
When Leaving the Ground Feels Like Falling Forever
A vestibular grounding protocol for the child who needs the earth beneath them — evidence-based, home-executable, parent-proven.
Sensory Solutions Series — Episode 79
Ages 2–10
Pinnacle Blooms Consortium

The Recognition Moment
Your five-year-old is frozen on the second rung of the climbing frame. His knuckles are white, his body rigid, tears streaming — and he can't go up and he can't go down. The other children swing and leap and tumble while he stands at the edge, watching, too terrified to join. When you pick him up, he doesn't melt into your arms like other children — he clings to your neck like he's falling off a building and screams to be put down.
This isn't stubbornness. This isn't defiance. This isn't "just being scared." Your child's nervous system is treating gravity as a threat.
There is a name for this. There is science behind it. And there are 9 materials — clinically validated, home-executable, parent-proven — that build trust between your child and movement, one inch at a time.
You are not failing. Your child's vestibular system is speaking. We're here to translate. WHO Nurturing Care Framework (2018): Early identification and parental awareness directly impacts developmental outcomes.

The Vestibular System: Why the Ground Is the Only Safe Place
What's Happening in Your Child's Brain
Deep inside your child's inner ear sits the vestibular system — a biological motion sensor that detects every tilt, turn, and change in head position. It coordinates with vision and proprioception (the body's sense of where it is in space) to maintain balance and spatial orientation.
In your child, this system is hypersensitive.
Ordinary movements — being lifted, swinging, climbing, jumping — are amplified by the vestibular system into signals that the brain reads as danger. The amygdala (the brain's threat detection centre) fires. Cortisol surges. The fear response activates.
This Is a Wiring Difference, Not a Behaviour Choice
Your child genuinely experiences gentle lifting as falling. A two-inch step as a cliff edge. A swing as an uncontrolled launch into space. The fear is neurologically real and involuntary — even when your child cognitively understands they are safe.
This is why we don't force. We build trust. One neural pathway at a time.
Research: Frontiers in Integrative Neuroscience (2020) — Neurological basis for sensory-based interventions. DOI: 10.3389/fnint.2020.556660

Your Child's Vestibular Development: The Map and the Path Forward
Gravitational insecurity typically becomes apparent between 18 months and 5 years — the period when movement exploration naturally accelerates. Children who previously seemed cautious now visibly differ from peers in playground participation, physical play, and movement confidence. The golden age of neuroplasticity (ages 0–7) means that intervention NOW has maximum impact — but vestibular system adaptation continues well into childhood. It is never too late.
1
0–6 Months
Vestibular system active in utero; responds to rocking, swaying; head control begins
2
6–18 Months
Sitting balance develops; tolerates supported movement; walking confidence builds
3
18–36 Months
Jumping, climbing, swinging typically emerge — gravitational insecurity becomes apparent here ← Your child may be here
4
3–5 Years
Motor confidence expanding; playground challenges most visible socially
5
5–10+ Years
Graduated tolerance building; grounded → supported → low elevation → independent movement
WHO Care for Child Development Package | UNICEF MICS indicators | References: PMC9978394 | WHO/UNICEF CCD Package (2023)

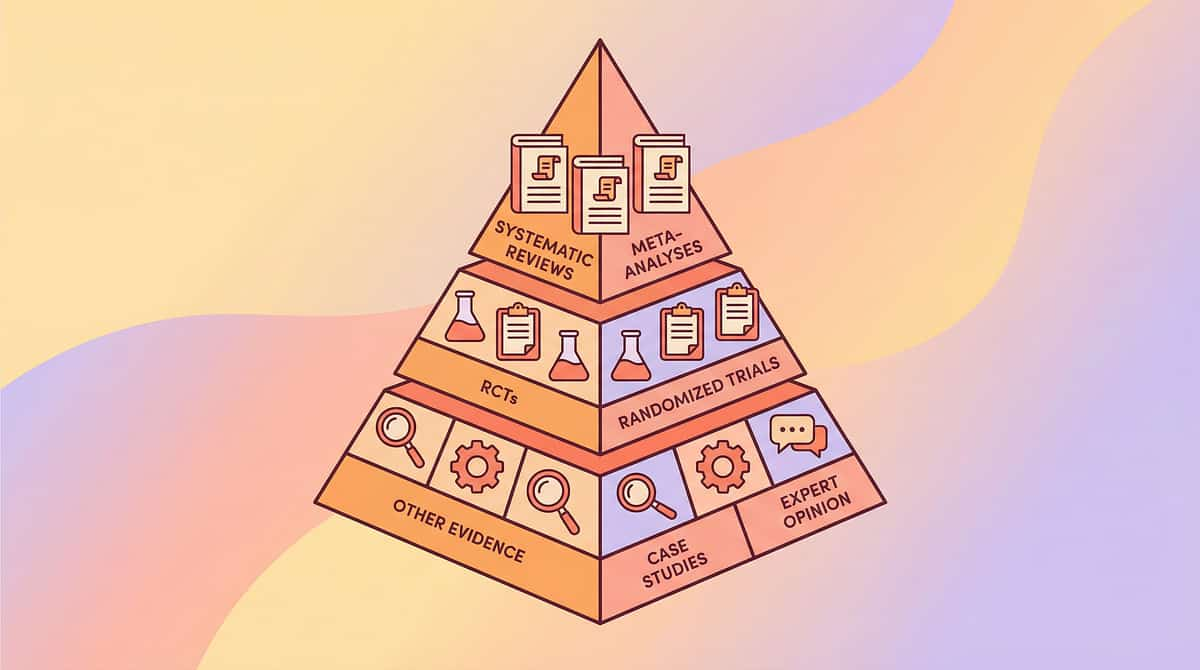
Clinically Validated. Home-Applicable. Parent-Proven.
Evidence Grade: Level I–II
Systematic Reviews + RCTs
The Pinnacle Blooms Consortium — representing OT, SLP, ABA, Special Education, NeuroDevelopmental Paediatrics, and Clinical Research — has reviewed and validated this protocol for home execution. Here is the evidence behind what you are about to learn.
1
PRISMA Systematic Review (2024)
16 articles from 2013–2023 confirm sensory integration intervention meets criteria for evidence-based practice for children with ASD. → PMC11506176
2
Meta-Analysis — World J Clin Cases (2024)
Sensory integration therapy effectively promotes social skills, adaptive behaviour, sensory processing, and motor skills across 24 studies. → PMC10955541 | DOI: 10.12998/wjcc.v12.i7.1260
3
Indian RCT — Padmanabha et al. (2019)
Home-based sensory interventions demonstrated significant outcomes in Indian paediatric populations. → DOI: 10.1007/s12098-018-2747-4
4
NCAEP Evidence-Based Practices (2020)
Sensory integration classified as evidence-based practice for autism — National Clearinghouse on Autism Evidence and Practice
5
WHO Nurturing Care Framework (2018)
Responsive caregiving and early learning through structured home intervention validated across 54 countries. → nurturing-care.org/ncf-for-ecd/ | PMC9978394
84%
Evidence Strength
4.2 / 5.0 evidence confidence rating across reviewed studies
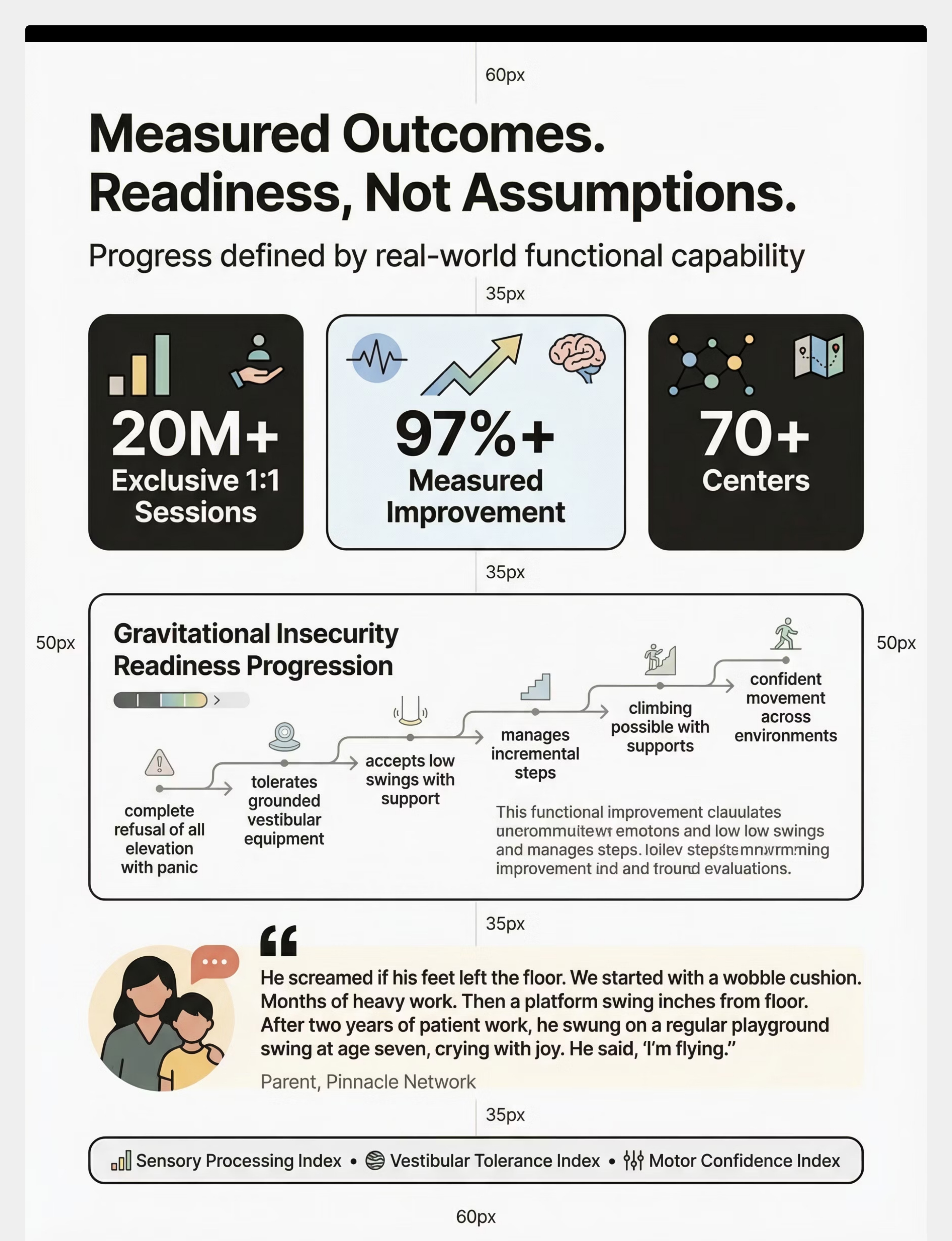
97%
Measured Improvement
Across 20M+ therapy sessions within the Pinnacle Blooms Network

Vestibular Grounding Protocol for Gravitational Insecurity
Parent-Friendly Name: "Ground-to-Air Trust Building"
The Vestibular Grounding Protocol is a structured, progressive intervention that builds a child's tolerance for movement and elevation through 9 categories of therapeutic materials — starting from completely grounded positions and incrementally introducing controlled, supported, child-paced elevation. The protocol uses grounded vestibular equipment, proprioceptive (heavy work) preparation, supported elevation, incremental stepping, climbing supports, weighted/compression aids, controlled descent practice, and visual preparation to systematically desensitise the vestibular system while building motor confidence.
This is not exposure therapy. This is neural trust-building — one inch at a time.
Domain
Sensory Processing | Vestibular System | Motor Development | Anxiety
Age Range
2–10 years
Session Duration
10–20 minutes (home sessions)
Frequency
Daily to 3×/week; heavy work preparation daily
Setting
Home + Playground + Therapy

A Multi-Disciplinary Protocol: How Each Expert Uses This Differently
This technique crosses therapy boundaries because the brain doesn't organise by therapy type. Each discipline brings a unique lens — together, they form a unified intervention system.
Occupational Therapist (Primary Lead)
Designs the sensory integration protocol, selects vestibular equipment based on sensory profile assessment, calibrates progression from grounded to elevated activities, monitors vestibular tolerance indices.
Physical Therapist
Addresses gross motor development gaps — balance, coordination, postural stability, bilateral integration. Supports climbing and jumping skill progression alongside vestibular work.
Board Certified Behaviour Analyst
Designs reinforcement schedules for movement attempts, addresses avoidance behaviour through graduated exposure protocols, implements systematic desensitisation with continuous data collection.
NeuroDevelopmental Paediatrician
Rules out medical causes of vestibular hypersensitivity, monitors co-occurring conditions, provides medical clearance for movement progression. The safety anchor of the team.
Reference: Adapted UNICEF/WHO Nurturing Care Framework for SLPs (2022). DOI: 10.1080/17549507.2022.2141327

Precision Targets: What This Protocol Addresses
This protocol works at multiple levels simultaneously — from the neurological core outward to social participation and everyday life. Understanding what you're targeting helps you measure meaningful progress.
🎯 Primary Target — Vestibular Tolerance
Building the nervous system's capacity to process movement and elevation without triggering fear responses. Observable indicator: Child tolerates 30+ seconds of gentle vestibular input without distress signals.
🔵 Secondary Targets
Motor confidence (approaches rather than avoids equipment), proprioceptive integration (improved body awareness), and anxiety regulation (reduced fear response to everyday elevation — being picked up, escalators, car over bumps).
🟢 Tertiary Targets
Social participation, gross motor development, emotional resilience in novel physical environments, and adaptive functioning — independent navigation of stairs, curbs, and uneven surfaces.
Meta-analysis (World J Clin Cases, 2024): Sensory integration therapy effectively promoted social skills, adaptive behaviour, sensory processing, and motor skills across 24 studies. Reference: PMC10955541

Your Therapeutic Toolkit: 9 Material Categories
Important: This card provides the overview. Steps 1–6 in Act III will guide you through exactly how and when to use each material. Start with the essentials — you can build your toolkit over time.
# | Material | What It Does | Price Range | Canon | |
1 | Grounded Vestibular Equipment | Movement input while maintaining ground contact — sit-and-spins, wobble boards, balance cushions | ₹800–3,500 | ||
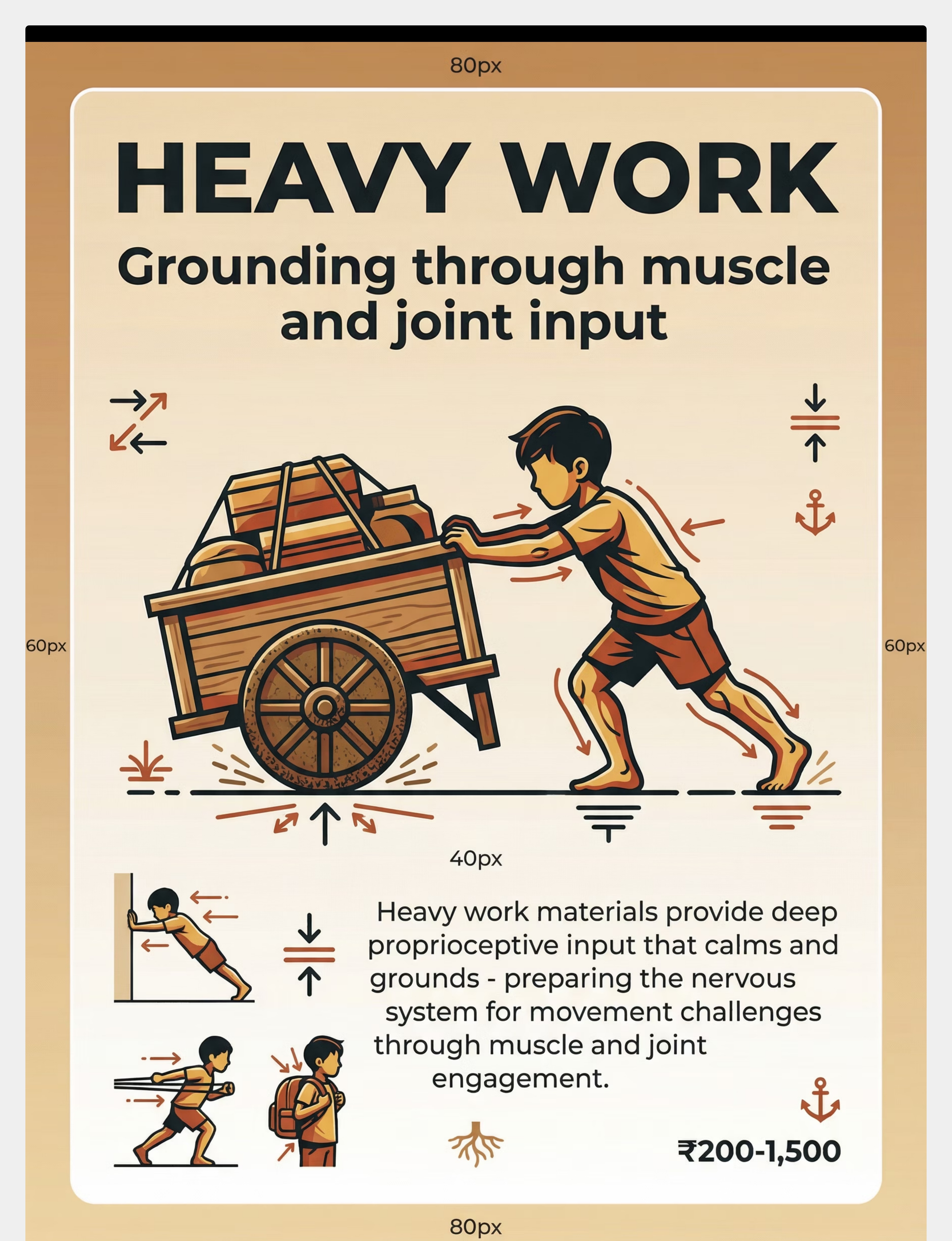
2 | Heavy Work Materials | Deep proprioceptive input that calms and organises the nervous system before movement challenges | ₹200–1,500 | ||
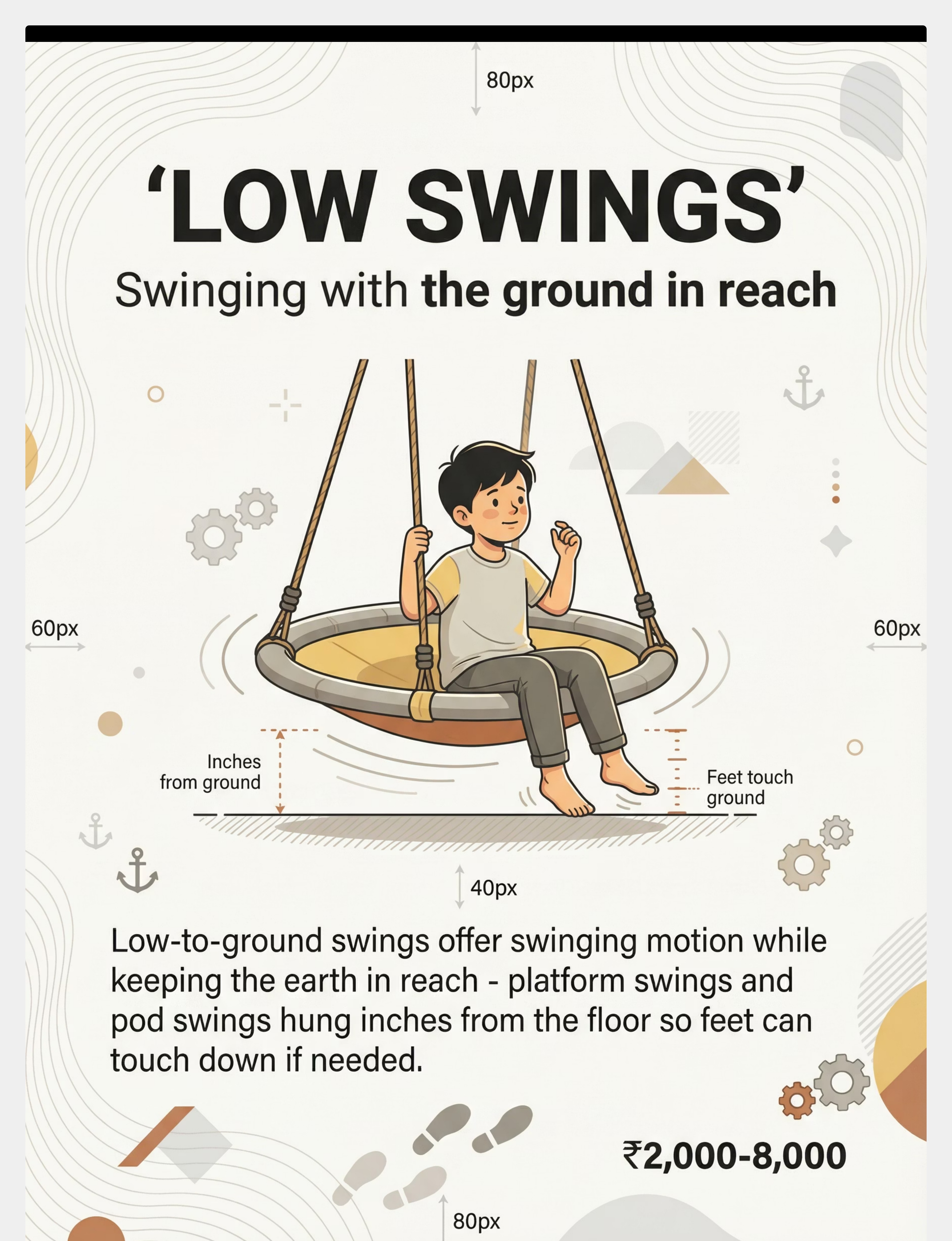
3 | Low-to-Ground Swings | Swinging motion with ground in reach — platform swings and pod swings hung inches from floor | ₹2,000–8,000 | ||
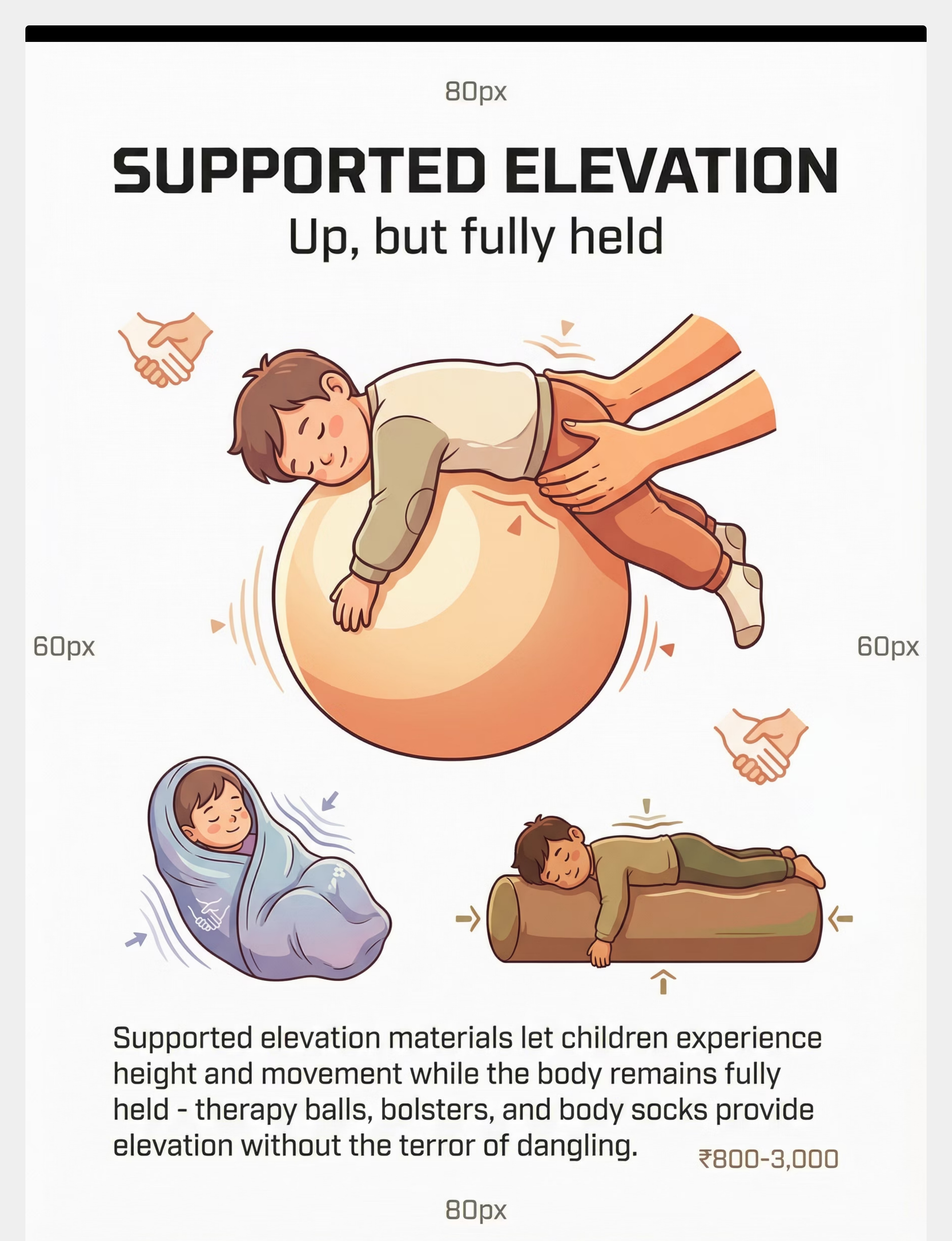
4 | Supported Elevation Materials | Height experience while body remains fully held — therapy balls, bolsters, body socks | ₹800–3,000 | ||
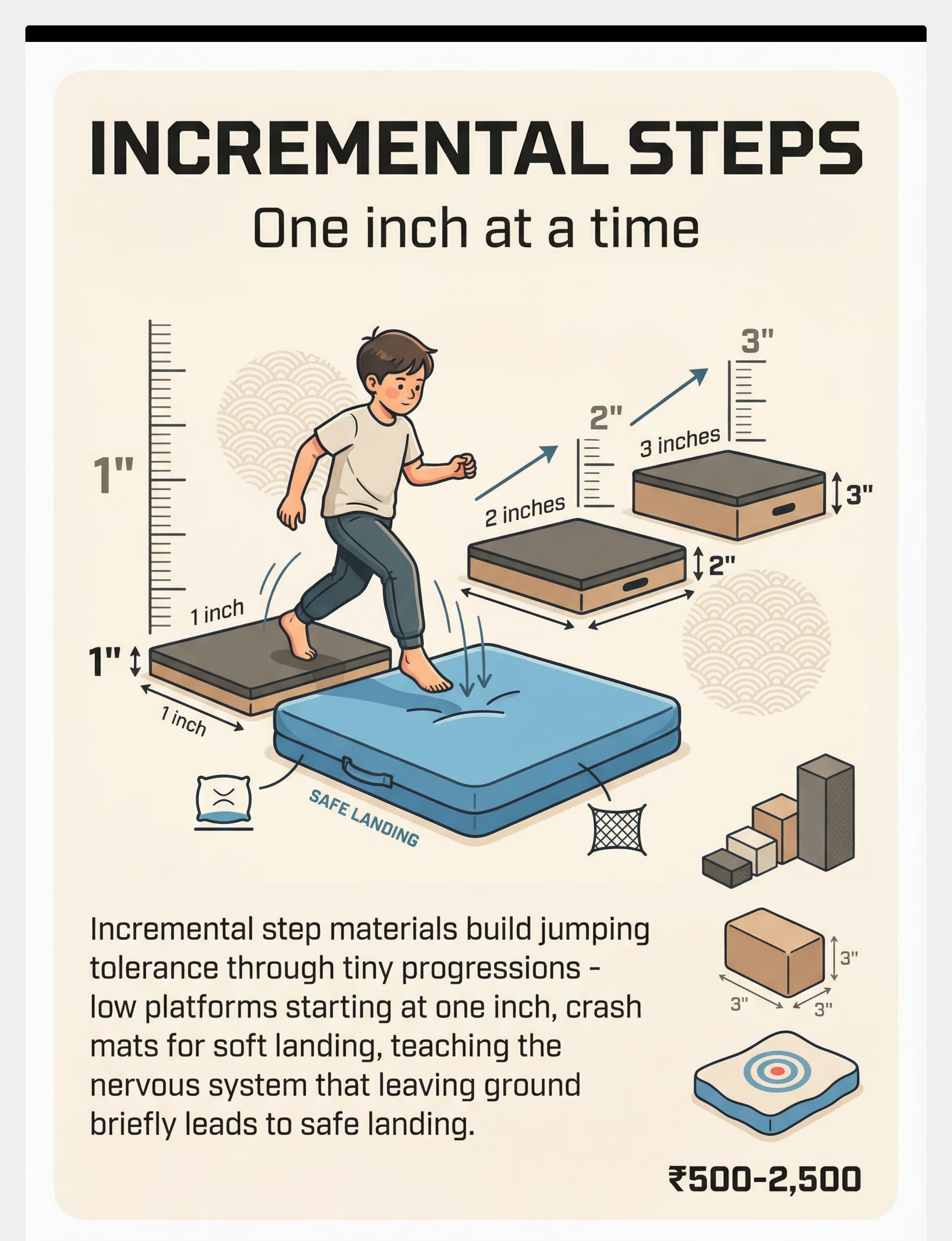
5 | Incremental Step Materials | Build jumping tolerance through tiny progressions — platforms starting at 1 inch, crash mats | ₹500–2,500 | ||
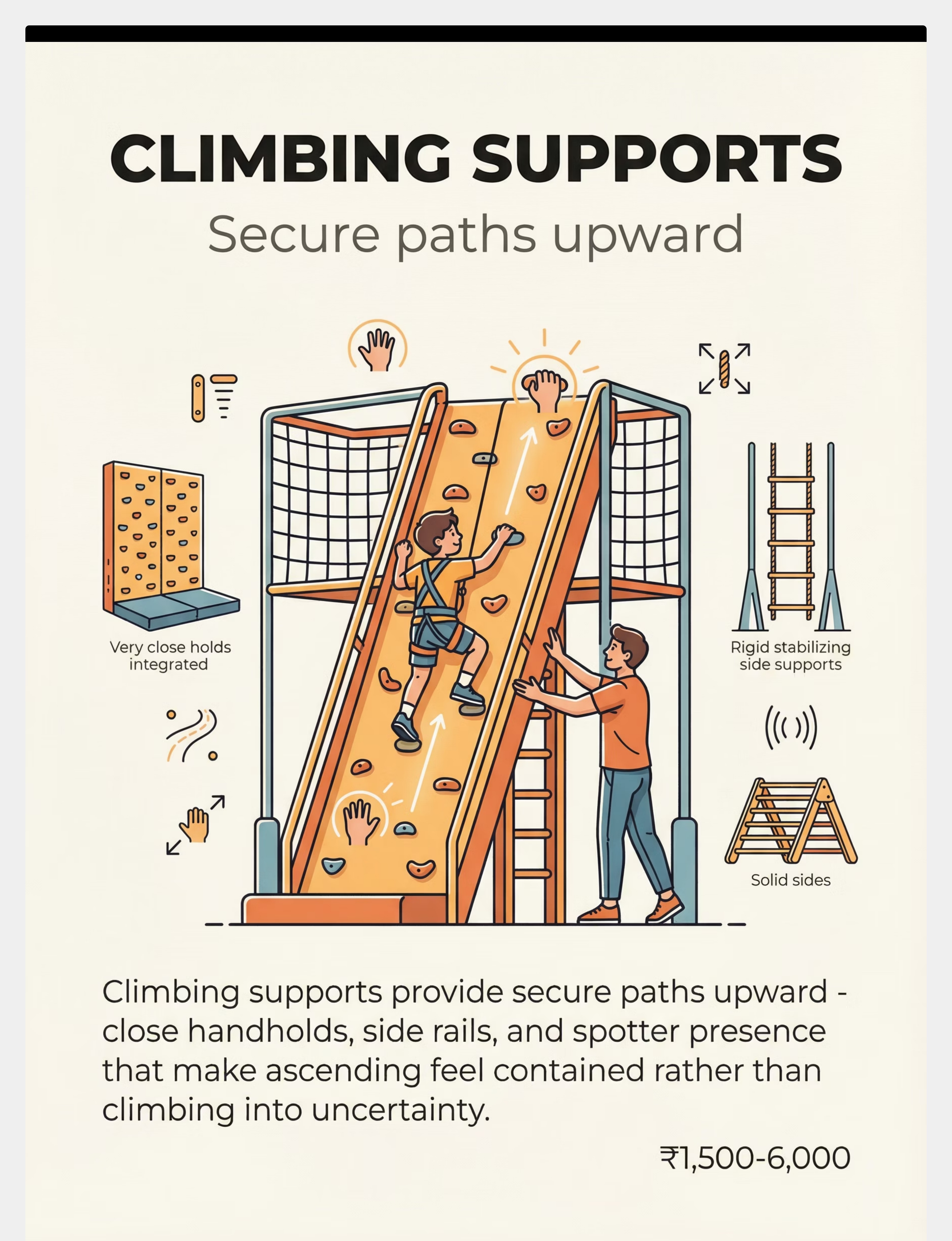
6 | Climbing Supports | Secure paths upward — close handholds, side rails, spotter presence | ₹1,500–6,000 | ||
7 | Weighted/Compression Supports | Body feedback when ground is gone — vests, squeezes, pressure that say "you are held" | ₹600–3,500 | ||
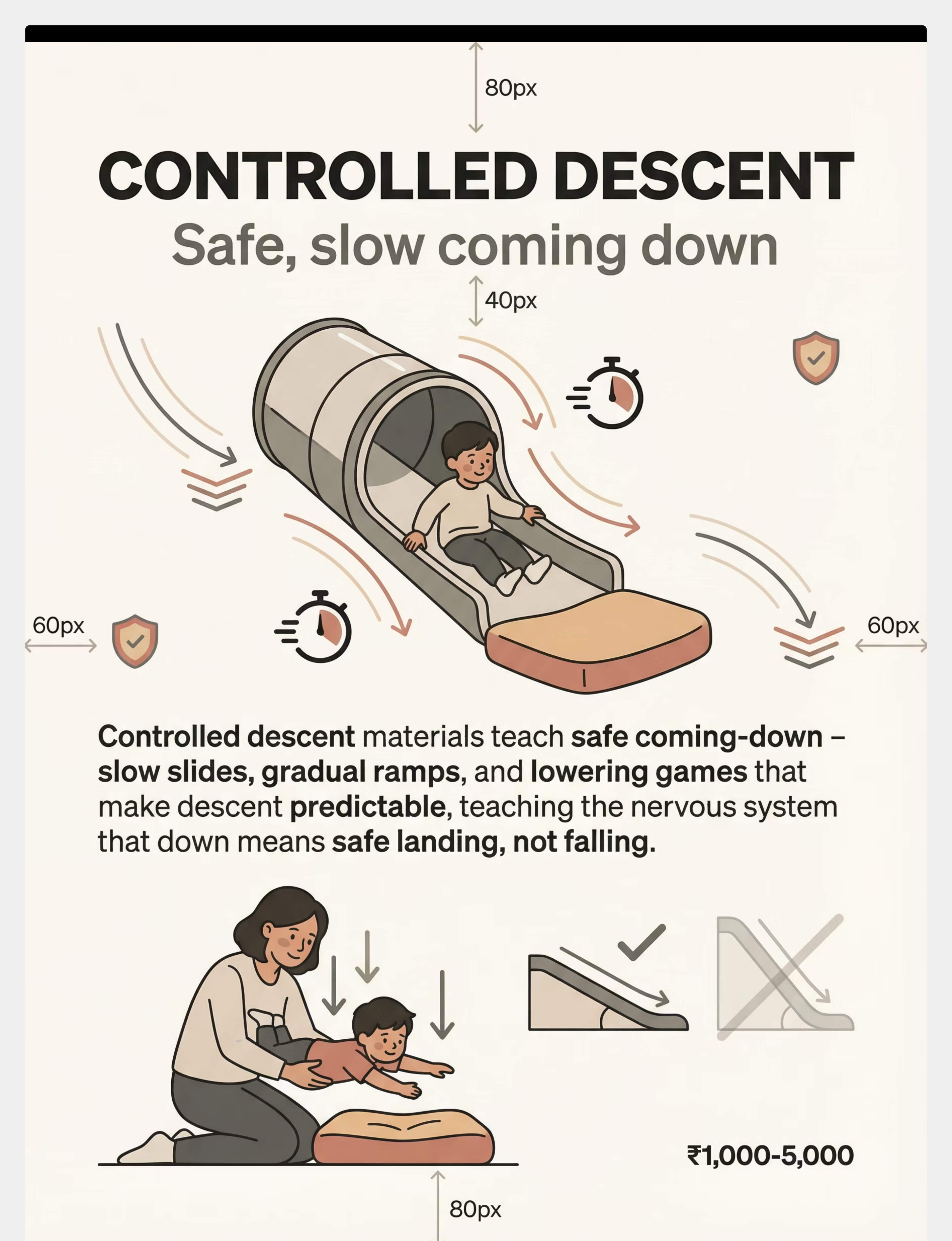
8 | Controlled Descent Materials | Safe, slow coming down — tunnel slides, gradual ramps, lowering games | ₹1,000–5,000 | ||
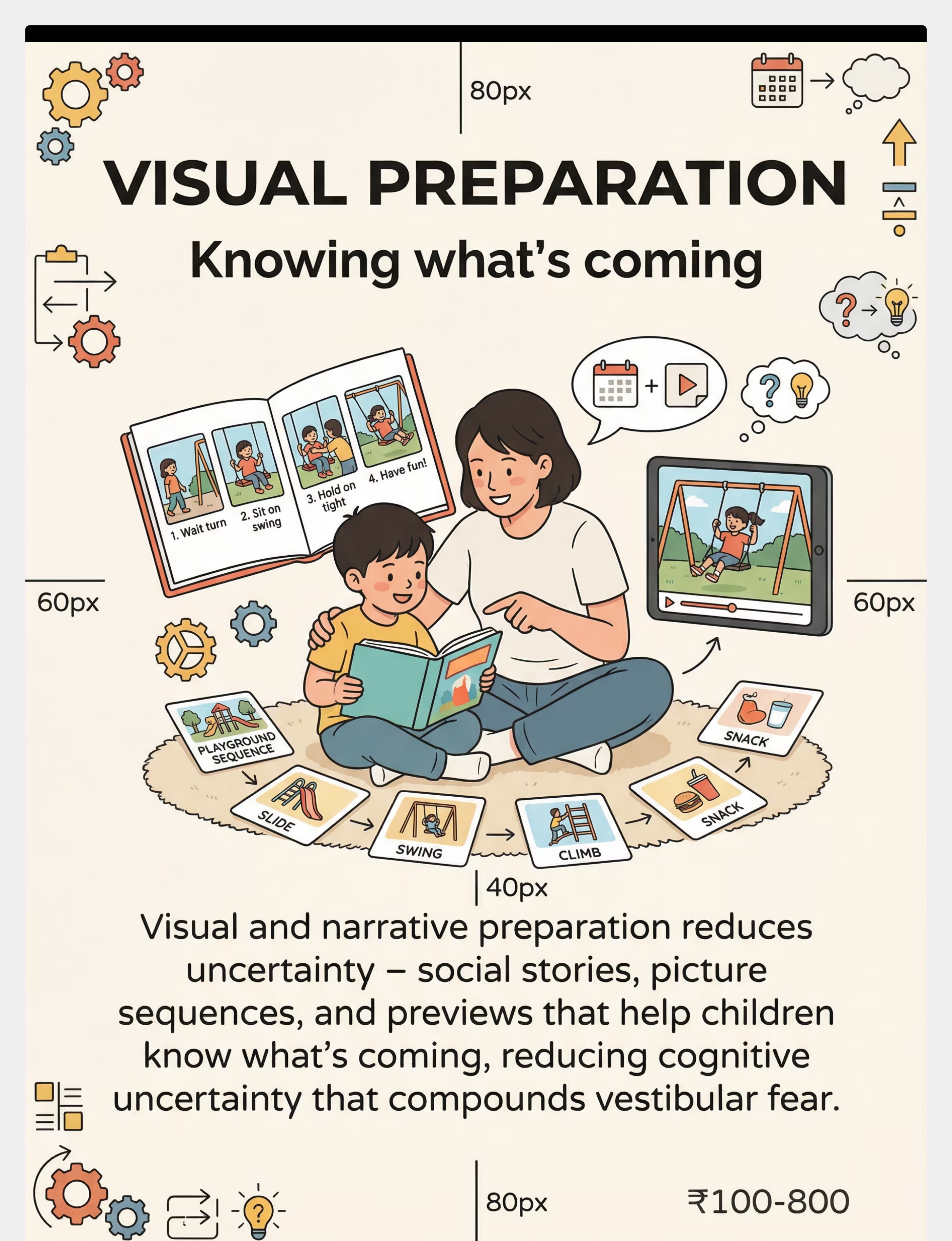
9 | Visual & Narrative Preparation | Knowing what's coming — social stories, picture sequences, previews that reduce cognitive uncertainty | ₹100–800 |
✅Pinnacle Recommends Starters: Wobble cushion (₹800–1,200) + Heavy work (often ₹0 — carrying, pushing, pulling household items). Total investment range: ₹100–8,000.

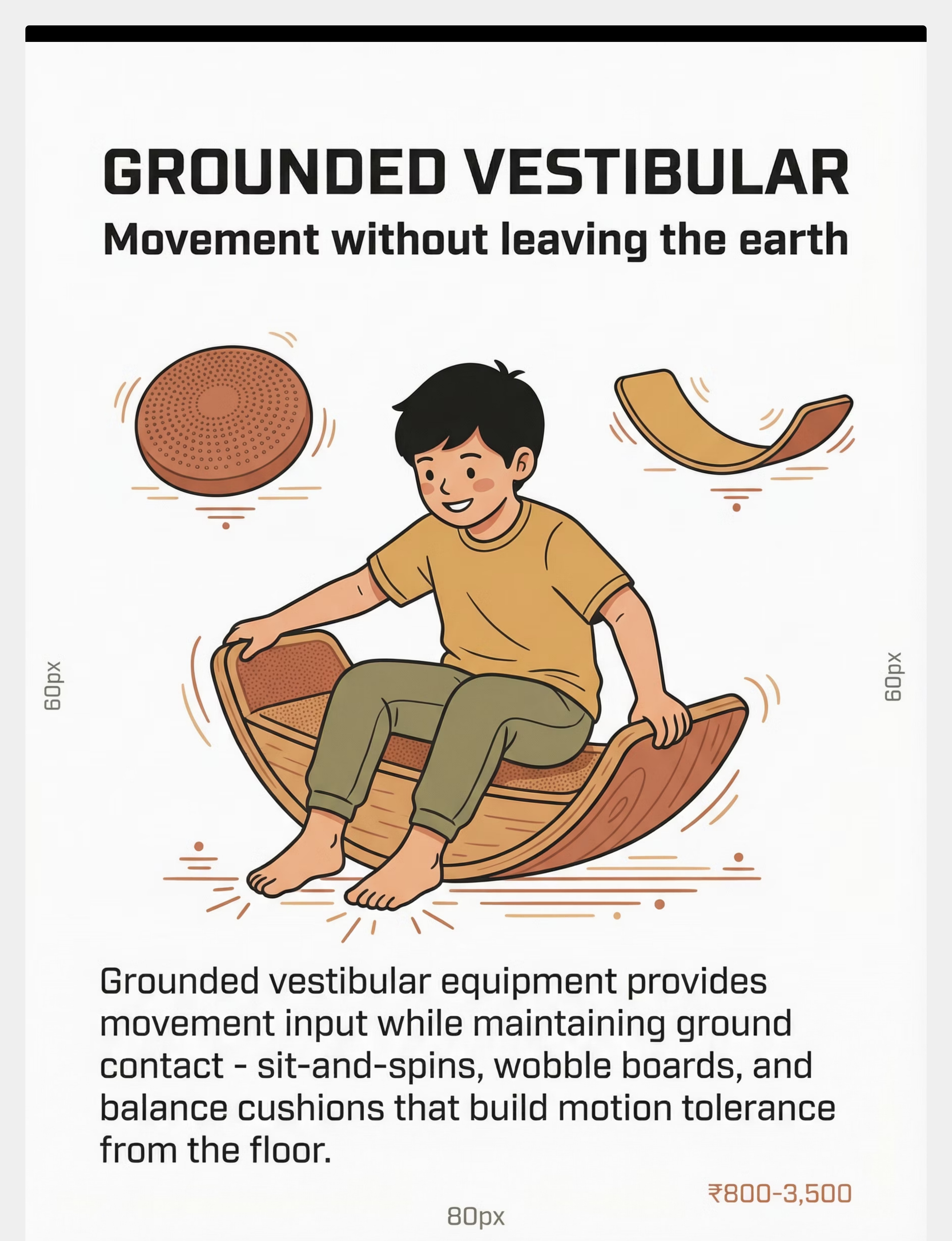
Material 1: Grounded Vestibular Equipment
Category 1 of 9
₹800–3,500
Starting Point for All Children

What It Is
Wobble boards, balance cushions, sit-and-spins, and rocking boards that provide vestibular movement input while both feet remain on the floor. The ground is always RIGHT THERE — making these the safest first vestibular tools.
Why It Works
Grounded vestibular equipment introduces the sensation of movement without the terror of elevation. The child's brain receives vestibular input while proprioceptive anchors (feet on floor, hands on surface) continuously confirm safety. Over time, the vestibular system begins to distinguish "movement" from "danger."
How to Use It
- Begin with child seated on wobble cushion on the floor
- Parent holds child's hands gently — support, not control
- Let child initiate the rocking at their own pace
- Progress to standing on balance board with wall support
- Introduce sit-and-spin when seated vestibular input is mastered

Material 2: Heavy Work Materials
Category 2 of 9
₹200–1,500 (or ₹0 with household items)
Daily Use — Non-Negotiable
Heavy work — activities that push deep pressure through joints and muscles — is the cornerstone preparation for every vestibular session. It calms the nervous system, organises sensory processing, and creates the regulatory foundation from which vestibular work becomes possible. Every session begins here.
Wall Pushups
Child faces wall, pushes with both hands. 10 repetitions. Free, always available, immediately organising.
Furniture Pushing
Push a heavy chair or ottoman across the room. Provides sustained joint compression — a powerful regulator.
Weighted Carrying
Backpack with books (5–10% body weight), grocery bags, laundry basket. 3 lengths across the room.

Material 3: Low-to-Ground Swings
Category 3 of 9
₹2,000–8,000
Introduce After Level 1 Mastery
What It Is
Platform swings and pod swings hung so close to the floor that the child's feet can touch the ground at any point during the swing. This crucial design feature — ground within reach — is what makes this tool accessible to gravitationally insecure children.
Why It Works
The vestibular system receives linear and rotational movement input while the proprioceptive system maintains its ground-contact anchor. The child experiences "swinging" without the terror of being unreachably airborne. Over multiple sessions, the swing height can gradually increase — one inch at a time.
How to Use It
- Hang swing so feet touch floor throughout entire arc
- Introduce with child seated, parent standing beside — not behind
- Let child self-propel first; then offer one gentle parent push
- Allow child to stop the swing by touching feet to floor at any time
- Over weeks, raise height by 1 inch as tolerance builds


Material 4: Supported Elevation Materials
Category 4 of 9
₹800–3,000
Level 2 — Full Body Support Throughout
Supported elevation materials allow the child to experience the sensation of being "up" — of the body being away from the floor — while remaining in full physical contact with the parent or caregiver throughout. This is the critical bridge between grounded vestibular work and true elevation tolerance.
Therapy Ball (Large)
Child lies draped over ball, belly-down. Parent holds hips firmly. Gently rock the ball side to side. Child's hands may touch floor. Full body contact with ball throughout — the elevation is experienced without free-space fear.
Body Sock
Lycra body sock provides deep proprioceptive feedback as child moves inside. Explores tilting and rolling while completely contained. Reduces the "falling into space" sensation with full-body compression input.
Scooter Board
Child lies flat on scooter board, parent provides gentle push. Body is fully supported. Introduces linear vestibular movement with ground immediately accessible.
Material 5: Incremental Step Materials
Category 5 of 9
₹500–2,500
Level 3 — Feet Briefly Leave Ground 1–3 Inches

The Principle of One Inch
Incremental step materials are precisely what the name suggests — platforms, stackable steps, and crash mats that create controlled, measurable elevation in tiny increments. A child who is terrified of a 12-inch step may have zero difficulty with a 1-inch step. That 1 inch is where neurological trust-building begins.
The Progression
- Week 1–2: Step onto platform of 1 inch height and immediately step back down
- Week 3–4: Stand on platform for 5–10 seconds, then step down
- Week 5–6: Step off platform onto crash mat — controlled "jump"
- Week 7+: Increase height by 1 inch per mastered session
DIY Version
Sturdy hardback books, yoga blocks, or folded towels stacked to 1–3 inch heights. Place crash mat (folded blankets) directly below. Zero cost.

Material 6: Climbing Supports
Category 6 of 9
₹1,500–6,000
Level 4 — Active Climbing With Full Spotter Support
Climbing supports provide a structured, predictable path upward — with handholds close together, side rails within reach, and an ever-present spotter. The critical insight is that gravitationally insecure children can tolerate climbing when the return path to ground is clearly visible and immediately accessible at every rung.
Pikler Triangle
Rungs closely spaced; parent stands at side. Child climbs 1–2 rungs, pauses, comes back down. The descent is practised before height is increased.
Step Stool With Rails
2–3 steps with side rails. Child holds both rails. Step up 1, step back down. Immediate ground return path visible at all times.
Sofa Arm Climbing
Low household sofa arm provides a 12–18 inch climbing height with large landing surface. Free. Familiar environment reduces novelty anxiety.
Critical principle: Master descent before increasing height. A child who can come back down confidently will climb more willingly. The fear is almost always about the descent, not the ascent.
Material 7: Weighted & Compression Supports
Category 7 of 9
₹600–3,500
Use During Any Level — Especially During Elevation
What These Materials Say to the Body
When your child's feet leave the ground, their proprioceptive system loses its primary anchor. Weighted and compression supports provide a substitute anchor — deep pressure input that continuously tells the nervous system: "You are held. You are bounded. You are safe."
This is not restraint. It is sensory information. Pressure is the proprioceptive language of safety.
How to Use Each
- Compression vest: Wear during sessions involving any elevation. Put on before getting on equipment, remove after returning to ground.
- Weighted lap pad: Use during grounded vestibular sessions for calming proprioceptive input.
- Body sock: Full-body compression for children who need maximum proprioceptive input before elevation work.
- Firm bear hug: Parent-provided, immediate, free. 10-second squeeze = significant proprioceptive anchor.
- Filled backpack: 5–10% body weight worn during any elevation activity as DIY alternative.

Material 8: Controlled Descent Materials
Category 8 of 9
₹1,000–5,000
The Return Path to Ground — Master This First
If climbing is about going up, controlled descent is about the neurological act of returning to ground safely. For gravitationally insecure children, the descent is often more frightening than the ascent — because it involves the unpredictable sensation of falling, however slow and supported. Controlled descent materials make the return to ground predictable, slow, and child-directed.
1
Tunnel Slide (Low)
Child controls entry and exit speed by bracing legs. The tunnel walls provide proprioceptive contact throughout — reducing the "free fall" sensation of open slides.
2
Gradual Ramp
Inclined surface at 10–15 degrees. Child walks down rather than slides. Full foot contact with surface throughout. The slowest, most controllable descent path.
3
Lowering Games
Parent slowly lowers child from a seated elevated position to the floor. Child controls the speed by holding parent's arms. "Slow as a turtle" narration during descent.
4
Step-Down Sequence
From 2-inch platform: place one foot down, feel ground, transfer weight, bring second foot. One step at a time, narrated. "One foot touches ground. Feel it? Now the other foot."
Material 9: Visual & Narrative Preparation
Category 9 of 9
₹100–800 (or free)
Use Before Every Session
Why Cognitive Preparation Reduces Fear
Uncertainty amplifies the vestibular fear response. When a child doesn't know what's coming, the amygdala pre-activates a threat response — before any movement has occurred. Visual and narrative preparation eliminates uncertainty, allowing the child to approach movement activities with their cognitive brain engaged rather than solely their threat-detection system.
Tools
- Social stories: Simple 4–6 page illustrated booklets showing the activity sequence
- Phone photos: Photos of your specific equipment taken before the session
- Verbal narration: "First we'll do wall pushups. Then we'll try the wobble cushion. Then we're all done."
- Video modelling: Short clips of a child using the same equipment
- Hand-drawn sequence: Simple stick figure drawings of the session steps
When to Use
Always. Begin preparation 10–15 minutes before the session. Revisit the sequence with the child 2 minutes before starting. This is the lowest-cost, highest-impact preparation tool in the toolkit.

Zero-Cost Versions: Every Family Can Start Today
Every child deserves intervention regardless of economic status. This is the WHO/UNICEF inclusion principle in action. The following household substitutes deliver comparable therapeutic input to their clinical-grade equivalents.
Clinical Material | Household Substitute | Why It Works | |
Wobble cushion (₹800) | Partially inflated beach ball placed on chair | Similar unstable seating surface for vestibular input | |
Balance board (₹1,500) | Sturdy pillow on floor — child stands on it | Creates mild balance challenge from grounded position | |
Heavy work equipment (₹500) | Grocery bags, pushing furniture, bucket carrying, wall pushups | Same deep proprioceptive input through joints and muscles | |
Low swing (₹2,000) | Blanket hammock held by two adults close to floor | Contained swinging sensation near ground | |
Therapy ball (₹800) | Large pillow stack — child lies over them while you rock gently | Approximates supported elevation with body contact | |
Incremental steps (₹500) | Sturdy books, yoga blocks, folded towels at 1–3 inch heights | Graduated stepping heights at zero cost | |
Climbing support (₹1,500) | Sturdy household step stool with adult spotting, sofa arm | Short, supported climbing experience in familiar setting | |
Weighted vest (₹600) | Filled backpack (5–10% body weight), firm bear-hug technique | Deep pressure proprioceptive input during elevation | |
Social stories (₹100) | Hand-drawn picture sequence, phone photos, verbal narration | Same cognitive preparation and predictability function |
For children with severe gravitational insecurity, clinical-grade therapy swings with adjustable heights and professional-grade crash mats provide safety margins that household substitutes cannot fully replicate. Consult your OT for assessment. | Reference: WHO NCF (2018) | PMC9978394

⚠️ Safety Gate: Read This Before Starting
🔴 DO NOT PROCEED IF:
- Child has recent head injury, concussion, or ear infection
- Child is running a fever or is physically unwell
- Child is in active meltdown or severe dysregulation
- Equipment is damaged, unstable, or not age-appropriate
- No adult is present to supervise
- Child has been diagnosed with seizure disorder without medical clearance
🟡 MODIFY THE SESSION IF:
- Child had a difficult day or is emotionally fragile → Use only grounded equipment + heavy work
- Child is hungry or tired → Food/rest first
- Environment is noisy or chaotic → Simplify to quiet room, one activity
- Child shows increased anxiety → Add extra visual preparation time
🟢 PROCEED WHEN:
- Child is fed, rested, and in a regulated state
- Environment is calm, safe, and distraction-free
- Equipment is inspected and age-appropriate
- Adult is present and focused (phone away)
- Child has had heavy work warm-up (minimum 5 minutes)
🚨STOP IMMEDIATELY IF: Child shows nausea, dizziness, or loss of colour | Child becomes non-responsive during vestibular input | Fear response escalates despite modified approach | Any equipment instability. CRITICAL PRINCIPLE: Forcing movement INCREASES fear and sensitisation. All vestibular input must be child-initiated and child-controlled. The child sets the pace. Always. | Reference: DOI: 10.1007/s12098-018-2747-4
Your Therapy Space: 5-Minute Setup
Room Layout — What Goes Where
- Crash mat / soft landing zone (centre) — Folded blankets, gym mat, or crash pad
- Grounded vestibular station (left of centre) — Wobble cushion or balance board on carpet
- Heavy work zone (near wall) — Wall for pushups, space for carrying/pushing
- Incremental step area (near crash mat) — Low platforms with soft landing below
- Parent position (within arm's reach of all stations) — Never more than one arm length from child
- Clear zone — Remove sharp furniture edges, hard objects in fall radius, loose rugs, distracting toys
Environmental Checklist
- ✅ Flooring: Carpet or mat. No hard/slippery floors.
- ✅ Lighting: Natural, calm. No harsh fluorescents.
- ✅ Sound: Quiet. TV off. Music optional — low, calming only.
- ✅ Space: Minimum 8×8 feet clear area around equipment.
- ✅ Emergency: Clear path to exit. First aid kit accessible.
"The environment is the first intervention. Get the space right and you've prevented 80% of session problems."
Reference: Sensory Integration Theory (Ayres): Environmental setup is a core principle. Meta-analysis confirms 1:1 individual treatment in structured environment was most effective. Reference: PMC10955541

60-Second Readiness Check ✓
Before every session, complete this check. It is observable — not subjective. If you are uncertain about any item, default to the more conservative option. A session started right is a session that succeeds.
1
Fed
Child has eaten within the last 2 hours. Hunger dramatically reduces regulatory capacity.
2
Rested
No signs of exhaustion — alert eyes, upright posture, responsive to conversation.
3
Regulated
No meltdown in the last 30 minutes. Breathing is even. Body is not in high-alert state.
4
Healthy
No fever, no ear infection, no recent illness. Vestibular input is contraindicated when unwell.
5
Willing
Child is not actively resisting or crying before you begin. Willingness ≠ enthusiasm. Neutral acceptance counts.
6
Heavy Work Done
Minimum 5 minutes of proprioceptive input completed — carrying, pushing, wall pushups, or similar.
7
Space Ready
Environment matches Card 12 setup requirements. Crash mat in place. Clear zone confirmed.
✅ All 7 Checked → GO
Begin with Step 1 (Card 14)
⚠️ 5–6 Checked → MODIFY
Grounded vestibular + heavy work only. Skip elevation. Short session (5–7 min).
⏸️ 4 or Fewer → POSTPONE
Deep pressure blanket, slow rocking in parent's lap, gentle heavy work only. Try tomorrow.

Step 1: Grounding Through Heavy Work (5–7 Minutes)
Every Session Begins Here — Non-Negotiable
"Let's do our strong work! Can you help me push the couch? Let's see how strong you are today!"
Proprioceptive input through joints and muscles calms the vestibular system. Heavy work floods the nervous system with organising input that counterbalances vestibular threat signals. This is the grounding anchor before any movement challenge — the physiological preparation that makes everything that follows possible.
Acceptance
Child engages with the activity, builds rhythm. May begin to anticipate and enjoy the heavy work routine after several sessions.
Calming
Breathing deepens, body tension reduces, movements become organised. You can see the regulation happening in real time.
Readiness
Child appears grounded, present, and calm after 5+ minutes. Eyes are alert, body is less rigid. This is the window for vestibular introduction.
If child refuses all heavy work options: Don't force. Offer deep pressure blanket time instead. Sometimes the session IS just heavy work. That is still progress. Timing: 5–7 minutes minimum.

Step 2: Grounded Vestibular Input — Movement Without Leaving Earth (3–5 Minutes)
Step 2 of 6
Material 1 in Action
"Want to try the wobbly cushion? I'll hold your hands. You control it."
Level A — Sitting Vestibular (Safest Start)
Place wobble cushion on floor. Child sits on it. Parent holds child's hands. Let child rock/wobble at their own pace. The floor is RIGHT THERE beneath the cushion.
Level B — Standing Vestibular (When A Is Comfortable)
Child stands on wobble cushion or balance board. Parent's hands always available. Movement is gentle, child-controlled. Feet stay on board throughout.
Level C — Rotation (When B Is Comfortable)
Sit-and-spin on floor. Child controls speed — always. Parent sits nearby. Slow, gentle, child-directed. Stop at first sign of nausea or distress.
✅ Engagement
Smiling, relaxed body — keep going
⚠️ Tolerance
Neutral, going along — acceptable, continue gently
🛑 Avoidance
Stiffening, pulling away — STOP, return to heavy work
Step 3: The Therapeutic Challenge — Choosing Your Child's Level Today (5–8 Minutes)
Step 3 of 6 — Core Therapeutic Action
Based on your child's current comfort, select one level to work at today. Never advance levels within a single session. The child's signals — not the calendar — determine progression.
🟢 Level 1 — Grounded
Child remains on the ground throughout. Wobble cushion rocking seated → Balance board standing with hand support → Rocking board gentle sway. Materials: #1 + #2. Duration: 5–8 minutes.
🔵 Level 2 — Supported Elevation
Child experiences being "up" while fully body-supported. Lying over therapy ball with parent holding hips → Body sock exploration → Scooter board lying flat. Materials: #4 + #7. Duration: 3–5 minutes.
🟡 Level 3 — Controlled Low Elevation
Feet briefly leave ground by 1–3 inches. Step off 1-inch platform → Low swing (feet can touch ground) → "Airplane" slow lowering. Materials: #5, #3, #8. Duration: 2–3 minutes with breaks.
🟠 Level 4 — Climbing and Descent
Active climbing with support and controlled return to ground. 2–3 rungs on Pikler triangle with spotter → Low slide with supported descent → Step up 3–4 inches and jump to crash mat. Materials: #6, #8, #7. Duration: 3–5 minutes with rest breaks.
CRITICAL: The child chooses. The child sets the pace. ❌ Never advance levels within a single session ❌ Never hold the child on equipment when they want off ❌ Never compare to peers or siblings ❌ Never promise rewards for "trying harder." Reference: PMC10955541

Step 4: Therapeutic Dosage — 3 Good Reps > 10 Forced Reps
Step 4 of 6
Quality of engagement, not quantity of repetitions, is the therapeutic measure. A child who completes 3 repetitions while relaxed and engaged receives more neurological benefit than 10 repetitions completed in distress.
Level | Target Reps | Rest Between | What Counts as a Rep | |
Level 1 | 5–8 cycles | 30 seconds | One complete weight shift or rotation cycle | |
Level 2 | 3–5 sequences | 1 minute | One therapy ball roll-and-return or body sock exploration | |
Level 3 | 2–4 sequences | 1–2 minutes | One step-off-and-land or one swing set (30 sec) | |
Level 4 | 2–3 cycles | 2 minutes | One complete up-and-down with controlled descent |
Variation Options to Maintain Engagement
- Change direction of movement (forward/backward, left/right)
- Add a playful element (reach for a toy while on wobble cushion)
- Sing a counting song during repetitions
- Change body position (seated → kneeling → standing on same equipment)
"3 good repetitions where the child is engaged and regulated are worth more than 10 repetitions where the child is enduring. Watch the face. Follow the signals."
Step 5: Celebrate the Attempt, Not Just the Success
Step 5 of 6 — Reinforce Within 3 Seconds
For Attempting
"You tried the wobble cushion! Your body is learning something new!"
For Tolerating
"You sat on that for so long! Your brave muscles are getting stronger!"
For Progressing
"You stepped off that platform! Your feet touched the ground and you were SAFE!"
For Persistence
"Even though it felt scary, you stayed. That takes enormous courage."
✅ Reinforce Using
- Verbal praise (always immediate, always specific)
- High five or special handshake
- Token on visual progress chart
- Preferred activity after session
- Sticker on "Bravery Board"
❌ Never Reinforce By
- Saying "See? That wasn't so bad" — this invalidates the real fear
- Promising bigger rewards for bigger steps — creates performance pressure
- Comparing to other children — "Look, that boy can do it"
- Withdrawing affection if child refuses
"The child who sits on a wobble cushion for 10 seconds after weeks of refusal deserves the same celebration as the child who climbs the jungle gym."
Step 6: Safe Landing — The Cool-Down (2–3 Minutes)
Step 6 of 6 — Always Close Every Session
Transition Warning (60 seconds before end):"Two more wobbles, then we're all done with movement time. Then we can [preferred calming activity]."
This structured cool-down sequence closes the vestibular input window, returns the nervous system to baseline, and provides a predictable transition that builds session-to-session trust. The ritual of the cool-down becomes as regulating as the session itself.
If Child Resists Ending (Wants to Continue)
This is a WIN — the child is enjoying vestibular input. Allow 2 more repetitions, then firm close. Consistency in session length builds predictability.
If Child Resists Ending (Is Dysregulated)
Skip cool-down activities. Move directly to deep pressure comfort. Hold firmly, speak slowly, wait for regulation before transitioning.
Visual timer and transition support evidence: Visual supports are classified as evidence-based practice for autism (NCAEP, 2020).
60 Seconds of Data Now Saves Hours of Guessing Later
Record these 3 data points within 60 seconds of session end. Over time, this data reveals which levels are mastered, how tolerance duration is trending, what conditions produce the best sessions, and when to consult your OT for professional reassessment.
Data Point 1 — Level Achieved Today
☐ Level 1 (Grounded) | ☐ Level 2 (Supported) | ☐ Level 3 (Low Elevation) | ☐ Level 4 (Climbing)
Data Point 2 — Tolerance Duration
Longest single period of vestibular engagement without distress: _____ seconds
Data Point 3 — Child State Rating
☐ Enjoyed (smiling, relaxed, wanted more) ☐ Tolerated (neutral, no distress) ☐ Endured (mild discomfort, completed with support) ☐ Refused (modified to heavy work only)
Advancement Rule
3 consecutive "Enjoyed" sessions at a given level = ready to introduce the next level in the following session.
Download Your Tracker
ABA Data Collection Standards: Continuous measurement (frequency, duration) as standard practice for behaviour-analytic intervention tracking. References: BACB Guidelines + Cooper, Heron and Heward (Applied Behavior Analysis)
When Sessions Go Sideways: This Is Not Failure — It's Data
Every session that doesn't go to plan is a session that teaches you something essential about your child's nervous system. There are no failed sessions — only data-rich ones. Here are the most common challenges and exactly what to do.
Child Refused All Equipment Today
Why it happened: Regulatory state wasn't ready, or environment triggered anticipatory anxiety. What to do: Next session, extend heavy work to 10 minutes. Offer only the wobble cushion. If still refused, the session IS heavy work today. That's data and that's progress.
Fine on Wobble Cushion But Panicked on Therapy Ball
Why it happened: Supported elevation triggered a different fear pathway. Feet-off-ground threshold was crossed. What to do: Return to grounded activities. Before trying the ball again, use it on the floor — child sits on floor and pushes/touches/lies beside it. Proximity without elevation.
Climbed 2 Rungs Then Froze and Couldn't Come Down
Why it happened: Ascending felt manageable but descent triggered fall-fear. What to do: Next session, practise only going up 1 rung and immediately coming back down. Descent mastery precedes height increase.
Physically, calmly support the child down.
Child Had a Meltdown During the Session
Why it happened: Vestibular input overwhelmed regulatory capacity. What to do: Stop all movement immediately. Deep pressure. Wait for full regulation. Document the trigger. Next session: work one level below the meltdown point.
No Progress After 4 Weeks
Why it happened: Inappropriate level selection, insufficient preparation, or underlying condition requiring professional assessment. What to do: Book a professional OT assessment. Call Pinnacle FREE Helpline: 9100 181 181.
"Session abandonment is not failure — it's data. Every 'no' from your child tells you exactly what their nervous system needs next."

No Two Children Are Identical: Personalising This Protocol
This protocol is a framework, not a prescription. Use it as a starting point and adapt continuously based on your child's signals, sensory profile, age, and daily state. The best protocol is the one your specific child responds to.
← Easier Modifications
For bad days, early stages, younger children
- Only grounded vestibular equipment
- Shorter sessions (5–7 minutes total)
- More heavy work, less movement challenge
- Parent provides constant physical contact throughout
- One material per session only
Harder Modifications →
For breakthroughs and mastery consolidation
- Combine materials (weighted vest + low swing)
- Introduce mild unpredictability (parent adds gentle push)
- Transition from indoor to outdoor equipment
- Increase height by 1 inch per week
- Reduce adult support gradually (hand hold → finger touch → nearby → watching)
Sensory Seeker Variation
Some children with vestibular differences SEEK intense movement while still fearing elevation. Provide abundant grounded spinning/rocking (sit-and-spin, rotational equipment) while separately addressing elevation fear. These are two distinct pathways.
Sensory Avoider Variation
Children who avoid ALL movement need an even slower progression. Start with the child holding a wobble cushion (not sitting on it), then touching it with one foot, then standing on it while holding the wall. Each sub-step may take days.
Age Adaptations
Ages 2–3: Maximum adult support; grounded equipment only; heavy work primary. Ages 4–6: Introduce supported elevation and incremental steps; social stories effective. Ages 7–10: Verbal processing possible; child can participate in goal-setting; playground integration becomes social motivation.
Weeks 1–2: Building the Foundation
Progress Bar: 15%
Act IV: The Progress Arc
Progress in the first two weeks is quiet, internal, and neurological. You may not see dramatic behavioural changes yet — and that is exactly right. The vestibular system is beginning to recalibrate at the level of neural pathways. Trust what you cannot yet see.
✅ What You May See
- Increased tolerance for heavy work activities — child may start requesting them
- Reduced anxiety around grounded vestibular equipment (approaches rather than avoids)
- Willingness to watch other children on movement equipment (not participation yet)
- 5–10 second improvement in tolerance duration on wobble cushion
❌ What Is NOT Progress Yet
- Child jumping or climbing — this is weeks/months away
- Enjoying swings — far too early
- Being comfortable when picked up — this improves gradually over many weeks
"If your child tolerates the wobble cushion for 3 seconds longer than last week — that's real progress. The nervous system is rewiring. Be patient with the biology."
Weeks 3–4: Neural Pathways Forming
Progress Bar: 40%
Consolidation Phase
Between weeks three and four, families typically notice the first clear signs that something has shifted. The nervous system has begun to build new associations between movement and safety. These changes are subtle but deeply meaningful.
Child Anticipates Movement Sessions
May approach equipment independently — a profound shift from earlier avoidance. The movement session is becoming safe in the child's predictive model.
Wobble Cushion Tolerance Extends
30+ seconds without hand support — a measurable neurological milestone. The vestibular system is processing the input without triggering the full threat response.
Brief Lifting Tolerance
Child begins tolerating being lifted for 3–5 seconds without panic. This is the vestibular system beginning to trust the parent's body as a safe elevation platform.
Spontaneous Vestibular Seeking
Child spontaneously rocks in chair; reduced rigidity when parent picks child up; approaching (not yet using) playground equipment.
When to increase challenge: If the child shows "Enjoyed" ratings on 3 consecutive Level 1 sessions → Introduce Level 2 materials in the next session. Parent milestone: "You may notice you're calmer too. Your body is learning to trust the process alongside your child's body."
Weeks 5–8: Trust Building in Action
Progress Bar: 75%
Mastery Indicators — Observable and Measurable
Level 1 MASTERED When
☑️ Child uses grounded vestibular equipment independently for 2+ minutes ☑️ Heavy work is accepted and sometimes requested ☑️ No distress on any grounded equipment across 5 consecutive sessions
Level 2 MASTERED When
☑️ Supported elevation tolerated for 60+ seconds ☑️ Child allows body to be "up" while held without rigid clinging ☑️ Some elevation experiences generate positive responses
Level 3 EMERGING When
☑️ Child steps off 1–2 inch platform onto crash mat voluntarily ☑️ Low swing tolerated for 30+ seconds with feet-touch-ground available ☑️ "Airplane" lowering game produces smiles rather than fear
Generalisation Indicators — Skill Appearing in Other Contexts
- Steps off curb at park without panic
- Tolerates being carried briefly to car
- Watches other children swing without visible distress
- Accepts escalator with hand-holding (previously refused)
"Mastery of Levels 1–2 within 8 weeks is excellent progress. Some children reach this in 4 weeks. Others need 16. Both are success stories."
Systematic review (Children, 2024): Sensory integration intervention outcomes emerge across 8–12 week timelines. Reference: PMC11506176

You Did This. Your Child Grew Because of Your Commitment.
Your child came to this protocol terrified of leaving the ground. Through weeks of patient, consistent, scientifically-guided intervention — YOUR intervention, in YOUR home — their nervous system has begun to rewire.
Every wobble cushion session you facilitated. Every heavy work warm-up you led. Every time you stopped when your child needed to stop. Every time you celebrated a 3-second improvement. That is therapeutic intervention at the highest level. That is a parent becoming a clinician of their own child's development.
Family Celebration Suggestion
Return to the playground where your child once stood frozen. Watch them approach equipment — even if they don't use it yet. The approach IS the milestone.
Photo / Journal Prompt
Take a photo of your child with the wobble cushion or balance board. Compare it to how they responded in Week 1. Document the journey. This evidence matters — to you, to your OT, and to your child's future self.

Explore More in Vestibular and Motor Development
You already own materials for 4 of these 6 techniques. Browse the full Sensory Processing domain at → techniques.pinnacleblooms.org/sensory-processing/
A-077: Playground Equipment Engagement
Difficulty: Advanced | Materials you own: Climbing supports, visual preparation
A-080: When Movement Never Stops
Difficulty: Core | Materials you own: Grounded vestibular, heavy work
A-081: Motion Sensitivity and Car Sickness
Difficulty: Core | Materials you own: Weighted supports, visual preparation
A-082: Balance and Postural Confidence
Difficulty: Core | Materials you own: Balance boards, incremental steps
A-083: Slide Tolerance Building
Difficulty: Intermediate | Materials you own: Controlled descent, incremental steps
K-1020: Understanding Vestibular Processing
Difficulty: Introductory — Parent Education | Materials you own: Visual preparation

One Technique, One Domain, One Piece of a Larger Plan
Gravitational insecurity is one challenge within one domain of a 12-domain developmental map. Understanding how this technique connects to the broader picture helps you and your therapy team build a comprehensive developmental plan — not just address single skills in isolation.
1
★ Domain A — Primary
Sensory Processing — the direct target of this protocol
2
Domain F — Secondary
Gross Motor Development — through climbing, jumping, and balance skill building
3
Domain C — Tertiary
Social-Emotional — through playground participation with peers
4
Domain L — Long-Term
Community Integration — environmental confidence in public spaces, schools, parks
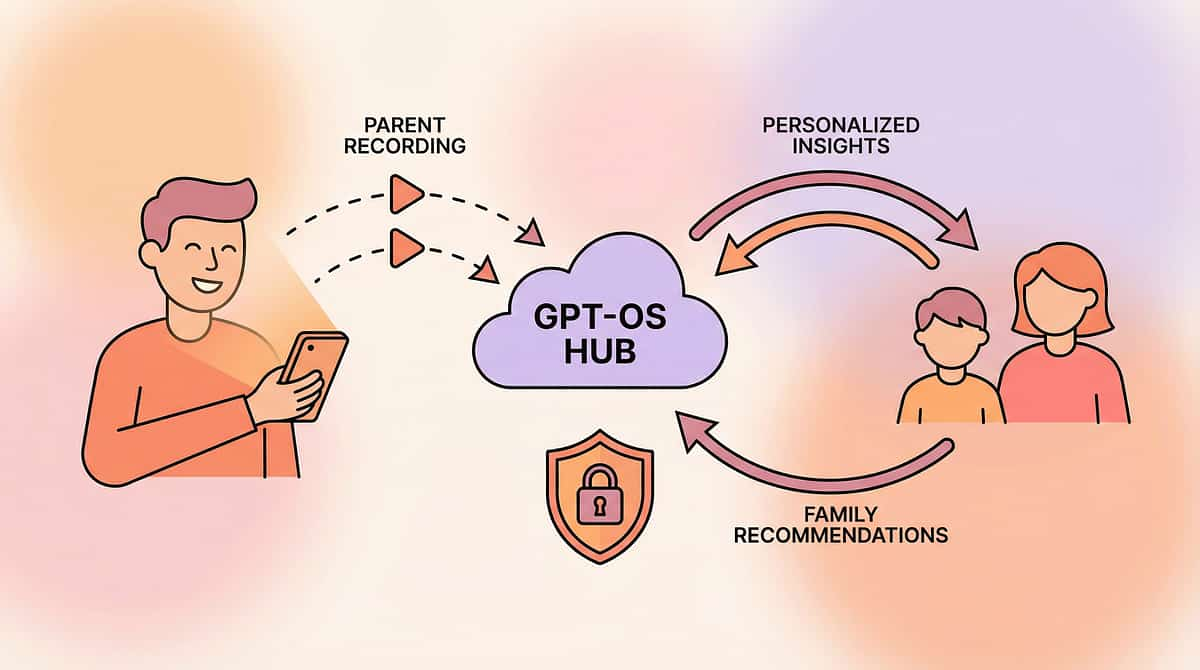
GPT-OS® Integration: See your child's full developmental profile across all 12 domains. → pinnacleblooms.org/enroll-autism-speech-aba-therapies-india | Reference: WHO NCF (2018) | UNICEF 2025 Country Profiles

From Terror to "I'm Flying": Real Family Journeys
Family Story 1
Before: "He screamed if his feet left the floor. Picking him up meant desperate clinging and crying. Swings were impossible." Journey: Started with wobble cushion — just sitting while parent held his hands. Months of heavy work before any elevation. Then a platform swing hung so low he could touch the floor. Then one inch off the ground on a step. After (2 years): "He swung on a regular playground swing for the first time at age seven. He was crying — but this time with joy. He said, 'I'm flying.'" — Parent, Pinnacle Network
Family Story 2
Before: "Our daughter wouldn't climb the two steps into our house without being carried. She was four." Journey: Daily heavy work (carrying the laundry basket became her favourite "job"). Wobble cushion during TV time. Incremental steps using stacked books. Visual preparation before every outing. After (8 months): "She climbed the playground ladder last month. Slowly, deliberately, with me spotting. But she climbed. She chose to climb." — Parent, Pinnacle Network
"Gravitational insecurity responds beautifully to patient, systematic intervention. The children who make the most progress are those whose parents understand that 1 inch of height gain represents a neurological revolution." — Senior OT, Pinnacle Blooms Network
Illustrative cases; outcomes vary by child profile.

From Fear to Mastery Starts With One Wobble Cushion
Validated by the Pinnacle Blooms Consortium
OT • SLP • ABA • SpEd • NeuroDev • CRO
Every milestone in this protocol starts with the same first step — a child who is fed, rested, and regulated, sitting on a wobble cushion while a parent holds their hands and says: "You control it." That's where the neurological revolution begins. Start today.
🟢 Start This Technique Today
Download the GPT-OS® Vestibular Grounding Protocol Guide. Begin with 5 minutes of heavy work + wobble cushion session. Track with the 3-data-point system. → Get Started
🔵 Book a Professional Assessment
AbilityScore® + Sensory Processing Assessment at your nearest Pinnacle centre. FREE Helpline: 9100 181 181 (16+ languages, 24/7). → Book Assessment
⚪ Explore Next Technique
A-080: 9 Materials That Help When Movement Never Stops. Browse all 12 developmental domains. → techniques.pinnacleblooms.org/sensory-processing/
20M+
Sessions
97%+
Improvement
70+
Centres
Preview of 9 materials that help when feet off ground scares Therapy Material
Below is a visual preview of 9 materials that help when feet off ground scares therapy material. The pages shown help educators, therapists, and caregivers understand the structure and content of the resource before use. Materials should be used under appropriate professional guidance.








Link copied!

From Fear to Mastery. One Technique at a Time.
Pinnacle Blooms Consortium
Clinical Research Organization | OT | SLP | ABA | SpEd | NeuroDev
A parent arrived on this page scared, confused, and exhausted. By now, they understand the science, have the materials, know the protocol, and see the path forward. This is what 20 million therapy sessions, 70+ centres, and thousands of clinicians working as one system can do — reach into a family's home and transform it into a therapeutic environment.
Every child deserves access to evidence-based intervention. Every parent deserves the knowledge to deliver it.
Built by Mothers. Engineered as a System.
Medical Disclaimer: This content is educational and does not replace assessment by a licensed occupational therapist, sensory integration specialist, or healthcare provider. Significant gravitational insecurity should be evaluated through comprehensive sensory processing assessment. Never begin a vestibular intervention programme without ruling out underlying vestibular pathology with a qualified medical professional.
CIN: U74999TG2016PTC113063 | DPIIT: DIPP8651 | MSME: TS20F0009606 | GSTIN: 36AAGCB9722P1Z2
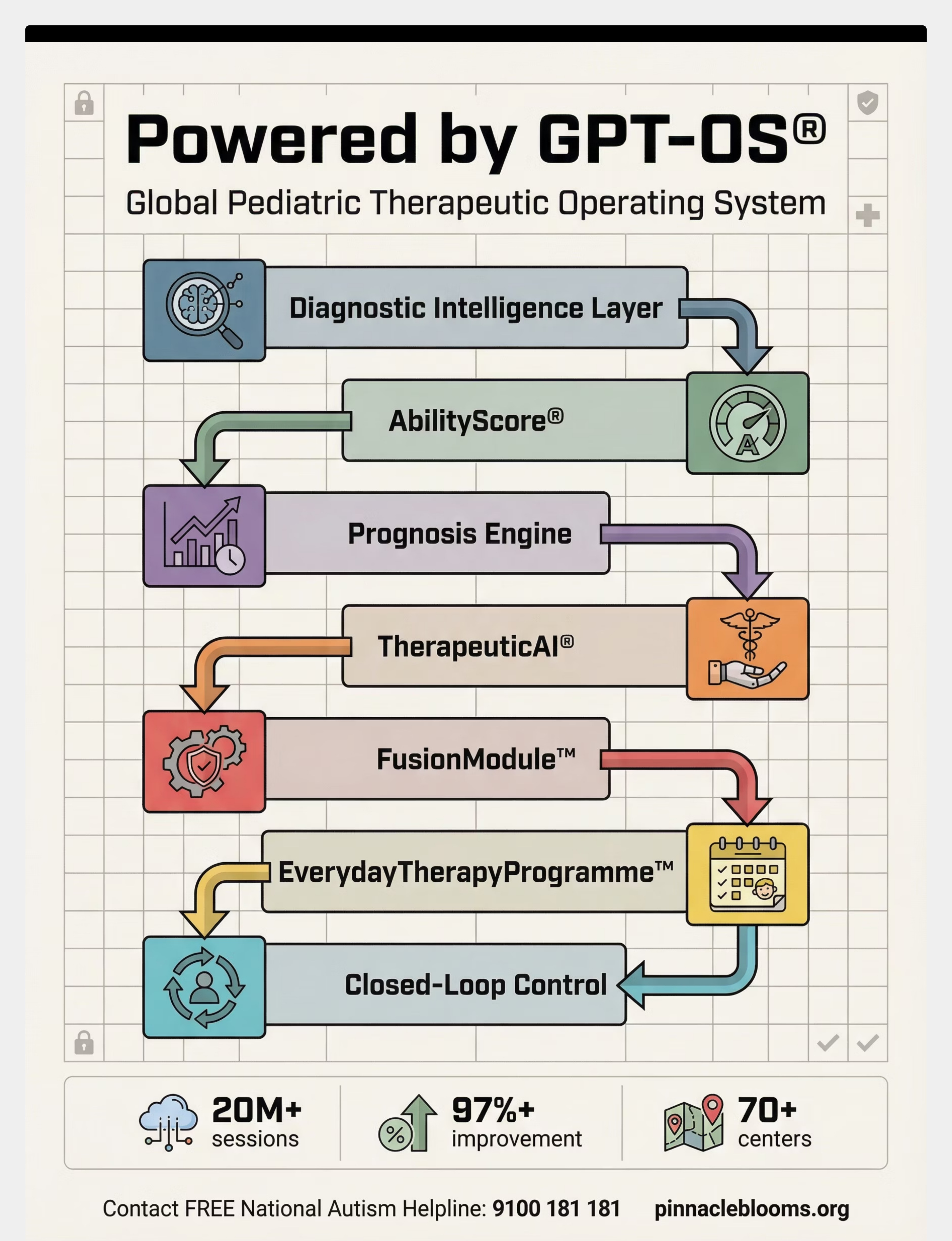
© 2026 Pinnacle Blooms Network®, unit of Bharath Healthcare Laboratories Pvt. Ltd. All rights reserved. GPT-OS®, AbilityScore®, TherapeuticAI®, FusionModule™, and EverydayTherapyProgramme™ are registered trademarks. Powered by GPT-OS® — Global Paediatric Therapeutic Operating System