
When Backward Feels Like Falling
Vestibular Backward Tilt Distress — Home Intervention Protocol A-087 | Sensory Solutions Series | Pinnacle GPT-OS®
"Bath time is a nightmare. It's not the water — my daughter loves water. It's the moment I try to tilt her head back to rinse her hair. The second her head goes backward even a little, she screams like she's being hurt. Her whole body goes rigid. She grabs onto me so hard her nails dig in. Tears streaming, absolute terror in her eyes. I'm just trying to wash shampoo out of her hair. But to her, it's like I'm dropping her off a cliff."
You are not failing. Your child's vestibular system is sending a false alarm — and there is a proven path to recalibrate it.
Sensory Processing
Vestibular System
Daily Living Skills
Ages 1–10
Home Protocol
Pinnacle Blooms Network® — Validated by CRO • OT • SLP • ABA • SpEd • NeuroDev Consortium
WHO Nurturing Care Framework (2018): Early identification and parental awareness of developmental challenges directly impacts outcomes across all domains. Reference: https://nurturing-care.org/ncf-for-ecd/

You Are Not Alone
Gravitational insecurity is a recognised clinical phenomenon — not a behavioural problem, not a phase, not something your child will simply outgrow without intervention. It is a vestibular processing difference where the brain's position-sensing system sets its 'falling alarm' too sensitively. It is real. It is neurological. And it is addressable.
80%
Sensory Difficulties in Autism
Of children diagnosed with autism display sensory processing difficulties — vestibular sensitivity is among the most common and most disruptive. (PRISMA Systematic Review, 2024)
1 in 6
Gravitational Insecurity
Children with sensory processing differences experience specific gravitational insecurity — disproportionate fear of head position changes including backward tilt. (SPD Foundation Research)
Millions
Families Worldwide
Navigate this exact challenge — the screaming at hair washing, the dental chair meltdowns, the playground avoidance. You are among millions. (WHO/UNICEF Data)
Across Pinnacle Blooms Network's 70+ centres, vestibular hypersensitivity including backward tilt intolerance is identified in a significant proportion of children presenting with sensory processing concerns. The GPT-OS® Diagnostic Intelligence Layer captures this through 591+ structured observations.
References: PMC11506176 | PMC10955541 | DOI: 10.12998/wjcc.v12.i7.1260

The Terror Is Real. The Danger Isn't.
Understanding what is happening inside your child's nervous system transforms how you respond — and how effectively you can help.

The Vestibular System — Your Child's Internal GPS
Deep inside your child's inner ear, tiny fluid-filled canals and gravity-sensing organs constantly monitor head position and movement. This vestibular system answers the most fundamental question the brain asks: "Where am I in space? Am I upright? Am I falling?"
What Happens Normally
When a typically-developing child tilts their head backward, the vestibular system registers the position change and the brain processes it automatically: "Head is tilted. I'm supported. All is well." No alarm. No fear. Hair gets washed, dental chairs recline, playground swings swing.
What Happens in Gravitational Insecurity
In your child's brain, the vestibular system's alarm threshold is set too low. The exact same backward tilt that another child barely notices triggers a full "FALLING!" alarm. The brain sends emergency signals: release stress hormones, tense all muscles, grab onto something, SCREAM. Your child is executing a genuine emergency response to a danger that their brain — not their imagination — perceives as real.
This IS
A neurological processing difference. A wiring variation in the vestibular system. A genuine fear response. A recalibratable system — with the right approach.
This is NOT
A behaviour choice. An attention-seeking strategy. A phase they'll grow out of. Defiance or manipulation.
Clinical Term: Gravitational Insecurity / Vestibular Hypersensitivity / Postural-Vestibular Fear Response | Domain Code: SENS-VEST-GRAV
Reference: DOI: 10.3389/fnint.2020.556660

Your Child's Position on the Developmental Map
Backward tilt distress can emerge at any point in early childhood — but knowing where your child sits on the developmental timeline helps you understand what you're seeing and what to expect from intervention.
Birth – 6 Months
Primitive vestibular reflexes (Moro reflex). Early signs: extreme startle to position changes, resistance to reclined positions.
1 – 2 Years
Walking establishes upright as "home base." Gravitational insecurity becomes visible: resistance to playground equipment, avoidance of reclining, hair washing difficulties begin.
2 – 4 Years ← Most Commonly Identified
Language allows the child to express fear. Anticipatory anxiety develops. Hair washing, dental visits, and medical exams become increasingly difficult.
With Intervention
The vestibular system is plastic — it can recalibrate through controlled, supported exposure. The earlier intervention begins, the more responsive the system. Improvement is possible at any age within this range.
Backward tilt distress commonly co-occurs with other sensory processing differences, general anxiety, autism spectrum conditions, and developmental coordination challenges. Understanding the full profile guides intervention.
References: PMC9978394 | WHO/UNICEF CCD Package (2023)

Clinically Validated. Home-Applicable. Parent-Proven.
Level I–II Evidence
Systematic Review Evidence (2024)
A PRISMA-model systematic review analysing 16 articles from 2013–2023 confirms that sensory integration intervention meets criteria to be considered evidence-based practice for children with autism spectrum disorder, encompassing graduated vestibular exposure. Source: PMC11506176
Meta-Analysis Evidence (2024)
A comprehensive meta-analysis of 24 studies published in World Journal of Clinical Cases confirms that sensory integration therapy effectively promotes social skills, adaptive behaviour, sensory processing, and motor skills. Vestibular-specific interventions showed particular efficacy for positional tolerance. Source: PMC10955541
Indian Clinical Evidence (2019)
A randomised controlled trial published in Indian Journal of Pediatrics demonstrated significant outcomes for home-based sensory interventions administered by trained parents, establishing the evidence base for parent-executed protocols in the Indian paediatric population. Source: Padmanabha et al., DOI: 10.1007/s12098-018-2747-4
Pinnacle Real-World Evidence
Across 20M+ exclusive 1:1 therapy sessions, Pinnacle Blooms Network has documented 97%+ measured improvement rates across sensory processing and vestibular challenges. Vestibular tolerance progression is tracked within the GPT-OS® Sensory Processing Index and Daily Living Skills Index.

Graduated Vestibular Desensitisation for Backward Tilt Tolerance
Parent-Friendly: "Building Trust Between Your Child's Brain and Backward Movement"
This intervention is a systematic, graduated approach to recalibrating your child's vestibular system so that backward tilt — the position change that currently triggers panic — gradually becomes tolerable, then manageable, then unremarkable.
Controlled Vestibular Exposure
Using therapy balls, swings, and wedges to introduce backward tilt in tiny, safe increments that the vestibular system can process without triggering full alarm.
Proprioceptive Grounding
Using weighted products, compression, and vibration to calm the nervous system during vestibular challenges — telling the body "you are safe, you are held."
Daily-Life Accommodation
Using bath supports and visual anchors to make necessary activities possible while the vestibular system recalibrates over weeks and months.
Session Details
Age Range: 1–10 years
Session Duration: 10–20 minutes (home sessions)
Frequency: 3–5x per week
Setting: Home + Therapy + Medical/Dental
Canon Materials
- Therapy Balls
- Platform Swings
- Weighted Products
- Vibrating Tools
- Bath Supports
- Incline Wedges
- Visual Anchors
- Compression Wraps
- Progression Protocols

A Consortium Approach — Because the Brain Doesn't Organise by Therapy Type
Vestibular processing connects to balance, coordination, anxiety, daily living skills, and social participation. When Pinnacle's consortium designs the intervention, each discipline contributes its unique lens. This is FusionModule™ in action.
There was an error generating this image
Occupational Therapist (Sensory Integration Specialist) — Lead
Designs the vestibular desensitisation hierarchy — identifying the child's exact threshold for backward tilt tolerance and creating the graduated exposure plan. Determines which materials to use, in what order, and how fast to progress.
There was an error generating this image
Paediatric Neurologist / Neurodevelopmental Paediatrician
Rules out medical causes (inner ear pathology, vestibular nerve issues) and provides the diagnostic framework. Confirms gravitational insecurity as neurological, not behavioural.
There was an error generating this image
Board Certified Behaviour Analyst (BCBA)
Designs the reinforcement system for vestibular exposure sessions, creates the data collection framework, and applies systematic desensitisation principles to ensure tolerance is shaped through reinforcement — never forced compliance.
There was an error generating this image
Special Educator
Adapts classroom and school activities requiring positional changes. Coordinates with teachers for dental health visits, PE activities, and playground participation to ensure vestibular accommodations generalise across settings.
Reference: DOI: 10.1080/17549507.2022.2141327

Precision Targeting — Not a Random Activity, a Calibrated Tool
Every element of this protocol is aimed at specific, measurable outcomes. Understanding what you're targeting helps you recognise progress — even when it comes in small, quiet steps.
Primary Target
Child tolerates head-below-heart positions and backward tilt during functional activities (hair washing, dental recline, medical exams) without panic response.
Observable indicator: Backward tilt of 30°+ tolerated with mild or no distress for 30+ seconds.
Why Tertiary Targets Matter
When a child's vestibular alarm quiets, the ripple effects are profound. Swings become possible. Playground friendships form. Hair washing stops being a daily trauma. The parent-child relationship heals. Every ring of the bullseye represents a dimension of your child's daily life that will improve.
Reference: PMC10955541

Your 9 Materials — The Vestibular Trust-Building Toolkit
These nine materials form the complete evidence-based toolkit for backward tilt desensitisation. Each is mapped to the Pinnacle 128 Canon Materials system and validated across 20M+ therapy sessions. You do not need all nine to start — see the essential starter kit below.
1
Therapy Ball / Peanut Ball
Canon: Vestibular Equipment | Price: ₹800–2,500
Controlled, gradual backward tilt with constant support. Foundational tool. Start here.
2
Platform Swing With Sides
Canon: Vestibular Equipment | Price: ₹3,000–15,000
Safe containment + controlled vestibular movement. The child can't fall out — containment IS the therapy.
3
Weighted Products
Canon: Proprioceptive Equipment | Price: ₹1,500–6,000
Deep pressure grounding — "you're anchored, not falling." Use BEFORE and DURING vestibular exposure.
4
Vibrating Tools and Cushions
Canon: Proprioceptive Equipment | Price: ₹500–3,000
Organising proprioceptive input that modulates vestibular alarm. Test first — some children love vibration, some don't.
5
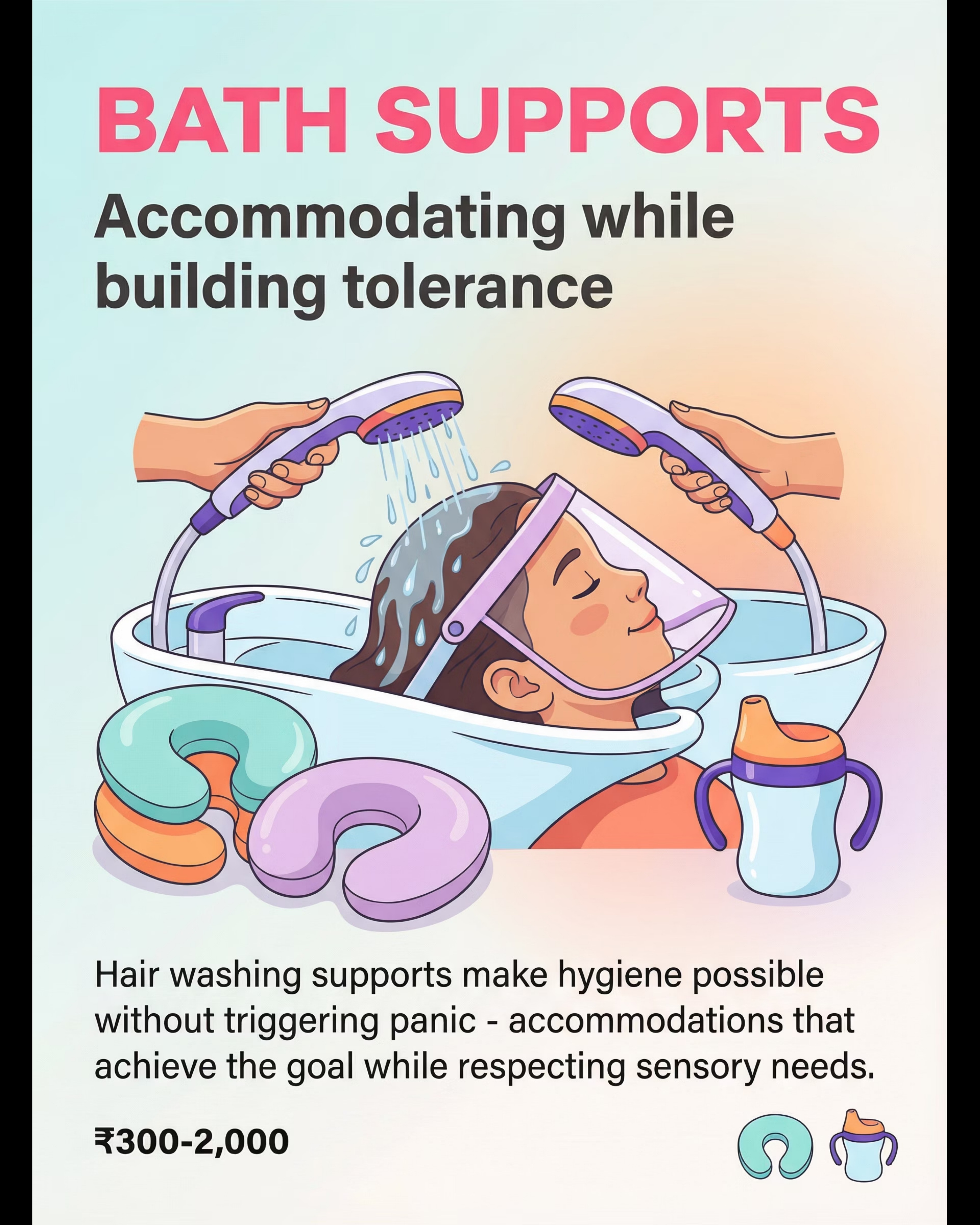
Bath and Hair Washing Supports
Canon: Daily Living Accommodations | Price: ₹300–2,000
Make hygiene possible without triggering panic. Accommodate daily needs. Do vestibular therapy separately.
6
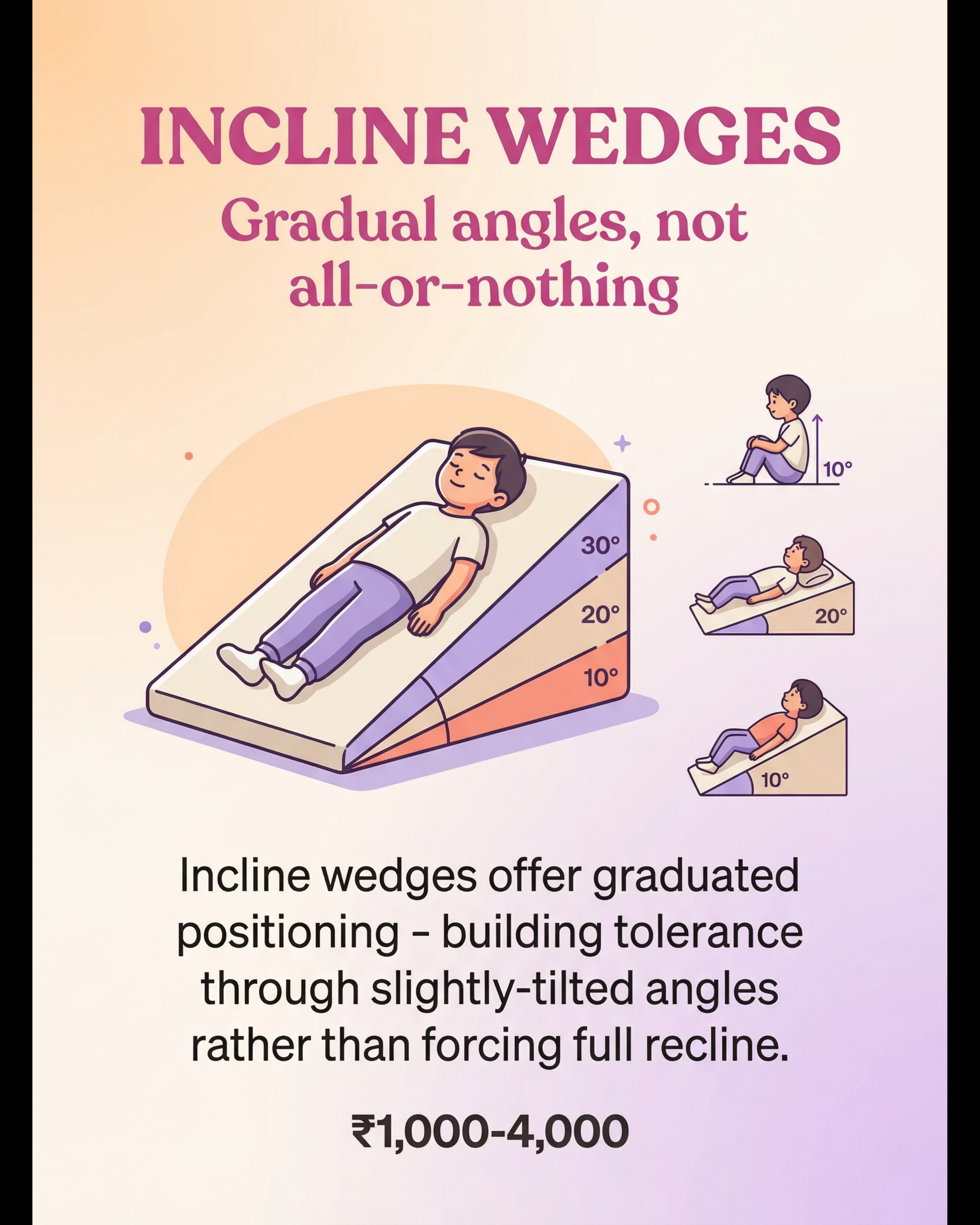
Incline Wedges and Positioning Supports
Canon: Positioning Equipment | Price: ₹1,000–4,000
Graduated angles — not all-or-nothing recline. From almost-upright to almost-flat, in weeks of tiny steps.
1
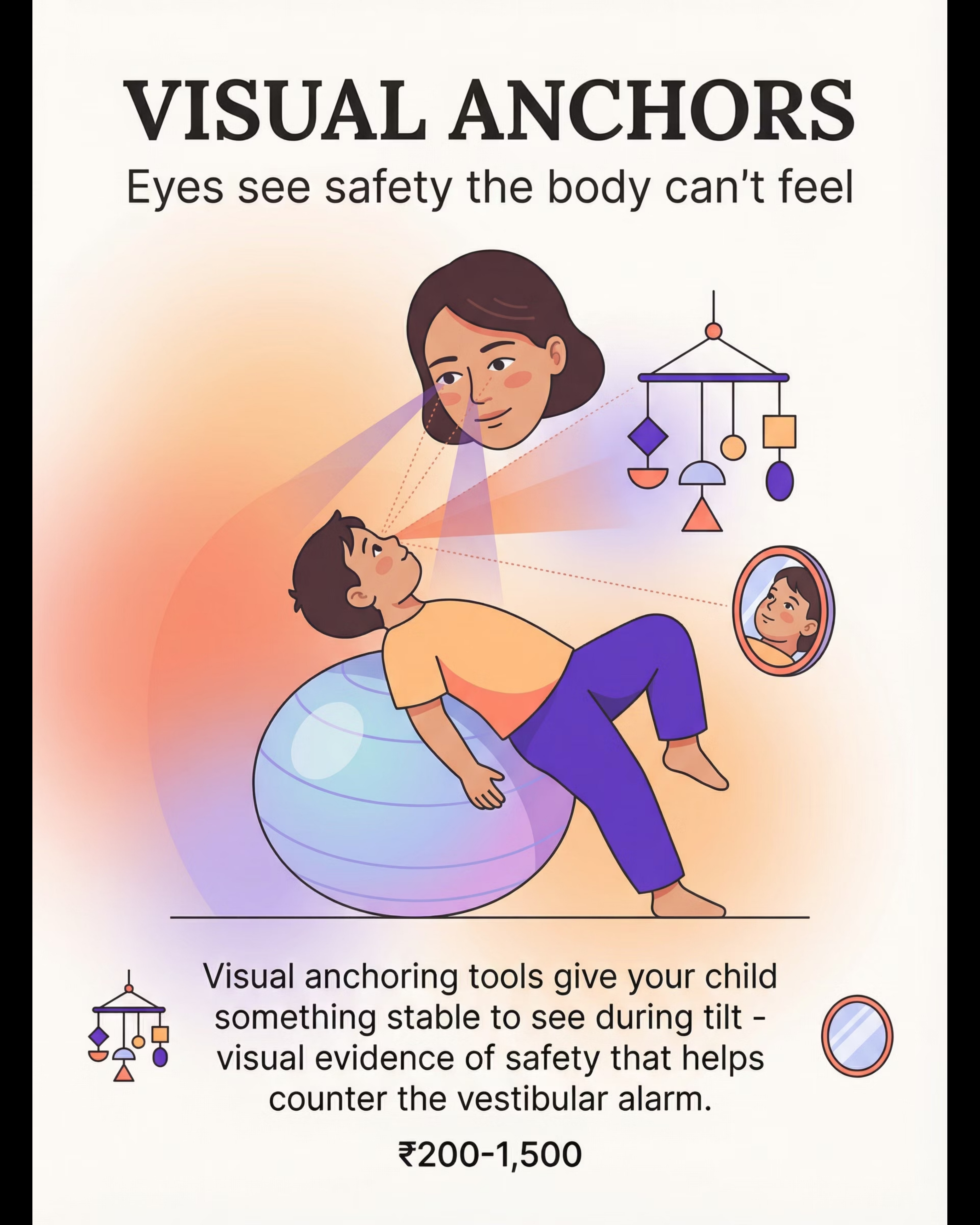
Visual Anchoring Tools
Canon: Visual Supports | Price: ₹200–1,500
Eyes see safety the body can't feel. Your face is the most powerful visual anchor.
2
Compression and Proprioceptive Wraps
Canon: Proprioceptive Equipment | Price: ₹800–3,500
Containing pressure that grounds during position changes. The child feels held even when the world tilts.
3
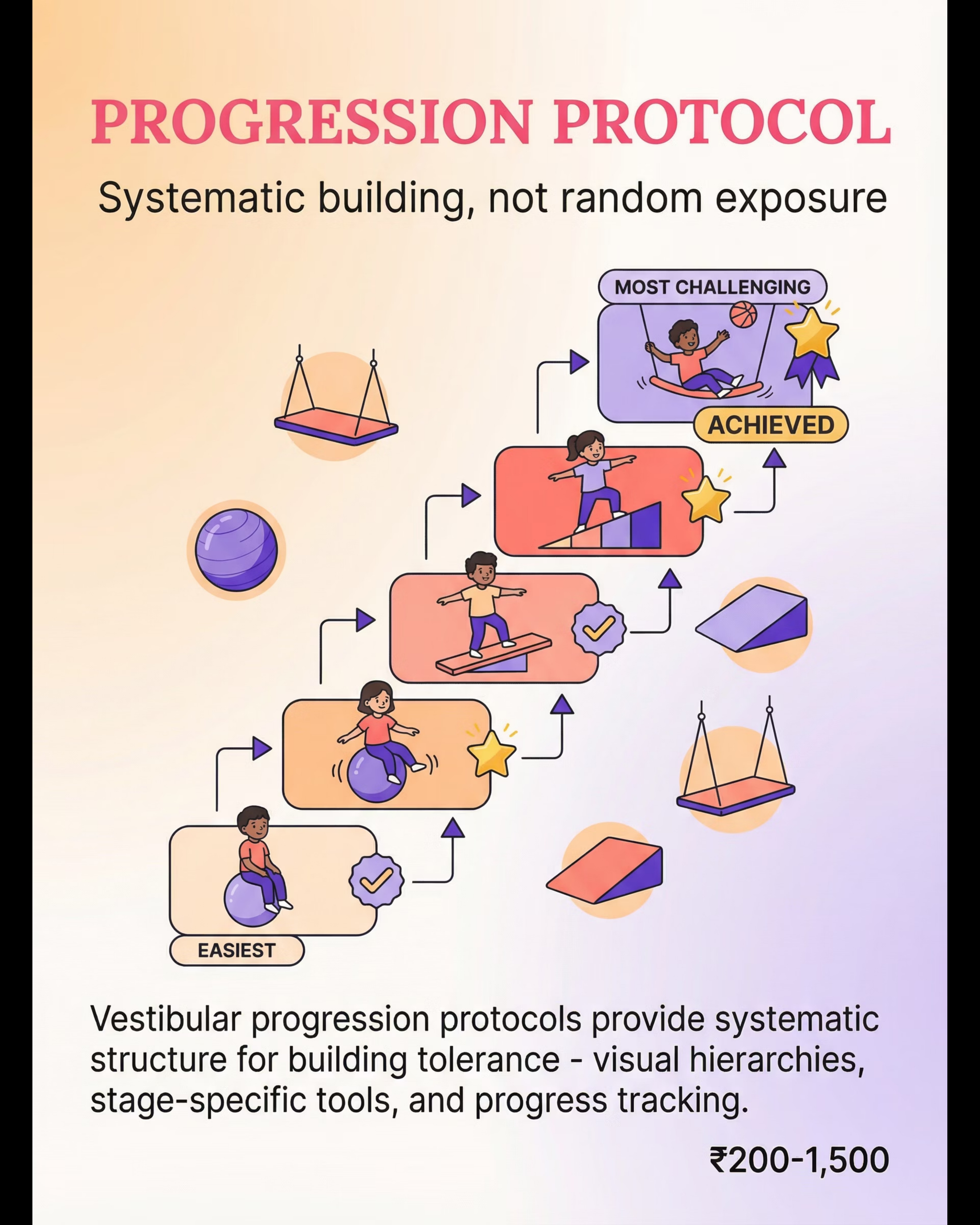
Vestibular Progression Protocol Materials
Canon: Tracking and Documentation | Price: ₹200–1,500
Systematic building, not random exposure. Track every degree of progress. Make the journey visible.
Total Investment: ₹200–15,000 (full range) | Essential Starters (minimum kit): Therapy ball + Weighted blanket + Hair washing accommodation = ₹2,600–10,500

Every Family Deserves Access — Zero-Cost Alternatives That Work
The Pinnacle Blooms Consortium believes that economic circumstance should never prevent a child from accessing evidence-based intervention. Every commercial material listed has a DIY alternative that preserves the therapeutic principle. The science doesn't live in the product — it lives in the approach.
1
Therapy Ball → Large Exercise Ball
Any large inflatable ball works. Start with the child sitting (feet on floor) with you stabilising. Progress to lying tummy-down with gentle rocking. Only introduce backward tilt when forward positions are comfortable. Never tip unexpectedly.
2
Weighted Products → Rice/Bean-Filled Fabric Pad
Sew a fabric rectangle, fill with rice or dried beans (5–10% of child's body weight). Test in calm situations before using during challenges. A heavy blanket folded across the lap works similarly.
3
Bath Supports → Rolled Towel + Visor
A rolled towel supporting the neck during slight recline. A visor or washcloth on the forehead to block water. Rinse with a cup in small sections with the child more upright — no deep recline required.
4
Incline Wedges → Stacked Firm Pillows
Stack firm pillows to create an inclined surface. Start with a very slight incline (nearly upright). Adjust gradually over weeks. Measure the angle and track progress on a simple chart.
Platform Swing → Wide Hammock With Sides
A hammock with edges or a sturdy blanket suspended securely provides similar contained vestibular input. Key: contained edges, not just a flat surface.
Vibrating Tools → Electric Massager
Battery-operated massagers serve the same purpose. Test preference when calm — some children respond positively, others find it overwhelming.
Visual Anchors → Your Face + Simple Mobile
Position yourself where the child can see you during tilted activities. Maintain eye contact. Hang a simple mobile above the bath area. Use a small mirror to let the child see themselves.
Progression Protocol → Handwritten Chart + Stickers
Draw a visual hierarchy chart. Add stickers for completed stages. Document progress. A simple notebook is sufficient — the tracking matters, not the tool.
Reference: PMC9978394 — WHO CCD Package emphasis on locally available, culturally appropriate materials.

Safety Is Not Optional — These Rules Protect Your Child
Read this card fully before beginning any vestibular work. These non-negotiables apply equally to commercial and DIY materials.
⛔ Contraindications — Do NOT Use If:
- Known vestibular pathology, inner ear condition, or current ear infection
- Seizure disorder triggered by positional changes (consult neurologist)
- Cervical spine instability (common in some genetic conditions)
- Recent head injury or concussion
- Acute illness or severe distress unrelated to vestibular challenges
⚠️ Material Safety Rules
- Therapy balls: Always hands on child. Non-slip surfaces. Never leave unattended.
- Platform swings: Hardware rated for child's weight PLUS movement forces. Check connections regularly.
- Weighted products: 5–10% body weight max. Never over face. Child must be able to remove independently. Never for unsupervised sleep.
- Vibrating tools: Test when calm first. Keep batteries secure.
- Bath supports: Never leave child unattended in bath. Check water temperature.
- Compression: Snug but NEVER restricting breathing or circulation.
🛑 STOP IMMEDIATELY IF: Skin colour changes (pale, bluish) during position changes • Child becomes limp or loses muscle tone • Child vomits during or after vestibular exposure • Eyes show persistent nystagmus after movement stops • Child reports pain (not fear — pain) in head, neck, or ears • Distress consistently escalates over 2+ weeks
If any red line is crossed: Stop the activity. Return child to upright. Comfort. Document what happened. Consult your occupational therapist or paediatrician before resuming.
Reference: DOI: 10.1007/s12098-018-2747-4 — Home-based sensory intervention safety protocols.

The Space Matters — Spatial Precision Prevents 80% of Session Failures
Your session environment is not just a backdrop — it is an active therapeutic tool. A well-prepared space reduces unpredictability, lowers the child's baseline anxiety, and allows the vestibular work to be the only challenge your child faces.
1
Child Position
Centre of space, on non-slip mat, away from hard edges and furniture corners. No obstacles within reach.
2
Parent Position
Always within arm's reach. Face visible to child. Hands ready to support. Eye contact is a vestibular anchor.
3
Therapy Ball
On non-slip surface or in ball holder for stationary work. Away from walls to allow movement in all directions.
4
Weighted Products
Within arm's reach for immediate grounding input pre/during session. Ready to apply without searching.
5
Visual Anchors
Positioned where child can see them during tilted positions. Mobile above, mirror at eye level, your face always visible.Reinforcement Items
6
Reinforcement Items
Visible but not accessible until earned. Motivating but not distracting during the vestibular work itself.
Remove From Space
- Hard furniture edges (pad or distance)
- Glass objects
- Electronic distractions
- Other children or pets
- Strong smells or sounds
Environmental Conditions
🌡️Temperature: Comfortable — overheating increases vestibular sensitivity
💡Lighting: Soft, natural preferred. Avoid harsh fluorescent.
🔊Sound: Quiet. Background noise increases vestibular processing load.
🏠Surface: Carpeted or padded mat. Never slippery floors.
Reference: PMC10955541 — Structured environment sessions showed maximum effectiveness.

The Best Session Is One That Starts Right
Your child's nervous system MUST be in a regulated state before you challenge the vestibular system. Adding vestibular input to a dysregulated nervous system is like adding fuel to a fire. Always ground BEFORE you tilt.
✅ Child has eaten within the past 2 hours (not hungry, not just eaten)
✅ Child has slept adequately (not overtired)
✅ No meltdown or significant distress in the past 30 minutes
✅ No illness symptoms (ear pain, fever, nausea)
✅ Child is in a calm-alert state (regulated, not hyperaroused or shut down)
✅ Space is set up and materials are ready and tested
🟢 All Green
Proceed to Step 1: The Invitation
🟡 1–2 Yellows
MODIFY: Do proprioceptive grounding only (weighted blanket, compression, heavy work) — no vestibular challenge today.
🔴 Any Red
POSTPONE: Do a calming activity instead. Attempt tomorrow. Skipping a session is not failure — forcing a bad session is worse than no session.

Step 1
The Invitation (Not a Command)
Timing: 1–2 minutes
"Hey [child's name], want to play the ball game? We're going to do our wobble practice. You tell me when to stop — you're the boss. Let's put on your heavy vest first. Feel that? That's your anchor. Now let's go say hi to the ball."
Body Language Guidance
- Get down to child's level
- Keep your voice calm, warm, and predictable
- Let the child approach the therapy ball — don't carry them to it
- Touch the ball yourself first to model safety
- Place weighted blanket or compression vest BEFORE approaching vestibular equipment
Acceptance Cues (what "yes" looks like)
- Child approaches the ball voluntarily
- Child touches the ball without prompting
- Eye contact and no pulling away
- Body is relatively relaxed, not rigid
Resistance Cues — What to Do
Child backs away: Increase distance. Do proprioceptive heavy work for 3–5 minutes first.
Child freezes: Stay at current distance. Talk calmly. Wait. Do not advance.
Child cries or panics: Stop. Comfort. Proprioceptive grounding only today.
Critical Principle
Every protocol begins with an INVITATION, not a command. If they say no — today is a grounding day, not a vestibular day. NEVER force.

Step 2
The Engagement
Timing: 2–3 minutes
Material Introduction
Position the therapy ball in front of the child. Let them touch it, push it, sit on it with their feet on the floor. You stabilise the ball with your hands or knees. The child should feel the ball is safe and controlled before any movement begins.
Proprioceptive Loading (Before Vestibular Challenge)
While the child sits on the ball, provide deep pressure: firm presses on shoulders, joint compressions to wrists and ankles, or place the weighted lap pad across their thighs. Load the proprioceptive system BEFORE any movement. This primes the nervous system for what's coming.
"You're sitting on the ball! Feel how your heavy pad is holding you? You're so stable. Now I'm going to hold you and we'll do a teeny tiny wobble. Ready? You say 'go.'"
Child Response Indicators
✅ Engagement
Calm, making eye contact, may be smiling, body relatively relaxed → Continue to Step 3
⚠️ Tolerance
Watchful, slightly tense, but not resisting → Proceed gently with reduced amplitude
🔴 Avoidance
Rigid, pulling away, whimpering, or refusing → Return to proprioceptive grounding only. Do not proceed to Step 3 today.
When the child sits on the ball and allows stabilisation, immediately praise: "You're on the ball! Look at you! You're so brave and strong!"
Reference: PMC11506176 — Structured material introduction meets evidence-based practice criteria.

Step 3
The Therapeutic Action: Building Backward Tilt Tolerance
Timing: 5–8 minutes (active vestibular work)
Stage A — Linear Movement (Start Here Every Session)
With the child seated or lying tummy-down on the therapy ball, introduce gentle forward-back linear rocking. Hands ALWAYS on the child. Movement amplitude: tiny — think 1–2 inches. Rhythmic. Predictable. Child controls 'stop' with a word or gesture.
Stage B — Lateral Movement (When Stage A Is Comfortable)
Introduce gentle side-to-side movement. Same principles: tiny amplitude, rhythmic, predictable, child controls stop. Do not progress until Stage A produces no visible tension.
Stage C — Backward Tilt Introduction (The Target)
From tummy-down on the ball, allow the child's upper body to extend slightly backward — perhaps 5 degrees past horizontal. Your hands support their torso fully. Hold for 2–3 seconds. Return to neutral. This is the active ingredient.
❌ Moving too fast or too far
If you can see the child's body tense, you've moved too far. Reduce by half.
❌ Surprising the child
Always narrate: "Here comes a tiny wobble..." Predictability is safety.
❌ Removing hands too early
Your hands = safety. Keep them on. Don't test independence prematurely.
❌ Continuing after stop signal
When they say stop, stop IMMEDIATELY. Trust is built by honouring their control.
Reference: PMC10955541 — Sessions with structured progressive vestibular exposure showed maximum effectiveness.

Step 4
Repeat & Vary — 3 Good Reps > 10 Forced Reps
Timing: 3–5 minutes
Target Repetitions
3–5 backward tilt exposures per session. NOT 10. NOT 20. Quality over quantity. Each backward tilt should end before the child reaches their distress threshold.
The Critical Principle
3 successful backward tilts where the child feels safe build more vestibular tolerance than 10 tilts where the child feels pushed past their limit. Trust builds tolerance. Fear destroys it.
Variation Options (to Maintain Engagement)
- Variation 1: Therapy ball position — sitting vs. tummy-down vs. side-lying
- Variation 2: Incline wedge — child lies at current tolerated angle
- Variation 3: Lap-based tilt — child in parent's lap, parent leans back gradually
- Variation 4: Platform swing — gentle swinging with controlled tilt component
- Variation 5: Play-based — reaching for a toy requiring slight backward lean
Satiation Indicators (Enough Is Enough)
- Engagement decreasing — looking away, losing interest
- Fidgeting increasing — wanting to get off the ball
- Verbal protest beginning — "all done" or equivalent
- Yawning, rubbing eyes — nervous system fatigue
When you see these signs: one more rep with maximum support, then transition to cool-down.

Step 5
Reinforce & Celebrate — Timing Matters More Than Magnitude
Timing: Immediate — within 3 seconds of desired behaviour
"You DID it! You leaned back and you were SAFE! Your body is learning! I am SO proud of you!"
Timing
Within 3 seconds of the desired behaviour. Delayed praise loses its power. This is not optional — it is neurological.
Specificity
Name what the child did. Not "good job" but "you leaned back on the ball and you were safe!" Specific praise builds specific skills.
Enthusiasm
Match your energy to the achievement. A tiny tilt deserves genuine excitement. Your enthusiasm IS the reinforcement.
Reinforcement Menu
Verbal praise + high-five + preferred activity after session + sticker on progress chart. Vary to maintain motivation across weeks.
Token Economy: Each backward tilt attempt = 1 token. 3 tokens = preferred activity after session. The attempt is reinforced, not just the success. Trying is winning.
Celebrate the Attempt: If the child sits on the ball but doesn't tolerate backward tilt today — STILL celebrate. "You sat on the ball! That's amazing! You're getting braver every day!" Every step toward the ball is progress.

Step 6
The Cool-Down — No Session Ends Abruptly
Timing: 2–3 minutes
Transition Warning: "'Two more wobbles, then all done with ball time.'" Always give advance notice before ending vestibular work.
Transition Script
"Ball time is all done. Now it's [next activity]. You worked SO hard today."
If Child Resists Ending
If the child wants to continue — that's actually a GREAT sign! It means the vestibular input is becoming enjoyable rather than threatening. Allow 1–2 more minutes if the child is regulated, then use a clear transition cue.
Why Cool-Down Matters
The nervous system needs a structured wind-down after vestibular input. An abrupt ending can leave the child's system in a partially activated state, increasing the likelihood of delayed meltdowns or sensory dysregulation in the 30 minutes following the session.
Proprioceptive input after vestibular work is the neurological equivalent of letting a spinning top slow down naturally rather than stopping it suddenly.
Reference: NCAEP Evidence-Based Practices Report (2020) — Visual supports evidence-based practice for autism.

60 Seconds of Data Now Saves Hours of Guessing Later
Record within 60 seconds of session end — while the detail is fresh. This data becomes the map that guides every future session decision.
1
Maximum Backward Tilt Angle Tolerated
Scale: 0° (upright only) | 10° | 20° | 30° | 45° | 60° | 90° (flat)
Today: ___°
2
Distress Level During Maximum Tilt
Scale: 1 (calm) | 2 (watchful) | 3 (tense) | 4 (protesting) | 5 (panic)
Today: ___
3
Successful Backward Tilt Exposures
Count: ___ out of ___ attempted
Each attempt counts — even partial tilts deserve to be recorded.
Quick Notes (Optional But Valuable)
"What went well: ___"
"What was challenging: ___"
"Child's state at end of session: ___"
Track With GPT-OS®
Digital tracking available at: pinnacleblooms.org/tracker
The GPT-OS® dashboard visualises your child's vestibular tolerance progression over time, generating reports you can share directly with your OT at each appointment.
Reference: BACB Guidelines + Cooper, Heron & Heward (Applied Behavior Analysis) — Continuous measurement as standard practice.

Session Abandonment Is Not Failure — It's Data
Every difficult session tells you something precise and useful about your child's vestibular threshold, nervous system state, and the protocol adjustments needed. Here is how to interpret and respond to the most common challenges.
My child refused to even approach the therapy ball today
This is information, not failure. Do proprioceptive work only today. Try again tomorrow. Consider whether something else stressed the child today — illness, schedule disruption, or emotional events all temporarily raise the vestibular alarm threshold.
Fine with forward-back rocking but panicked at any backward tilt
You found the threshold — that IS the vestibular alarm in action. Stay at forward-back for 3–5 more sessions. When reintroducing backward tilt, make it so tiny it's almost imperceptible — 1–2 degrees.
Child cried through the entire session
You pushed past their threshold too quickly. Next session: proprioceptive loading only (no vestibular). The session after: vestibular work at 50% of today's intensity. Rebuild trust from the foundation.
Fine during session but meltdown 30 minutes later
Delayed vestibular response. The nervous system was overloaded but held together during the session and released later. Reduce session intensity or duration. Extend the cool-down period significantly.
Were making progress but suddenly regressed this week
Regression is normal and expected. Illness, sleep disruption, schedule changes, or emotional stress can temporarily reduce vestibular tolerance. Drop back 2–3 stages and rebuild. Progress is not linear — it is a spiral.
Child is getting more anxious ABOUT sessions, not less
Anticipatory anxiety means sessions are too challenging. Drop intensity significantly. Focus on making ball time FUN with no vestibular demand for 1–2 weeks. Re-pair the equipment with exclusively positive experiences before reintroducing tilt.
Not sure if I'm doing this right
You're asking the question — that means you care deeply. Record a session on your phone and share with your OT. Call the FREE National Autism Helpline: 9100 181 181.

Your Child Is Unique — The Protocol Should Be Too
The protocol is a framework, not a rigid script. Understanding how to adjust it for your child's current state, age, and sensory profile is what transforms this from a set of instructions into genuine therapeutic skill.
Easier — Bad Days / High Anxiety
- Proprioceptive loading only — no vestibular challenge
- Child sits on ball with feet on ground — you stabilise, no movement
- Weighted blanket time on the floor — no ball needed
- Play near the equipment without engaging it
Standard — Most Sessions
- Full sequence: ground → linear → lateral → backward tilt
- 3–5 backward tilt exposures at current tolerated angle
- All 6 steps executed in order
Harder — Breakthrough / Building Mastery
- Increase backward tilt angle by 5 degrees
- Reduce support (one hand instead of two — only when child is ready)
- Transfer to new equipment (incline wedge, platform swing)
- Introduce functional context (practice hair-washing lean with bath support)
Ages 1–2
Primarily parent-controlled. Child in parent's lap for tilts. Very brief exposures (2–3 seconds). Heavy reliance on proprioceptive grounding (deep pressure, swaddling-style holds).
Ages 3–5
Child begins to participate actively. "You say go" control. Visual progress chart with stickers. Playful, game-based framing throughout all sessions.
Ages 6–10
More cognitive engagement. Explain the brain science at their level. Self-monitoring ("How scary was that, 1–5?"). Greater independence in progression decisions.
Vestibular Avoider vs. Seeker: Most children with backward tilt distress are vestibular AVOIDERS — approach: slow, gradual, proprioceptive-heavy. Some SEEK vestibular input in other directions but specifically fear backward — use their preferred vestibular input as warm-up before targeting backward tilt.

Week 1–2
Weeks 1–2: Tolerance, Not Mastery
The first two weeks of vestibular desensitisation are about building the trust foundation that everything else is built on. Progress will be quiet, incremental, and profound — if you know what to look for.
What Progress Looks Like
- Child approaches the therapy ball with less resistance
- Child tolerates sitting on the ball with your support (even if briefly)
- Proprioceptive grounding activities are accepted and calming
- Anticipatory anxiety about sessions may still be present but child engages
- Tolerates 2–3 seconds of very gentle linear rocking
What Is Not Progress Yet
- Full backward tilt tolerance (not expected at this stage)
- Enjoying vestibular input (tolerance comes before enjoyment)
- Immediate transfer to daily activities like hair washing
- Elimination of all distress
The Honest Truth
If your child tolerates the therapy ball for 3 seconds longer this week than last week — that is real, measurable, neurological progress. The vestibular system recalibrates in tiny increments.
You may feel frustrated that progress seems slow. This is normal. Vestibular systems don't change overnight. Your patience IS the intervention.
Reference: PMC11506176 — Sensory integration intervention outcomes emerge across 8–12 week timelines.

Week 3–4
Weeks 3–4: The Neural Pathways Are Forming
By weeks three and four, something is genuinely changing in your child's nervous system. The vestibular alarm is beginning to recalibrate. You may begin to see it first not in sessions, but in daily life.
The chart illustrates a typical progression arc — gradual increases in tolerated tilt angle alongside decreasing distress levels. Individual timelines vary; what matters is the directional trend across your own data.
Consolidation Indicators
- Child anticipates ball time with less anxiety — may even show interest
- Tolerates gentle linear and lateral rocking with decreased tension
- First successful backward tilts — perhaps 5–10° with full support — without panic
- Recovery time after vestibular challenge is decreasing
- Proprioceptive tools actively sought by child
Generalisation Seeds
Your child may begin tolerating slight recline in other contexts — leaning back on the couch, tilting slightly during play. These spontaneous moments are MORE important than session performance because they show the vestibular system is actually recalibrating, not just tolerating the session.
When to Increase Intensity
If 5° backward tilt is tolerated calmly for 3 consecutive sessions → try 8–10°. Never jump more than 5° at a time.

Week 5–8
Weeks 5–8: Mastery Emerging
This is where the work becomes visible — not just in sessions, but in the daily activities that brought you here in the first place. Mastery is not perfection; it is functional tolerance that makes life possible.
Backward Tilt Tolerated
On therapy ball with support — mild discomfort, not panic
1
Progress Milestone
Functional daily activities becoming manageable across multiple contexts
2
Contexts Generalising
Skill appearing in settings beyond the therapy session itself
3
✅ Hair washing with accommodation (tray/visor) completed without significant distress
✅ Dental chair tolerated with preparation and supports (weighted lap pad, visual anchor)
✅ Lies on incline wedge at 30°+ watching a favourite show
✅ Can lie back on the couch or look up at the ceiling without panic
✅ Distress response is "I don't love this" rather than "I'm terrified"
Mastery Unlocked Criteria: Backward tilt of 30°+ produces discomfort (not panic) that resolves within 10 seconds, across 3+ different contexts, across 3 consecutive sessions.
References: PMC10955541 | BACB mastery criteria

You Did This. Your Child Grew Because of Your Commitment.
"Five to eight weeks ago, you arrived on this page with a specific pain: your child screamed when their head tilted backward. Hair washing was a nightmare. The dental chair was impossible. Backward meant falling. Today, your child has experienced — through YOUR hands, YOUR patience, YOUR consistency — that backward doesn't mean falling. Their vestibular system has begun to recalibrate. The alarm is quieter. The trust is deeper. This is not just a therapy milestone. This is a daily living skill milestone. This is a family quality-of-life milestone. This is your child's nervous system literally rewiring because you showed up, session after session, tilt after tiny tilt."
Family Celebration Suggestion: Mark this moment. Take a photo of your child doing something that used to be impossible — lying on the couch watching the ceiling, getting their hair washed with minimal fuss, sitting in a dental chair. Put it on the fridge. Show grandparents. This is real.
Photo/Journal Prompt: Document this milestone. Write the date. Write what your child can do now that they couldn't 8 weeks ago. You'll want to remember this.

Trust Your Instincts — If Something Feels Wrong, Pause and Ask
Celebrations are warranted — but the commitment to your child's safety continues. These red flags apply throughout the programme and should never be dismissed or waited out.
🚩 Distress INCREASING Over 2+ Weeks
What it looks like: Sessions are getting harder, not easier. Child is more anxious, not less.
What to do: Stop vestibular work. Return to proprioceptive-only. Consult your occupational therapist.
🚩 Child Develops NEW Fears Not Related to Vestibular Input
What it looks like: Child who only feared backward tilt now fears other movements or new situations.
What to do: Possible generalised anxiety developing. Pause protocol. Consult OT and paediatrician.
🚩 Physical Symptoms — Nausea, Vomiting, Headaches, Ear Pain
What it looks like: Physical complaints during or after sessions.
What to do: Stop immediately. Consult paediatrician. May indicate vestibular pathology requiring medical evaluation.
🚩 Child Becomes Fearful of YOU During Sessions
What it looks like: Child resists being held by you, avoids you before sessions, trust in relationship affected.
What to do: Stop the protocol. Rebuild relational trust. This is the most critical red flag — the relationship matters more than the vestibular system.
🚩 Progress Plateau Lasting 3+ Weeks
What it looks like: Same tolerance level, no change, despite consistent sessions.
What to do: Consult OT for protocol modification. May need different approach, additional assessment, or consideration of other factors.

Your Child's Developmental GPS — Where You've Been, Where You're Going
Backward tilt distress does not exist in isolation. It sits within a broader vestibular and sensory processing landscape. Understanding the full map helps you plan intelligently for what comes next.
Long-Term Developmental Goal
Functional vestibular tolerance across daily living activities — the child participates fully in hygiene, medical care, play, and physical activity without vestibular fear limiting their life.
Your Position in the Map
You have completed A-087. Your child's vestibular system has begun to recalibrate for backward tilt. The next techniques build on this foundation — each one expanding the range of movements and positions your child can access with confidence.

Techniques That Work Alongside This One
Vestibular processing connects deeply to multiple domains of your child's development. These related techniques extend and complement the work you've done here — each addressing a related vestibular or sensory challenge.
1
A-088 — When Spinning Creates Distress
Rotary vestibular challenge. If your child also struggles with spinning or circular movement, this technique complements backward tilt work perfectly — addressing the next vestibular domain.
2
A-089 — Height and Elevation Fear
Vertical vestibular challenge. Addresses fear of being on high surfaces or being lifted — a closely related vestibular trigger that often co-occurs with backward tilt distress.
3
A-090 — Fear of Playground Equipment
Functional application. Translates the vestibular tolerance built in A-087 to playground participation — swings, slides, and climbing structures become accessible.
4
A-092 — Fear of Being Picked Up
Positional change challenge. Addresses the related vestibular trigger of unexpected position changes — connecting to backward tilt through the same gravitational insecurity mechanism.
K-1070
Understanding Vestibular Processing (Parent Education Module)
K-1075
Sensory Integration at Home (Complete Guide)
K-1080
When Daily Routines Trigger Sensory Distress

This Technique Within the Full 999-Technique Library
"Your child's development is not a single path — it's a constellation. Each technique you master illuminates another point. This technique — building vestibular trust for backward tilt — connects to self-regulation, daily living skills, social participation, and physical activity. Everything connects."
Your Position
A-087 of 999 techniques across 12 domains
Domain A: Sensory Processing (100 techniques)
← THIS TECHNIQUE LIVES HERE
The Full Map Awaits
Every technique you master opens a new constellation of possibilities for your child. The GPT-OS® AbilityScore® Assessment maps your child's complete developmental profile and generates a personalised sequence across all 12 domains.

From Screaming to "I Did It, Mama!"
"Bath time used to end in screaming — every single time. Rinsing her hair meant tilting her head back, and tilting meant terror. We tried everything — distraction, rewards, holding her tight — nothing worked because we didn't understand what was happening. Her OT explained it: her brain was literally telling her she was falling. We started with the therapy ball — just sitting on it, then tiny movements, then eventually she could lie back over it with my hands supporting. We got a hair washing tray so she didn't have to tilt as far. We used the weighted lap pad at the dentist. Six months later, she washed her hair with just a slight lean back and said 'I did it, Mama!' She still doesn't love backward positions, but she can tolerate them. The terror is gone." — Parent, Pinnacle Blooms Network
Illustrative case; outcomes vary by child profile.
Your story matters. When you're ready, share your journey: care@pinnacleblooms.org

You're Not Doing This Alone
Building vestibular tolerance in your child is a journey that is infinitely easier — and more effective — with the right community and support structure around you. Pinnacle Blooms Network provides multiple layers of connection for every family.
FREE National Autism Helpline
9100 181 181 — 16+ languages, 24x7. Speak with trained specialists who understand vestibular challenges, sensory processing, and what your family is navigating.
Pinnacle Blooms Community
pinnacleblooms.org/community — Connect with families navigating the same challenges. Share wins, ask questions, and find parents who truly understand.
Email Support
care@pinnacleblooms.org — Write to us with your questions, your wins, or your worries. A real person reads every message.
WhatsApp Support Groups
Ask your centre coordinator for access to WhatsApp groups for parents navigating sensory processing challenges — available across multiple languages and regions.
Parent Support Resources
- Understanding Vestibular Processing — Parent Education Module
- Sensory Integration at Home — Complete Guide
- Managing Your Own Stress as a Therapy Parent

When You Need More Than This Page Can Offer
This page equips you for home-based vestibular work. There are moments, however, when the expertise of a trained clinician — working with your child directly — becomes essential. Recognising that moment is a sign of wisdom, not failure.
When to Seek Professional OT
- Gravitational insecurity is severe — panic at ANY position change
- Progress has plateaued despite 4+ consistent weeks
- You are unsure about execution or material selection
- Any red flag from Card 27 has appeared
- Child has complex co-occurring conditions (autism, anxiety disorder, neurological diagnosis)
What to Expect at a Pinnacle Assessment
The AbilityScore® Assessment maps your child's complete sensory processing profile across 349 skills and 79 abilities. You'll leave with a personalised intervention plan, prioritised by the GPT-OS® Prognosis Engine, and coordinated across all relevant disciplines.
70+ Centres Across India
Find your nearest Pinnacle Blooms centre for a comprehensive sensory processing assessment. Our sensory integration-trained occupational therapists work directly with the vestibular challenges described on this page.
Book an Assessment
📞9100 181 181

The Evidence Base — For Parents Who Want to See the Science
Every element of this protocol is grounded in peer-reviewed research. The following studies form the primary evidence base for the approach described on this page.
Systematic Review (2024) — PMC11506176
PRISMA model systematic review of 16 articles (2013–2023). Confirms sensory integration intervention meets evidence-based practice criteria for children with ASD, including graduated vestibular exposure protocols. View on PubMed →
Meta-Analysis (2024) — PMC10955541
24 studies analysed. Confirms efficacy for social skills, adaptive behaviour, sensory processing, and motor skills. Vestibular-specific interventions showed particular efficacy for positional tolerance and daily living skill participation. View on PubMed → | DOI: 10.12998/wjcc.v12.i7.1260
Indian RCT (2019) — Padmanabha et al.
Randomised controlled trial demonstrating significant outcomes for parent-administered sensory protocols in the Indian paediatric population. Indian Journal of Pediatrics. DOI: 10.1007/s12098-018-2747-4
WHO CCD Framework — PMC9978394
Care for Child Development Package implementation across 54 low- and middle-income countries. Multi-country evidence for caregiver-delivered developmental interventions with locally available materials.
Neurological Basis (2020)
Frontiers in Integrative Neuroscience. Establishes neurological basis for sensory-based interventions in ASD, confirming vestibular system dysregulation as mechanism. DOI: 10.3389/fnint.2020.556660
Foundational Theory — Jean Ayres, PhD, OTR
Ayres Sensory Integration Theory: The foundational research establishing vestibular-proprioceptive integration mechanisms and intervention principles. The grandmother of all vestibular therapy research — everything in this protocol builds on her work.

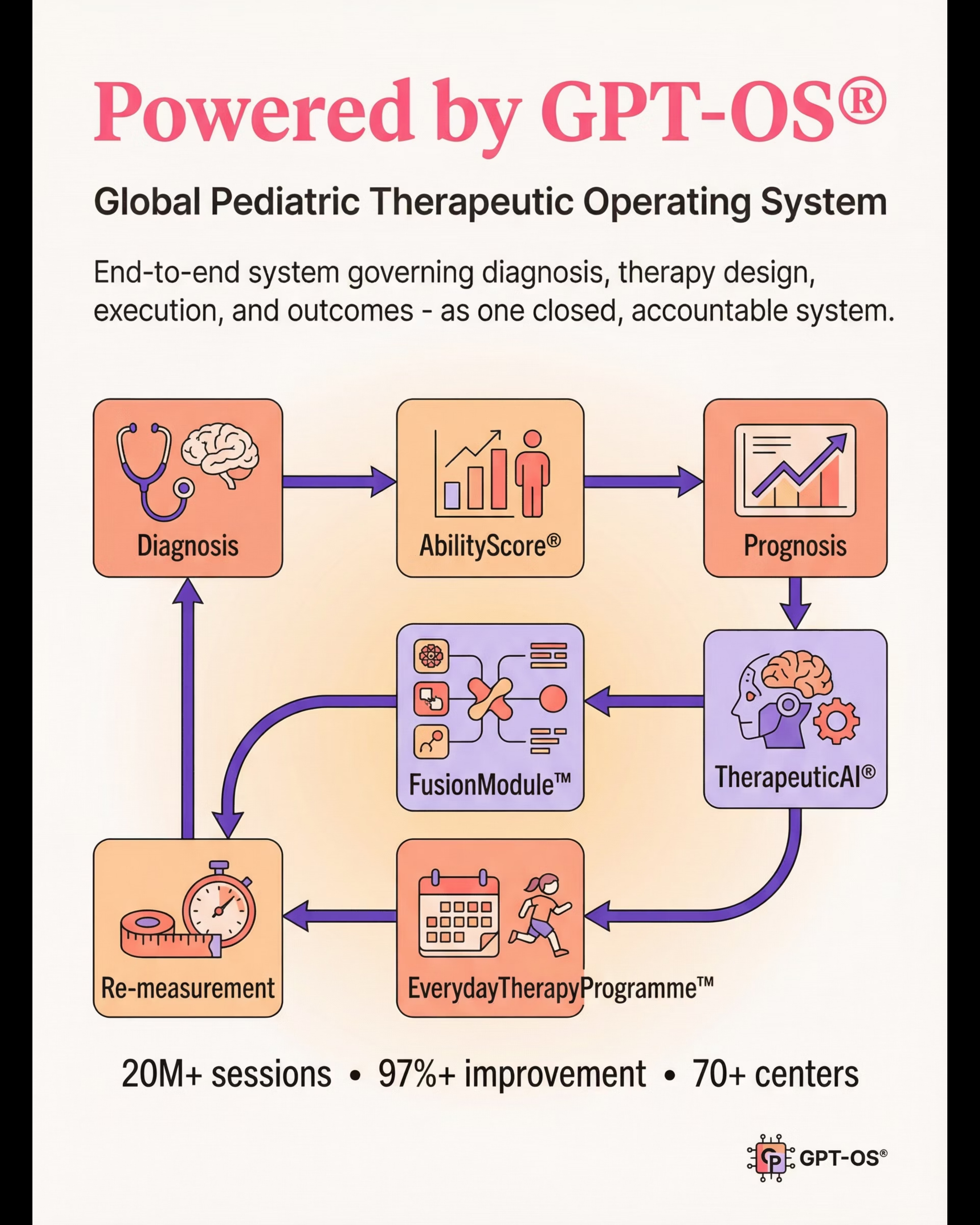
Powered by GPT-OS® — Global Pediatric Therapeutic Operating System
"GPT-OS® is the end-to-end operating system governing diagnosis, therapy design, execution, monitoring, and readiness outcomes in child development — as one closed, accountable system."
Diagnostic Intelligence Layer
591+ structured observations across 349 skills and 79 abilities — capturing the complete profile of your child's developmental landscape.
AbilityScore®
Patented universal developmental score (0–1000) that places your child's current abilities on a precise, meaningful scale.
EverydayTherapyProgramme™
Daily home-executable micro-interventions — including vestibular work like the protocol on this page — generated for your child's specific profile.
Closed-Loop Therapeutic Control
Observe → Score → Plan → Execute → Re-measure → Adapt. The system never stops learning from your child's progress.
20M+
Exclusive 1:1 Sessions
97%+
Measured Improvement
70+
Centres Across India
160+
Countries with Filed Patents
For this technique: GPT-OS® tracks backward tilt distress progression within the Sensory Processing Index and Daily Living Skills Index, from severe intolerance to functional vestibular tolerance.

Watch: 9 Materials That Help When Tilting Backward Distresses
A-087 Series: Sensory Solutions | Episode 87
Domain: Sensory Processing + Vestibular System + Daily Living
"This 60-second reel introduces all 9 materials featured on this page. Share it with family members, therapists, or teachers who need a quick visual overview of the vestibular trust-building toolkit."
📱Share this reel: Forward to co-parents, grandparents, classroom teachers, and anyone who interacts with your child during activities that require positional changes.

Consistency Across Caregivers Multiplies Impact
If only one parent executes this technique, progress is limited. The vestibular system recalibrates through consistent, predictable experiences. When grandparents force hair washing, teachers trigger dental panic, and one parent grinds against all the progress the other is building — the therapy stalls. Share this with everyone.
📱 WhatsApp
Share this page directly to your family group. One tap, full protocol.
📧 Email
Send to co-parent, grandparent, teacher, or school coordinator with context about your child's needs.
🔗 Copy Link
techniques.pinnacleblooms.org/sensory-processing/backward-tilt-distress
📄 One-Page Family Guide (PDF)
Simplified version of the full protocol for all caregivers — what to do, what to avoid, and how to respond when the child shows distress.
📄 "Explain to Grandparents" Guide
Why tilting backward terrifies your grandchild — explained with warmth and clarity for family members who may not be familiar with sensory processing.
📄 Teacher/School Communication Template
For PE, dental health visits, and field trips. A professional, ready-to-send communication explaining your child's needs and requesting reasonable accommodations.
"[Child's name] has gravitational insecurity — their brain perceives backward tilt as falling. Please don't force them to lean back or dismiss their fear. Here's what helps: [link to this page]. Thank you for understanding."
Reference: PMC9978394 — WHO CCD Package: Multi-caregiver training is critical for intervention generalisation.

Your Questions Answered
These are the questions families ask most frequently — answered with the same clinical honesty and parental warmth that runs through every part of this protocol.
Will my child ever be able to have their hair washed normally?
Many children with gravitational insecurity achieve functional hair washing tolerance — meaning they can tolerate the necessary tilt with mild discomfort rather than panic. Some children always prefer forward-leaning hair rinsing, and that is perfectly fine. The goal is manageable daily living, not perfect vestibular function.
How long will this take?
Typically 8–12 weeks of consistent practice (3–5 sessions per week) to see meaningful functional improvement. Some children progress faster, some slower. Severe gravitational insecurity may take 6+ months. Progress is not linear — it is a spiral that sometimes revisits earlier stages before moving forward.
Can I do this without an occupational therapist?
This page provides a parent-executable protocol based on clinical evidence. For mild to moderate backward tilt sensitivity, many parents can implement this successfully at home. For severe gravitational insecurity (panic at ANY position change), we recommend working with an OT who specialises in sensory integration.
My child is fine with forward and side movement but only panics at backward tilt. Is that normal?
Yes. Backward tilt is the most commonly feared direction because it moves the head away from upright — the position of maximum security. Many children tolerate other vestibular inputs well but have specific backward tilt sensitivity. You're not imagining the pattern — it is neurologically real.
Should I keep forcing hair washing while we work on this?
No. Use accommodations (hair washing tray, visor, cup rinsing) for daily hygiene. Do vestibular work in SEPARATE sessions. Forcing hair washing as exposure therapy in the bath creates chronic daily stress and is counterproductive — it sensitises the vestibular system rather than recalibrating it.
The dentist says my child needs dental work but can't recline. What do I do?
Share this page with your dentist. Ask about: gradual recline (a few degrees at a time with pauses), weighted lap pad during the procedure, modified positioning, or sedation for necessary procedures. Call our helpline (9100 181 181) for guidance on preparing your child for dental visits specifically.
Is gravitational insecurity the same as fear of heights?
Related but distinct. Gravitational insecurity specifically involves fear of positional changes relative to gravity — particularly backward tilt and inversion. Fear of heights (acrophobia) is about elevation. They can co-occur, and both involve the vestibular system, but backward tilt distress can occur at ground level with no height involved at all.
What if my child has autism AND gravitational insecurity?
Very common co-occurrence. The protocol remains the same, with additional attention to: ABA-based reinforcement structures, visual supports for communication, sensory profile considerations beyond vestibular (tactile, auditory), and coordination with your child's comprehensive therapy plan through the FusionModule™ approach.

You've Read the Science. You Have the Materials. Your Child Is Waiting.
The hardest moment in any intervention is the first session. Everything after that gets easier — not because the work disappears, but because you and your child build trust, competence, and a shared language for this challenge. That first session starts right now.
🟢 Start This Technique Today
Begin with the Readiness Check. Then follow the 6-step protocol. Your child's vestibular recalibration starts with the first invitation.
📞 Book an Assessment
9100 181 181 | pinnacleblooms.org/assessment — Start with the AbilityScore® Assessment to map your child's full sensory profile.
🔄 Explore Next Technique
A-088: When Spinning Creates Distress — the next vestibular domain awaits at techniques.pinnacleblooms.org
Validated by the Pinnacle Blooms Consortium
OT
SLP
ABA
SpEd
NeuroDev
CRO
Preview of 9 materials that help when tilting backward distresses Therapy Material
Below is a visual preview of 9 materials that help when tilting backward distresses therapy material. The pages shown help educators, therapists, and caregivers understand the structure and content of the resource before use. Materials should be used under appropriate professional guidance.





Link copied!

From Fear to Mastery. One Technique at a Time.
Pinnacle Blooms Network® transforms homes into evidence-based, 24x7, personalised, multi-sensory, multi-disciplinary therapy environments — powered by GPT-OS® and backed by 20M+ sessions of real-world evidence.
Built by Mothers. Engineered as a System.
FREE National Autism Helpline
9100 181 181 — 16+ languages, 24x7
Website
Statutory Identifiers: CIN: U74999TG2016PTC113063 | DPIIT: DIPP8651 (Govt. of India) | GSTIN: 36AAGCB9722P1Z2
Medical Disclaimer: This content is educational. It does not replace assessment by a licensed occupational therapist or healthcare provider. Significant gravitational insecurity or vestibular processing differences should be comprehensively evaluated to understand the child's full sensory profile and guide appropriate intervention. Individual results may vary. Statistics represent aggregate outcomes across the Pinnacle Blooms Network.
© 2025 Pinnacle Blooms Network®, unit of Bharath Healthcare Laboratories Pvt. Ltd. All rights reserved.
techniques.pinnacleblooms.org