"Bedtime in our house is a warzone."
Every night. The screaming. The stalling. The child who is clearly exhausted but cannot — will not — sleep. You say the words 'time for bed' and something in your child switches. Forty minutes later you are still in the hallway, negotiating.
BEDTIME TRANSITION SUPPORT
9 Evidence-Based Materials
You are not failing as a parent. Your child's nervous system is speaking. There is a language it understands — and these 9 materials speak it.
🏛️Pinnacle Blooms Network® Consortium | OT · SLP · ABA/BCBA · SpEd · NeuroDev · Pediatrics
Validated across 20M+ therapy sessions · 70+ centers · 70+ countries
Validated across 20M+ therapy sessions · 70+ centers · 70+ countries
📞 FREE National Autism Helpline: 9100 181 181 | Available 24x7 in 16+ languages
This Is Not a Parenting Problem. It Is a Population-Level Challenge.
50–80%
Children with Autism
Experience significant sleep difficulties — a documented clinical challenge, not willful defiance.
25–40%
Neurotypical Children
Also struggle with sleep onset and bedtime transitions across all populations.
21M+
Therapy Sessions
Sleep and routine challenges rank among the top 3 referral reasons at Pinnacle centers worldwide.
"You are among millions of families navigating this exact challenge — and evidence-based tools exist that work."
India is home to an estimated 18 million children on the autism spectrum (WHO, 2023). Sleep disturbances are documented in over 70% of these children. You are not alone. You are among millions navigating the same night.
📞9100 181 181 | FREE | 24x7 | 16+ Languages

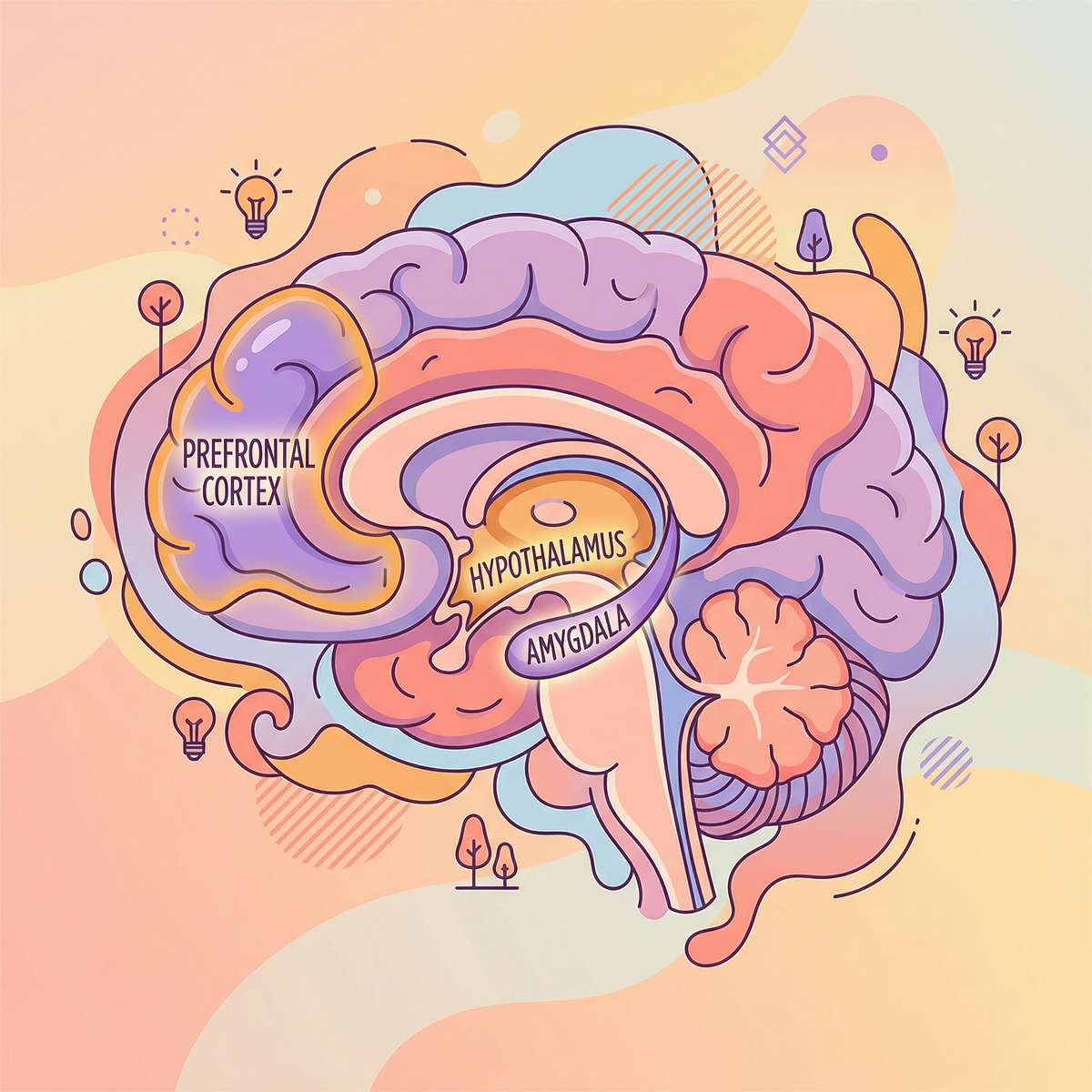
This Is Not Defiance. This Is Dysregulation. Here Is the Neuroscience.
What's Happening in the Brain
At bedtime, the brain must perform a complex physiological shift — from high arousal (active, alert, engaged) to low arousal (quiet, still, surrendering conscious control). For children with sensory processing differences, anxiety, ADHD, or autism, this shift is genuinely, neurologically difficult.
- Amygdala: Scans for threat. Darkness and silence can register as danger, triggering fight-or-flight precisely when the body needs rest.
- Reticular Activating System: Governs the brain's alertness dial. In many neurodivergent children, this dial is stuck at "high."
- Sensory Cortex: May be amplifying every input — the pajama seam, the distant dog bark, the light under the door.
- Prefrontal Cortex: Immature; cannot override arousal states without external support.
🧠"The child who screams at bedtime is not manipulating you. Their nervous system is in genuine distress. Understanding this changes everything about how we respond." — Pinnacle NeuroDev Consortium
This is a wiring difference, not a behavior choice. These 9 materials are calibrated to speak directly to the nervous system — bypassing the behavior and addressing the biology.

Your Child Is Not Behind. They Are on a Different Trajectory — With a Clear Forward Path.
0–12 Months
Typical: Sleep associations forming; multiple wakings normal.
Neurodevelopmental: Sensory sensitivities emerge; irregular sleep architecture begins.
Neurodevelopmental: Sensory sensitivities emerge; irregular sleep architecture begins.
1–3 Years
Typical: Separation anxiety peaks; resistance emerges; 11–14 hrs needed.
Neurodevelopmental: Transitions extremely difficult; routine dependency high.
Neurodevelopmental: Transitions extremely difficult; routine dependency high.
3–5 Years
Typical: Imagination and fear emerge; stalling behaviors common.
Neurodevelopmental: Anxiety amplified; sensory environment becomes critical.
Neurodevelopmental: Anxiety amplified; sensory environment becomes critical.
6–8 Years
Typical: Beginning self-regulation capacity; 9–12 hrs needed.
Neurodevelopmental: Sleep onset delays; racing thoughts; ADHD sleep impacts emerge.
Neurodevelopmental: Sleep onset delays; racing thoughts; ADHD sleep impacts emerge.
9–12 Years
Typical: Growing independence; academic stress enters the picture.
Neurodevelopmental: Circadian shifts may begin; anxiety peaks; screen exposure adds complexity.
Neurodevelopmental: Circadian shifts may begin; anxiety peaks; screen exposure adds complexity.
Co-occurring Conditions: Sensory Processing Disorder · Autism Spectrum · ADHD · Separation Anxiety · Generalized Anxiety · Night Terrors · Circadian Rhythm Differences

Not Opinion. Not Trend. Peer-Reviewed Evidence for What Works.
LEVEL I — SYSTEMATIC REVIEW + RCT EVIDENCE
Behavioral sleep interventions, sensory-based approaches, and environmental modifications for pediatric bedtime difficulties are supported by multiple systematic reviews and randomized controlled trials.
Study | Key Finding | Level | |
Systematic Review, Children 2024 — PMC11506176 | Sensory integration intervention meets evidence-based practice criteria across 16 studies (2013–2023) for children with ASD | Level I | |
Meta-analysis, World J Clin Cases 2024 — PMC10955541 | SI therapy effectively promotes adaptive behavior and self-regulation across 24 studies | Level I | |
WHO/UNICEF CCD Package 2023 — PMC9978394 | Caregiver-implemented home interventions demonstrate measurable outcomes across 54 countries | Level II | |
Padmanabha et al., Indian RCT 2019 | Home-based sensory interventions in Indian pediatric population: significant outcomes | Level II | |
NCAEP Evidence-Based Practices Report 2020 | Visual schedules, structured routines, parent training: evidence-based practices for autism | Level I |
"Clinically validated. Home-applicable. Parent-proven. The materials on this page are not suggestions — they are precision tools backed by global research."
BEDTIME TRANSITION SUPPORT
Parent Alias: "Making bedtime work — finally"
Formal Definition
Bedtime Transition Support refers to the structured, multi-modal application of environmental, sensory, visual, and behavioral tools to facilitate a child's neurological and psychological shift from waking activity to restful sleep. It is an evidence-based intervention domain spanning Occupational Therapy, Applied Behavior Analysis, Child Psychology, and NeuroDevelopmental Pediatrics — designed for home delivery by trained caregivers.
In Plain Terms
Bedtime is hard because your child's brain and body need specific inputs to downshift. These 9 materials provide those inputs — turning the transition from chaos to calm, one consistent night at a time.
Specification Badges
Age Range
2–12 years
Duration
20–60 min/night
Frequency
Every night — consistency is critical
Setting
Home / Bedroom
Canon Materials
📦 Visual Schedules · Weighted Items · Sound Tools · Light Regulation · Time Visualization · Sensory Calm-Down · Social Narratives · Comfort Objects · Relaxation Tools
🎬 See the original Reel: I-792 — 9 Materials That Help With Bedtime Transition | Domain I — Sleep & Daily Living | Episode 792 of 999

Five Disciplines. One Converged System. All Working for the Same Child.
Occupational Therapy (OT)
Assesses sensory processing profile; selects weighted, textural, and proprioceptive tools; designs the sensory environment; leads weighted blanket protocols.
Applied Behavior Analysis (ABA/BCBA)
Designs the visual schedule architecture; establishes reinforcement protocols for routine compliance; shapes behavior using antecedent modification and positive reinforcement.
Speech-Language Pathology (SLP)
Creates Social Narratives and personalized bedtime stories; develops communication supports for pre-sleep anxiety expression; scripts parent language for transitions.
Special Education (SpEd)
Transfers routine structure across home and school environments; trains teaching assistants on consistency protocols.
NeuroDevelopmental Pediatrics
Rules out medical contributors (sleep apnea, circadian disorders); guides melatonin consultation; monitors developmental trajectory.
"This technique crosses therapy boundaries because the brain doesn't organize by therapy type. The same child who needs OT for sensory regulation needs ABA for routine structure needs SLP for anxiety communication — all at bedtime, every night." — Pinnacle Blooms Consortium

This Is a Precision Intervention Targeting Specific Neural and Behavioral Outcomes.
Primary Targets
- Reducing time to fall asleep (sleep onset latency)
- Reducing bedtime resistance behaviors
- Establishing a predictable, consistent bedtime routine
- Building the child's capacity to self-soothe for sleep
Secondary & Tertiary Outcomes
- Improved daytime attention and impulse control
- Reduced anxiety through predictability
- Stronger immune function (sleep is the primary immune restoration window)
- School performance and memory consolidation
- Family wellbeing and parental mental health
9 Materials. 9 Mechanisms. One Complete Bedtime System.
MATERIALS 1–5

Material 01 — Visual Bedtime Routine Charts
📋Canon Category: Visual Schedules / Routine Boards
Why It Works: Transforms the abstract concept of "bedtime" into a concrete, predictable visual sequence. The chart becomes the authority — not the parent — dramatically reducing power struggles.
Price: ₹300–1,500
Why It Works: Transforms the abstract concept of "bedtime" into a concrete, predictable visual sequence. The chart becomes the authority — not the parent — dramatically reducing power struggles.
Price: ₹300–1,500

Material 02 — Weighted Blankets & Compression Items
🛏️Canon Category: Weighted / Deep Pressure Items
Why It Works: Deep pressure input activates the proprioceptive system and triggers the parasympathetic nervous system — the neurological "rest and digest" state. 10% of child's body weight is the evidence-based guideline.
Price: ₹2,000–6,000
Why It Works: Deep pressure input activates the proprioceptive system and triggers the parasympathetic nervous system — the neurological "rest and digest" state. 10% of child's body weight is the evidence-based guideline.
Price: ₹2,000–6,000

Material 03 — Nightlights & Light Control Systems
💡Canon Category: Environmental Regulation / Light Tools
Why It Works: Red/amber spectrum light minimally suppresses melatonin production. Correct lighting eliminates fear of darkness while supporting sleep chemistry.
Price: ₹300–2,500
Why It Works: Red/amber spectrum light minimally suppresses melatonin production. Correct lighting eliminates fear of darkness while supporting sleep chemistry.
Price: ₹300–2,500

Material 04 — White Noise Machines & Sound Systems
🔊Canon Category: Auditory Regulation / Sound Masking
Why It Works: Consistent sound provides "auditory cover" — the brain stops scanning for novel threats and can disengage the vigilance system that prevents sleep.
Price: ₹800–3,500
Why It Works: Consistent sound provides "auditory cover" — the brain stops scanning for novel threats and can disengage the vigilance system that prevents sleep.
Price: ₹800–3,500

Material 05 — Visual Timers & Time-to-Sleep Clocks
⏱️Canon Category: Time Visualization / Routine Cueing
Why It Works: Makes the invisible concept of time concrete and visual. Time-to-sleep clocks become non-negotiable authority ("the clock isn't showing morning yet") — removing the parent from the enforcement role.
Price: ₹1,500–4,000
Why It Works: Makes the invisible concept of time concrete and visual. Time-to-sleep clocks become non-negotiable authority ("the clock isn't showing morning yet") — removing the parent from the enforcement role.
Price: ₹1,500–4,000
9 Materials — Complete System
MATERIALS 6–9

Material 06 — Calm-Down Kits & Sensory Boxes
🧘Canon Category: Sensory Regulation / Self-Soothing Toolkits
Why It Works: Bridges the physiological gap between active wakefulness and sleep readiness. Gives the child something constructive to DO with their body and mind during the transition.
Price: ₹500–2,000
Why It Works: Bridges the physiological gap between active wakefulness and sleep readiness. Gives the child something constructive to DO with their body and mind during the transition.
Price: ₹500–2,000

Material 07 — Bedtime Stories & Social Narratives
📚Canon Category: Social Narratives / Language Tools
Why It Works: Stories normalize the bedtime experience, address specific fears, build positive associations with sleep, and provide the connection the child needs before separation.
Price: ₹200–1,500 (or DIY free)
Why It Works: Stories normalize the bedtime experience, address specific fears, build positive associations with sleep, and provide the connection the child needs before separation.
Price: ₹200–1,500 (or DIY free)

Material 08 — Comfort Objects & Transitional Items
🧸Canon Category: Transition Objects / Comfort Items | Pinnacle Canon SKU: Product #118 | ₹425 | ✅ Active
Why It Works: Donald Winnicott's transitional object theory: the comfort object represents the caregiver's presence, allowing the child to self-soothe through the separation that sleep requires.
Price: ₹425–2,500 | View on Amazon.in
Why It Works: Donald Winnicott's transitional object theory: the comfort object represents the caregiver's presence, allowing the child to self-soothe through the separation that sleep requires.
Price: ₹425–2,500 | View on Amazon.in

Material 09 — Relaxation Scripts & Guided Meditation
🎧Canon Category: Relaxation / Mind-Calming Tools
Why It Works: Provides the mind with structured content to follow, interrupting the racing-thought cycle. Progressive muscle relaxation activates the parasympathetic nervous system directly.
Price: ₹0–2,000 (apps + audio) | Headspace Kids · Calm Kids · Moshi Sleep App
Why It Works: Provides the mind with structured content to follow, interrupting the racing-thought cycle. Progressive muscle relaxation activates the parasympathetic nervous system directly.
Price: ₹0–2,000 (apps + audio) | Headspace Kids · Calm Kids · Moshi Sleep App
🏆Reinforcement Menus — Product #803 | ₹589 | For rewarding bedtime routine compliance | View on Amazon.in
Every Material Has a Zero-Cost Version. Geography and Budget Are Not Barriers to Therapy.
WHO/UNICEF Equity Principle in Action.
Material | Clinical Version | DIY / Household Alternative | |
Visual Schedule | Velcro schedule board ₹300–1,500 | Printed A4 photos laminated, stuck with tape — photos of YOUR child are actually more powerful | |
Weighted Blanket | Commercial weighted blanket ₹2,000–6,000 | Extra quilt layers + small sand-filled pouches sewn in; or simply layer 2 thick blankets (monitor at 10% body weight) | |
Nightlight | Red-spectrum LED nightlight ₹300–2,500 | Torch with red cellophane; salt lamp; string fairy lights on lowest setting — red spectrum preserved | |
White Noise Machine | Dedicated device ₹800–3,500 | Free apps: myNoise, Insight Timer, YouTube white noise on airplane mode; fan in another room | |
Visual Timer | Time Timer or Sand Timer ₹1,500–4,000 | Sand in a plastic bottle (DIY sand timer); drawing shrinking countdown on paper | |
Calm-Down Kit | Commercial sensory kit ₹500–2,000 | Smooth garden stones · fabric scraps · DIY glitter jar (jar + water + glitter glue) · pinwheels ₹20 | |
Bedtime Stories | Published books ₹200–1,500 | Printed social narrative you write about YOUR child's bedtime (free); record yourself reading on phone | |
Comfort Object | Weighted stuffed animal ₹500–2,500 | Child's own chosen toy; a piece of parent's worn clothing; smooth stone — the attachment is to the specific object | |
Relaxation Scripts | Apps ₹0–2,000 | Parent reads a simple body-scan script: "Notice your toes... let them go heavy..." — parent voice has added attachment benefit |
💛Complete Zero-Cost Bedtime Transition Kit: Printed photo schedule ✓ · Free white noise app ✓ · Child's own comfort toy ✓ · Extra layers for deep pressure ✓ · Parent-read relaxation script ✓ · DIY glitter calm jar (jar + water + glitter glue = ₹50) ✓
Total investment: ₹0–100. Total clinical equivalence: Complete.
Total investment: ₹0–100. Total clinical equivalence: Complete.

Read This Before Every Session. Safety Is Not Optional.
🔴 RED — Absolute Contraindications
- Weighted blankets on any child under 2 years, or any child who cannot independently remove the blanket
- Weighted blankets on children with respiratory, cardiac, or circulatory conditions without physician clearance
- Any technique when the child is acutely unwell, feverish, in active meltdown/crisis, or severely distressed
- Sound machines above 65dB — risk of hearing damage; always use "conversation level" as maximum
- Any unsupervised sensory item with infants or children with swallowing/mouthing concerns
🟡 AMBER — Modify With Caution
- Child had a particularly difficult day, trauma trigger, or unusual anxiety event → simplify routine
- First introduction of any new material → present during daytime calm first; never introduce at bedtime crisis
- Child demonstrates increased distress with a specific material → that material is not right; do not force
- Different caregiver implementing for first time → walk through visual schedule together before bedtime begins
🟢 GREEN — Proceed With Confidence
- Child is fed (not hungry), not overtired, in regulated state
- Routine materials are laid out before child arrives at bedroom
- Both/all caregivers present tonight have been briefed on the routine
- You have reviewed tonight's visual schedule and it reflects tonight's actual plan
🛑STOP IMMEDIATELY IF: Child shows breathing difficulty under weighted item · Severe escalation with genuine safety risk · Signs of genuine fear or trauma response · Any allergic reaction to new material
📞 Pinnacle Free Helpline: 9100 181 181 | Available 24x7 | Clinical guidance available
📞 Pinnacle Free Helpline: 9100 181 181 | Available 24x7 | Clinical guidance available

Spatial Precision Prevents 80% of Session Failures. Set Up Before the Child Arrives.
 a {
font-size: 0.75rem !important;
font-weight: 600 !important;
text-transform: uppercase !important;
letter-spacing: 0.05em !important;
color: #3a2a4d !important;
margin-bottom: 1rem !important;
}
/* Logo Section */
.pb-footer-logo-brand {
font-size: 1.25rem;
font-weight: 600;
color: var(--primary);
margin-bottom: 0.25rem;
}
.pb-footer-logo-tagline {
font-size: 0.75rem;
color: var(--muted-foreground);
}
.pb-footer-about {
font-size: 0.875rem;
color: var(--muted-foreground);
line-height: 1.65;
margin-bottom: 1.75rem;
max-width: 420px;
}
/* Links */
.pb-footer-link,.cm-f-l-block div:last-child ul li a {
display: block;
font-size: 0.875rem !important;
color: #5b2aad !important;
text-decoration: none;
padding: 0.25rem 0 !important;
transition: color 0.2s ease !important;
}
.pb-footer-link:hover,.cm-f-l-block div:last-child ul li a:hover {
color: var(--primary-dark);
text-decoration: underline;
}
/* Materials Grid */
.pb-materials-grid {
display: grid;
grid-template-columns: 1fr;
gap: 0 1.5rem;
}
/* Contact */
.pb-contact-item {
display: flex;
align-items: center;
gap: 0.5rem;
font-size: 0.875rem;
color: #3a2a4d;
text-decoration: none;
margin-bottom: 0.75rem;
}
.pb-contact-item:hover {
color: var(--primary);
}
.pb-contact-item svg {
width: 16px;
height: 16px;
}
.pb-contact-phone svg {
color: var(--phone);
}
.pb-contact-email svg {
color: var(--primary);
}
/* Social Icons */
.pb-social-links {
display: flex;
gap: 0.75rem;
margin-top: 1.5rem;
}
.pb-social-link {
width: 40px;
height: 40px;
border-radius: 12px;
display: flex;
align-items: center;
justify-content: center;
background: var(--muted);
color: var(--muted-foreground);
transition: all 0.2s ease;
}
.pb-social-link:hover {
background: var(--primary-light);
}
.pb-social-link svg {
width: 20px;
height: 20px;
}
.pb-social-linkedin:hover {
color: #0A66C2;
}
.pb-social-youtube:hover {
color: #FF0000;
}
.pb-social-instagram:hover {
color: #E4405F;
}
/* Corporate Bar */
.pb-footer-corporate {
border-top: 1px solid var(--border);
background: #faf9fc;
padding: 1rem 0;
}
.pb-corporate-inner {
display: flex;
flex-direction: column;
gap: 0.75rem;
align-items: center;
font-size: 0.75rem;
color: var(--muted-foreground);
}
.pb-corporate-name {
font-weight: 500;
}
.pb-corporate-ids {
display: flex;
flex-wrap: wrap;
justify-content: center;
gap: 0.25rem 1rem;
}
/* Disclaimer */
.pb-footer-disclaimer {
border-top: 1px solid var(--border);
background: #faf7fd;
padding: 1.25rem 0;
}
.pb-disclaimer-text {
font-size: 0.6875rem;
line-height: 1.6;
color: var(--muted-foreground);
text-align: center;
max-width: 900px;
margin: 0 auto;
}
.pb-disclaimer-text strong {
color: #3a2a4d;
}
/* Tablet */
@media (min-width: 640px) {
.pb-materials-grid {
grid-template-columns: repeat(2, 1fr);
}
.pb-corporate-inner {
flex-direction: row;
justify-content: space-between;
}
}
/* Desktop */
@media (min-width: 1024px) {
.pb-footer-main {
padding: 4rem 0;
}
.pb-footer-grid {
grid-template-columns: 1fr 2fr 1fr;
gap: 3rem;
}
}
.card-wrapper.card-collapsed .chakra-stack {
display: none;
}
a {
font-size: 0.75rem !important;
font-weight: 600 !important;
text-transform: uppercase !important;
letter-spacing: 0.05em !important;
color: #3a2a4d !important;
margin-bottom: 1rem !important;
}
/* Logo Section */
.pb-footer-logo-brand {
font-size: 1.25rem;
font-weight: 600;
color: var(--primary);
margin-bottom: 0.25rem;
}
.pb-footer-logo-tagline {
font-size: 0.75rem;
color: var(--muted-foreground);
}
.pb-footer-about {
font-size: 0.875rem;
color: var(--muted-foreground);
line-height: 1.65;
margin-bottom: 1.75rem;
max-width: 420px;
}
/* Links */
.pb-footer-link,.cm-f-l-block div:last-child ul li a {
display: block;
font-size: 0.875rem !important;
color: #5b2aad !important;
text-decoration: none;
padding: 0.25rem 0 !important;
transition: color 0.2s ease !important;
}
.pb-footer-link:hover,.cm-f-l-block div:last-child ul li a:hover {
color: var(--primary-dark);
text-decoration: underline;
}
/* Materials Grid */
.pb-materials-grid {
display: grid;
grid-template-columns: 1fr;
gap: 0 1.5rem;
}
/* Contact */
.pb-contact-item {
display: flex;
align-items: center;
gap: 0.5rem;
font-size: 0.875rem;
color: #3a2a4d;
text-decoration: none;
margin-bottom: 0.75rem;
}
.pb-contact-item:hover {
color: var(--primary);
}
.pb-contact-item svg {
width: 16px;
height: 16px;
}
.pb-contact-phone svg {
color: var(--phone);
}
.pb-contact-email svg {
color: var(--primary);
}
/* Social Icons */
.pb-social-links {
display: flex;
gap: 0.75rem;
margin-top: 1.5rem;
}
.pb-social-link {
width: 40px;
height: 40px;
border-radius: 12px;
display: flex;
align-items: center;
justify-content: center;
background: var(--muted);
color: var(--muted-foreground);
transition: all 0.2s ease;
}
.pb-social-link:hover {
background: var(--primary-light);
}
.pb-social-link svg {
width: 20px;
height: 20px;
}
.pb-social-linkedin:hover {
color: #0A66C2;
}
.pb-social-youtube:hover {
color: #FF0000;
}
.pb-social-instagram:hover {
color: #E4405F;
}
/* Corporate Bar */
.pb-footer-corporate {
border-top: 1px solid var(--border);
background: #faf9fc;
padding: 1rem 0;
}
.pb-corporate-inner {
display: flex;
flex-direction: column;
gap: 0.75rem;
align-items: center;
font-size: 0.75rem;
color: var(--muted-foreground);
}
.pb-corporate-name {
font-weight: 500;
}
.pb-corporate-ids {
display: flex;
flex-wrap: wrap;
justify-content: center;
gap: 0.25rem 1rem;
}
/* Disclaimer */
.pb-footer-disclaimer {
border-top: 1px solid var(--border);
background: #faf7fd;
padding: 1.25rem 0;
}
.pb-disclaimer-text {
font-size: 0.6875rem;
line-height: 1.6;
color: var(--muted-foreground);
text-align: center;
max-width: 900px;
margin: 0 auto;
}
.pb-disclaimer-text strong {
color: #3a2a4d;
}
/* Tablet */
@media (min-width: 640px) {
.pb-materials-grid {
grid-template-columns: repeat(2, 1fr);
}
.pb-corporate-inner {
flex-direction: row;
justify-content: space-between;
}
}
/* Desktop */
@media (min-width: 1024px) {
.pb-footer-main {
padding: 4rem 0;
}
.pb-footer-grid {
grid-template-columns: 1fr 2fr 1fr;
gap: 3rem;
}
}
.card-wrapper.card-collapsed .chakra-stack {
display: none;
}