
School Gets the Performance. Home Gets the Collapse.
It's not defiance. It's depletion. And it happens in millions of homes — every single afternoon. Here are 9 science-backed materials that help.
🧠 After-School Restraint Collapse
Domain: REG-ASE
Episode H-709

"He walked through the door, dropped his bag, and that was it. The meltdown that followed lasted two hours. His teacher had sent a message that morning saying he'd had 'a wonderful day.' I stopped telling people about the afternoons. No one believed me anyway."— Real parent, Pinnacle Network
You are not failing. Your child's nervous system is speaking. And now — finally — someone is listening. After-School Restraint Collapse (ASRC) is a real, documented neurological phenomenon — not a parenting failure, not a discipline problem, and not something your child is choosing.
🌸 Pinnacle Blooms Consortium
India's largest pediatric therapy network
✅ Validated Clinical Content
Evidence Grade Level I–II
📊 20M+ Sessions
97%+ measured improvement

You Are Among Millions.
The silence around After-School Restraint Collapse isn't because it's rare. It's because parents don't have the words for it. You do now.
80%
Sensory Differences
of autistic children show significant sensory processing differences (PMC11506176)
1 in 36
Neurodivergent
children in the world are neurodivergent in some form (WHO/CDC 2023)
70%+
ADHD Depletion
of children with ADHD show executive function depletion after school
📊India: 1 in 66 children diagnosed on the autism spectrum. Estimated 10–12 million children with neurodevelopmental conditions. After-school restraint collapse affects the majority of these families — every weekday. You are among an estimated 8–10 million Indian families navigating after-school dysregulation right now. This afternoon. On a school day like today.

This Is Not a Behaviour Problem. It's a Biology Problem.
Every child has a finite capacity to regulate their behaviour, emotions, sensory input, and impulses each day. At school, this battery depletes through managing classroom noise and crowds, suppressing natural movement and stimming, reading social cues constantly, following hundreds of explicit and unspoken rules, and masking — performing as neurotypical.
By 3pm, many neurodivergent children are running on empty.
"The school version is the performance. The home version is the truth. Both are real. Only one costs everything." — Pinnacle Blooms OT Consortium
The Safe Space Paradox
The collapse happens at home specifically because your child feels safe. The prefrontal cortex releases its vigilance. The accumulated stress floods out.
This isn't misbehaviour. This is the autonomic nervous system finally releasing what it has been containing for 7 hours.
Clinical Term
After-School Restraint Collapse (ASRC) — Post-School Dysregulation. First described in occupational therapy literature. Now validated across autism, ADHD, anxiety, and sensory processing research.

This Challenge Has a Developmental Window. It Also Has a Way Forward.
Ages 3–5
Pre-school regulation foundations forming
Ages 5–9 ⭐
Peak ASRC window begins. Maximum school demand meets developing, incomplete regulation capacity.
Ages 10–12 ⭐
Gap widest here. Demands exceed capacity for many neurodivergent children. Prime intervention window.
Ages 13–16
With consistent support, capacity builds. ASRC can reduce significantly.
Emerging Independence
Long-term self-regulation architecture fully in place.
Children's self-regulation capacity develops gradually into the mid-20s — prefrontal cortex maturation is a long process. ASRC is often more severe in children with Autism Spectrum Condition, ADHD, Sensory Processing Differences, Anxiety Disorders, and Learning Differences. The gap between demands and capacity is widest in ages 6–12. With consistent support, capacity builds faster than it depletes.

After-School Decompression Protocol
Parent-Friendly Alias: "The Arrival Reset Routine"
The After-School Decompression Protocol is a structured, evidence-based set of environmental, sensory, and nutritional supports designed to help neurodivergent children recover from the regulatory depletion caused by the school day. It transforms the dangerous transition window (3pm–6pm) from a meltdown flashpoint into a supported recovery period.
🧠 Self-Regulation
👁️ Sensory Processing
🏠 Daily Living
⏱️ Transition Support
4–16
Age Range
years
30 min
Setup Time
one-time setup
90 min
Daily Duration
30–90 min/day
Daily
Frequency
Every school day
Domain H — Daily Living & Self-Regulation | Code: REG-ASE | Episode: 709 | Theme: 9MAT | Series Position: H-709. Rather than a single technique, this protocol is a system of 9 materials working together — each targeting a different dimension of post-school dysregulation: sensory, auditory, spatial, nutritional, temporal, tactile, occupational, visual, and physical.

9 Materials. 9 Dimensions of Recovery. One Protocol That Works.
Autonomic Reset
Weighted Blanket / Lap Pad — reduced heart rate, calmer body within 20–30 min
Auditory Relief
Noise-Canceling Headphones — less flinching, reduced ear-covering at home
Blood Sugar
High-Protein Snack Station — fewer hunger-linked meltdowns in first 30 minutes
Temporal Anxiety
Visual Timer — fewer "what's next?" questions, smoother transitions
Sensory Discharge
Fidget Kit — hands engaged, body calmer, less destructive stimming
Cognitive Relief
Low-Demand Activity Box — child engages without prompting or facilitation
Predictability
Transition Visual Schedule — child references schedule independently
Proprioceptive Discharge
Movement Outlet / Crash Space — decreased explosive outbursts
Spatial Safety
Sensory Retreat Space / Calm Corner — child self-initiates within 5 minutes of arrival
📞 Not sure where to start? Call 9100 181 181 — Our therapists will guide your personalised toolkit selection.
Your After-School Recovery Toolkit
9 Materials. All Evidence-Based. All Home-Applicable.

🛏️ Weighted Blanket / Lap Pad
₹2,000–8,000 | DIY: ₹0

🎧 Noise-Canceling Headphones
₹1,500–15,000 | DIY: ₹300–800

🏕️ Calm Corner / Sensory Retreat
₹2,000–10,000 | DIY: ₹0
🥗 High-Protein Snack Station
₹100–500/week
⏱️ Visual Timer & Transition Support
₹500–2,500

🎮 Fidget Kit & Sensory Tools
₹500–2,500

📦 Low-Demand Activity Box
₹500–2,000
📋 Transition Visual Schedule
₹200–800

🏃 Movement Outlet / Crash Space
₹1,500–15,000
💡Essential Starter Kit (under ₹5,000): Lap pad + Ear-muff headphones + Blanket fort corner + Consistent snack + Phone visual timer. DIY alternatives available for every item (₹0 option).

Material 1 of 9
Sensory Regulation
Weighted Blanket or Lap Pad
"Deep pressure calms the overloaded nervous system. Weight isn't restraint — it's the physical message: You're safe now."
Price Range: ₹2,000–8,000 | DIY Option: ₹0 (rice bags, multiple blankets)
The Science
Deep pressure input is one of the most reliable activators of the parasympathetic nervous system — the 'rest and digest' state that counters the fight-or-flight response of a stressful school day. Proprioceptive input from weight signals safety directly to the brainstem, bypassing the cortex. This is why children who are too dysregulated to hear words will still calm under a weighted blanket — the message arrives at the level of the nervous system, not the mind.
Ideal weight: approximately 10% of child's body weight. Lap pad (1–2 kg): Car rides, desk use, immediate transition. Full blanket (2–7 kg): Extended decompression periods.
What, Why, Where, When
WHAT: A blanket or pad filled with weighted material (glass beads, poly pellets) applying gentle, sustained deep pressure across the body.
WHY: Activates deep pressure touch receptors → triggers parasympathetic activation → lowers arousal → supports return to regulated state.
WHERE: In the car during the ride home. At the front door on arrival. In the calm corner. During any low-demand recovery activity.
WHEN: Begin the moment the child enters the car. Continue through the first 30–60 minutes at home. Remove when child shows signs of regulation.
🔧DIY Protocol: Stack 2–3 regular blankets · Tight sleeping bag · Rice-filled fabric bags (10% body weight guide) · Bean bags layered across lap · Adult firm sustained pressure (bear hug). Safety: Never use during sleep (young children). Start with lighter weights. Child must be able to remove independently.
📞 Not sure which weight is right? Call 9100 181 181

Material 2 of 9
Sensory Regulation
Noise-Canceling Headphones
"Silence for overloaded auditory systems. Sound you don't have to process is energy you don't have to spend."
Price Range: ₹1,500–15,000 | DIY Option: ₹0–500 (ear-muff style from hardware store)
The Science
School environments are acoustically intense. For children with auditory sensitivity or central auditory processing differences, the school soundscape — bells, announcements, cafeteria noise, playground chaos — requires continuous active processing at high cognitive cost. By afternoon, the auditory cortex is fatigued. Normal home sounds (siblings, TV, kitchen noise) that would be tolerable in the morning become intolerable.
Noise-canceling headphones immediately reduce the incoming auditory load, allowing the auditory system to begin recovery. Active noise-canceling (ANC) eliminates unpredictable environmental sound. Child may then choose: complete silence, white noise, calming music, or nature sounds — whichever is most regulating for them.
How to Use
WHERE: In the car from school pickup. At home entry. Calm corner. Any environment where environmental noise is unavoidable.
HOW: Have charged in car or at front door — remove friction from access. Child puts on as soon as they enter car or home. Let child choose: silence, preferred music, nature sounds, or audiobook. Duration: as long as child chooses, typically 15–60 minutes.
WHEN: Begin immediately after school. Continue until child voluntarily removes. Do not require conversation while headphones are on — this defeats the purpose.
Types
- Over-ear ANC (best): Sony WH, JBL, Anker — full ambient sound reduction
- Ear-muff style (budget): Peltor, Howard Leight — passive isolation ₹300–800 at hardware stores
- Child-sized options: Important for comfort and effective seal
Safety: Monitor volume levels. Child should be able to hear emergency calls. Do not use while navigating traffic independently. 📞9100 181 181 | SLP team guidance on auditory regulation tools.

Material 3 of 9
Spatial Safety
Calm Corner / Sensory Retreat Space
"A dedicated space that signals: Here, you are safe. Here, you can let go."
Price Range: ₹2,000–10,000 | DIY Option: ₹0 (blanket fort, corner with cushions)
The Science
The nervous system reads environmental cues before the conscious mind does. A dedicated space — consistently associated with safety, low demand, and sensory comfort — begins triggering the parasympathetic response the moment the child enters or sees it. Over time, the spatial cue itself becomes a regulation tool. The retreat space targets both the autonomic nervous system reset and the spatial safety signal simultaneously.
The space should be small enough to feel enclosed and protective, with controllable sensory input: dimmable light or no overhead light, soft surfaces, access to weighted materials, and proximity to snack and activity options.
Setup Essentials
- Small, enclosed feel — corner, tent, or under a loft bed
- Soft flooring: cushions, bean bag, or foam mat
- Dimmable or fairy light option — not overhead bright light
- Weighted blanket/lap pad within reach
- Fidget kit or sensory items accessible
- Visual schedule posted nearby
- No screens required — but can include if regulating for child
- Child involved in setting it up on a calm day
🚨Critical rule: This space is NEVER withdrawn as a consequence. It is a recovery resource — unconditional access, every day.

Material 4 of 9
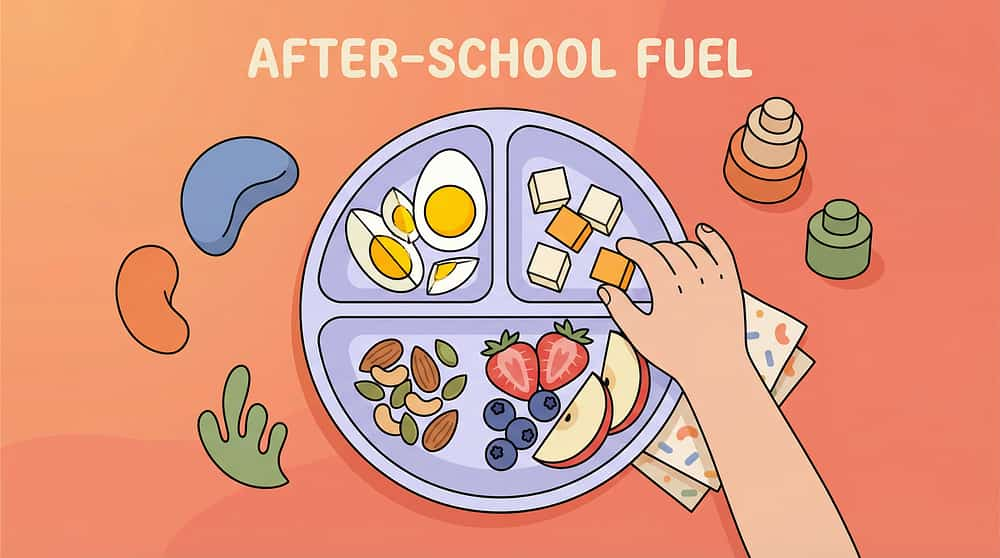
Nutritional Regulation
High-Protein Snack Station
"Blood sugar crashes amplify emotional dysregulation. The right snack, at the right time, is a regulation tool."
Price Range: ₹100–500/week | Available in every home — no special purchase required
The Science
The prefrontal cortex — already depleted from a day of regulatory effort — is exquisitely sensitive to blood glucose fluctuations. After 6–7 hours at school with limited or rushed eating, many children arrive home in a combined state of regulatory depletion AND blood sugar drop. This compounding effect dramatically amplifies meltdown likelihood in the first 30 minutes after arrival.
High-protein snacks stabilise blood glucose more sustainably than carbohydrates alone, supporting the regulatory recovery process. Consistency matters: the same snack, available without decision-making, removes another demand from a depleted system.
Protocol
WHAT: High-protein snack prepared and placed within reach before child arrives home. No announcement, no choices, no interaction required.
OPTIONS: Boiled eggs, cheese and crackers, nuts and seeds, peanut butter on toast, paneer cubes, chana chaat, yoghurt. Crunchy textures add proprioceptive oral input — additionally regulating.
WHAT NOT TO DO:
- Don't ask "are you hungry?" — just have it ready
- Don't introduce new snacks during the first 4 weeks
- Don't make snack contingent on behaviour
- Don't serve high-sugar options that spike and crash blood sugar

Material 5 of 9
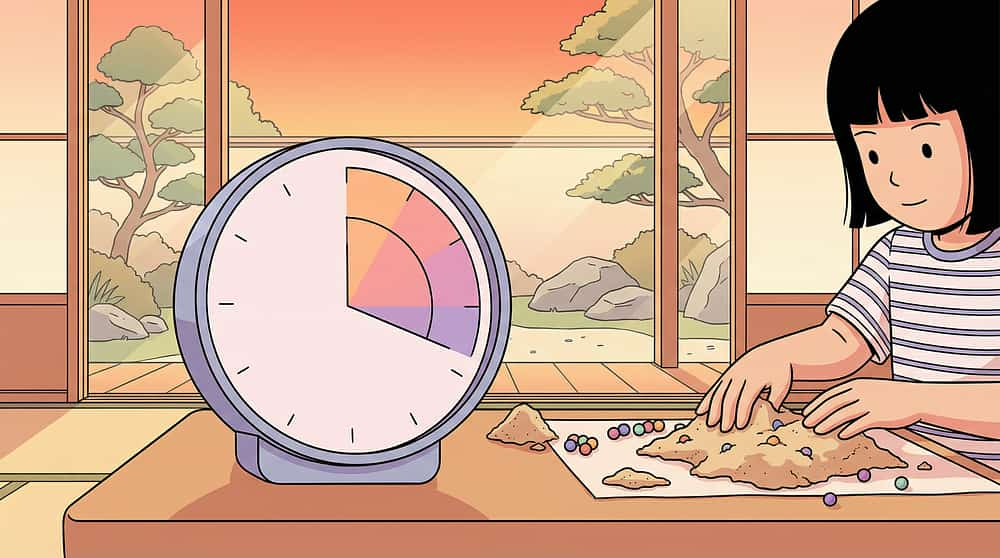
Temporal Regulation
Visual Timer & Transition Support
"Predictability is a regulation tool. When a child knows how long, the waiting itself becomes manageable."
Price Range: ₹500–2,500 | DIY: Free phone app timers with visual countdown
The Science
Temporal uncertainty — not knowing when a demand will arrive, how long recovery lasts, or what comes next — activates anticipatory anxiety in the prefrontal cortex and amygdala. For children with ASRC, this anxiety compounds the existing regulatory depletion. The visual timer solves this by making time visible and concrete rather than abstract.
By letting the timer govern transitions rather than parental announcements, you remove yourself as the source of demand. The child's conflict shifts from "parent versus me" to managing a known, visible countdown — which is far less dysregulating.
Recommended Durations
- Ages 4–6: 20–30 minutes protected time
- Ages 7–10: 30–45 minutes protected time
- Ages 11+: 45–90 minutes protected time
- Severe ASRC: Up to 90 minutes before any demand placement
Transition Warnings
- 5-minute warning: gentle alert, no demand language
- 2-minute warning: "Almost done — finishing up time"
- Timer ends: Reference visual schedule — child moves to next step

Material 6 of 9
Sensory Input Discharge
Fidget Kit & Sensory Tools
"Hands that are engaged are bodies that are calmer. Fidgets aren't distractions — they're regulation tools."
Price Range: ₹500–2,500 | DIY: Homemade sensory bags, dried beans, textured fabrics
The Science
The tactile and proprioceptive systems are two of the most reliable pathways to autonomic regulation. When a child handles fidget tools — squeezing, stretching, pressing, rolling — they receive continuous low-grade proprioceptive and tactile input that occupies the sensory-seeking part of their nervous system, freeing regulatory resources for calming.
During ASRC, many children engage in destructive or disruptive stimming because their nervous system is seeking the input it needs. A well-stocked fidget kit provides that input through appropriate channels — reducing property destruction and improving the quality of the recovery period.
Kit Components
- Squeeze balls of varying resistance levels
- Putty / theraputty / kinetic sand
- Textured surfaces and tactile boards
- Chew necklaces or chewable tools (for oral sensory seekers)
- Stretchy resistance bands
- Spiky massage balls or rolling pins
- Spinning or visual fidgets (for visual-vestibular regulation)
Allow stimming during recovery — this is the nervous system's own regulation mechanism. Do not redirect or discourage. Presence of appropriate fidget tools reduces destructive alternatives.

Material 7 of 9
Cognitive Demand Reduction
Low-Demand Activity Box
"Recovery requires zero cognitive effort. This box exists so the mind can rest while the hands stay gently occupied."
Price Range: ₹500–2,000 | DIY: Entirely DIY — assembled from items already in the home
The Science
After a day of maximum cognitive effort, the prefrontal cortex requires a period of low-demand engagement — not passive screen time (which maintains arousal) and not academic work (which demands the same depleted resources). Low-demand activities occupy the hands and eyes with familiar, non-evaluative tasks, maintaining gentle engagement without adding to cognitive load.
The key criterion: the activity should be completable without instruction, without evaluation, and without the possibility of failure. Familiarity is essential — introducing a new activity adds novelty-processing demand.
What Goes In the Box
- Colouring books (pre-selected, no blank-page pressure)
- Simple puzzles (familiar, completed before — no frustration)
- Building blocks or LEGO (free play, no instructions)
- Sticker books
- Preferred special interest materials (trains, dinosaurs, maps)
- Sand tray or kinetic sand container
- Familiar favourite small toys
Rotate contents every 2–3 weeks to maintain novelty while keeping individual items familiar. Child helps select contents on a calm day — this increases engagement during recovery.

Material 8 of 9
Predictability & Safety Signalling
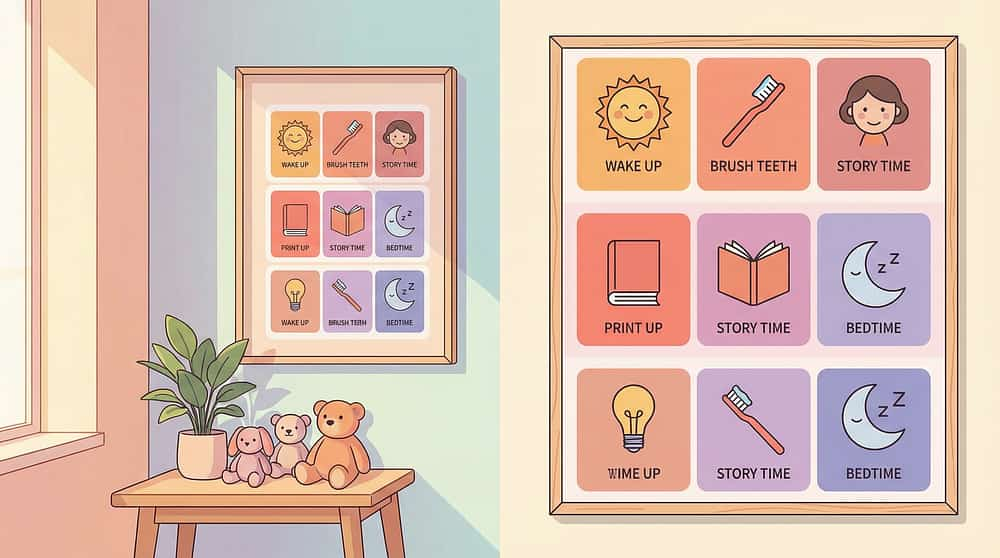
Transition Visual Schedule
"When the child knows what comes next, the nervous system stops bracing for the unknown."
Price Range: ₹200–800 | DIY: Free (printed pictures, drawn schedule, phone photo sequence)
The Science
Anticipatory anxiety — anxiety about what will happen next — is a significant driver of ASRC severity. For many neurodivergent children, transitions are not just logistically challenging; they are neurologically threatening because they represent unpredictability. The visual schedule converts the unpredictable into the predictable, providing a concrete, external map of the afternoon's sequence.
Unlike verbal reminders (which require the child to hold information in working memory — already depleted), a visual schedule externalises the sequence so working memory doesn't have to. The child can reference it independently, reducing the number of times they need to seek parental reassurance about "what happens next."
Setup
- Posted at child's eye height in or near the calm space
- Picture-based for younger/pre-literate children
- 5–7 steps maximum for the after-school period
- Sequence: Arrive home → Calm time → Snack → [Activity] → Dinner → Bath → Bed
- Use Velcro strips to let child physically move completed steps
- Introduce the schedule to child on a calm day — not mid-meltdown
Point to schedule once on arrival: "Look — this is what happens." No further explanation. The schedule does the communicating. Child references it independently within 7–14 days.
Material 9 of 9
Proprioceptive & Vestibular Discharge
Movement Outlet / Crash Space
"A body that has been still for 7 hours needs to move before it can be still again."
Price Range: ₹1,500–15,000 | DIY: ₹0 (outdoor yard, hallway jumping, sofa cushion crash pad)
The Science
Proprioceptive and vestibular input — from jumping, crashing, pushing, and heavy muscle work — are among the most powerful inputs for nervous system downregulation. After a school day spent suppressing natural movement, the motor system is in a state of sensory deprivation that drives explosive physical behaviour at home.
Providing a structured, sanctioned movement outlet allows this physical discharge to happen safely and purposefully, rather than through property destruction or aggressive behaviour. For explosive-presentation children, movement outlet before the weighted rest phase is not optional — it is step one.
Options by Budget
- Mini trampoline (₹2,500–8,000): Most effective for vestibular input
- Crash pad / foam pit corner (₹1,500–5,000): Safe crashing and falling
- Resistance bands and tunnels: Crawling and pushing activities
- Heavy work outdoors: Carrying bags of rice, pushing wheelbarrow — free
- Hallway running + crashing into cushion pile: ₹0
Protocol
15–20 minutes physical discharge → heavy proprioceptive work (carrying, pushing) → THEN weighted blanket + quiet sensory engagement → THEN snack. For shutdown children, movement is less essential; for explosive children, it is the mandatory first step.
Step 1 of 6: The Arrival Invitation
Not a Command. An Invitation.
ACT III: Step 1
For Shutdown Children
"Hey. Good to have you home. Your spot is ready." Say nothing else. Point to calm corner. Walk away.
For Explosive Children
"You can jump / crash / move. Your crash space is ready." Match their energy with calm. Nothing more.
For Children Who Can Receive It
"Rough day? Your corner has your blanket. Snack's ready whenever you want it."
What NOT to Say ❌
- "How was your day?"
- "Homework is due tomorrow."
- "Why are you acting like this?"
- "At school you were fine, so..."
- Anything that requires a verbal response
Body Language Guidance
- Calm, low-energy presence
- Don't stand in doorway blocking escape
- Match the child's arousal level — don't introduce new energy
- If child ignores you, that's fine. Follow silently.
Timing: 30–60 seconds. Less is more.
Step 2 of 6: The Sensory Engagement
Let the Materials Do the Work.
ACT III: Step 2
Child Response Indicators
Engagement: Child uses tools, body quiets, breathing normalises
Tolerance: Child accepts presence of tools without using them
Avoidance: Child refuses — respect it. Presence of tools still helps.
Parent Role During This Phase
"Your most therapeutic act in the next 30 minutes is doing nothing. No questions. No interaction unless initiated. Your calm presence is the most regulating input."
Timing: 5–15 minutes for initial sensory engagement phase
Step 3 of 6: Activate the Structure
Predictability Is a Regulation Tool.
ACT III: Step 3
Set the visual timer for the protected decompression period. Show child: "You have this much time. It's yours." Walk away. The timer governs transitions — not your announcements. This removes you as the source of demand.
Ages 4–6
20–30 minutes protected time
Ages 7–10
30–45 minutes protected time
Ages 11+
45–90 minutes protected time
Severe ASRC
Up to 90 minutes before any demand placement
Crash Space / Movement First Variation: If child is explosive rather than withdrawn → Movement outlet BEFORE weighted rest (15–20 mins physical discharge) → THEN weighted blanket + quiet sensory engagement → THEN snack. The timer runs. You wait. This is the protocol working.
Step 4 of 6: The Daily Repetition Principle
Consistency Builds the Neural Pathway. Daily Repetition Is the Intervention.
ACT III: Step 4
Unlike many therapeutic techniques where 10–15 minutes of the right activity drives change, ASRC recovery is about routine consistency. The materials alone don't build regulation. The predictable daily routine built around the materials does. When your child's nervous system learns the sequence, it begins to anticipate recovery — the arousal level actually starts decreasing in the car, before they even reach home.
Days 7–10
Child begins to expect the routine
Days 14–21
Child starts initiating parts of the routine independently
Weeks 4–6
Observable reduction in meltdown frequency and intensity
Weeks 8–12
Measurable progress on Self-Regulation Readiness Index
Variation within Consistency: The materials can vary slightly while the sequence stays constant. Same order. Same timing. Same non-demand arrival script. Different fidgets or different snacks — fine. Different sequence — disrupts the nervous system's learning. Dosage: Every weekday. Weekends not required.
Step 5 of 6: Reinforce & Celebrate
Celebrate the Attempt — Not Just the Success.
ACT III: Step 5
What to Reinforce ✅
- Child entered calm space without refusal
- Child accepted any tool (blanket, headphones, snack)
- Meltdown was shorter than usual
- Child self-initiated any part of routine
- Child emerged from decompression ready to engage
Reinforcement Scripts (deliver within 3 seconds)
"I noticed you went to your spot. That was a great choice."
"You used your blanket today — I saw that. Well done."
"That was a shorter hard time. You're getting better at this."
"You came to dinner tonight. I'm proud of you."
Reinforcement Menu
- Verbal praise (specific, warm, low-key)
- Physical affection (if child accepts)
- Preferred 5-minute activity with parent
- Token toward preferred reward
Avoid
- Food as primary reinforcer (disrupts nutritional regulation)
- Extravagant celebrations (overwhelming for depleted child)
- Reinforcing "recovery speed" — it varies legitimately
For Explosive Presentations
Even if meltdown occurred, reinforce the recovery: "You came back. That's the important part."

Step 6 of 6: The Transition Out
End Recovery Without Triggering a New Crisis.
ACT III: Step 6
The Problem with Hard Stops: If recovery time ends abruptly — a knock on the door, an announcement, a sibling interruption — the child's nervous system registers threat. The regulation achieved in 40 minutes can unravel in 40 seconds.
Timer Governs Transition
Child sees the countdown and internally prepares. No parent announcement needed. Calm, neutral: "Timer's done. Looks like [next visual on schedule] is up."
Graduated Demand Reintroduction
First demand post-recovery: low-demand (snack, preferred activity). Second demand: slightly higher. Full demand placement only after 10–15 minutes of graduated re-engagement.
If Child Can't Transition
Extend timer by 10 minutes without negotiation or consequence. If still severely dysregulated after 90 minutes: professional assessment needed. Do not force transition.
"After full recovery — the evening you both actually want. Homework gets done (eventually). Dinner happens. Connection is possible. This is the payoff of the protocol."

When the Protocol Isn't Working: Troubleshooting
Real Problems. Evidence-Based Solutions.
Child refuses the calm space entirely
Follow them — the protocol works wherever they land. Start with the most accepted tool (often snack or movement). Let child lead materials selection for 2 weeks. Redesign the space with the child on a calm day.
Meltdown starts in the car, not at home
Begin protocol in car: lap pad, headphones, water. Eliminate conversation on car ride entirely. Drive in silence or with child's preferred music. The car IS the transition — start recovery there.
Weighted blanket causes overheating or rejection
Try lap pad only, not full blanket. Reduce weight to 5% body weight. Try compression garment instead. Try deep pressure massage — same mechanism, less heat.
Child uses movement outlet and then can't calm
Movement type matters: jumping/crashing = calming. Spinning/running = can excite further. Follow movement with heavy proprioceptive work (carrying, pushing), then transition to weighted blanket and rest.
Protocol works some days but not others
Vary by day of week — Thursday/Friday often harder due to week fatigue. Check for school day events: assembly, PE, trip, social conflict. Adjust duration on hard days. Protocol is correct; dosage needs calibration.
Siblings disrupt the recovery routine
Brief sibling training: "This is [child]'s recovery time." Give siblings a parallel quiet activity — normalises the structure. Schedule sibling connection time AFTER recovery is complete.
My child's school doesn't believe ASRC is real
Use the school communication template (Card 37). Bring data from your daily tracker to the school meeting. Reference NCAEP 2020 + ASRC occupational therapy literature. Request 504/IEP accommodation for homework timing flexibility.

Weeks 1–2: You Are Building the Runway. The Flight Comes Later.
Progress: 15% — Initiation Phase
ACT IV: Progress Arc
Do NOT Expect (Weeks 1–2) ❌
- Dramatic reduction in meltdowns
- Child using all 9 tools enthusiastically
- Evening functioning fully restored
- School reports changing
What You WILL See ✅
- Child stops resisting the calm space after 3–5 days
- Recovery time may shorten by 5–10 minutes
- Child accepts 1–2 tools consistently
- At least one manageable evening per week
- You feel more empowered because you have a protocol
The Neural Pathway Reality
Weeks 1–2 is system establishment. The nervous system is learning: "After school → these materials → safety." This learning is happening even when you can't see it — even on the days it looks like nothing is working.
"If your child tolerates the calm space for 10 seconds longer than last week — that is real progress. Measure from the baseline, not from the ideal."
Struggling in weeks 1–2? 📞9100 181 181 — Free guidance session with a Pinnacle OT

Weeks 3–4: The Nervous System Is Learning. Watch for These Signs.
Progress: 40% — Consolidation Phase
🧠 Anticipatory Behaviour
Child begins to anticipate the routine before arriving home — asking "is my blanket ready?" from the car. The neural pathway is forming.
📉 Reduced Frequency
Meltdown frequency has reduced by 1–2 episodes per week on average. Recovery time shortening consistently — visible in your tracking data.
🎯 Tool Preference Emerging
Child shows preference for specific tools — personalisation is emerging. Synaptic connections are strengthening through repeated structured input.
✨ Self-Initiation
Child uses tools without being reminded at least once this week — the pattern is becoming automatic rather than effortful.
"You may notice you're calmer during the transition too. You now have a protocol. Uncertainty was the hardest part. You've reduced yours along with your child's."
What to Increase in Weeks 3–4: Begin very gentle demand placement after recovery time ends. Single low-demand request only (e.g., "shoes in the rack"). Extend this very gradually each week.

Weeks 5–8: This Is Where the Work Pays Off.
Progress: 70% — Functional Recovery Phase
50%
Recovery Time Reduction
From baseline, by week 8
60%
Meltdown Frequency Reduction
40–60% fewer meltdowns
4–6
Tools Used Independently
From the toolkit, without prompting
Week 5
Single low-demand request post-recovery
Week 6
Snack + brief homework (1 task only, timer-limited)
Week 7
Standard homework with structured support
Week 8
Near-normal evening routine with recovery time protected
If progress is slower than expected: AbilityScore® reassessment recommended | OT sensory profile update | School accommodation review | Medical: check for unaddressed anxiety or sleep disorders. 📞9100 181 181 for clinical pathway guidance.
Stop. Celebrate. Your Child's Nervous System Just Learned Something New.
🎉 Milestone Recognition
🎉 First self-initiated calm corner visit
🎉 First evening homework completed without major dysregulation
🎉 First meltdown under 10 minutes
🎉 First "I need my blanket" said independently
🎉 First full dinner at the table without incident
🎉 First school morning where the previous evening's recovery held
"You were told by well-meaning people that this was a phase, that you were overreacting, that all kids have rough afternoons. You knew it was more. You were right. And you did something about it. That matters." — Pinnacle Blooms Network® Consortium
The child who self-initiates decompression at age 8 is the adolescent who recognises their emotional state at 16 and takes proactive action. This is long-term self-regulation architecture.
When to Stop and Seek Professional Support.
These Are Not Normal Variations.
🔴 Seek Immediate Assessment
- After-school collapse involves self-harm (hitting, scratching, biting self)
- Collapse duration exceeding 3+ hours regularly
- Child unable to function at school AND at home
- Signs of suicidal ideation or statements about not wanting to exist
- Regression to much younger developmental stage (beyond temporary)
- Child is not sleeping — exhaustion compounding dysregulation
⚠️ Seek Non-Urgent Assessment
- Protocol followed consistently for 8 weeks with no measurable improvement
- Meltdown severity increasing despite protocol
- Physical symptoms after school (persistent headaches, stomach aches)
- Child explicitly expresses that school is unbearable
What Escalation Looks Like at Pinnacle
- Free helpline assessment — 9100 181 181
- AbilityScore® comprehensive assessment
- OT + ABA + NeuroDev evaluation
- School accommodation review
- FusionModule™ multi-disciplinary programme
This is not failure. If your child needs more than a home protocol, that means the need is bigger than a home protocol. Getting that assessment is the right next step. The protocol you've built still matters — it feeds the clinical data. 📞9100 181 181 (24×7 | 16+ languages)
Real Families. Real Recovery. Because Progress Looks Different in Every Home.
Parent Stories
ACT V: Community
Priya, 8, ASD Level 1 — Bangalore
"Every afternoon was a disaster. We set up the calm corner with her weighted blanket and noise headphones. Day 7, she walked in and went straight to her corner without being told. I cried. My husband said 'she's got this.' She does."
Arjun, ADHD — Chennai
"The weighted lap pad in the car was the single biggest change. The meltdowns used to start in the carpark. Now the carpark is where they start to end."
Family — Hyderabad
"We were spending ₹3,000 a week in broken things during meltdowns. The entire protocol cost us ₹4,500 to set up. Best investment of our life." — GPT-OS® EverydayTherapyProgramme™
Indian Family — London
"We're Indian, living in London. The helpline works here too. The bilingual support for my mother-in-law who doesn't speak English was something I didn't expect. They explained the protocol to her in Tamil."
Stories shared with permission. Names changed for privacy. Outcomes vary by child profile, environmental factors, and consistency.
The Science Behind This Protocol. For Parents Who Want the Deeper Reading.
Research Library
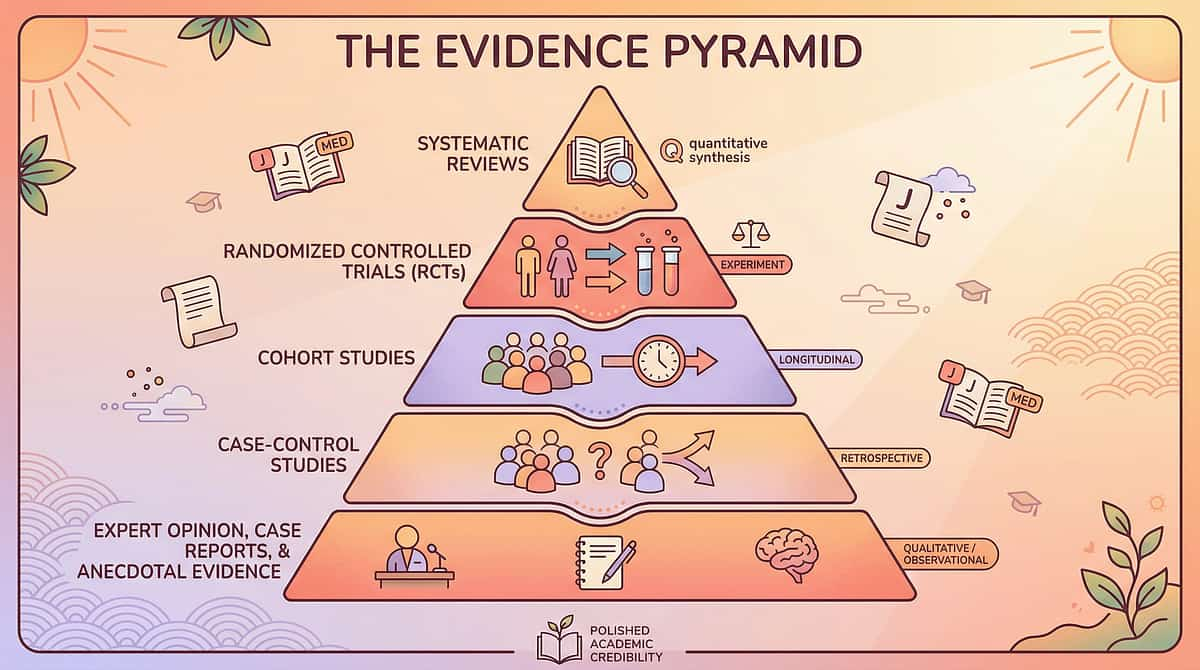
📄 Level I — Systematic Reviews
PMC11506176 (2024): PRISMA review — 16 studies confirm sensory integration is evidence-based practice for ASD. pubmed.ncbi.nlm.nih.gov
PMC10955541 (2024): Meta-analysis — sensory integration improves social skills, adaptive behaviour, sensory processing, motor skills. DOI: 10.12998/wjcc.v12.i7.1260
📄 Level II — RCTs
Padmanabha et al., Indian J Pediatr (2019): Home-based sensory interventions — RCT in Indian paediatric population. DOI: 10.1007/s12098-018-2747-4
📄 Level III — Practice Guidelines
NCAEP Evidence-Based Practices (2020): Visual supports, sensory integration, structured routines for autism. ncaep.fpg.unc.edu
WHO Nurturing Care Framework (2018): nurturing-care.org/ncf-for-ecd
PMC9978394: WHO Care for Child Development Package.
Additional reading: Polyvagal Theory (Porges) | Regulatory Battery concept | Masking/Camouflage in autism: Hull et al., Autism (2017) | ADHD post-school dysregulation: CHADD & ADDitude literature
Pinnacle Internal Evidence Base: 20M+ exclusive 1:1 sessions | AbilityScore® longitudinal database | Outcome tracked via Self-Regulation Readiness Index. Aggregate data shared with permission — individual data protected.

Your Data Helps Every Child Like Yours. Here Is Exactly How.
GPT-OS® Technology
What GPT-OS® Learns from H-709 Data
- Which of the 9 materials shows fastest recovery time improvement
- At what weeks specific tools are self-initiated (generalisation indicators)
- Correlation between meltdown severity and school day events
- Effectiveness variance by sensory profile type
Privacy Protection ✅
- Data encrypted at rest and in transit
- Identifiable data never shared externally
- De-identified aggregate data used for population-level learning
- Parent controls data sharing preferences
- DPDP Act 2023 (India) compliant
"Your child's data, combined with data from 20M+ sessions, helps GPT-OS® give better recommendations to every family navigating this exact challenge. Your afternoons are teaching the system. The system gets better for everyone."
Related Techniques. After-School Regulation Is Part of a Larger Map.
Daily Living & Self-Regulation Cluster
← H-708
Morning Routine Challenges — Starting the Day Right
📍 H-709
After-School Exhaustion Recovery (YOU ARE HERE)
H-710 →
Evening Routine Support — From Recovery to Rest
H-707
Transition Difficulties — When Any Change is a Crisis
H-711
Weekend Regulation — When Structure Disappears
H-715
Homework Battles — The Post-Recovery Challenge
G-620
Sensory Processing and Daily Life
C-254
Emotional Regulation — Weighted Calming
A-180
Sensory Integration — Deep Pressure Protocols
Domain H: Daily Living & Self-Regulation | Episodes 700–799 | 100 techniques in this domain. "Every hour of the child's day has a corresponding support structure within GPT-OS®." Browse all Domain H techniques — techniques.pinnacleblooms.org

You Don't Have to Figure This Out Alone. We Are Here. Right Now.
Connect with Pinnacle
ACT V: Community
📞 Free Helpline
9100 181 181
Available 24×7 | 16+ Languages | No appointment needed. A trained therapist picks up — not a call centre. You describe your child's challenges. They guide you to the right starting point.
Available 24×7 | 16+ Languages | No appointment needed. A trained therapist picks up — not a call centre. You describe your child's challenges. They guide you to the right starting point.
🌐 Online
pinnacleblooms.org
care@pinnacleblooms.org
Book teleconsultation — available internationally. AbilityScore® assessment online. EverydayTherapyProgramme™.
care@pinnacleblooms.org
Book teleconsultation — available internationally. AbilityScore® assessment online. EverydayTherapyProgramme™.
📍 70+ Centres
Across India. Find your nearest centre at pinnacleblooms.org. Serving families from 70+ countries through digital platforms. Language is not a barrier — we operate in 16+ languages.
What Professional Support Actually Looks Like. Step by Step. No Confusion.
Professional Support Pathway
Free Helpline Triage
📞 9100 181 181 | 15-minute intake assessment. Determines: urgency level, relevant domains, next step.
AbilityScore® Assessment (₹1,500–3,000)
Comprehensive 591-point developmental observation. Outputs: Standardised baseline score, domain profile, severity level, priority intervention areas. Available at 70+ centres or online (video-based).
Occupational Therapy Evaluation
Sensory profile assessment | SIPT/SPM administration. Customised sensory diet design | After-school protocol calibration.
FusionModule™ Programme
OT + ABA + SLP + SpEd coordinated around single protocol. Session data feeds GPT-OS® for personalised adaptation.
EverydayTherapyProgramme™ Home Extension
Clinician-designed home protocol | Daily micro-interventions. Data capture integrated | Therapist review at each session.
Government Scheme Access: UDID (Unique Disability Identity Card) guidance | RBSK (Rashtriya Bal Swasthya Karyakram) access | NIMHANS Referral network guidance — available through Pinnacle.
Frequently Asked Questions
FAQ
ACT VI: The Close
Q: My child's teachers say they're fine at school. Should I trust that?
Yes — AND understand it doesn't contradict your experience at home. The school version is a performance that costs everything the child has. Both realities are true simultaneously. The discrepancy IS the evidence of ASRC, not evidence that you're wrong. Bring your tracking data to the school conversation.
Q: How long will the recovery routine need to be in place?
Most children with significant ASRC benefit from a structured recovery routine through primary school (ages 5–12 approximately). Think of it as scaffolding: it reduces as the structure builds itself. With consistent support, intensity required typically decreases as self-regulation capacity builds.
Q: Is After-School Restraint Collapse only for autistic children?
No. ASRC affects all neurodivergent children significantly — autism, ADHD, anxiety, sensory processing differences, learning disabilities. It can also affect neurotypical children in high-pressure environments, though typically with less severity. The materials and protocol in this guide work across profiles.
Q: My child refuses ALL the materials. What do I do?
Start with the most accepted tool only — even if it's just the snack. Build the routine around one anchor. Over 2–3 weeks, silently introduce a second tool. Presence of tools without use still helps — your child sees the space exists and is prepared for them. See the Troubleshooting card for full guidance.

More Frequently Asked Questions
Q: Can I do homework during the recovery period?
Not in the first 30–60 minutes for most children with significant ASRC. Homework requires exactly the regulatory resources most depleted — sustained attention, impulse control, frustration tolerance. Attempting homework during peak depletion typically produces 3× longer conflict than waiting. Homework after recovery is faster and of better quality. Advocate for flexible homework timing with school.
Q: We can't afford all 9 materials. Where do we start?
Start with these 3: (1) Any heavy blanket — stacked regular blankets. (2) Quiet corner with comfortable surface — free. (3) Consistent protein snack — you may already have this. These three alone, applied consistently, can produce meaningful improvement in weeks 1–4. Full DIY protocols are provided for every material.
Q: How do I know if my child needs professional OT beyond this protocol?
If after 6–8 consistent weeks the recovery time hasn't shortened at all, meltdown severity is unchanged, and the evening is still entirely lost — this level of dysregulation likely requires individualised OT assessment. The protocol prepares excellent clinical data to bring to that assessment. 📞 9100 181 181
Q: Does this protocol work for children who shut down rather than melt down?
Yes — and shutdown children often respond even faster than explosive ones. The weighted blanket, quiet space, and zero-demand approach are precisely calibrated for the freeze/shutdown response. Dim the space, reduce all interaction, offer weight silently. The shutdown is the nervous system conserving energy — the protocol gives it permission to rest without threat.
Didn't find your answer? Ask GPT-OS® — pinnacleblooms.org/ask | 📞 Call free helpline: 9100 181 181 | Book a teleconsultation
One Parent Knowing Is Not Enough. Consistency Across All Caregivers Multiplies Impact.
Share This Protocol
For Grandparents (Simplified)
When [child's name] comes home from school, they need quiet time and their blanket for about 30–40 minutes. Please:
- Don't ask how school was right away
- Have their snack ready
- Let them be quiet
- They are not being rude — they are recovering
After their quiet time, they will be themselves again.
For School Teachers
"My child experiences After-School Restraint Collapse — a documented phenomenon in occupational therapy literature. The child you see at school is giving everything they have. The child we see at home is what that cost looks like.
This is not about home management. This is about support at both ends. I'd welcome a conversation about school-side accommodations — particularly homework timing flexibility and transition support."
Full template available to download via pinnacleblooms.org
"Every person who interacts with your child in the post-school window is either supporting recovery — or accidentally extending the collapse. Share this page." — WHO CCD Package: Multi-caregiver training is critical for intervention generalisation. (PMC9978394)

Stop Reading. Start Building. Your Child's Recovery Routine Starts Today.
You've read the science. You understand what's happening in your child's nervous system. You have the materials list, the protocol, the scripts. The only thing left is to start. Not perfectly. Not completely. Start with one material. Today.
🦾 Occupational Therapy
🗣️ Speech Pathology
🧩 ABA / BCBA
📚 Special Education
🧬 NeuroDev Paediatrics
🔬 Clinical Research
🌸 Validated by the Pinnacle Blooms Consortium | WHO/UNICEF Grade Clinical Standards | 📞9100 181 181 FREE | 24×7 | 16+ Languages | "One call. A therapist answers. Your questions, answered."
Preview of 9 materials that help with after school exhaustion Therapy Material
Below is a visual preview of 9 materials that help with after school exhaustion therapy material. The pages shown help educators, therapists, and caregivers understand the structure and content of the resource before use. Materials should be used under appropriate professional guidance.




















Link copied!

🌸 Pinnacle Blooms Network®
Built by Mothers. Engineered as a System.
"From fear to mastery. One technique at a time."
20M+
Sessions
Exclusive 1:1 therapy sessions
97%+
Improvement
Measured across all programmes
70+
Centres
Across India
70+
Countries
Families served globally
"Pinnacle Blooms Network® is the world's most comprehensive paediatric therapy consortium — serving 70+ centres, 70+ countries, 20M+ exclusive 1:1 therapy sessions, 97%+ measured improvement. Every technique in this library is validated by the GPT-OS® platform — the world's first closed-loop paediatric therapeutic operating system."
← H-708
Morning Routine Challenges
📞 9100 181 181
FREE National Autism Helpline | 16+ Languages | 24×7
H-710 →
Evening Routines — Continue the Recovery Arc
CIN: U74999TG2016PTC113063 | DPIIT: DIPP8651 (Govt. of India Recognised Startup) | MSME: Udyog Aadhaar TS20F0009606 | GSTIN: 36AAGCB9722P1Z2
This content is educational. It does not replace individualised assessment and intervention from licensed occupational therapists, behavioural therapists, or mental health professionals. If your child's after-school difficulties are severe, persistent, or significantly impacting daily functioning, seek professional assessment. Call 9100 181 181 for free guidance. Individual results may vary. Statistics represent aggregate outcomes across the Pinnacle Blooms Network®.
© 2025 Pinnacle Blooms Network®, a unit of Bharath Healthcare Laboratories Pvt. Ltd. All rights reserved. techniques.pinnacleblooms.org