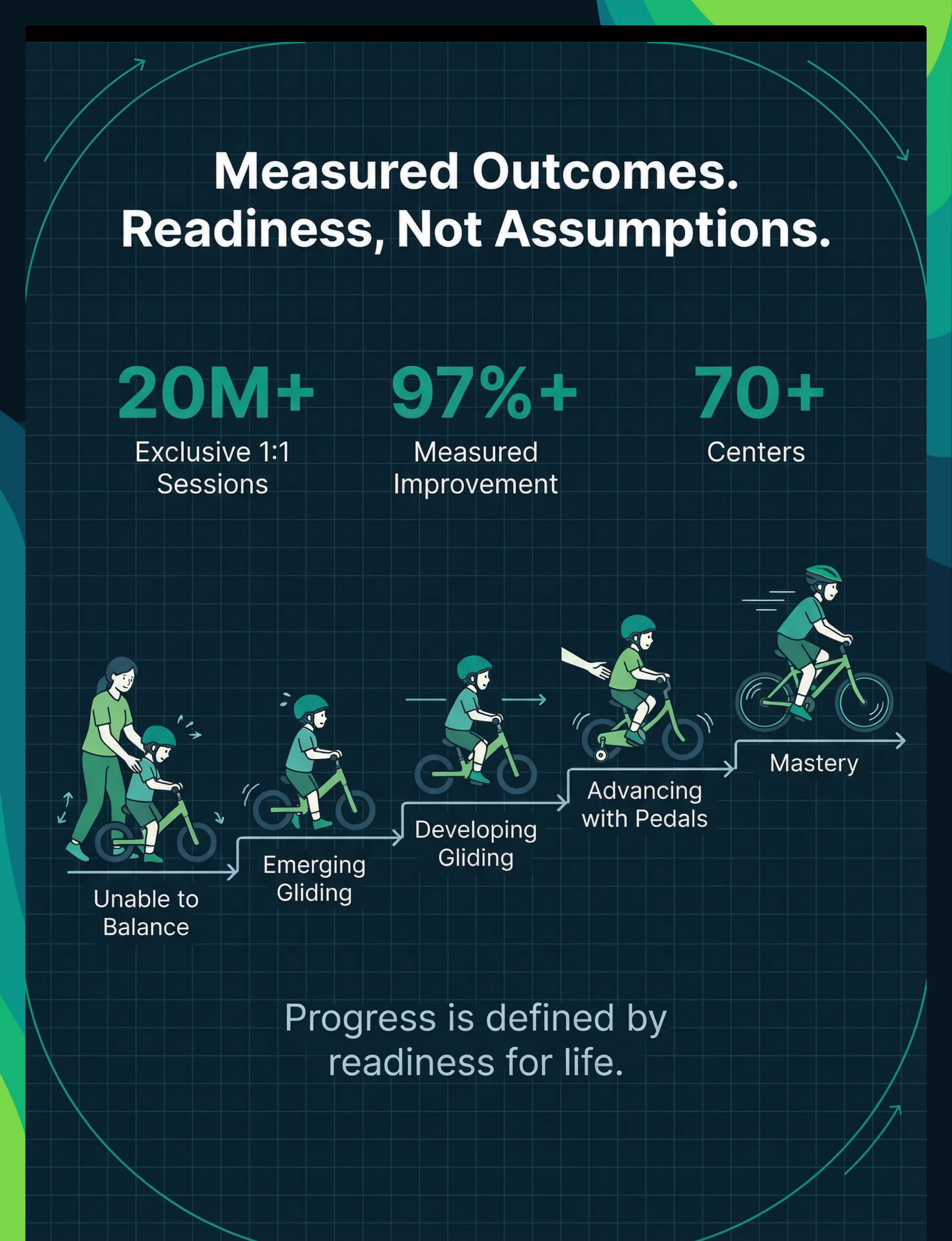
20M+
Exclusive 1:1 Sessions
Clinical evidence powering GPT-OS® recommendations
97%+
Measured Improvement
Across families implementing structured Pinnacle protocols
70+
Centers Across India
Physical, teleconsultation, and community support
☎FREE National Autism Helpline: 9100 181 181 | 16 Languages | 24×7 | pinnacleblooms.org
Preview of 9 materials that help with bike riding Therapy Material
Below is a visual preview of 9 materials that help with bike riding therapy material. The pages shown help educators, therapists, and caregivers understand the structure and content of the resource before use. Materials should be used under appropriate professional guidance.










Link copied!

🌸 Pinnacle Blooms Network®
India's Largest Pediatric Therapy Consortium
"From fear to mastery. One technique at a time."
We exist to transform every home — in every city, in every village, in every country — into a proven, scientific, 24×7, personalized, multi-sensory, multi-disciplinary pediatric therapy environment. Powered by GPT-OS®. Built on 20 million sessions. Committed to every child.
Medical Disclaimer
This content is educational and informational. It does not replace individualized assessment and intervention from licensed physical therapists, occupational therapists, or developmental specialists. Motor coordination difficulties can stem from multiple underlying causes requiring professional evaluation. Always prioritize safety with appropriate protective gear and supervision. Individual readiness varies — never force skill progression. If your child has a known medical condition, consult your physician before beginning any physical activity program.
Consortium
🦾 OT • 🏃 PT • 🎯 ABA/BCBA • 📚 SpEd • 🧠 NeuroDev • 👶 Pediatrics | CRO | WHO/UNICEF Aligned
Statutory Identifiers
CIN: U74999TG2016PTC113063 DPIIT Startup India: DIPP8651 MSME: TS20F0009606 GSTIN: 36AAGCB9722P1Z2 Entity: Bharath Healthcare Laboratories Pvt. Ltd.
Loop Navigation
☎Helpline: 9100 181 181 FREE | 16 Languages | 24×7
© 2026 Pinnacle Blooms Network®, unit of Bharath Healthcare Laboratories Pvt. Ltd. All rights reserved. Technique code F-570. GPT-OS® is a registered trademark.