
"Every time we say time to stop, the world ends."
It's 6:47 PM. Dinner is ready. Your son has been playing with his trains for 40 minutes — calm, focused, happy. You say time to put trains away. Within 4 seconds, he's on the floor, screaming. Not because he's bad. Not because you did something wrong. Because his brain genuinely cannot shift gears — and nobody told you that changing activities is one of the hardest neurological tasks a developing child can face.
🧠 You are not failing. Your child's nervous system is speaking.

The Numbers Behind the Daily Battle
If your child collapses at every activity change, you are among millions of families navigating this exact neurological challenge. Transition difficulty is not rare. It is not a parenting failure. It is one of the most documented challenges in pediatric developmental science — and it has real, evidence-backed solutions.
80%+
Children with ASD
show transition difficulties as a primary daily challenge
1 in 36
Children in India
diagnosed with ASD — 85% show transition difficulty as a core challenge
20M+
Therapy Sessions
at Pinnacle where transition difficulty ranks in the top-3 presenting concerns
"You are among an estimated 3–5 million families in India alone navigating daily transition challenges. The struggle is real. The science is clear. The support exists." — Pinnacle Blooms Consortium, GPT-OS® Clinical Intelligence
PRISMA systematic review (2024, PMC11506176): 80% of children diagnosed with autism display transition and sensory processing difficulties as clinically documented challenges. India prevalence: 1 in 36 children (Pediatric data, 2023). Pinnacle GPT-OS® RWE: Transition difficulty ranked in top-3 presenting challenges across 20M+ therapy sessions.

This Is Brain Science, Not Behaviour
What's Happening Neurologically
The Prefrontal Cortex governs executive functions — including the ability to stop one thing and start another. In many children with autism, ADHD, and developmental differences, this system is neurologically immature or differently wired. Set-shifting — the clinical term for changing mental gears — is genuinely harder.
The Set-Shifting Pathway must fire perfectly for every single activity change your child faces throughout the day.
The 4-Step Transition Process
Disengage
Stop the reward loop of the current activity — the hardest step neurologically
Manage Emotion
Tolerate the frustration of stopping before the brain has fully let go
Mental Shift
Release the previous mental "set" — the cognitive anchor to what was happening
Re-Engage
Orient to the new activity and build a new focus loop
All four steps happen simultaneously in under 10 seconds. For a developing prefrontal cortex, this is neurological heavy lifting.
"This is a wiring difference, not a behaviour choice. Punishment doesn't rewire the brain. The right supports do."
Frontiers in Integrative Neuroscience (2020, DOI: 10.3389/fnint.2020.556660): Established neurological basis for set-shifting difficulties in ASD and developmental conditions. Prefrontal cortex maturation continues into early adulthood, making childhood the critical window for scaffolded transition support.

Your Child's Development — Right Now, Right Here
Understanding where your child sits on the developmental timeline transforms a crisis into a waypoint. Every age brings its own relationship with transitions — and every age has its own power window for intervention.
Age 2
Basic routine awareness emerging. Transition difficulty is developmentally expected — even neurotypical children struggle here.
Ages 3–4
Cognitive flexibility begins developing. With neurodevelopmental differences, the struggle is more intense and persists significantly longer.
Ages 5–7 ★
Critical intervention window. The prefrontal cortex is actively developing. Consistent transition supports now build the neural scaffolding that makes future flexibility easier.
Ages 8–10
Executive function refines significantly. Children who received consistent transition support from ages 4–7 show measurably better self-regulation.
Age 10+
Adult-like flexibility emerging. Strategies become internalised when the neural scaffolding was built early.
Transition difficulty commonly co-occurs with: Autism Spectrum Disorder (ASD) | ADHD | Anxiety Disorders | Sensory Processing Differences | Developmental Delays | PDA Profile. If multiple apply to your child, transition difficulty will be more intense — but the strategies still work. They just require more consistency.
"Your child is here. With the right supports, consistent practice, and the 9 materials in this guide — transitions become manageable moments, not daily crises."
WHO Care for Child Development Package (CCD, 2023) | UNICEF MICS indicators for developmental monitoring across 197 countries | PMC9978394: Home-based intervention in the 3–7 age window shows strongest neuroplasticity response.
Clinically Validated. Home-Applicable. Parent-Proven.
Evidence Grade: I — Systematic Review + RCT Supported
The 9 materials in this guide are not opinions. They are tools with a documented evidence trail — validated by international systematic review, confirmed in Indian clinical settings, and refined across 20 million real therapy sessions.
Source | Finding | Grade | |
PRISMA Review (2024, PMC11506176) | Visual supports + transition strategies classified as evidence-based practice for ASD across 16 studies (2013–2023) | Level I | |
NCAEP (2020) | Visual supports + antecedent-based interventions confirmed evidence-based practices for autism | Level I | |
Meta-analysis World J Clin Cases (2024, PMC10955541) | Structured behavioural + sensory supports effectively promote adaptive behaviour and flexibility in 24 studies | Level I | |
Padmanabha et al., Indian J Pediatr (2019) | Home-based structured interventions demonstrate significant outcomes in Indian pediatric population | Level II RCT | |
Pinnacle GPT-OS® RWE | 97%+ measured improvement across 20M+ sessions including transition-specific interventions | Population-Level |
"The evidence trail leads here — validated by international systematic review, confirmed in Indian clinical settings, refined across 20 million real therapy sessions."
Transition Support Toolkit: What It Is
Technique I-786
Ages 2–10
Behavioral Flexibility
Formal Name: Transition Support Material Systems — also called "The Gear-Shift Toolkit."
Transition Support Material Systems are structured, evidence-based tools that reduce the cognitive and emotional demands of shifting from one activity to another. They work by making abstract concepts — time, sequence, what's next — visible and concrete. They provide graduated warnings instead of abrupt stops, offer sensory and emotional regulation support during the moment of change, and restore the child's sense of agency within transitions. These are not behaviour management tricks — they are external scaffolds that support developing executive function until the brain's own regulatory systems mature.
🏠 Setting
Home + School + Community
⏱ Session
5–20 minutes
📅 Frequency
Daily — every transition
👶 Age Range
2–10 years
🎓 Lead Disciplines
OT + ABA + SpEd
Transition Objects
Visual Schedule Systems
Reinforcement Menus
Calming Tools
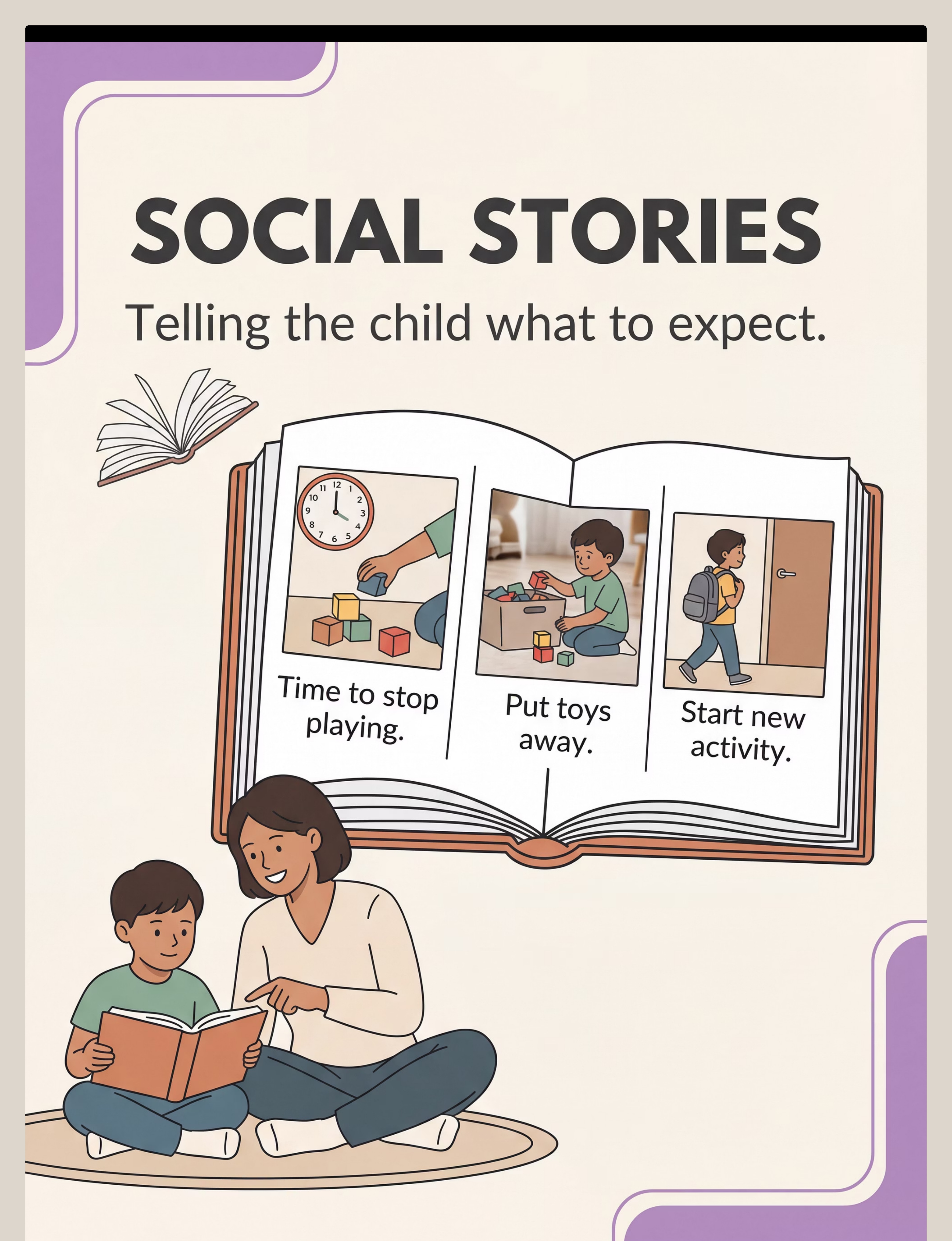
Social Narrative Systems
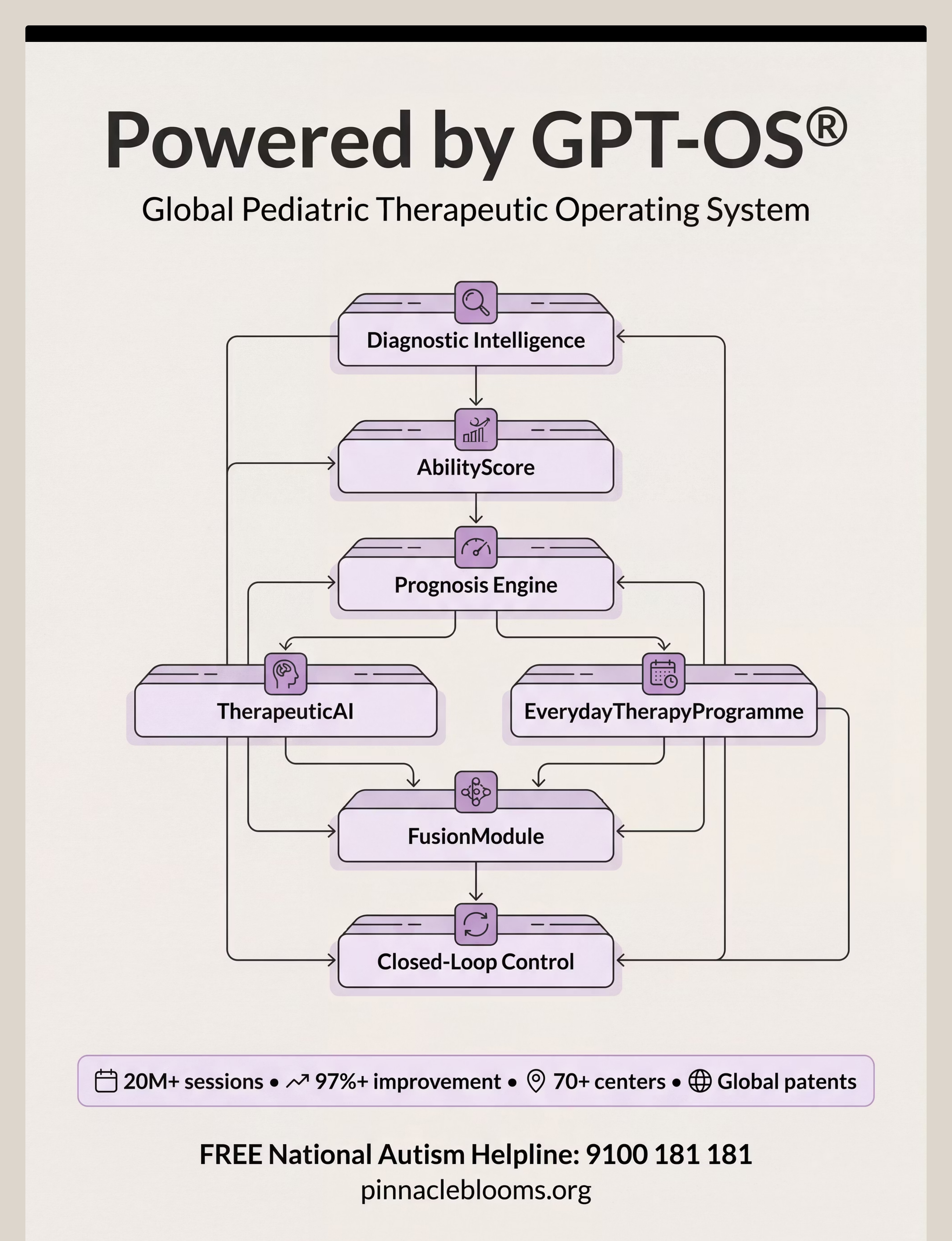
Five Therapy Disciplines. One Unified Approach.
Transition difficulty sits at the intersection of sensory processing, behaviour, communication, learning, and neurology. This is why single-discipline approaches often plateau. The Pinnacle GPT-OS® FusionModule™ integrates all five into one converged transition support plan.
🔵 Occupational Therapy (Lead)
Environmental setup, sensory regulation during transitions, transition object selection, calming toolkit curation. "The OT designs the sensory scaffold around every transition."
🟣 Applied Behaviour Analysis (Co-Lead)
Antecedent manipulation, countdown systems, reinforcement schedules, data collection, First-Then boards as contingency tools. "The BCBA builds the behavioural structure that makes transitions predictable."
🟢 Speech-Language Pathology
Visual schedules as AAC supports, social stories for language comprehension, transition song selection for auditory processing profiles. "The SLP ensures every transition support works for the child's communication level."
🟡 Special Education
Classroom transition systems, teacher training, IEP goal alignment, school-home consistency of transition protocols. "The SpEd specialist bridges home strategies into the school day."
🔴 Neurodevelopmental Paediatrics
Diagnostic clarity, medication considerations, family psychoeducation, medical red-flag monitoring. "The NeuroDev doctor provides the neurological map that guides all other disciplines."
UNICEF/WHO Nurturing Care Framework for SLPs (2022, DOI: 10.1080/17549507.2022.2141327): Multi-disciplinary convergence essential for comprehensive developmental support.
Precision Targets. Not Random Activities.
Every material in this toolkit targets a specific layer of transition difficulty. Understanding the three-ring target helps you measure progress at the right level — daily, weekly, and across months.
Primary — Daily Measurement
- Transition time decreasing (from 20 min toward 5 min)
- Intensity of distress during transitions reducing
- Child acknowledging the transition cue
- Physical resistance decreasing (no more going limp or running away)
Secondary — Over Weeks
- Child using calming strategies independently
- Asking about what's next rather than refusing to move
- Accepting warnings without pre-emptive meltdowns
- Tolerating unexpected changes with support (not independently yet)
Tertiary — 3–6 Month Horizon
- School-reported improvement in activity changes
- Community participation increasing (less avoidance)
- Family able to attempt outings without transition dread
PMC10955541 (Meta-analysis, 24 studies): Structured supports promote adaptive behaviour (primary), social skills (secondary), and broad developmental participation (tertiary). NCAEP (2020): Visual supports show measurable outcomes across all three target rings.

9 Materials. 9 Tools to Transform Transitions.
Each material addresses a different layer of transition difficulty. Together, they create a complete transition support ecosystem. You do not need all 9 at once — start with 1–2 that feel most natural for your child's profile.
I-786 Material System
Canon Materials
GPT-OS® Validated
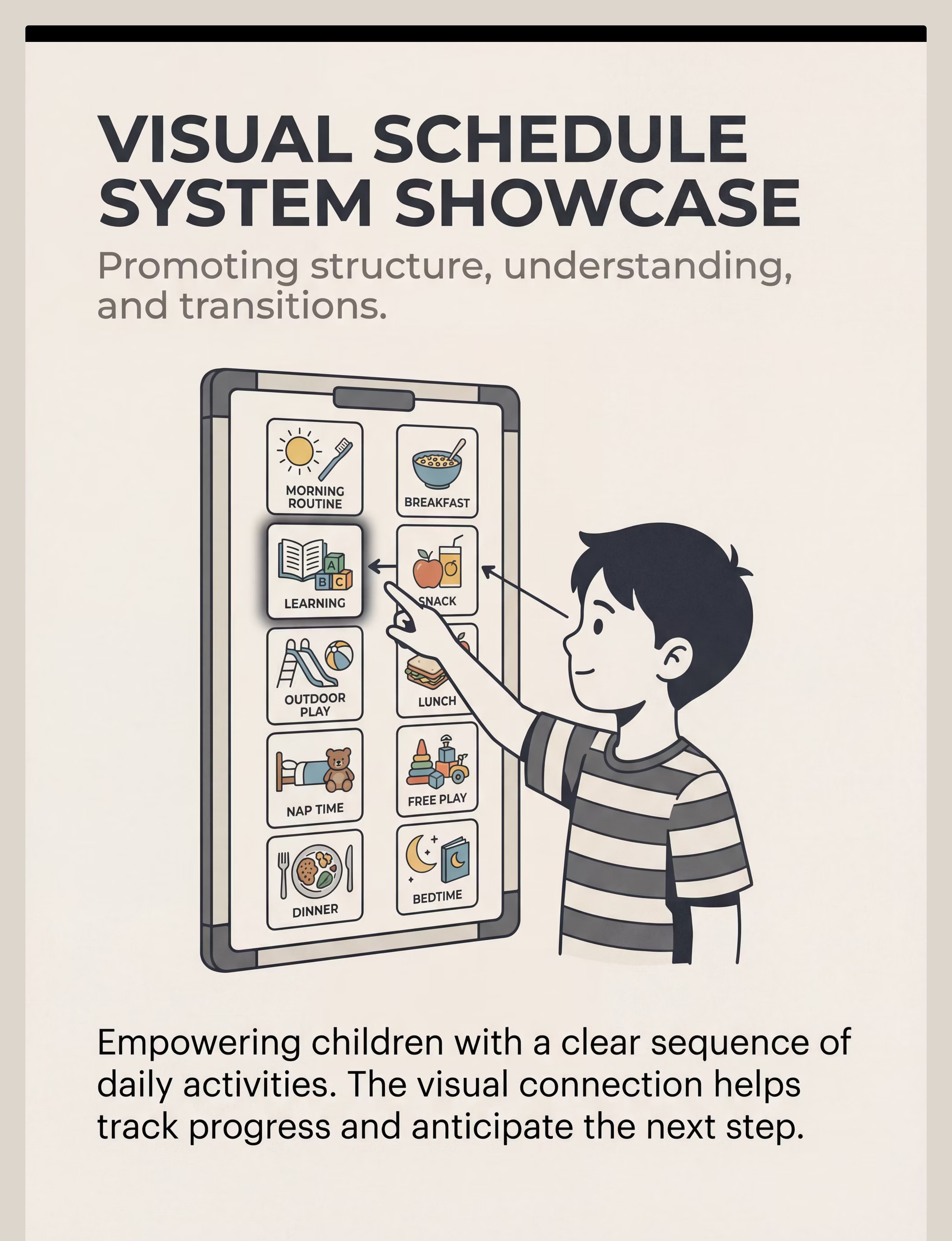
Visual Schedule Systems
Canon Category: Visual Schedule Systems
What It Does: Makes the day's sequence visible — eliminates "what's next?" anxiety completely
Price Range: ₹300–2,000 | Search Amazon.in →
What It Does: Makes the day's sequence visible — eliminates "what's next?" anxiety completely
Price Range: ₹300–2,000 | Search Amazon.in →
Visual Timers
Canon Category: Visual Timers / Time Concept Tools
What It Does: Makes invisible time concrete — child watches time "shrink" and prepares mentally
Price Range: ₹400–1,500 | Search Amazon.in →
What It Does: Makes invisible time concrete — child watches time "shrink" and prepares mentally
Price Range: ₹400–1,500 | Search Amazon.in →
Transition Objects (Comfort Items)
Canon Category: Transition Objects / Comfort Items
What It Does: A sensory anchor — something familiar the child carries through the change
Price: ₹425 | Animal Soft Toys — Amazon.in →
What It Does: A sensory anchor — something familiar the child carries through the change
Price: ₹425 | Animal Soft Toys — Amazon.in →
First-Then Boards
Canon Category: First-Then Boards / Visual Contingency Tools
What It Does: Simplifies every transition to just two things — NOW and NEXT
Price Range: ₹200–800 | Search Amazon.in →
What It Does: Simplifies every transition to just two things — NOW and NEXT
Price Range: ₹200–800 | Search Amazon.in →
Transition Songs / Audio Cues
Canon Category: Auditory Transition Cues
What It Does: A consistent sound/song that conditions the brain to expect change
Price Range: ₹0–500 | Search Amazon.in → | ✓ DIY: any consistent song
What It Does: A consistent sound/song that conditions the brain to expect change
Price Range: ₹0–500 | Search Amazon.in → | ✓ DIY: any consistent song
Countdown & Warning Systems
Canon Category: Countdown Visual Systems
What It Does: Graduated warnings (5→3→1→done) replace abrupt stops
Price Range: ₹100–600 | Search Amazon.in → | ✓ DIY: fingers + verbal
What It Does: Graduated warnings (5→3→1→done) replace abrupt stops
Price Range: ₹100–600 | Search Amazon.in → | ✓ DIY: fingers + verbal
Social Stories for Transitions
Canon Category: Social Narrative Systems / Story-Based Learning
What It Does: Short narratives that prepare the child for what will happen — before it happens
Price Range: ₹200–1,000 | Search Amazon.in → | ✓ DIY: parent-made with photos
What It Does: Short narratives that prepare the child for what will happen — before it happens
Price Range: ₹200–1,000 | Search Amazon.in → | ✓ DIY: parent-made with photos
Calming Tools (Regulation Support)
Canon Category: Calming & Regulation Tools / Sensory Support
What It Does: Gives the nervous system something to DO with the distress of transition
Price Range: ₹200–1,200 | Search Amazon.in →
What It Does: Gives the nervous system something to DO with the distress of transition
Price Range: ₹200–1,200 | Search Amazon.in →
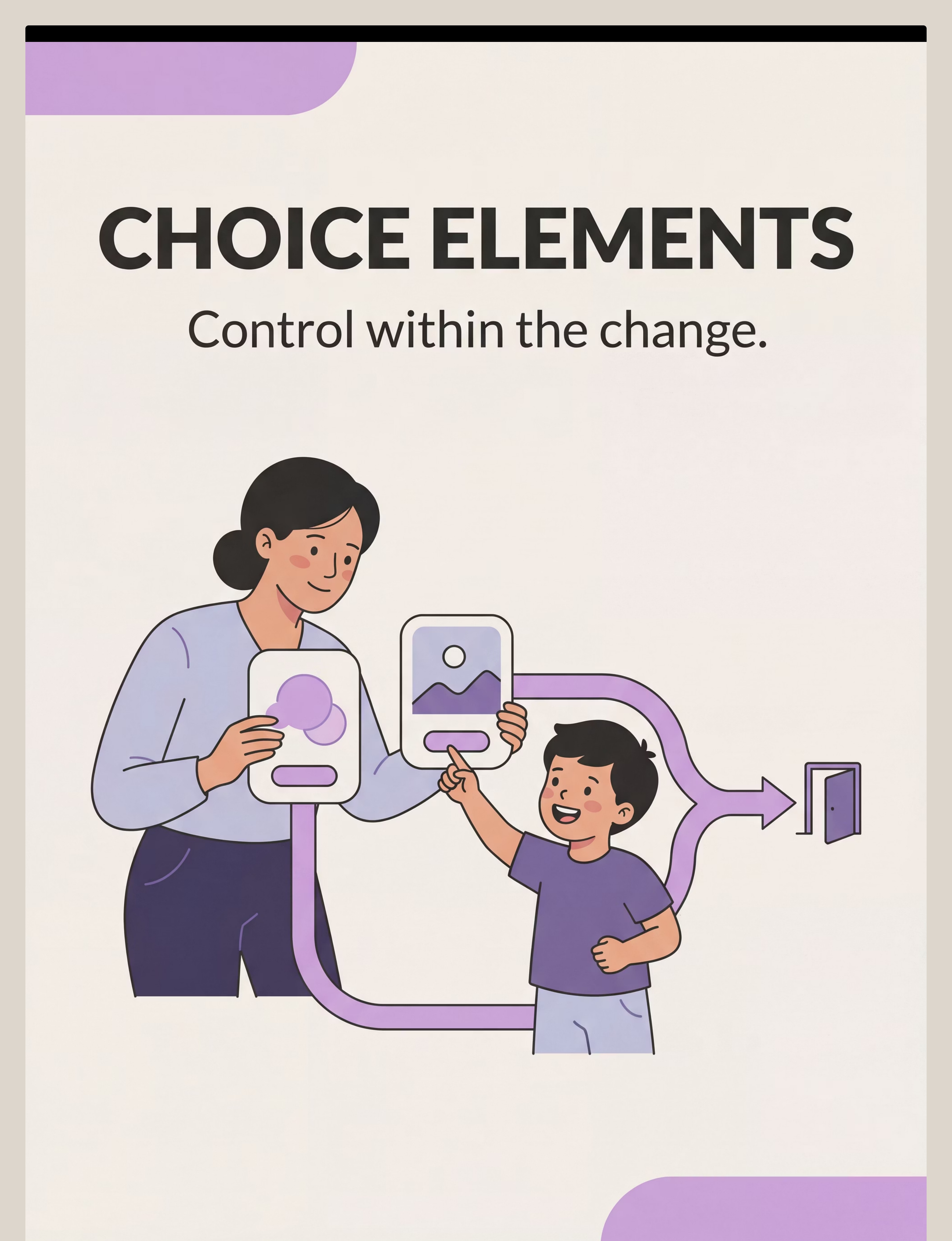
Choice & Control Elements
Canon Category: Choice Boards / Agency Tools
What It Does: Restores the child's sense of agency WITHIN the transition — not whether, but how
Price Range: ₹0–300 | Search Amazon.in → | ✓ DIY: any two-option visual
What It Does: Restores the child's sense of agency WITHIN the transition — not whether, but how
Price Range: ₹0–300 | Search Amazon.in → | ✓ DIY: any two-option visual
🎁Reinforcement Integration: The Rosette Imprint Reward Jar | ₹589 | Amazon.in — Use with Material 9 to celebrate successful transitions and build positive associations with change.
NCAEP (2020): All 9 material categories align with evidence-based practices for ASD. PMC11506176: Visual supports + behavioural tools + sensory regulation = strongest evidence base for transition difficulty.

Every Material Has a ₹0 Version
WHO/UNICEF equity principle in action: every family, regardless of income, can execute these techniques today with household items. Consistency matters more than quality. A permanent DIY visual schedule used daily beats a commercial one used occasionally.
Material | Buy Version | ₹0 DIY Version | |
Visual Schedule | Laminated picture board (₹300–800) | Printed photos or drawn pictures on A4 paper, taped to wall | |
Visual Timer | Sand hourglass or Time Timer (₹400–1,500) | Phone timer app with visual countdown (free) or draw a simple clock face | |
Transition Object | Soft toy (₹425) | Any small item the child values — stone, keychain, mini-toy from home | |
First-Then Board | Commercial board (₹200–800) | Fold A4 paper in half, write "FIRST" and "THEN," tape pictures | |
Transition Song | Chime/bell (₹100–500) | Sing the same song every time — free and infinitely portable | |
Countdown System | Flip cards (₹100–600) | Hold up fingers + verbal countdown (zero cost) | |
Social Story | Printed/laminated (₹200–1,000) | Write a simple 5-sentence story with real photos of your child, print at home | |
Calming Tools | Fidget/stress ball (₹200–800) | Playdough (homemade), a cup of water to sip through a straw, hand squeezes | |
Choice Elements | Choice board (₹100–300) | Hold up two objects and let child point — no board needed |
When the commercial version matters: Some children respond better to purpose-made, visually consistent materials. If your DIY version is inconsistently available, the tool loses effectiveness. Consistency is the non-negotiable variable — not cost.
WHO NCF (2018): Context-specific, equity-focused interventions. CCD Package implemented across 54 LMICs confirms household-material-based intervention efficacy. PMC9978394.

Read This Before Your First Session
🔴 DO NOT PROCEED if:
- Child is currently in a meltdown or post-meltdown recovery state
- Child is unwell, feverish, or in physical pain
- You are at emotional capacity — your calm is the first requirement
- The transition environment is chaotic (loud, crowded, unpredictable)
🟡 MODIFY before proceeding if:
- Child is tired but not dysregulated — shorten session, reduce demands
- Child is hungry — feed first, transition after
- Transition involves an activity the child has never done before — add extra preparation time
- You're introducing a new material today — introduce during calm time, not a live transition
🟢 PROCEED when:
- Child is fed, rested, and in a baseline regulated state
- Environment is prepared (materials ready before announcing transition)
- You have 5–10 minutes to support the transition without time pressure
- You are calm and have the emotional capacity to follow through
Material Safety Notes
- Visual schedule Velcro pieces: ensure firmly attached; small picture cards away from very young children (choking risk)
- Sand timers (glass): supervise use; choose plastic versions for younger children
- Transition objects: ensure small enough to carry but not a choking hazard developmentally
- Calming fidgets: no small detachable parts for children with oral seeking behaviours
- All materials: age-appropriate for developmental level, not just chronological age
🛑STOP IMMEDIATELY if you observe: child showing signs of severe panic (not frustration), physical self-harm, inability to breathe/regulate, or complete dissociation. Contact your Pinnacle therapist or call 9100 181 181.
Indian J Pediatr (2019, DOI: 10.1007/s12098-018-2747-4): Home-based intervention safety protocols. Pinnacle GPT-OS® clinical safety framework for parent-administered sessions.

Prepare the Stage Before the Curtain Rises
"The right environment prevents 80% of transition failures before they begin."
Room Setup Guide
Visual Schedule
Mounted at child eye level — visible, updated for today's sequence
Visual Timer
Placed where child can see it clearly from their current activity position
Calming Kit
Within child's reach but not distracting during current activity
Transition Object
In your hand, ready to give at transition start — proactively, not reactively
Setup Checklist
- Visual schedule visible and updated for today
- Visual timer accessible and functioning
- Distracting screens/toys from ending activity OUT OF SIGHT (not just off)
- Next activity space/materials SET UP before announcing transition
- Transition object in your hand, ready
- Calming tools within child's reach
- Your phone face-down or on silent
- You have taken 3 deep breaths and feel ready
"Set up the NEXT activity before ending the CURRENT one. A child who sees where they're going transitions far more easily than one stepping into the unknown."
Sensory Integration Theory (Ayres): Environmental setup is a core protocol element. PMC10955541: Structured session environments show significantly higher outcome rates than unstructured.
60-Second Pre-Flight Check
Before every session, run this quick readiness check. A session that starts right is a session that succeeds. "The best session is the one that starts right. There is no shame in postponing — that IS the clinical decision."
Indicator | ✓ GO | ⚠ MODIFY | ✗ POSTPONE | |
Physical state | Fed, rested | Tired but not crying | Visibly unwell/in pain | |
Emotional state | Baseline/calm | Slightly elevated but engageable | Dysregulated/post-meltdown | |
Engagement level | Focused on current activity | Transitioning spontaneously | Completely checked out or overstimulated | |
Time available | 5–10 min to support | 2–3 min only | Less than 2 min or extreme time pressure | |
Your state | Calm and present | Manageable stress | At capacity or triggered |
ALL GREEN
Proceed to Step 1: Full Protocol
SOME AMBER
Proceed with Simplified Version — reduce to ONE material only
ANY RED
Postpone — offer a calming activity and try again in 30–60 minutes
ABA antecedent manipulation principles: setting events and establishing operations fundamentally determine session effectiveness. Pinnacle GPT-OS® session readiness protocols.

Step 1 of 6
🎯 Step 1 — The Invitation
Timing: 30–60 seconds before the transition. Move to the child's level. Make eye contact (without forcing it). Use a calm, warm, matter-of-fact voice — not a warning voice, not a negotiation voice.
Say:"[Child's name], I can see you're really enjoying your trains. In a little while, we'll have dinner. Let me show you what's coming." [Point to visual schedule]
Acceptance Cues — What to Look For
- Brief glance at schedule
- Body remains relaxed (not tightening)
- No immediate protest
- Continues current activity without escalating
Resistance Signals — What to Do
- ⚠ Immediate "no" → Acknowledge: "I hear you — you love your trains. And in a few minutes, dinner. Let me set the timer." Do not argue. Move to timer immediately.
- ⚠ Body stiffening → Lower your voice further. Don't increase urgency.
- ⚠ Running away → Do not chase. Stay calm. Allow 10 more seconds, then gently re-introduce.
Parent Body Language Guide: Position yourself BESIDE the child, not in front of (blocking) them. Stay at their physical level. No hands on hips. Soft, forward-open posture.
ABA Pairing Procedures: Establishing motivating operations before demand placement. OT "Just-Right Challenge" principle: matching task demand to current capacity.

Step 2 of 6
🎯 Step 2 — The Engagement
Timing: 2–3 minutes before the transition. This step introduces your chosen transition material. Your job is to make it a bridge, not a barrier.
If Using Visual Timer
"See this timer, [name]? I'm going to set it for 3 minutes. When the red is all gone, that's when we do dinner. Can you watch the timer for me?" [Hand or show timer. Let child interact briefly if they want.]
If Using First-Then Board
"Look here — FIRST trains [point]. THEN dinner [point]. See? Trains, then dinner." [Use child's name for each activity. Keep it simple. Two words each.]
If Using Countdown
"We have 5 more minutes with the trains. I'm going to count down: 5... 4... 3... 2... 1." [Show fingers. Pause between each number. This is not a fast countdown.]
Child Response Spectrum
🟢 Ideal
Child acknowledges material, remains in current activity
🟡 Acceptable
Child ignores material but doesn't escalate
🔴 Concerning
Child throws material, intense protest → withdraw, try just verbal countdown
When child glances at the timer or schedule: "That's right — you're watching the timer! Great job." [Simple, immediate, genuine — within 3 seconds]
PMC11506176: Structured material introduction as evidence-based practice. ABA reinforcement scheduling: immediate positive reinforcement within 3 seconds.
Step 3 of 6
🎯 Step 3 — The Therapeutic Action
The actual transition moment — the neurologically hardest step. Your approach here determines whether the transition succeeds or escalates. This is the actual stop.
Announce Calmly
"Timer's done. Trains go to sleep now. Let's see the schedule." [Touch the visual schedule — "Now it's dinner time."]
Hand the Transition Object
"Here's [child's name]'s special helper. He/she comes with us to dinner." — Proactive, not reactive
Create Movement Momentum
Move toward the next activity space yourself first. Don't wait for child to lead — you go first, they follow.
Acknowledge the Hard
"I know it's hard to stop. You did really well with your trains today." — Validation, not sympathy
✓ Correct Execution
- Announcement made ONCE — not repeated multiple times
- Transition object handed BEFORE resistance begins
- You move toward next space — create momentum
- Verbal acknowledgment of the difficulty
✗ Common Errors
- Repeating "it's time to stop" more than twice — weakens the signal
- Waiting for child to initiate movement
- Negotiating after timer ends — teaches timer is not reliable
- Physical rushing — escalates nervous system arousal immediately
Duration: The actual transition moment: 30 seconds to 2 minutes. If still escalating at 3 minutes, move to the Troubleshooting card.
PMC10955541: Structured, consistent transition procedures show fastest improvement in set-shifting tolerance. NCAEP (2020): Antecedent-based interventions most effective for preventing meltdowns.
Step 4 of 6
🎯 Step 4 — Repeat & Vary
3 good transitions beat 10 forced ones. Your daily goal is not to complete every transition perfectly — it's to complete 2–3 with full support, consistently, every day.
Weeks 1–2
Aim for 2 fully supported transitions per day using your chosen materials. Consistency is everything right now.
Weeks 3–4
Extend to 3–4 transitions with the same support. Look for anticipation cues — the child turning toward the schedule before you point.
Weeks 5–8
Begin introducing variation: different timer durations, different transition objects for different contexts, fading the First-Then toward verbal.
Variation Options
Vary the timer duration: Start with 2–3 minute warnings. As tolerance builds, try 5 minutes, then 10.
Vary the transition objects: Different objects for different contexts — home vs. school vs. community outings.
Vary the song/cue: Once conditioned to one cue, a second cue for a different context builds flexible cueing.
Fade the First-Then to verbal: After weeks of success with the board, try saying "First [activity], then [activity]" without showing the board. Success = internalisation.
Satiation Indicators — stop here: Child ignoring the material and transitioning anyway (it's working — begin fading!) | Child fixated ON the material (vary the tool) | Child is visibly done — seeking break — shorten this session.
SI therapy dosage (clinical consensus): 2–3 sessions per week for 8–12 weeks. ABA: distributed practice (daily, brief, consistent) shows stronger long-term retention than massed practice.

Step 5 of 6
🎯 Step 5 — Reinforce & Celebrate
Timing: Within 3 seconds of transition completion. Not after dinner. Not before bed. Immediately when the child completes the transition — even partially. The science of timing is non-negotiable.
Level 1 — Verbal (Free, Immediate)
"[Name], you stopped the trains and came to dinner. That was HARD and you did it. I'm so proud of you."
Formula: Specific behaviour + acknowledgment of difficulty + specific praise — not just "good job"
Formula: Specific behaviour + acknowledgment of difficulty + specific praise — not just "good job"
Level 2 — Token Economy
Use the Rosette Imprint Reward Jar (₹589 — Amazon.in) or any jar + stickers.
"One token for completing the transition. [Drop token.] When we have 5, we [chosen reward]."
"One token for completing the transition. [Drop token.] When we have 5, we [chosen reward]."
Level 3 — Natural Reinforcement
The next activity IS the reinforcement. "First trains. THEN [something the child wants]." The completion of the First-Then board IS the reward — the "Then" delivers automatically.
Reinforce the attempt, not just the success. If the child attempted the transition and was partly successful: "You tried. That was really hard and you kept going. I noticed that."
What NOT to Do
- ✗ Withhold ALL reinforcement when child was partially compliant
- ✗ Save praise until the child is "perfectly calm"
- ✗ Say "you were so difficult today, but good job finishing"
ABA reinforcement principles: immediate, specific reinforcement increases behaviour occurrence. Token economy systems: strong evidence in autism intervention (multiple systematic reviews). BACB ethical reinforcement guidelines.

Step 6 of 6
🎯 Step 6 — The Cool-Down
Timing: 1–2 minutes post-transition. No session ends abruptly. The cool-down transitions the child from heightened alertness back to baseline. This prevents post-transition dysregulation — the "calm, then crash" pattern many families recognise and dread.
Acknowledge Completion
"We're here now. You made it." Simple, calm, matter-of-fact.
Offer Sensory Regulator
Transition object still in hand, or a brief calming input — sip of water through a straw, deep pressure on shoulders if tolerated.
Give 60 Seconds of Low Demand
Don't immediately demand participation in the next activity. Let the child arrive before starting. This gap is neurologically essential.
Material Put-Away Ritual
"The timer goes on the shelf now. It will be there for next time." [Child participates in putting materials away if developmentally appropriate]
If child refuses to put materials away:"The timer stays HERE. It will be here next time. Let's put it in its spot." — Designated permanent spot for each material resolves this consistently.
NCAEP (2020): Visual supports and transition procedures as evidence-based practices include structured ending procedures. Sensory processing research: post-activation recovery time improves generalisation of regulated states.

60 Seconds of Data Now = Months of Insight Later
Your data feeds the GPT-OS® AbilityScore® — tracking whether transition duration is decreasing, distress intensity is reducing, and which materials are most effective for YOUR child's profile. Without data, progress is invisible. With data, every week shows movement.
What to Record — 3 Fields Only
Field 1 — Duration: How many minutes did the transition take?
☐ Under 2 min ☐ 2–5 min ☐ 5–10 min ☐ Over 10 min
☐ Under 2 min ☐ 2–5 min ☐ 5–10 min ☐ Over 10 min
Field 2 — Distress Level:
☐ 1 — No distress, smooth
☐ 2 — Mild protest, manageable
☐ 3 — Moderate upset
☐ 4 — Significant meltdown
☐ 5 — Full crisis response
☐ 1 — No distress, smooth
☐ 2 — Mild protest, manageable
☐ 3 — Moderate upset
☐ 4 — Significant meltdown
☐ 5 — Full crisis response
Field 3 — What Worked:
☐ Visual Schedule ☐ Visual Timer ☐ First-Then Board ☐ Transition Object ☐ Song/Cue ☐ Countdown ☐ Social Story ☐ Calming Tool ☐ Choices
☐ Visual Schedule ☐ Visual Timer ☐ First-Then Board ☐ Transition Object ☐ Song/Cue ☐ Countdown ☐ Social Story ☐ Calming Tool ☐ Choices
Why This Data Matters
Your data feeds the GPT-OS® Transition Readiness Index, tracking whether:
- Transition duration is decreasing over time
- Distress intensity is consistently reducing
- Which materials are most effective for YOUR child's specific profile
💾 Track online: pinnacleblooms.org/start/I-786
Or download the Pinnacle Transition Tracker PDF at the same link.
Or download the Pinnacle Transition Tracker PDF at the same link.
Your 60 seconds of daily logging shapes a system that helps millions. When 50,000 families track their child's transition data, the patterns that emerge calibrate recommendations for the next family.
BACB Data Collection Standards: Frequency, duration, and intensity measurement as standard ABA practice. GPT-OS® Transition Readiness Index: tracks progression across 5 readiness stages.

Every Imperfect Session Is Data
Setbacks are not failures — they are diagnostics. Each troubleshooting scenario below is a clinical signal pointing you toward a specific adjustment, not a reason to stop.
"My child threw the visual schedule."
Why: The schedule still represents the demand, not the solution yet.
What to do: Don't react to the throw. Put it away for today. Tomorrow, introduce the schedule during a calm, non-transition moment — make it a fun activity first. The schedule must be positive before it's functional.
What to do: Don't react to the throw. Put it away for today. Tomorrow, introduce the schedule during a calm, non-transition moment — make it a fun activity first. The schedule must be positive before it's functional.
"The countdown made it WORSE."
Why: Countdowns can increase anticipatory anxiety in some children.
What to do: Switch to the visual timer only (watching it shrink is less confrontational). Or shorten from 5→3→1 to just a 60-second timer.
What to do: Switch to the visual timer only (watching it shrink is less confrontational). Or shorten from 5→3→1 to just a 60-second timer.
"Child ignored the First-Then board completely."
Why: The board isn't yet meaningful — generic images don't connect.
What to do: Use PHOTOS of your actual child doing the actual activities (not clip art). Personalisation dramatically increases engagement with visual supports.
What to do: Use PHOTOS of your actual child doing the actual activities (not clip art). Personalisation dramatically increases engagement with visual supports.
"The transition object became a distraction."
Why: Child is more interested in the object than the transition.
What to do: Reserve the object exclusively FOR transitions. It never appears at other times. Its value comes from its scarcity and its association with transition moments.
What to do: Reserve the object exclusively FOR transitions. It never appears at other times. Its value comes from its scarcity and its association with transition moments.
"We made it through, then had a meltdown 20 minutes later."
Why: Delayed release — the neurological cost of the transition emerges after the fact. Very common.
What to do: Build a 5-minute low-demand cool-down into every post-transition period (Step 6). Don't immediately demand participation in the new activity.
What to do: Build a 5-minute low-demand cool-down into every post-transition period (Step 6). Don't immediately demand participation in the new activity.
"Nothing works every time."
This is normal. No strategy works 100% of the time. The goal is improvement over time — fewer full meltdowns, shorter recovery times, increasing independence. Track across weeks, not individual sessions.
🛑Emergency Protocol: If child becomes severely distressed (self-harm, unable to breathe, complete dissociation): Stop the transition. Provide calm physical presence. Do not speak demands. Contact your therapist within 24 hours. Immediate safety concern: 9100 181 181.
ABA functional analysis principles applied to session-level problem solving. Pinnacle clinical troubleshooting database from 70+ centers.
Your Child Is Not a Template
The 9 materials are evidence-based starting points. Your child's sensory profile, communication level, and age determine how you configure them. Here is how to adapt for the profiles most commonly seen in clinical practice.
For the Sensory Seeker
Make transitions ACTIVE. Movement IS the transition. "Time to hop to the kitchen." Physical movement between activities reduces resistance significantly for sensory seekers.
For the Sensory Avoider
Use quieter, less stimulating materials. Soft verbal cues, not bells. Muted colour schedules. Transition objects should be calming-textured, not stimulating.
For the Language-Limited Child
Remove all verbal explanations from the transition. Only the visual material speaks. Hand visual, point, wait. Silent, predictable, visual-only transitions.
For the Language-Strong Child
Co-create the schedule WITH the child each morning. "What are we doing today? Let's put your pictures up." Agency in building the schedule = investment in following it.
For the Anxiety Profile
Maximum predictability above all else. Never change the transition sequence without warning. Add a "surprise change" slot to the schedule for days when unexpected changes occur.
Age-Based Modifications
Ages 2–4
Single-image First-Then boards only. Real photos of child. No words. Keep every visual as simple as possible.
Ages 5–7
Full daily visual schedule. Introduce countdown verbals alongside visual timer. Begin building language around transitions.
Ages 8–10
Child manages their own visual schedule. Social stories written BY the child about THEIR transitions. Agency leads to mastery.
OT sensory profile-based adaptation. ABA function-based individualisation. SLP communication-profile-based modification. Pinnacle GPT-OS® TherapeuticAI® personalisation engine.
Progress Arc — Week 1–2
Week 1–2: Tolerance, Not Mastery
15%
Progress Stage
Week 1–2 position on the journey to full transition mastery
✓ What "Progress" Looks Like
- Transition DURATION begins to decrease — even 15 min to 12 min counts
- Child begins LOOKING at the visual schedule or timer, even briefly
- Verbal protest without physical escalation (an improvement from physical)
- One transition per day with noticeably less distress than before
- Child no longer fights the transition OBJECT — accepts carrying it
✗ What Is NOT Progress Yet (Normal)
- Child still protests verbally — expected
- Not all transitions are smooth — expected
- Some days are worse than others — fatigue, illness, novelty all increase difficulty
- Child doesn't seem to "understand" the schedule yet — trust the process
"In weeks 1–2, the work you are doing is building the neural scaffold — laying down the pathways your child's brain will eventually use automatically. You won't see the scaffold. You'll see the house it builds in weeks 3–8. Keep going."
Patience Metric: If your child's transition time has decreased by even 2 minutes, or their distress intensity has dropped by even one point on the scale — you have evidence of progress. Log it.
PMC11506176: Sensory and behavioural intervention outcomes emerge across 8–12 week timelines. Early-phase indicators focus on tolerance and participation rather than mastery.
Progress Arc — Week 3–4
Week 3–4: The Neural Pathways Are Forming
40%
Progress Stage
Week 3–4 consolidation — the neural pathways are actively strengthening
Consolidation Indicators to Watch For:
Anticipation
Child turns to look for the schedule BEFORE you point to it — the framework is becoming internal
Shorter Protests
Protest duration decreases — if it used to last 10 minutes, now 4 minutes
Board Engagement
First-Then board being engaged with — child points or acknowledges both steps
Cue Response
Transition songs/cues triggering a visible behavioural shift — child begins winding down when they hear the cue
The "Spontaneous Generalisation" Sign:"My child asked 'what's next?' before I showed the schedule." This is the first sign of internalisation. The child's brain has begun using the same framework internally that the visual schedule provides externally. This is the neural pathway forming.
When to increase support intensity: If Week 3–4 shows NO improvement on any indicator, the current support level or material choice may not match the child's profile. This is the right moment to book a teleconsultation — not to give up, but to calibrate.
Neuroplasticity research: synaptic strengthening through repeated structured input follows predictable timelines in paediatric populations. Behavioural consolidation markers align with neural adaptation research.

Progress Arc — Week 5–8
Week 5–8: Mastery Is Close. Here's How You Know.
75%
Progress Stage
Week 5–8 mastery markers — measurable, observable, specific
Mastery Criteria — Specific, Observable, Measurable
Duration Mastery
Most (>70%) transitions completed within expected duration WITHOUT major distress
Spontaneous Use
Child independently reaches for or points to transition support material — unprompted
Verbal Only
Verbal protest present but NOT physical — and protest duration under 2 minutes consistently
Generalisation
Transition support working at SCHOOL or other settings, not just home
Self-Regulation
Child beginning to use calming tool mid-transition WITHOUT being prompted
Generalisation Check
A child who transitions smoothly at home but has meltdowns at school has not yet generalised. This is normal — it requires active cross-setting implementation. School receives the same visual supports your home uses.
Maintenance Check
Take one day per week with REDUCED support (just verbal countdown, no visual materials). Does the transition still go better than Week 1? Yes = maintenance confirmed.
🏅TRANSITION READINESS MILESTONE UNLOCKED
This child has moved from severe transition challenges to emerging/functional transition ability on the GPT-OS® Transition Readiness Index.
This child has moved from severe transition challenges to emerging/functional transition ability on the GPT-OS® Transition Readiness Index.
PMC10955541: Mastery criteria derived from behavioural measurement standards. BACB mastery criteria: 80% accuracy across 3 consecutive sessions.

You Did This. Your Child Grew Because of You.
Not "good job" — but an honest accounting of what you actually did.
You chose, through exhaustion and doubt, to show up with a visual timer instead of an ultimatum. You sang the same clean-up song on the days it worked and the days it didn't. You handed the transition object before the meltdown, not during it. You logged the data when you would rather have sat down. You learned, applied, adjusted, and reapplied.
This is what evidence-based parenting looks like from the inside.
✓ Duration Decreased
Your child's transition time has measurably shortened
✓ Intensity Reduced
Meltdown intensity has dropped — fewer crises, shorter recoveries
✓ Anticipation Emerging
Your child has begun to anticipate, not just react
✓ Safety Created
You've built a predictable, safe transition experience — possibly for the first time in your child's life
🌟Family Celebration Suggestion: Create a Transition Victory Board — a visible chart showing weekly progress. Let your child add a sticker each week. Make the progress visible to them too.
Journal Prompt: "Write down one specific moment from this 8-week journey that you want to remember. The moment you knew something was shifting."
Parental self-efficacy research: parent confidence is the strongest predictor of continued home-based intervention adherence. Pinnacle outcome data: families who celebrate milestones show 3× higher continuation rates.
6 Signs to Pause and Seek Professional Guidance
Consistent home practice is powerful — and professional support is the escalation layer that makes it sustainable. Know these six signals so you can act early, not after the crisis deepens.
🚩 1. Self-Harming During Transitions
Head-banging, biting self, scratching — beyond occasional frustration gestures. This indicates dysregulation exceeding what these strategies can address alone.
🚩 2. Zero Improvement After 6 Weeks
If no indicator has moved after 6 weeks of consistent implementation, the technique needs professional calibration — not more parental effort.
🚩 3. Transition Difficulty Spreading
Child was okay with some transitions but now all transitions are crisis-level — could indicate an emerging anxiety component or environmental change trigger.
🚩 4. Significant Regression After Improvement
Common during illness or major life change, but if persistent beyond 2 weeks post-trigger, professional review is indicated.
🚩 5. Sleep Disruption + Transition Difficulty Together
The combination suggests nervous system dysregulation beyond transition-specific intervention.
🚩 6. School Refusal or School-Based Deterioration
Transition difficulty is now impacting education and requires school-clinic coordination.
Mild Concern
Monitor 1 week → Teleconsultation
Moderate Concern
Teleconsultation within 3 days → Possible centre visit
Significant Red Flag
Centre appointment within 1 week
Immediate (Self-Harm/Safety)
Call 9100 181 181 now
WHO NCF: Primary health care as platform for early identification. Pinnacle clinical escalation protocols — 70+ centres.
You're Not Done. You're on a Journey.
I-786 is one technique in a carefully sequenced domain. Where you go next depends on how your child responded — and the path forward is already mapped.
Path A — Visual Supports Excelled
→ I-787 Environmental Transitions
Visual schedule scaling to community settings — the natural next frontier.
Visual schedule scaling to community settings — the natural next frontier.
Path B — Sensory/Calming Tools Dominant
→ Domain A: Sensory Processing
Deeper regulation work that will improve all transitions across every domain.
Deeper regulation work that will improve all transitions across every domain.
Path C — Anxiety Prominent
→ Coordinate with Pinnacle Psychologist for anxiety management integrated with transition strategies. Anxiety and transition difficulty have a bidirectional relationship that requires both lenses simultaneously.
Long-Term Goal
Full independent transition management → school participation → community independence → occupational participation in adolescence and adulthood.
WHO developmental milestones framework. GPT-OS® 12-domain progression architecture. Evidence-based developmental cascade sequencing.
One Technique. One Domain. One Piece of a Complete Picture.
"A child who cannot manage transitions will also struggle with social situations (which are constantly transitioning), emotional regulation (which requires shifting emotional states), and learning (which requires shifting between topics and tasks). Transition mastery is not one skill — it is the keystone for many others."
Current Domain Status
Domain D: Behavioral Flexibility — Activity Changes (I-786) is your active technique. This domain feeds directly into: Social Communication (B), Emotional Regulation (C), and Adaptive Behavior (I).
GPT-OS® AbilityScore® Assessment
See your child's full developmental profile across all 12 domains. Request an AbilityScore® assessment to understand which domains are developing on track and where targeted support will have the greatest cascade effect.
Or call 9100 181 181
WHO Nurturing Care Framework: Five components require holistic developmental monitoring. UNICEF 2025 Country Profiles: 42 cross-domain indicators.

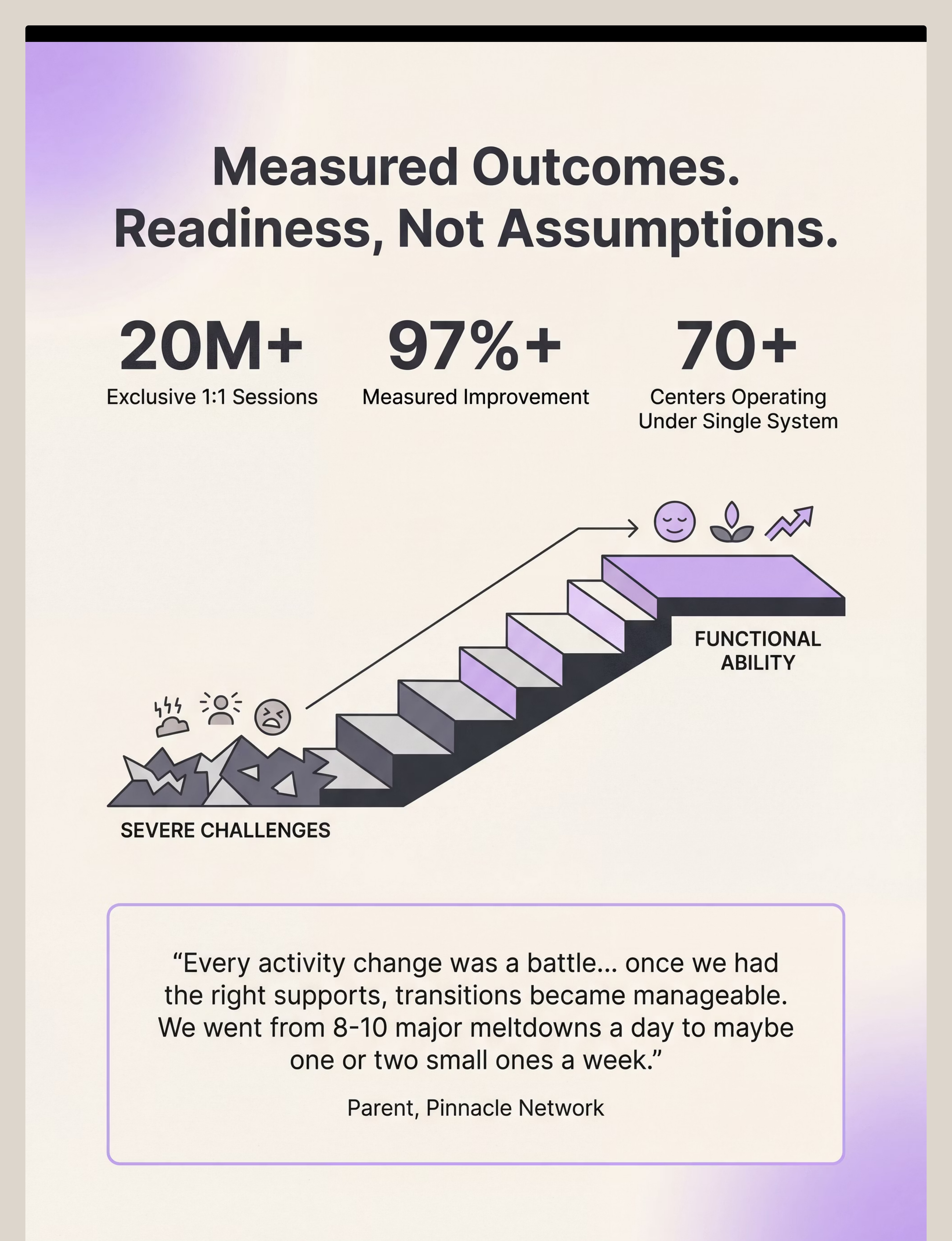
From Battleground to Manageable: Real Families, Real Progress
Arjun, Age 5 — Hyderabad
Before: Every screen-time ending triggered 45 minutes of screaming. Family dreaded transitions so severely they avoided outings entirely. Arjun's transition difficulty was ranked at Stage 1 (severe) on GPT-OS® Transition Readiness Index.
8 Weeks Later: Visual timer introduced from Day 1. By Week 3, Arjun began watching the timer voluntarily. By Week 6, he was reminding his mother to "set the timer." Current status: Stage 4 (emerging independence). Screen time transitions now under 3 minutes.
"The timer didn't just help Arjun — it helped me. I stopped dreading transitions because I had a system. The system being there made me calmer, which made him calmer."
From the Therapist's Notes: Arjun's case demonstrates the bidirectional effect of transition supports — parent regulation improves alongside child regulation when a consistent system reduces uncertainty for both parties.
Kavya, Age 7 — Bangalore
Before: Morning routine taking 90+ minutes. Late to school daily. Kavya's teachers reporting extreme distress at every classroom transition. Family considering pulling her from school.
12 Weeks Later: Visual schedule created with Kavya's own photos. First-Then boards deployed for school transitions. Teacher trained on same protocol. By Week 8: morning routine under 40 minutes.
"I didn't believe a picture on a board could change our mornings. I was wrong. The picture board changed everything."
"She still needs the board, but she uses it herself now." — Kavya's teacher, Week 12
Qualitative research on parent motivation: peer narratives are the strongest motivator for continued home-based intervention adherence. Pinnacle center outcome data across 70+ centres.

You Are Not Doing This Alone
Isolation is the most common — and most harmful — experience for parents navigating transition difficulty. Parents who connect with others navigating the same challenge show measurably higher intervention adherence and lower burnout. Community is not optional — it is clinical.
📱 Pinnacle WhatsApp Community
Flexibility & Transitions Group — Parents navigating activity changes, morning routines, and transition meltdowns. Share, ask, and support in real time.
Join → pinnacleblooms.org/community
Join → pinnacleblooms.org/community
💬 Online Forum: Pinnacle Parent Community
Moderated by Pinnacle therapists. Evidence-based discussion, parent-to-parent support, technique questions answered by clinicians in real time.
Forum → pinnacleblooms.org/forum
Forum → pinnacleblooms.org/forum
🤝 Peer Mentoring Programme
Connect with a parent who is 6–12 months ahead of you on the same journey. Ask what you can't ask the therapist. Share what only a fellow parent can understand.
Request a Mentor → pinnacleblooms.org/peer-mentor
Request a Mentor → pinnacleblooms.org/peer-mentor
"If this technique page has helped your family, share your story. Your journey — anonymised — can become the testimonial that gives another parent the courage to begin."
WHO NCF: Community engagement as core principle. Parent support network literature: community belonging improves intervention outcomes and reduces parental burnout.
Home + Clinic = Maximum Impact
Home-based intervention is powerful. Home-based intervention supported by a professional team is transformational. The Pinnacle network provides the clinical backbone that makes your home practice sustainable and escalatable when you need the next level of support.
📞 FREE National Autism Helpline
9100 181 181
16+ languages | 24×7
"Not sure where to start? Start here."
16+ languages | 24×7
"Not sure where to start? Start here."
💻 Teleconsultation
Speak with a Pinnacle OT/ABA/SLP from home — no travel required.
Book → pinnacleblooms.org/book
Book → pinnacleblooms.org/book
🏥 70+ Centres Across India
In-person assessment and therapy at your nearest centre.
Find Nearest → pinnacleblooms.org/centres
Find Nearest → pinnacleblooms.org/centres
Discipline Matching for This Technique: For activity changes + transitions, your primary specialist is an Occupational Therapist (environmental + sensory regulation), supported by a BCBA/ABA Therapist (behavioural framework) and a Special Educator (school coordination).
WHO NCF Progress Report (2023): 48% increase in countries adopting ECD policies. Primary health care as key platform for reaching all families.

For the Parent Who Wants to Go Deeper
Every recommendation in this guide traces to a specific research source. Here is the evidence base — from systematic reviews at the top of the evidence pyramid to expert consensus frameworks at the base.
Study | Finding | Link | |
PRISMA Review (Children, 2024) | Visual supports + antecedent strategies confirmed evidence-based practice for ASD across 16 studies | ||
Meta-analysis (World J Clin Cases, 2024) | Structured behavioural supports effectively promote adaptive behaviour and flexibility in 24 studies | ||
WHO/UNICEF CCD Package (2023) | Home-based structured interventions implemented across 54 LMICs with proven outcomes | ||
Padmanabha et al., Indian J Pediatr (2019) | Home-based structured interventions significant in Indian paediatric population | ||
NCAEP (2020) | Visual supports + antecedent-based interventions confirmed evidence-based for autism | ||
Journal of Autism & Developmental Disorders | Ongoing indexed research on transition supports and cognitive flexibility |
Evidence grading: Oxford Centre for Evidence-Based Medicine (OCEBM) levels. WHO NCF | NCAEP EBPs

Your 60 Seconds of Daily Data Shapes a System That Helps Millions
Every time you log a transition, your data contributes to a pattern-recognition system that refines recommendations for thousands of families. Your 60 seconds of daily logging has a reach far beyond your own home.
What GPT-OS® Learns from I-786 Data
- Which of the 9 materials shows the fastest response in this child's profile
- Whether visual, auditory, or tactile supports are dominant for this child
- The child's baseline transition duration and rate of improvement
- Predicted week of mastery based on individual response curve
🔒 Privacy Assurance
Your data is protected under Indian Data Protection frameworks and Pinnacle's clinical privacy standards. Population-level insights are anonymised and aggregated. Your family's data is never individually identifiable in research outputs.
"When 50,000 families track their child's transition data, the patterns that emerge help calibrate the recommendations for the 51st family. Your data helps children you will never meet."
Digital health ASD interventions: 21 RCTs, 1,050 participants per 2024 meta-analysis showing gamified digital tracking improves adherence. GPT-OS® Closed-Loop Therapeutic Control architecture.

See the 9 Materials in Action
Watching is different from reading. For parent skills — demonstrating beats explaining. The reel shows you exactly what correct use looks like, what child response to expect, and how to troubleshoot in real time. Video + written protocol together give you the complete picture.
🎬 Reel I-786 Details
Title: 9 Materials That Help With Activity Changes
Series: Flexibility & Transitions | Episode 786
Duration: 60–75 seconds
Domain: BEH-TRANS | Behavioral Flexibility
Series: Flexibility & Transitions | Episode 786
Duration: 60–75 seconds
Domain: BEH-TRANS | Behavioral Flexibility
Therapist Introduction
In this reel, our Pinnacle OT and BCBA specialists walk through each of the 9 materials you've just read about — showing you exactly what correct use looks like, what child response to expect, and how to troubleshoot in real time.
"Read this page for the science and depth. Watch the reel for the implementation. Together they are the complete learning experience."
Video modelling is classified as an evidence-based practice for autism by NCAEP (2020). Multi-modal learning (visual + text + demonstration) improves parent skill acquisition across all education research.
Consistency Across Every Caregiver Multiplies Impact
A visual schedule that exists only when you're home is half a visual schedule. The research is clear: cross-caregiver consistency is among the strongest predictors of transition improvement. This card makes it easy to share the same knowledge with everyone who matters.
Share with Family
Send via WhatsApp or email — bring grandparents, relatives, and babysitters into the same system.
📱 Share via WhatsApp | 📧 Share via Email
📱 Share via WhatsApp | 📧 Share via Email
📄 Download Family Guide (1-Page PDF)
A simplified version of the 9 materials for family members, babysitters, and extended family. Everything they need to know on one printable page.
👵 Explain to Grandparents Version
"Why isn't Rohit just behaving?" — A grandfather-friendly explanation of why transitions are hard and what to do. Warm, non-clinical, respectful of generational perspectives.
🏫 Teacher Communication Template
A ready-to-send message to school requesting the same transition supports used at home. Cross-setting consistency is critical — this template makes advocating easy.
"Our child struggles with activity changes because of how their brain processes the shift from one thing to another. We've learned that visual schedules, timers, and consistent transition routines help enormously. Here's what we do — and what we're asking everyone to do too."
WHO CCD Package: multi-caregiver training as critical for intervention generalisation and maintenance. PMC9978394.

Questions Parents Actually Ask
These are real questions from real families navigating the same journey. If your answer isn't here, the resources at the bottom of this card will connect you with a clinician directly.
Q1: How long before I see results?
Most families see measurable improvement in transition duration within 2–3 weeks of consistent implementation. Full reduction in distress intensity typically emerges by weeks 4–6. Complete mastery at weeks 8–12 for many children, though individual profiles vary considerably.
Q2: My child refuses to look at the visual schedule.
Don't use it FOR transitions at first. Spend 3–5 days making the visual schedule a fun activity — let the child help choose pictures, decorate it, point to pictures. The schedule must have positive associations before it functions as a transition tool.
Q3: Do I need all 9 materials?
No. Start with 1–2 that feel most natural for your child's profile. The visual timer alone has transformed thousands of families' mornings. Add materials one at a time as you see results.
Q4: My child's school doesn't use these strategies.
Download the Teacher Communication Template from the previous card. Schedule a meeting with the class teacher and special educator. Request that the same First-Then board and visual timer be used at school transition times. Advocate for cross-setting consistency.
Q5: Is this just for autism?
No. Transition difficulty is documented in ADHD, anxiety disorders, developmental delays, sensory processing differences, and in neurotypical children during early childhood. These strategies benefit any child who struggles with activity changes.
Q6: We had a terrible week after doing well. Did we lose progress?
No. Regression during illness, major changes, or high-stress periods is normal and expected. The neural pathways are still there. Return to full support for a week and progress will usually re-establish within days, not weeks.
Q7: When should I stop using the visual schedule?
When your child transitions successfully WITHOUT the schedule for 2+ consecutive weeks. Fade it gradually — try alternate days, then every few days. Never remove it abruptly. The goal is a child who has internalised the structure, not one who simply lacks access to support.
Q8: I didn't find my answer here.
Ask GPT-OS® → | Book Teleconsultation → | Call FREE Helpline: 9100 181 181

You Have Everything You Need. Start Today.
Your child's next successful transition is one strategy away.
🚀 Start This Technique Today
GPT-OS® Guided Session Launcher — your personalised protocol begins here
📞 Book a Consultation
Speak with a Pinnacle Transition Specialist — centre visit or teleconsultation available
🗺 Explore the Next Technique
Ready for the next level? I-787: Environmental Transitions — visual schedule scaling to community settings
🔵"Clinically validated by the Pinnacle Blooms Consortium — OT • SLP • ABA/BCBA • SpEd • NeuroDev Paediatrics • WHO/UNICEF Aligned • India's Largest Autism Therapy Network"
OT
ABA
SLP
SpEd
NeuroDev
FREE HELPLINE: 9100 181 181 | 16 languages | 24×7
Preview of 9 materials that help with activity changes Therapy Material
Below is a visual preview of 9 materials that help with activity changes therapy material. The pages shown help educators, therapists, and caregivers understand the structure and content of the resource before use. Materials should be used under appropriate professional guidance.









Link copied!

The Pinnacle Promise
"From fear to mastery. One technique at a time."
Pinnacle Blooms Network® exists to transform every home into a 24×7, personalised, multi-sensory, multi-disciplinary, integrated therapy environment — for every child, regardless of geography or economic status. GPT-OS® powers 70,000+ evidence-linked techniques, 20 million therapy sessions, and 97%+ measured improvement across one unified clinical system.
🔵 OT
Occupational Therapy
🟢 SLP
Speech-Language Pathology
🟣 ABA/BCBA
Applied Behaviour Analysis
🟡 SpEd
Special Education
🔴 NeuroDev
Neurodevelopmental Paediatrics
Medical Disclaimer: This content is educational. It does not replace individualised assessment and intervention from qualified occupational therapists, behavioural therapists, psychologists, or special educators. Transition difficulties vary significantly based on individual profile and underlying conditions. Consult your child's therapy team for personalised recommendations. Individual results may vary. Statistics represent aggregate outcomes across the Pinnacle Blooms Network.
Contact & Legal
pinnacleblooms.org | care@pinnacleblooms.org | 9100 181 181
© 2025 Pinnacle Blooms Network®, unit of Bharath Healthcare Laboratories Pvt. Ltd. All rights reserved. GPT-OS® is a registered system.
© 2025 Pinnacle Blooms Network®, unit of Bharath Healthcare Laboratories Pvt. Ltd. All rights reserved. GPT-OS® is a registered system.
CIN: U74999TG2016PTC113063 | DPIIT: DIPP8651 | MSME: Udyog Aadhaar TS20F0009606 | GSTIN: 36AAGCB9722P1Z2