'My child hasn't felt grass under her feet in 3 years.'
She screams if her feet even touch the grass. Beach trips are impossible. She sleeps in socks. You've tried bargaining, bribing, forcing — nothing works. Everyone says she's being dramatic.
She's not being dramatic. Her nervous system is speaking.
The soles of the feet contain approximately 200,000 nerve endings — among the highest concentrations in the entire body. For your child, surfaces that feel neutral to others can register as intensely uncomfortable, even painful. This is not stubbornness. This is a measurable neurological response called plantar tactile hypersensitivity.
There are 9 evidence-based materials that help. This page shows you exactly how to use them — at home, today.
You are not failing. Your child's nervous system is processing the world differently. And there is a path forward.
Pinnacle Blooms Consortium®
OT • SLP • ABA • SpEd • NeuroDev

You Are Among Millions.
You are not isolated. You are among millions of families navigating this exact challenge — from Mumbai to Melbourne, from Delhi to Dubai. Plantar tactile sensitivity is one of the most common and most actionable sensory challenges in pediatric therapy.
80%
Children with Autism
experience sensory processing difficulties including tactile hypersensitivity affecting the feet. Source: PRISMA Systematic Review, Children (2024) — PMC11506176
1 in 6
All Children
across all developmental profiles show some degree of tactile over-responsivity. Foot-specific sensitivity is among the most common manifestations. Source: Dunn, Sensory Profile 2 (2014)
78M+
Global Families
navigate autism-related sensory challenges daily. In India alone, that number exceeds 18.5 million families. Source: WHO Global Autism Prevalence Estimates (2023)
"When I found out 80% of children with autism have sensory processing differences, I stopped blaming myself." — Parent, Pinnacle Network

The Science Behind the Screams
Understanding what's happening in your child's nervous system is the first step toward compassionate, effective intervention.
What's Happening in the Foot
The plantar surface (sole) of the foot contains four types of sensory receptors that detect pressure, vibration, texture, and stretch:
Meissner Corpuscles
Light touch detection
Merkel Discs
Sustained pressure
Pacinian Corpuscles
Vibration sensing
Ruffini Endings
Stretch detection
Plain English Explanation
These receptors send signals to the somatosensory cortex — the brain region that interprets touch. In children with plantar tactile hypersensitivity, these receptors have lower thresholds for activation.
Think of it this way: your child's foot is receiving the same signal at 10x volume. Grass doesn't feel soft to them — it feels sharp. Sand doesn't feel warm — it feels like needles.
This is a wiring difference, not a behavior choice. Not a discipline problem. A neurological reality.
Reference: Frontiers in Integrative Neuroscience (2020) — DOI: 10.3389/fnint.2020.556660 | Ayres, A.J. — Sensory Integration and the Child (25th Anniversary Edition)
Your Child Is Here. Here Is Where We're Heading.
Per WHO Care for Child Development standards, barefoot walking provides crucial proprioceptive feedback for balance and gait development. The period from birth to age 5 is the most sensitive window for sensory integration.
12–18 Months
Typical barefoot walking begins
18–36 Months
Texture exploration typical window
2–4 Years
Outdoor barefoot play typical milestone
2–8 Years
🎯 Plantar Sensitivity Intervention Window — You Are Here
Why Barefoot Avoidance Matters Beyond Comfort
Motor Development
Barefoot walking provides essential proprioceptive feedback for balance, gait pattern, and foot muscle development.
Social Participation
Inability to go barefoot excludes your child from pools, beaches, gymnastics, martial arts, splash pads, and peer play.
Emotional Impact
Chronic avoidance of typical childhood experiences can affect self-esteem and increase anxiety over time.
Independence
Dependence on shoes and socks in all situations limits self-care development and autonomy.
The intervention window is NOW. Early, systematic desensitization has the highest success rates. Every week matters.
Reference: WHO Nurturing Care Framework (2018) | WHO/UNICEF CCD Package (2023) — PMC9978394
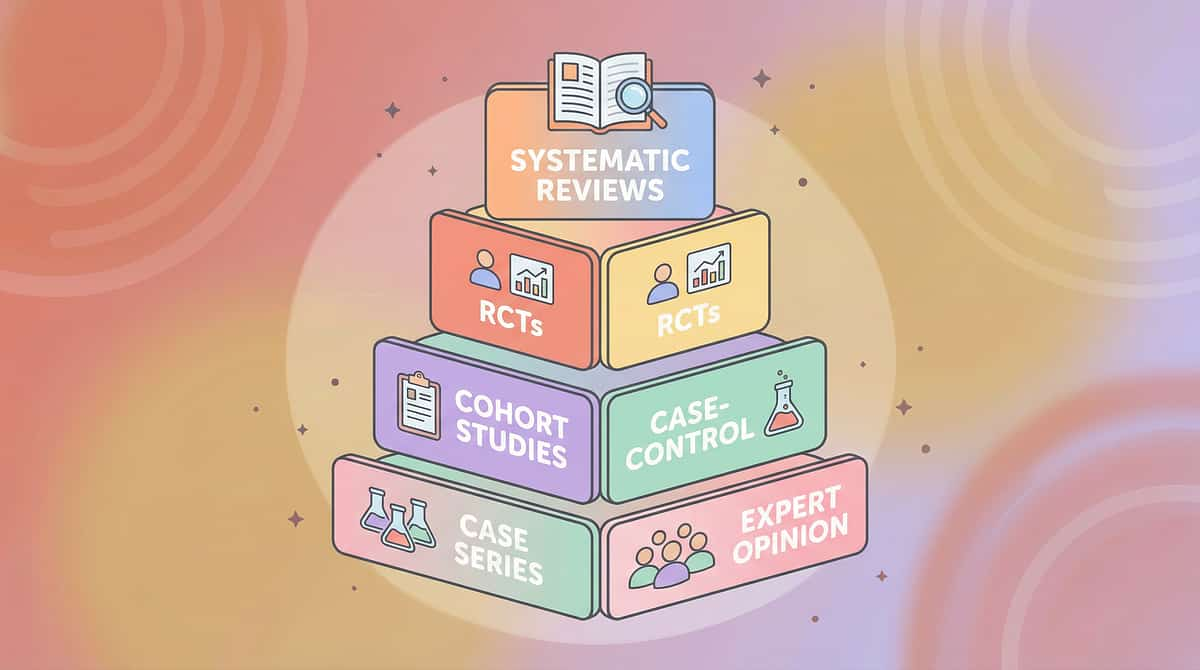
Clinically Validated. Home-Applicable. Parent-Proven.
Evidence Grade: LEVEL I–II
Systematic Review + RCT Supported
This protocol is not experimental. It is grounded in multiple peer-reviewed systematic reviews, meta-analyses, and controlled trials — and it is designed to be executed by parents at home, today.
PRISMA Systematic Review (2024)
16 articles from 2013–2023 confirm that sensory integration intervention meets criteria to be considered an evidence-based practice for children with ASD. Tactile desensitization protocols are a core component. PMC11506176
Meta-Analysis — World Journal of Clinical Cases (2024)
Across 24 studies, sensory integration therapy effectively promoted social skills, adaptive behavior, sensory processing, and gross/fine motor skills. Individual treatment sessions (1:1) were most effective. PMC10955541 | DOI: 10.12998/wjcc.v12.i7.1260
Indian RCT — Indian Journal of Pediatrics (2019)
Padmanabha et al. demonstrated significant outcomes in home-based sensory interventions for children with ASD in the Indian population. Parent-administered protocols showed measurable improvement. DOI: 10.1007/s12098-018-2747-4
NCAEP Evidence-Based Practices Report (2020)
Sensory integration is classified as an evidence-based practice by the National Clearinghouse on Autism Evidence and Practice at University of North Carolina, following decades of research review.
WHO Nurturing Care Framework (2018)
Context-specific, equity-focused interventions delivered through caregivers are the gold standard for early childhood development globally.
85%
Evidence Confidence
Strong evidence base with multiple systematic reviews, meta-analyses, and controlled trials supporting systematic tactile desensitization in pediatric populations.

Plantar Tactile Desensitization Through Graded Material Exposure
Parent-Friendly Name: "The Barefoot Journey"
A systematic desensitization protocol that uses 9 specific therapy materials to gradually rebuild your child's tolerance for foot-ground contact across progressively challenging textures. The approach begins with deep pressure preparation to regulate the nervous system, progresses through controlled texture exposure in safe contexts, and bridges to real-world barefoot participation.
The child maintains control throughout — they decide when to touch, how long, and when to stop.
Domain
Sensory Processing — Tactile (SEN-TAC)
Age Range
2–8 years
Session Duration
5–10 minutes daily
Protocol Duration
8–16 weeks (5 phases)
Setting
Home-executable
Difficulty
Introductory — parent-led, no clinical equipment required
Taxonomy: Pinnacle 128 Canon Materials System | 20 Category Classification | Domain A — Sensory

This Technique Crosses Therapy Boundaries
Because the brain doesn't organize by therapy type. Multiple disciplines converge on this single intervention — each contributing a distinct and essential lens.
Occupational Therapy — PRIMARY LEAD
OTs design and execute the sensory desensitization protocol. They assess the child's sensory profile, determine texture hierarchies, and calibrate the graded exposure plan. OTs specialize in sensory integration — the core mechanism behind this technique.
Speech-Language Pathology — SUPPORTING
SLPs address the communication aspect: helping the child express discomfort, request breaks, and communicate about sensory experiences. For non-verbal children, SLPs create AAC supports for sensory vocabulary.
Applied Behavior Analysis — SUPPORTING
BCBAs structure reinforcement schedules, data collection protocols, and the systematic desensitization hierarchy. ABA provides the behavioral framework — the "how fast" and "when to reinforce" decisions.
Special Education — SUPPORTING
Special educators adapt the protocol for classroom and school environments — transition support for shoe-removal activities, PE participation, and sensory-friendly accommodations.
Neuro-Developmental Pediatrics — CONSULTING
NeuroDev physicians rule out medical causes, provide differential diagnosis, and monitor for co-occurring conditions that may affect treatment response.
Reference: Adapted UNICEF/WHO Nurturing Care Framework for SLPs (2022) — DOI: 10.1080/17549507.2022.2141327

Precision Targets — This Is Not a Random Activity
Every material selected, every phase structured, and every session timed serves specific, measurable therapeutic goals across three levels of impact.
🎯 Primary Target: Plantar Tactile Tolerance
Increase the child's tolerance for diverse foot-ground textures from single-texture tolerance through multi-texture acceptance to functional barefoot participation. Observable Indicator: Child places bare feet on 5+ textures for 30+ seconds each without distress.
🎯 Secondary Targets
Sensory Regulation: Improved nervous system regulation through deep pressure and proprioceptive input. Anxiety Reduction: Decreased anticipatory anxiety. Motor Development: Improved balance and gait. Observable Indicator: Child voluntarily approaches new surfaces; reduced flight/fight responses.
🎯 Tertiary Targets
Social Participation: Beach trips, pool visits, gymnastics, outdoor play. Self-Care Independence: Reduced dependence on shoes/socks. Emotional Wellbeing: Increased confidence and reduced avoidance anxiety. Observable Indicator: Child participates in age-appropriate barefoot activities with minimal distress.
Reference: PMC10955541 — Meta-analysis confirming multi-domain outcomes from sensory integration therapy

Your Complete Barefoot Toolkit — 9 Materials, 3 Categories
Category 1: Deep Pressure Preparation
Regulate the nervous system first. These tools calm and organize before any texture challenge is introduced.

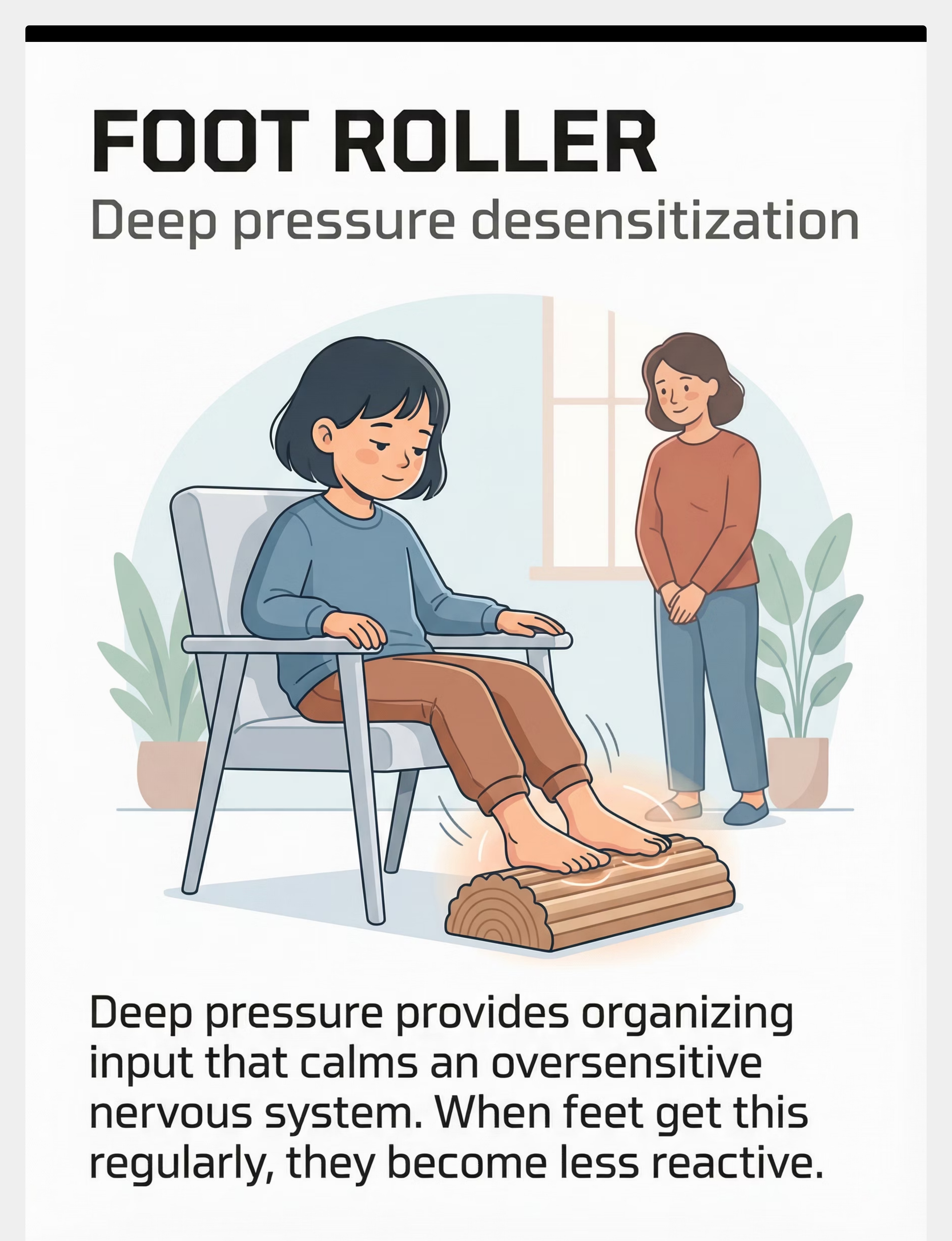
1. Foot Fidget Roller
Canon Category: Tactile Sensory Kit
Price: ₹300–800
Purpose: Deep pressure desensitization through firm rolling surface
Price: ₹300–800
Purpose: Deep pressure desensitization through firm rolling surface
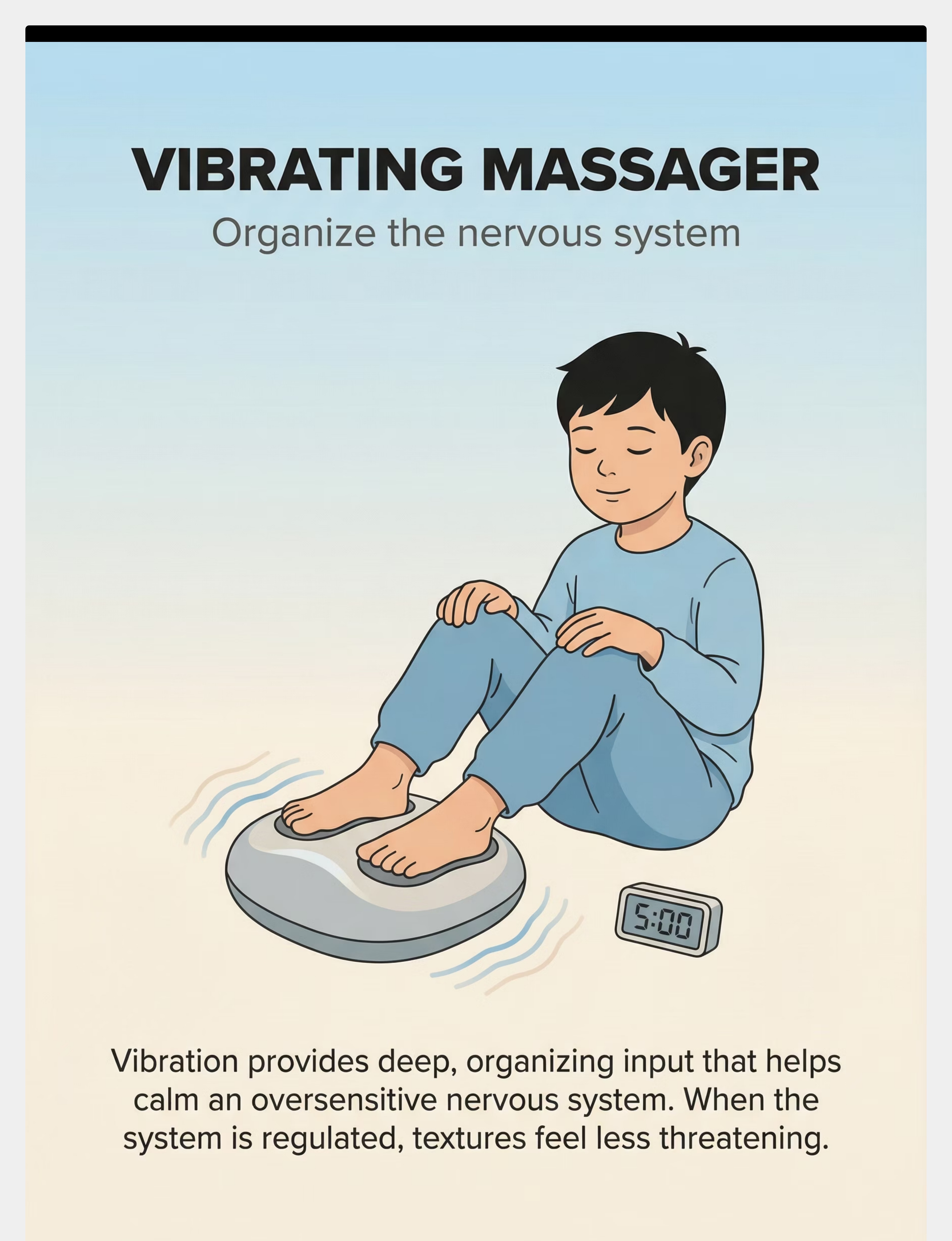
2. Vibrating Foot Massager
Canon Category: Vibrating Sensory Tools
Price: ₹500–1,500
Purpose: Nervous system organization through vibration input
Price: ₹500–1,500
Purpose: Nervous system organization through vibration input

3. Compression Foot Sleeves
Canon Category: Compression Garments
Price: ₹400–900
Purpose: Constant calming proprioceptive pressure
Price: ₹400–900
Purpose: Constant calming proprioceptive pressure
Category 2: Controlled Exposure
Introduce textures safely, in child-paced, controlled environments.
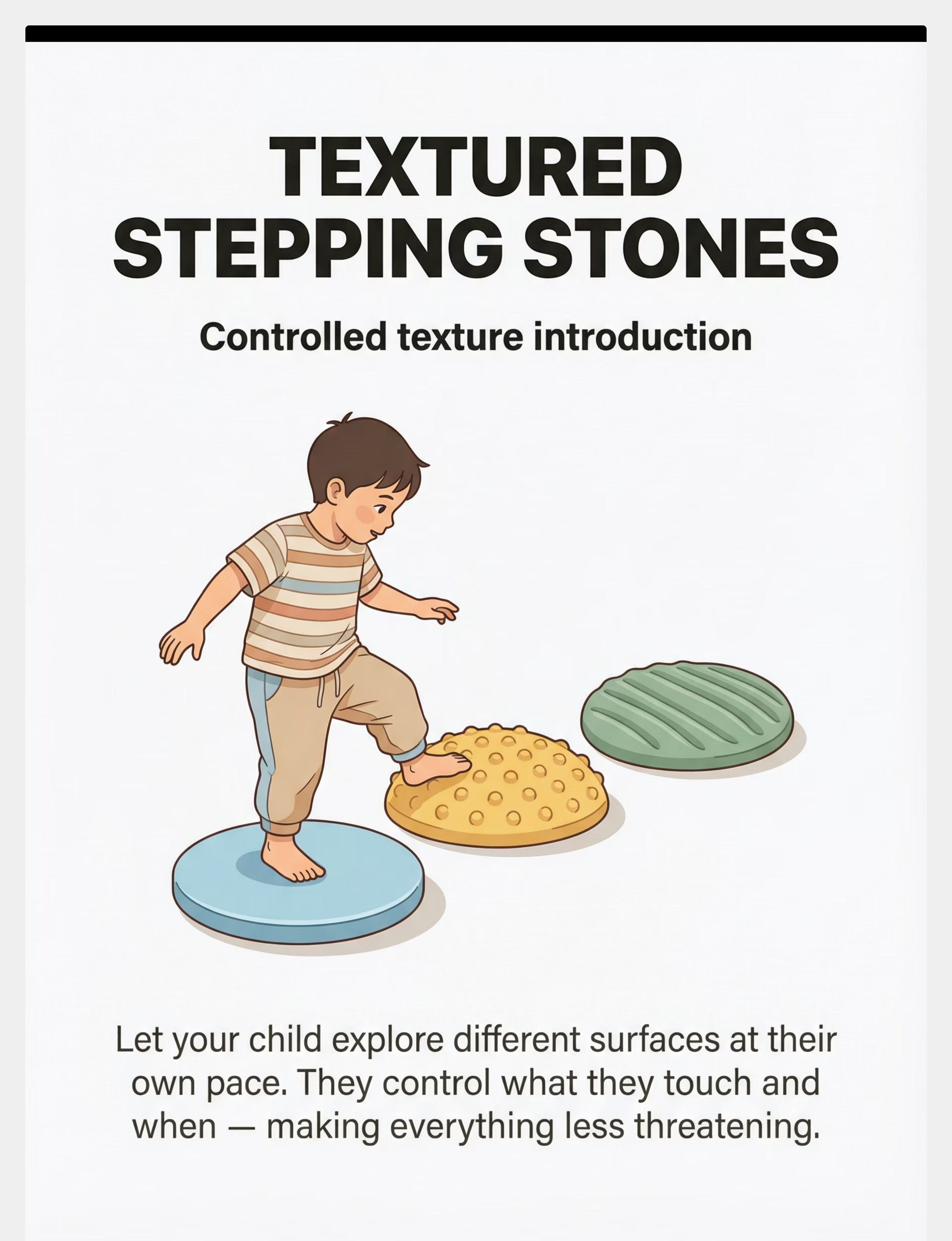
4. Textured Stepping Stones
Price: ₹800–2,000
Purpose: Controlled texture introduction in game format
Purpose: Controlled texture introduction in game format
5. Sensory Bin for Feet
Price: ₹200–600
Purpose: Child-paced texture exploration in a contained space
Purpose: Child-paced texture exploration in a contained space
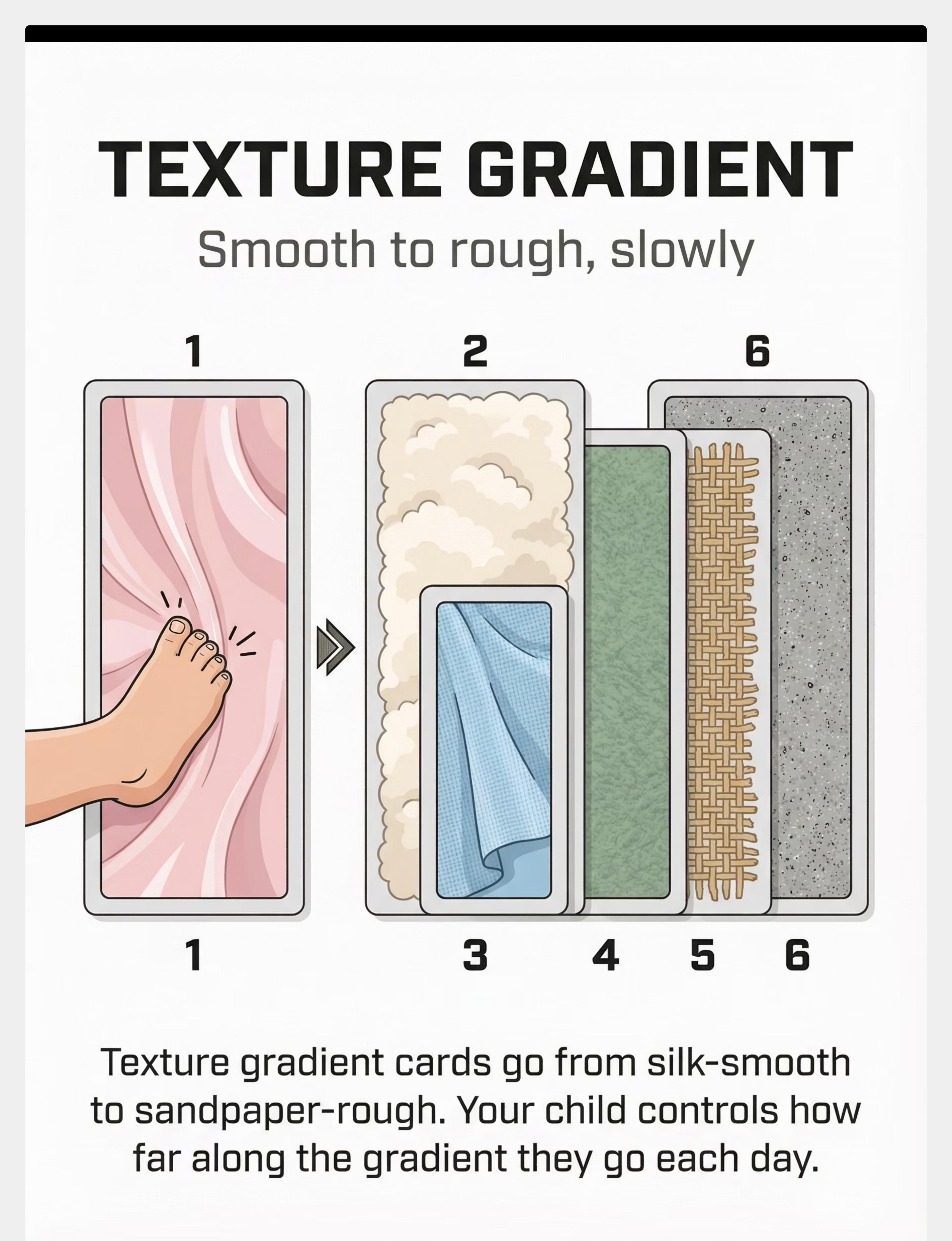
6. Texture Gradient Cards
Price: ₹300–700
Purpose: Systematic smooth→rough progression
Purpose: Systematic smooth→rough progression

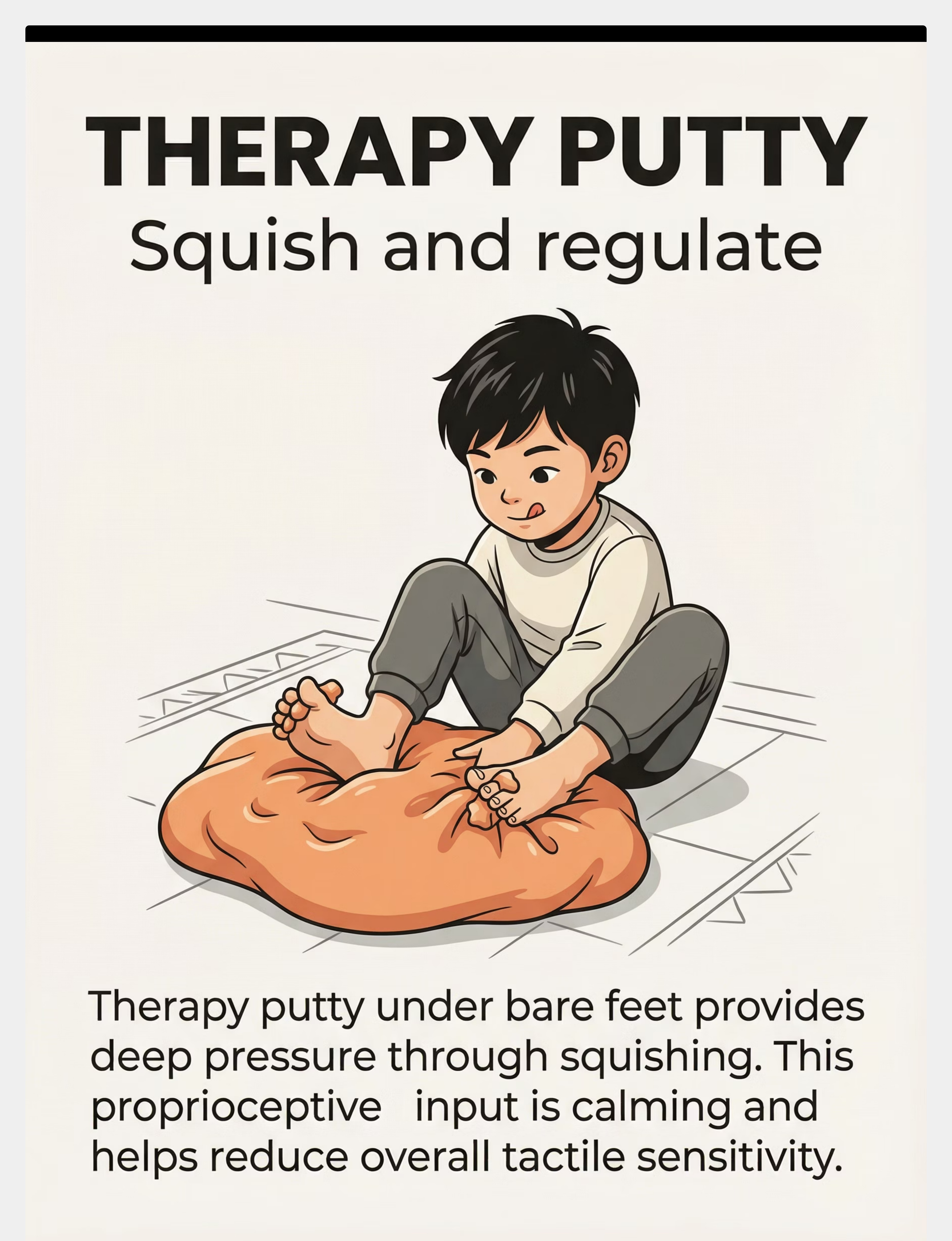
7. Therapy Putty for Feet
Price: ₹200–500
Purpose: Resistive proprioceptive input through feet
Purpose: Resistive proprioceptive input through feet
Category 3: Accommodation & Bridging

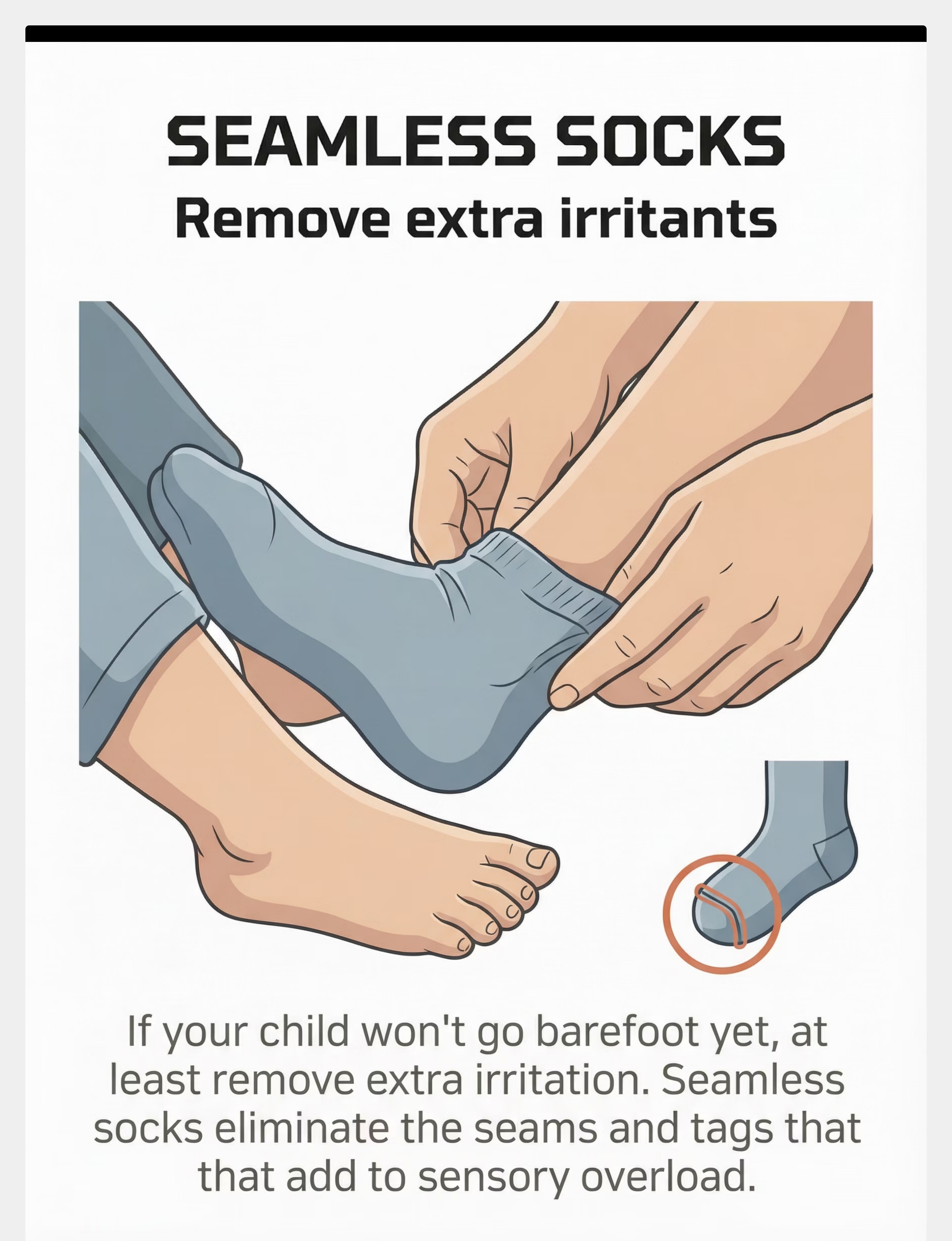
8. Seamless Socks
Price: ₹300–600/pair
Purpose: Remove extra irritants while building comfort
Purpose: Remove extra irritants while building comfort

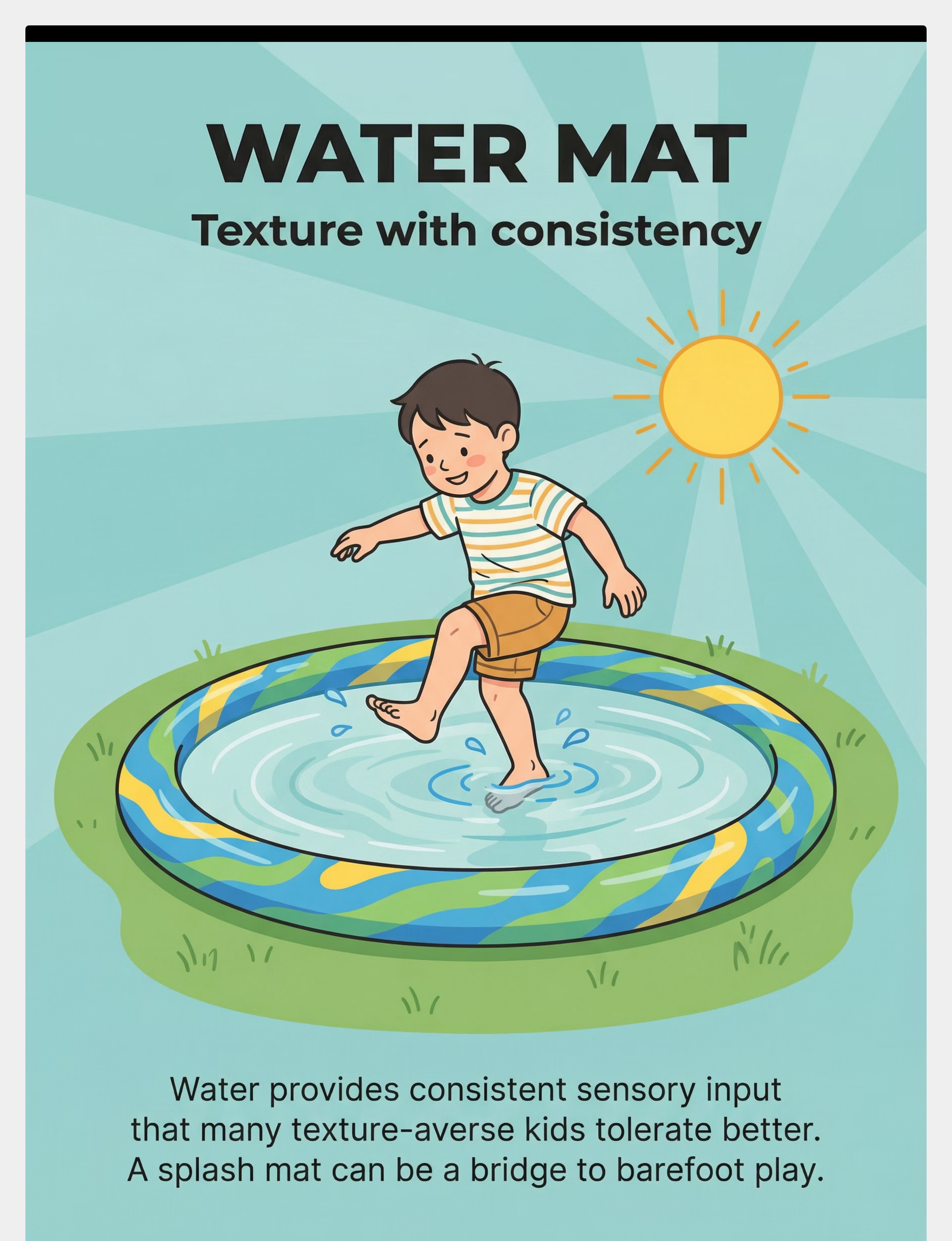
9. Water Play Mat / Splash Pad
Price: ₹500–2,000
Purpose: Bridge to real-world textures through enjoyable water play
Purpose: Bridge to real-world textures through enjoyable water play
Complete Toolkit Cost: ₹3,200–8,500 | Essential Starters (budget-limited): Foot Roller + Sensory Bin + Textured Stepping Stones = ₹1,300–3,400

No Amazon? No Problem. Start Today With What You Have.
Every family deserves access to these interventions — regardless of economic status or delivery logistics. The WHO Nurturing Care Framework emphasizes equity-focused, context-specific solutions. Here are household substitutes that work on the same sensory principles.
Buy This | Make This | Same Principle | |
Foot Roller (₹300–800) | Tennis ball or frozen water bottle rolled under feet | Deep pressure through firm rolling surface | |
Vibrating Massager (₹500–1,500) | Phone on vibrate under cushion; vibrating toothbrush on soles | Vibration organizes the nervous system | |
Compression Sleeves (₹400–900) | Tight-fitting athletic socks layered over regular socks | Compression provides proprioceptive calming | |
Textured Stepping Stones (₹800–2,000) | Cardboard squares covered in felt, fleece, faux fur, rubber shelf liner, smooth plastic | Controlled texture variety on manageable surfaces | |
Sensory Bin (₹200–600) | Large shallow storage bin with dried rice, dried beans, dried pasta, or kinetic sand | Contained texture exploration at child's pace | |
Texture Gradient Cards (₹300–700) | Mount on cardboard: silk → fleece → cotton → felt → burlap → sandpaper (6–10 levels) | Systematic progression from smooth to rough | |
Therapy Putty (₹200–500) | Firm homemade playdough (flour + salt); cloud dough (conditioner + cornstarch) | Resistive proprioceptive input through feet | |
Seamless Socks (₹300–600) | Turn regular socks inside out (seams on outside); thin smooth cotton socks | Eliminate seam irritation | |
Water Play Mat (₹500–2,000) | Shallow tub with warm water + smooth stones once comfortable | Consistent sensory input as texture bridge |
Zero-Cost Version: Tennis ball foot rolling + inside-out socks + rice in a baking tray + fabric scraps on cardboard = complete starter kit from household items.
Reference: WHO NCF Handbook (2022) | PMC9978394 — CCD Package efficacy with household materials across 54 LMICs

Read This Before Your First Session
Safety is non-negotiable. Take 60 seconds to review these guidelines before every session — they protect your child and protect the therapeutic relationship you're building.
🔴 DO NOT PROCEED IF:
Child has open wounds, skin infections, or foot injuries • Child is currently ill, feverish, or recovering • Child is already severely dysregulated (active meltdown, exhaustion, hunger) • Medical concern about peripheral neuropathy — consult NeuroDev first • Known skin allergies to therapy putty ingredients — test on hand first
🟡 MODIFY THE APPROACH IF:
Child has had a difficult day — use ONLY deep pressure materials, skip texture exposure • Child shows anticipatory anxiety — reduce to 2–3 minutes, use only preferred textures • Previous session triggered distress — return to previous phase, do not push forward
🟢 PROCEED WITH CONFIDENCE WHEN:
Child is fed, rested, and in a calm-alert state • Environment is quiet, familiar, and free of additional sensory triggers • All materials are prepared and within reach • You (the parent) are calm and unhurried — your regulation co-regulates your child • Child shows willingness or at least neutral affect
⛔ ABSOLUTE RED LINES — STOP IMMEDIATELY IF:
- Child shows signs of extreme distress: prolonged crying (>2 minutes), self-injury, gagging, or panic
- Child reports sharp pain (not just discomfort)
- You observe skin irritation, redness, or swelling on feet
- Child becomes non-responsive or dissociative
CONTRAINDICATIONS — NEVER:
- Force barefoot exposure through a meltdown
- Use barefoot walking as punishment
- Surprise the child with texture exposure
- Dismiss reports of pain as "drama"
- Remove shoes/socks without the child's knowledge and consent
Reference: DOI: 10.1007/s12098-018-2747-4 — Home-based sensory intervention safety protocols
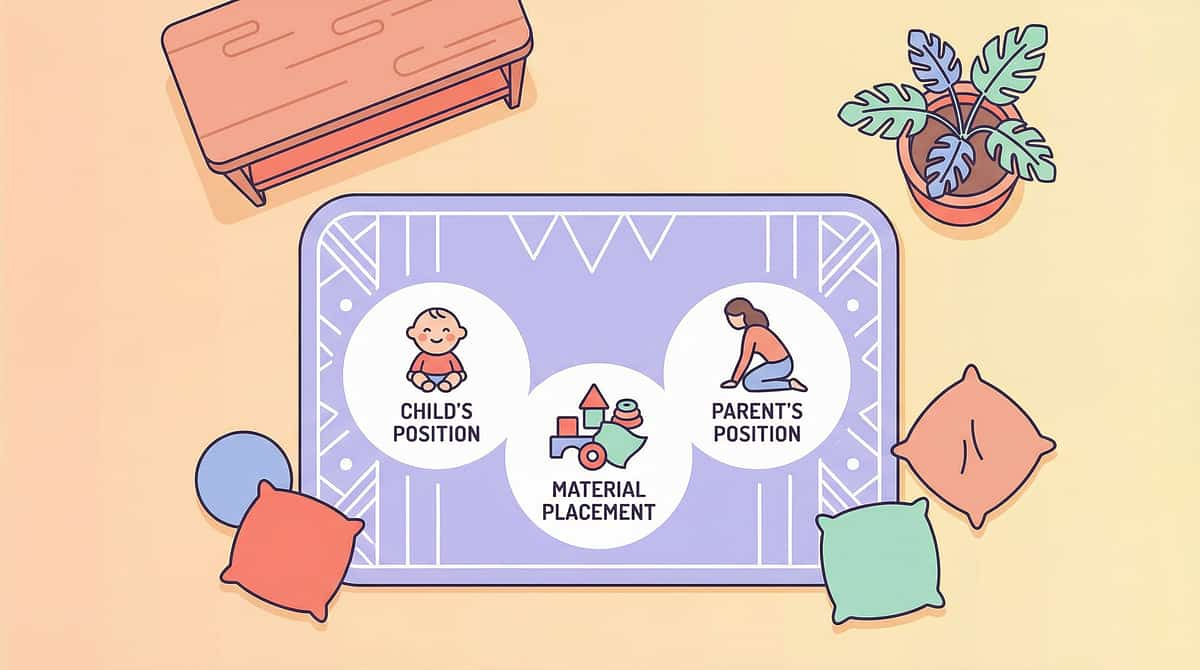
The Perfect Session Starts With the Right Setup
How you arrange the physical space shapes the child's sense of safety before a single material is introduced. Follow this layout every time — consistency reduces anticipatory anxiety.
What to REMOVE from the space
- Screens and electronic distractions
- Siblings (unless a calming presence)
- Competing sensory input: TV, loud music, strong smells
- Clutter around the foot area
- Materials not being used today
Environment Checklist
- Lighting: Natural or warm — avoid harsh fluorescents
- Temperature: Warm (cold feet increase sensitivity)
- Floor: Clean, smooth surface as the starting base
- Sound: Quiet or child's preferred calming music at low volume
- Exit: Child must always feel they can leave — non-negotiable
Your energy matters — calm, unhurried, present. The child reads your affect before they read the room.
Reference: PMC10955541 — Meta-analysis on structured environment efficacy for sensory integration sessions

The 60-Second Pre-Flight Check
Before every session, run through this checklist. It takes 60 seconds and prevents 80% of session failures. This is not optional — it is the protocol.
1
Has your child eaten within the last 2 hours?
Hunger = dysregulation. A hungry nervous system cannot process new sensory input safely.
2
Has your child had adequate sleep?
Fatigue = lower tolerance. Sleep-deprived children have measurably reduced sensory thresholds.
3
Has your child been meltdown-free for at least 30 minutes?
Post-meltdown = depleted system. The nervous system needs recovery time before new challenges.
4
Is the environment set up per Card 12?
Space ready = session ready. Consistent setup reduces anticipatory anxiety before you begin.
5
Are YOU calm and unhurried?
Your state co-regulates theirs. If you're rushed or anxious, the child will feel it.
6
Does the child know what's coming?
No surprises — predictability equals safety for a sensitized nervous system.
7
Is the safe retreat visible and accessible?
Escape option = reduced anxiety. Paradoxically, when children know they can leave, they're more likely to stay.
All Green → GO
Begin with Step 1: The Invitation
1–2 Amber → MODIFY
Use only Phase 1 deep pressure materials. Shorter session (3 minutes).
Any Red → POSTPONE
Do a calming activity instead. Tomorrow is fine. Consistency over intensity.
"The best session is one that starts right. A forced session teaches the wrong lesson."

Step 1 — The Invitation (Not a Command)
Protocol Step 1 of 6
Timing: 30–60 seconds
What to Say (Script)
"Hey [child's name], I have something fun for your feet today. Want to see? You don't have to do anything you don't want to. You're the boss of your feet."
Body Language
- Sit at child's level
- Keep voice low and calm
- Present the material in YOUR hands first — show it's safe
- Smile. Your face tells them everything is okay.
What Acceptance Looks Like
- Child looks at the material
- Child reaches toward it
- Child leans forward or says "okay"
- Child doesn't actively pull away
What Resistance Looks Like
- Child turns away or covers eyes
- Child pulls feet up under body
- Child says "no" verbally or with body language
- Child's face shows distress or anxiety
IF RESISTANCE: That's fine. Place the material near them (not on them). Say: "It's just here if you want it. No rush." Move to a preferred activity and try again tomorrow. Resistance is data, not failure.

Step 2 — The Engagement (Follow the Child's Lead)
Protocol Step 2 of 6
Timing: 1–3 minutes
The child has accepted the invitation. Now introduce the material gradually — always following the child's pace, never your timeline.
1
Phase 1 — Deep Pressure Tools (Weeks 1–2)
Present the foot roller, vibrating massager, or compression sleeves. Place near the child's feet but don't apply. Let them explore by touching with hands first if they prefer. Proximity without demand builds tolerance.
2
Phase 2+ — Texture Tools (Weeks 3+)
Present the sensory bin, stepping stones, or gradient cards. Demonstrate with YOUR feet first — show them it's safe, it doesn't hurt you. Then place near their feet. Your modeling is therapeutic.
Reinforcement Cue
The moment the child shows ANY approach behavior — looking, reaching, touching — immediately reinforce: "Look at you! You're checking it out! That's so brave."
Engagement (Ideal)
Child voluntarily touches or steps toward material → Continue to Step 3
Tolerance (Acceptable)
Child allows material near feet but doesn't engage → Stay here, don't push forward
Avoidance (Concerning)
Child actively withdraws → Return to invitation, try simpler or more familiar material
Reference: PMC11506176 — Structured material introduction in sensory integration

Step 3 — The Therapeutic Action (Where Change Happens)
Protocol Step 3 of 6
Timing: 3–5 minutes
This is the core therapeutic window — where neural pathways are built, session by session. The action varies by phase. Match today's action to your child's current phase.
Phase 1 (Weeks 1–2): Deep Pressure Foundation
Child's feet contact the foot roller, vibrating massager, or compression sleeves. Apply firm, even pressure — NOT light touch (light touch is more alerting than deep pressure). Roll the foot roller slowly. Start with 30-second intervals. "Feel that? That's deep pressure. It tells your feet 'you're safe.'"
Phase 2 (Weeks 3–5): Controlled Texture Exposure
Child places bare feet (or one foot, or just toes) into the sensory bin. Begin with the most tolerated texture (smooth rice, beans). The child controls depth, duration, and can withdraw instantly. "Your feet are exploring! How does the rice feel? You can take them out any time."
Phase 3 (Weeks 6–9): Texture Gradient Expansion
Child moves along the texture gradient cards — from silk to fleece to cotton to felt to burlap. They choose how far to go each day. Textured stepping stones become a game — "island hopping" between preferred textures.
Phase 4 (Weeks 10–12): Real-World Bridging
Water play mat → stepping stones on grass → brief standing on grass with retreat option → patio surfaces. Each real-world introduction is paired with a familiar comfort material.
Phase 5 (Weeks 13–16+): Functional Participation
Walking on grass, beach visits, pool area barefoot, barefoot play with peers. This is the goal — spontaneous, joyful participation without anticipatory anxiety.
Common Execution Errors
- Going too fast (most common mistake — trust the phase timeline)
- Using light touch instead of deep pressure in Phase 1
- Removing the child's escape option
- Conducting sessions during a dysregulated state
Reference: PMC10955541 — Therapy session effectiveness data

Step 4 — Repeat & Vary (3 Good Reps > 10 Forced Reps)
Protocol Step 4 of 6
Timing: 3–5 minutes total
Target Repetitions
3–5 per session (not 10, not 20)
Why Less Is More
Three successful, voluntary exposures build more neural pathways than ten forced ones. The nervous system learns from positive experiences, not endured ones. Quality of contact beats quantity of contact. Every time.
Variation Options Within a Single Session
- Different feet: left foot, then right foot, then both
- Different materials: roller first, then bin, then stepping stones
- Different positions: seated, standing, walking
- Different temperatures: warm rice, cool beans, room-temperature putty
Satiation Indicators — The Child Has Had Enough
Loss of interest or engagement — eyes wandering, body turning away
Fidgeting or looking away from the activity
Increased foot withdrawal speed compared to earlier in session
Verbal or nonverbal "all done" signals
Any sign of distress — facial grimacing, body tension, vocalizations
WHEN THE CHILD HAS HAD ENOUGH → STOP. Celebrate what was achieved. Never push for "one more." Ending on a positive note builds positive anticipation for next time.
"3 good reps > 10 forced reps. Quality of contact beats quantity of contact. Every time."

Step 5 — Reinforce & Celebrate (Within 3 Seconds)
Protocol Step 5 of 6
The 3-Second Rule
THE RULE: Reinforcement must arrive within 3 seconds of the desired behavior. Timing matters more than magnitude. A delayed reward loses most of its therapeutic power.
Reinforcement Script — What to Say
"Your feet are so brave today! Look at what you did!" — For ANY foot contact with material
"You stayed on the stepping stone for even longer! Your feet are learning!" — For increased duration
"You tried something NEW with your feet! That takes real courage!" — For trying a new texture
"We did our whole foot practice and you were the boss the entire time! I'm so proud." — For completing without distress
Reinforcement Menu — Choose What Motivates YOUR Child
Verbal Praise
Immediate, specific, enthusiastic
Preferred Activity
Immediately after session ends
Token / Sticker
Toward a visual reward chart
Physical Celebration
High-five, dance, celebration song
Social Sharing
"Tell Daddy/Nani what your feet did today!"
THE GOLDEN PRINCIPLE: Celebrate the ATTEMPT, not just the success. A child who touches grass for 1 second and then withdraws has made extraordinary progress. Honor that moment exactly as it deserves.

Step 6 — The Cool-Down (Never End Abruptly)
Protocol Step 6 of 6
Timing: 1–2 minutes
How a session ends is as important as how it begins. An abrupt ending can undo the positive associations built during the session. Always transition with intention and predictability.
Transition Warning (30 seconds before ending)
"Two more touches, then we're all done with foot practice." or "One more, and then feet get a rest." Predictability is safety.
Cool-Down Activities
Gentle foot massage with firm (not light) pressure for 60 seconds • Compression sleeves on for 1–2 minutes post-session • Child puts preferred socks/shoes back on (their choice) • Preferred calming activity: favorite song, comfort object, quiet play
Material Put-Away Ritual
Let the child participate if willing. "Can you help put the stepping stones in the box?" This creates a clear "session over" signal and gives the child agency over the end of the experience.
Transition to Next Activity
"Foot practice is all done! What shall we do next?" Immediate transition to a preferred activity reinforces the entire session positively in memory.
IF THE CHILD RESISTS ENDING (wants to continue): This is wonderful. It means they're enjoying it. Allow 1–2 more minutes, then repeat the transition sequence. Ending while the child WANTS more is ideal — it creates positive anticipation for next time.
Reference: NCAEP Evidence-Based Practices Report (2020) — Visual supports and transition strategies

60 Seconds of Data Now Saves Hours of Guessing Later
Record immediately after session — within 60 seconds. Data captured while fresh is accurate. Data recalled hours later is approximate. These three data points are all you need to track meaningful progress.
1
Duration
How long did your child's feet stay in contact with the material? Record in seconds. Even 5 seconds matters — document it.
2
Textures Tolerated
How many different textures did your child voluntarily contact today? Record as a number. Track variety, not just duration.
3
Distress Level
1 = Calm/happy → 2 = Neutral/cautious → 3 = Mildly uncomfortable → 4 = Distressed → 5 = Refused/meltdown
Optional Additional Notes
- Which specific materials were used
- Any new textures attempted for the first time
- Spontaneous approach behaviors observed
- Anything unusual or noteworthy about the session
📋 Downloadable PDF Tracker
pinnacleblooms.org/trackers/A-012 — Simplified single-page session log
📱 GPT-OS® In-App Tracker
In-app session logger — auto-populates your child's progress profile and generates adaptive recommendations
"Your data doesn't just track your child's progress. It feeds GPT-OS® to improve recommendations for every child like yours."
Reference: BACB data collection standards | Cooper, Heron & Heward — Applied Behavior Analysis

Most Sessions Don't Go Perfectly. That's Normal.
Troubleshooting is not a sign of failure — it is a sign of an engaged, observant parent. Every challenge below has a solution. Read through the ones that match your experience.
Problem 1: "My child refused to even look at the materials."
This is common in Week 1. Place materials in the room during preferred activities. Let them exist without demand. Try again tomorrow with zero pressure. Proximity without demand builds tolerance.
Problem 2: "My child screamed the moment I mentioned feet."
Drop the word "feet." Just have the materials available during play. Roll the foot roller with your hands first. Let curiosity drive the first approach. Anticipatory anxiety decreases with predictability and zero pressure.
Problem 3: "She tolerated it for 2 seconds and then pulled away."
Two seconds IS progress. Celebrate it. Two seconds today → five seconds next week → ten seconds the week after. Neural pathways build in increments, not leaps.
Problem 4: "We were making progress and now he's refusing again."
Regression is normal and expected. Common triggers: illness, life changes, schedule disruption, growth spurts. Return to the previous phase temporarily. The pathways don't disappear — they're just paused.
Problem 5: "Nothing has changed after 3 weeks."
Check: Are sessions happening daily? Is the child in control? Did you complete Phase 1 before moving to textures? Is the child regulated during sessions? If yes to all, a plateau beyond 8–10 weeks warrants professional OT consultation.
Problem 6: "The child became severely distressed."
Stop immediately. Comfort first — no discussion about the materials. Return to preferred calming activity. Wait 24–48 hours before attempting again. If severe distress occurs repeatedly, consult a qualified OT.
"Session abandonment is not failure — it's data."
No Two Children Are Identical. Here's How to Make This Yours.
The protocol provides the structure. You provide the personalization. Use this guide to calibrate the difficulty level based on your child's state, history, and response patterns on any given day.
1
◄ EASIER VERSION
For: Bad days, regression periods, very young children
• Phase 1 tools only (roller, compression, vibration)
• Socks ON — don't require bare feet
• Seated only — no standing or walking
• 2-minute sessions maximum
• Preferred music playing throughout
• Comfort object within reach
• Phase 1 tools only (roller, compression, vibration)
• Socks ON — don't require bare feet
• Seated only — no standing or walking
• 2-minute sessions maximum
• Preferred music playing throughout
• Comfort object within reach
2
STANDARD VERSION
For: Progressing children in a regulated state
• Phase-appropriate materials per protocol
• One bare foot, one sock foot
• Mix of seated and brief standing
• 5–7 minute sessions
• Calm, familiar environment
• Phase-appropriate materials per protocol
• One bare foot, one sock foot
• Mix of seated and brief standing
• 5–7 minute sessions
• Calm, familiar environment
3
HARDER VERSION ►
For: Breakthrough days, children seeking input
• Multiple textures in single session
• Both feet bare
• Standing → walking → hopping
• 10-minute sessions
• Introduce novel textures
• Outdoor surfaces: patio, deck
• Multiple textures in single session
• Both feet bare
• Standing → walking → hopping
• 10-minute sessions
• Introduce novel textures
• Outdoor surfaces: patio, deck
Alternative Pathways (If Standard Approach Isn't Progressing)
Water-First Pathway
Begin all texture exposure underwater. Smooth stones underwater → textured bath mat underwater → sand underwater → wet grass → dry grass. Water reduces sensory defensiveness.
Sock Gradient Pathway
Thick socks → medium socks → thin socks → one sock off → toe sock → bare feet. Intermediate steps for children who can't tolerate any barefoot exposure yet.
Proprioceptive Loading First
Heavy work before exposure: jumping → pushing heavy objects with feet → immediate texture exposure while proprioceptive system is activated and organized.
Functional Context Motivation
Swimming, martial arts, trampoline — activity motivation may enable tolerance that transfers to other barefoot contexts. Follow the child's intrinsic motivation.
Sensory Seeker vs. Avoider: Seekers may tolerate rough textures but avoid specific ones — map their specific hierarchy. Avoiders need slower progression and more deep pressure preparation before any texture introduction.
Weeks 1–2: Foundation Phase — Regulate the System
Progress: ~15%
Deep Pressure Foundation
What You're Doing in Weeks 1–2
Daily deep pressure and proprioceptive input to feet — foot roller, vibrating massager, compression sleeves. NO texture challenge yet. You are preparing the nervous system. A house without a foundation collapses — these two weeks are the foundation.
✅ IS Progress
Child tolerates foot roller for 30+ seconds (up from 0) • Child allows compression sleeves during calm activities • Child may begin to seek out the foot roller • Reduced foot-withdrawal reflex during deep pressure
❌ Is NOT Progress Yet
Child walking barefoot on grass (that's Phase 5) • Child enjoying all textures (weeks away) • Zero distress (mild discomfort is normal; distress is not)
"If your child tolerates the foot roller for 3 seconds longer than last week — that's real, measurable progress."
Success Criterion: Child tolerates and may seek out foot pressure input.
Weeks 3–4: Controlled Exposure — Safe Contexts
Progress: ~40%
Consolidation Phase
You're introducing the sensory bin, therapy putty, and seamless socks. Feet enter contained texture environments — rice bins, putty squishing — where the child maintains complete control over depth, duration, and withdrawal.
Consolidation Indicators
- Child willingly puts bare feet in the sensory bin for 1–2 minutes
- Child shows curiosity rather than avoidance toward texture materials
- Reduced anticipatory anxiety — child doesn't tense when session is announced
- Child may spontaneously explore textures during free play
- Therapy putty squishing becomes a preferred activity
Behavioral Changes Signaling Neural Pathway Formation
- Child says "my feet" or points to materials (awareness developing)
- Child chooses which material to start with (agency emerging)
- Session initiation becomes smoother (habituation occurring)
- Post-session mood is neutral or positive (positive association forming)
When to Increase: If child consistently completes Phase 2 without distress for 5+ consecutive sessions, introduce Phase 3 materials. Don't rush — consistent tolerance at Phase 2 predicts success at Phase 3.
"You may notice you're more confident too. That's not incidental — your confidence IS part of the therapy."
Success Criterion: Child willingly puts bare feet in sensory bin for 1–2 minutes without distress.
Weeks 5–8: Texture Gradient Expansion
Progress: ~75%
Mastery Approaching
Texture gradient cards are progressing from smooth to rough. Stepping stones with gradually increasing variety. Mixed texture bins. Your child is actively expanding their tolerance map — and may be doing so voluntarily and with enjoyment.
01
Mastery Criteria
Child tolerates 5+ different textures for 30+ seconds each • Child voluntarily tries new textures (approach behavior) • Child can articulate or indicate preferences • Texture exploration has become a game, not a therapy session • Stepping stone "island hopping" is fun, not stressful
02
Generalization Signs
Child notices textures in daily life ("this floor feels different") • Reduced need for specific socks/shoes in some environments • Willingness to explore new surfaces briefly • Less anticipatory anxiety about foot-related activities
03
Maintenance Check
Does progress persist on days without formal sessions? Generalization beyond structured sessions is the clearest sign that neural pathways are forming and consolidating.
🏆 MASTERY UNLOCKED when: Child tolerates 5+ textures for 30+ seconds each without distress, approaches novel textures voluntarily, and progress persists without daily protocol. This is a genuine neurological achievement.

You Did This. Your Child Grew Because of Your Commitment.
Remember Card 01? "My child hasn't felt grass under her feet in 3 years."
Look where you are now. Your child's feet have touched textures they've never tolerated before. Every 5-minute session, every data point captured, every day you chose consistency over frustration — it built to this moment.
What Your Child Has Achieved
- A nervous system that can process foot-ground contact with reduced defensive response
- The beginnings of texture tolerance that will expand for years
- Increased confidence and reduced anxiety around barefoot situations
- A toolkit of coping materials they know and trust
What You Have Achieved
- Competence in sensory desensitization protocol execution
- Data-driven therapy skills applicable to future challenges
- Deeper understanding of your child's neurological needs
- Proof that home-based intervention works
Family Celebration Suggestion: Document this milestone. Take a photo of your child's feet touching a texture that was impossible 8 weeks ago. Write the date on it. This is a milestone as significant as any first step.
Trust Your Instincts — If Something Feels Wrong, Pause and Ask
Progress should feel gradual and positive. These red flags signal that the home-based protocol has reached its limits and professional support is needed — not as a failure, but as the next appropriate step.
🚩 Red Flag 1
Extreme distress at ANY foot touch, including during bathing — may indicate broader sensory or medical issue.
→ Consult OT + NeuroDev.
→ Consult OT + NeuroDev.
🚩 Red Flag 2
Self-injury to avoid barefoot exposure (biting, hitting self, head-banging during sessions).
→ Stop protocol immediately. Consult BCBA + OT.
→ Stop protocol immediately. Consult BCBA + OT.
🚩 Red Flag 3
Complete avoidance of ALL floor contact — always needing to be carried or seated.
→ This exceeds plantar sensitivity — comprehensive sensory assessment needed.
→ This exceeds plantar sensitivity — comprehensive sensory assessment needed.
🚩 Red Flag 4
No progress after 8–10 weeks of consistent, child-led approach.
→ Professional OT assessment recommended. Plateau may indicate underlying factors.
→ Professional OT assessment recommended. Plateau may indicate underlying factors.
🚩 Red Flag 5
Barefoot avoidance as part of broader tactile defensiveness affecting multiple body areas (hands, face, trunk).
→ Comprehensive sensory profile assessment needed.
→ Comprehensive sensory profile assessment needed.
🚩 Red Flag 6
New onset of toe-walking or gait changes.
→ Orthopedic and neurological screening warranted.
→ Orthopedic and neurological screening warranted.
Escalation Pathway
Where You Were. Where You Are. Where You're Going.
Technique A-012 sits within a structured progression. Knowing what came before and what comes next helps you see the larger therapeutic journey your child is on.
← Prerequisite
- A-011: Nail Cutting Resistance
- General tactile defensiveness awareness
⬤ You Are Here
A-012: Barefoot Refusal — Plantar Tactile Desensitization
Position: 12 of 30 in Texture & Surface Tolerance Series
Position: 12 of 30 in Texture & Surface Tolerance Series
→ Next-Level Options
- Path A: A-014 Sand Play Avoidance
- Path A: A-016 Grass Avoidance
- Path B: A-013 Clothing Tag Sensitivity
- Path C: A-020 General Tactile Defensiveness
More Techniques in Tactile Processing — Materials You Already Own
The 9 materials in your barefoot toolkit unlock multiple techniques across the tactile processing domain. You've already invested — now extend that investment.
A-010: Hair Brushing Meltdowns
Difficulty: Introductory
Your Materials: Foot Roller ✓, Compression ✓
Domain: Sensory → Tactile (Head/Scalp)
Your Materials: Foot Roller ✓, Compression ✓
Domain: Sensory → Tactile (Head/Scalp)
A-011: Nail Cutting Resistance
Difficulty: Introductory
Your Materials: Vibrating Massager ✓
Domain: Sensory → Tactile (Hands/Feet)
Your Materials: Vibrating Massager ✓
Domain: Sensory → Tactile (Hands/Feet)
A-013: Clothing Tag Sensitivity
Difficulty: Introductory
Your Materials: Seamless Socks ✓, Compression ✓
Domain: Sensory → Tactile (Body)
Your Materials: Seamless Socks ✓, Compression ✓
Domain: Sensory → Tactile (Body)
A-014: Sand Play Avoidance
Difficulty: Core
Your Materials: Sensory Bin ✓, Stepping Stones ✓
Domain: Sensory → Tactile (Hands/Feet)
Your Materials: Sensory Bin ✓, Stepping Stones ✓
Domain: Sensory → Tactile (Hands/Feet)
A-015: Messy Play Refusal
Difficulty: Core
Your Materials: Sensory Bin ✓, Therapy Putty ✓
Domain: Sensory → Tactile (Hands)
Your Materials: Sensory Bin ✓, Therapy Putty ✓
Domain: Sensory → Tactile (Hands)
A-016: Grass Avoidance
Difficulty: Core
Your Materials: Stepping Stones ✓, Water Mat ✓
Domain: Sensory → Tactile (Outdoor)
Your Materials: Stepping Stones ✓, Water Mat ✓
Domain: Sensory → Tactile (Outdoor)
✓ = You already own materials for this technique. Your toolkit unlocks the entire tactile domain.
This Technique Is One Piece of a Larger Plan
The nervous system doesn't work in silos — and neither does this protocol. Barefoot tolerance connects to motor development, communication, behavior, and social participation in measurable, documented ways.
Domain A: Sensory Processing
← YOU ARE HERE — Primary domain
Domain B: Motor Development
Connected — barefoot walking feeds gross motor development and balance
Domain D: Behavioral Regulation
Connected — meltdown reduction through systematic desensitization
Domain E: Social Participation
Connected — barefoot play activities with peers become accessible
Domain H: Emotional Regulation
Connected — reduced sensory anxiety and increased confidence
Domain J: Play Skills
Connected — outdoor barefoot play and full recreational participation
GPT-OS® tracks your child across all 12 domains simultaneously. Every data point you enter feeds a comprehensive developmental profile that personalizes recommendations across the entire spectrum.
From Where You Are to Where They Are Now
These families were exactly where you are today. Their outcomes are not exceptional — they are what this protocol produces when applied consistently and with child-led compassion.
Family Story 1 — 16-Week Journey
Before: "Our son hadn't walked barefoot anywhere in 4 years. Beach holidays were impossible. He wore shoes to bed. We thought this was forever."
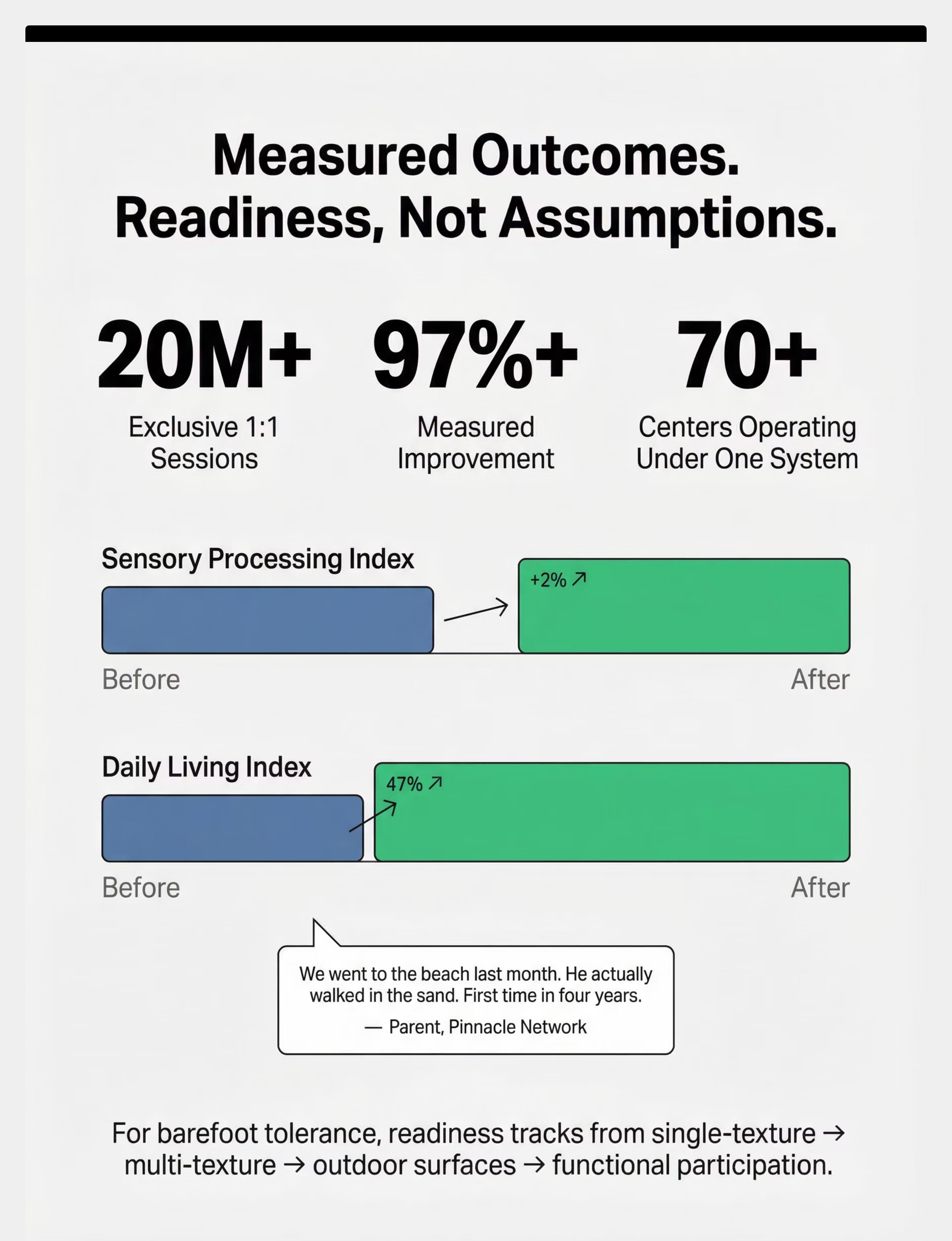
After (12 weeks later): "We went to the beach last month. He actually walked in the sand. First time in four years. I cried."
Timeline: Phase 1 took 3 weeks. Breakthrough came at Week 10 with the water play mat. — Parent, Pinnacle Network
Family Story 2 — 8-Week Journey
Before: "She screamed if her feet touched anything other than smooth tile. Getting dressed for school was a 45-minute battle every morning."
After (8 weeks later): "She now runs barefoot on our balcony. She chose the stepping stones as her 'game.' She asks for foot practice."
Timeline: The sensory bin was the turning point — once she controlled the experience, everything changed. — Parent, Pinnacle Network
From the Therapist's Notes
"Plantar tactile desensitization is one of the most responsive interventions we deploy. The combination of deep pressure preparation and child-led texture exposure works because it respects the child's nervous system rather than fighting it. Most families see meaningful progress within 6–10 weeks." — OT Lead, Pinnacle Blooms Network
Note: Illustrative cases; individual outcomes vary by child profile.

Isolation Is the Enemy of Progress. You Are Not Alone in This.
The parents who make the fastest progress are those who are connected — to other parents who understand, to communities who share strategies, and to professionals who support. Don't navigate this alone.
📱 Tactile Sensitivity Parent Support Group
WhatsApp community of parents navigating texture-related challenges. Share tips, ask questions, celebrate wins with families who understand your daily reality. Join thousands of parents across India.
🌐 Pinnacle Parent Forum
Online community for exchanging experiences, asking therapists questions, and finding local support. Moderated by Pinnacle professionals — clinical accuracy guaranteed.
🤝 Local Parent Meetups
Pinnacle centers organize monthly parent meetups in 70+ cities across India. Connect with families near you who understand your daily reality — in person, in your language.
👩🏫 Peer Mentoring Program
Connect with an experienced parent who has completed the barefoot journey. They've been exactly where you are — and they have practical wisdom that no clinical resource can replace.
"Your experience helps others. Consider sharing your journey when you're ready."
Home + Clinic = Maximum Impact
This protocol is designed for home execution — but professional support amplifies every session you run at home. Clinical assessment, ongoing guidance, and specialist expertise are available when you need them.

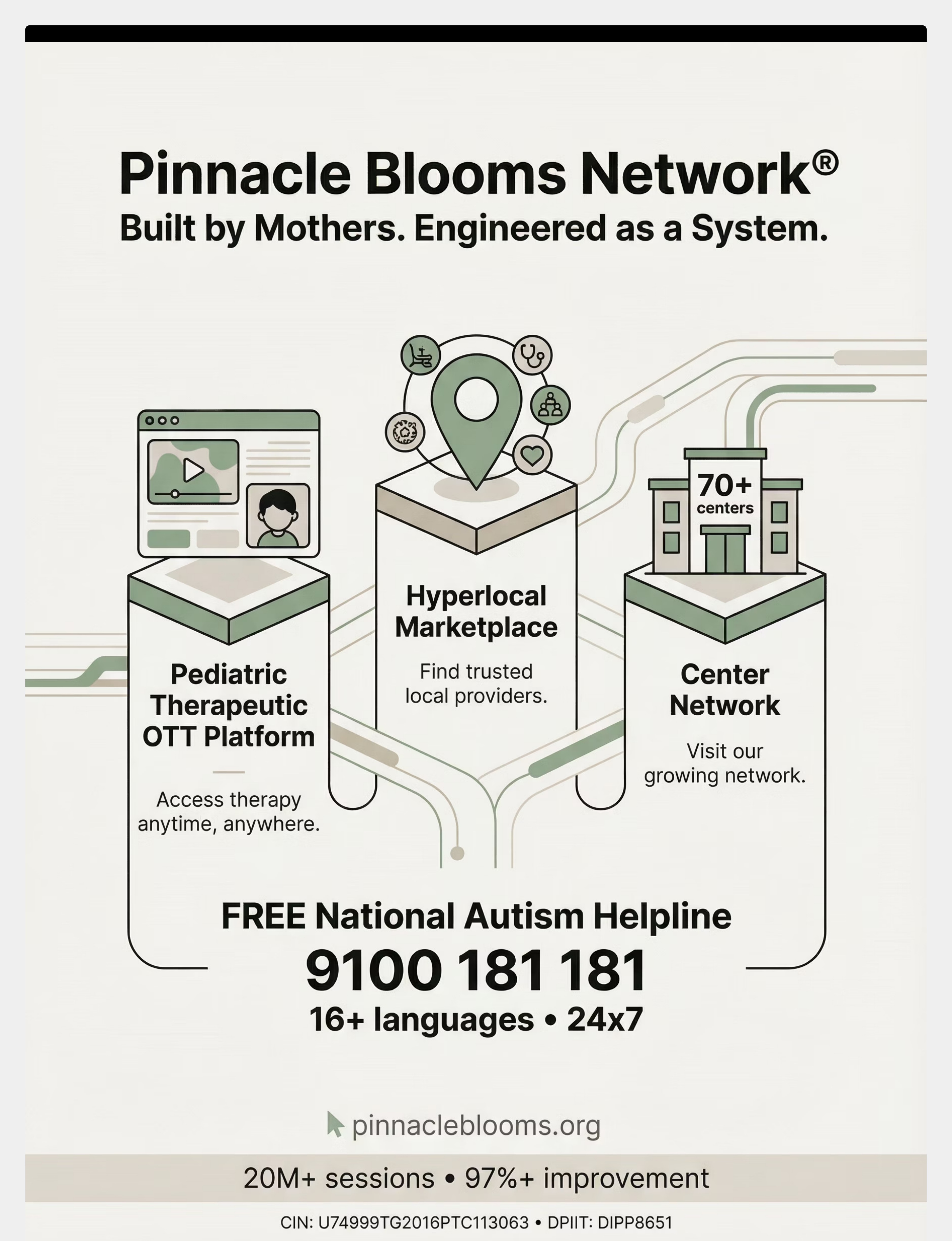
🏥 Find Your Nearest Pinnacle Center
70+ centers across India. Each center operates under GPT-OS® standards with OT, SLP, ABA, SpEd, and NeuroDev professionals under one roof.

👩⚕️ Therapist Matching
Get matched with an OT who specializes in tactile desensitization and sensory integration for your child's specific age and profile.

📹 Teleconsultation
Can't visit a center? Book a video consultation with a qualified OT who can review your child's specific sensory profile and customize this protocol.
📞FREE National Autism Helpline: 9100 181 181 | 16+ languages | 24x7 | Speak to a qualified professional about your child's sensory concerns — at no cost.
Services Relevant to This Technique
- Occupational Therapy & Sensory Integration Therapy
- Parent Training (EverydayTherapyProgramme™)
- AbilityScore® Assessment — sensory profile within Diagnostic Intelligence Layer
Reference: WHO NCF Progress Report 2018–2023 — Primary health care as platform for ECD
Deeper Reading for the Curious Parent
The protocol on this page is grounded in peer-reviewed science. For parents and professionals who want to go deeper, here is the evidence library behind every recommendation.
Study 1 — Systematic Review (Level I)
"Sensory Integration Intervention for Children with Autism Spectrum Disorder" — PRISMA systematic review. 16 articles (2013–2023) confirm sensory integration meets evidence-based practice criteria. PubMed: PMC11506176
Study 2 — Meta-Analysis (Level I)
"Efficacy of Sensory Integration Therapy" — World Journal of Clinical Cases. 24 studies. Promoted social skills, adaptive behavior, sensory processing, and motor skills. PubMed: PMC10955541 | DOI: 10.12998/wjcc.v12.i7.1260
Study 3 — RCT, India (Level II)
Padmanabha et al., Indian Journal of Pediatrics (2019). Home-based sensory interventions demonstrated significant outcomes in the Indian ASD population. DOI: 10.1007/s12098-018-2747-4
Study 4 — Neuroscience Framework (Level IV)
Frontiers in Integrative Neuroscience (2020). Comprehensive framework for evaluating sensory integration treatment in ASD. DOI: 10.3389/fnint.2020.556660
Study 5 — WHO/UNICEF (Level V)
WHO Care for Child Development Package (2023). Caregiver-mediated developmental interventions across 54 LMICs. PMC9978394
Foundational Texts
- Ayres, A.J. — Sensory Integration and the Child (25th Anniversary Edition). Western Psychological Services.
- Dunn, W. — Sensory Profile 2: User's Manual (2014). Pearson.
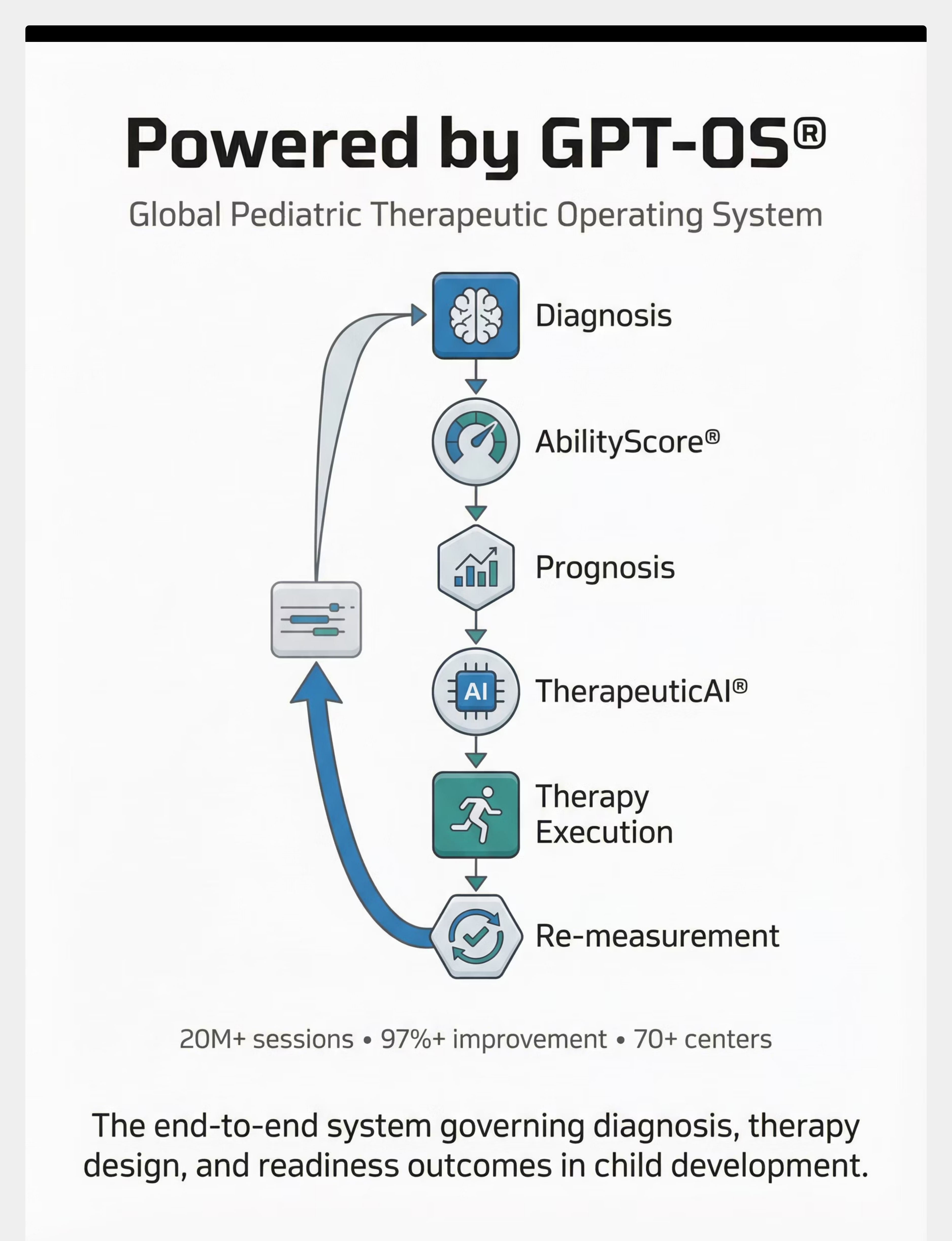
Powered by GPT-OS® — Global Pediatric Therapeutic Operating System
Every data point you record feeds an adaptive system that learns your child's specific patterns and improves recommendations across every session, every phase, and every domain.
What GPT-OS® Learns from This Technique
- Your child's specific texture hierarchy and preferences
- Optimal session timing and duration for your child
- Phase transition readiness signals — when to advance
- Material effectiveness ranking for your child's profile
- Predictive trajectory for barefoot tolerance development
Your Data Tracked Within
- Primary: Sensory Processing Index
- Secondary: Daily Living & Independence Index
- Sub-Index: Tactile Processing & Environmental Navigation
Readiness Progression
Single-texture tolerance → Multi-texture tolerance → Novel texture approach → Outdoor surface tolerance → Functional barefoot participation
20M+
1:1 Sessions
Completed across the network
97%+
Measured Improvement
Across tracked outcome domains
70+
Centers
Across India, GPT-OS® powered
160+
Countries
Patents filed across global jurisdictions
"Your data helps every child like yours. This is not software. This is therapeutic infrastructure."
Privacy: Your child's data is secured within GPT-OS® under ISO/IEC 27001 information security standards. Data is used to improve recommendations for your child and, in aggregate, for all children in the network.

Watch: 9 Materials That Help When Child Won't Walk Barefoot
Reel ID: A-012
Domain: Sensory → Tactile
Series: Sensory Solutions — Episode 12
Watch a Pinnacle therapist demonstrate each of the 9 materials in this technique. See exactly how to present them, how children respond, and what successful engagement looks like in a real session — before you try it at home.
📹 What the Reel Covers
- All 9 materials demonstrated in sequence
- Therapist narration of each material's purpose
- Real child responses — approach and avoidance
- Correct technique for applying deep pressure
- How to set up your sensory bin
⏱ Format
Duration: 60 seconds
Format: Therapist-presented | Vertical mobile-first
Language: English with subtitles
Accessibility: Captions available
Format: Therapist-presented | Vertical mobile-first
Language: English with subtitles
Accessibility: Captions available
"Video modeling is classified as an evidence-based practice for autism (NCAEP, 2020). Multi-modal learning — visual + text + demonstration — improves parent skill acquisition significantly over text alone."

Consistency Across Caregivers Multiplies Impact
If only one parent executes this technique, progress is real — but limited. When every caregiver in your child's life understands and supports the protocol, progress accelerates dramatically. Share this page today.
📲 Share on WhatsApp
Send this page with a single tap to your spouse, your child's grandparents, aunts, uncles, and extended family. The more caregivers who understand, the faster the progress.
📧 Share by Email
Forward to your child's school, therapy team, and extended support network. Include the Teacher Communication Template for school-specific guidance.
🔗 Copy the Link
Share anywhere — social media, therapy groups, parenting forums. This resource is free and publicly accessible.
Downloadable Resources
📄 Family Guide PDF
1-page simplified version for grandparents and extended family
📄 Teacher Communication Template
Explain your child's sensory needs to school staff with clinical authority
📄 Caregiver Quick-Reference Card
Wallet-sized do's and don'ts for every caregiver in your child's life
"Explain to Grandparents" Version: "Your grandchild's feet are extra sensitive — like having a sunburn on the bottom of their feet. We're using special materials to help them get used to different surfaces slowly. When they visit, please don't remove their socks or make them walk barefoot. If you'd like to help, use the foot roller during play time — they'll show you how."
Reference: PMC9978394 — WHO CCD Package emphasizes multi-caregiver training for intervention generalization
Frequently Asked Questions
These are the questions parents ask most often — answered clearly, practically, and without clinical jargon.
How long until my child walks barefoot on grass?
Most children in the protocol show meaningful progress within 6–10 weeks, with functional barefoot participation emerging at 13–16 weeks. Every child's timeline is different. Progress is measured in centimeters, not kilometers.
Can I do this without buying any materials?
Yes. Card 10 provides zero-cost alternatives for every material using household items. A tennis ball, rice in a baking tray, and inside-out socks is a complete starter kit.
What if my child is also sensitive to hand textures?
Tactile defensiveness often affects multiple body areas. This protocol focuses on feet, but the same materials (sensory bins, therapy putty, texture gradients) can be adapted for hands. See A-020: General Tactile Defensiveness for a whole-body protocol.
Is this safe to do without a therapist?
This protocol is designed for parent execution at home. The safety card (Card 11) and red flags card (Card 27) provide clear boundaries. If you stay within these guidelines and follow the child-led principle, home execution is safe and evidence-supported.
My child is under 2 years old. Can I start?
The protocol is designed for ages 2–8. For younger children, focus on Phase 1 (deep pressure) only and consult an OT for age-appropriate adaptation before proceeding.
Should I stop clinic-based OT if I'm doing this at home?
No. Home + clinic = maximum impact. This protocol extends therapy into daily life. It does not replace professional assessment and treatment — it deepens and extends it.
What if my child's school requires barefoot activities?
Share the Teacher Communication Template (Card 37) with your child's school. Request sensory accommodations while the protocol is in progress. Most schools are receptive when provided clear clinical guidance.
My child is non-verbal. How do I know if they're in distress?
Watch for behavioral distress signals: facial grimacing, body rigidity, foot withdrawal, crying, self-injury attempts, or attempts to leave. For non-verbal children, behavioral observation replaces verbal report. When in doubt, stop — safety first, always.

You've Read the Science. You've Seen the Materials. You Know the Protocol. Now Begin.
Everything you need is on this page. The knowledge is in your hands. The materials can be gathered today — many from your own home. The only remaining step is the first one.
🟢 Start This Technique Today
Launch GPT-OS® Guided Session for A-012 — step-by-step voice-guided protocol execution with automatic data capture and progress tracking.
📞 Book a Consultation
Speak to a Pinnacle OT about your child's specific sensory profile. FREE National Autism Helpline: 9100 181 181 (24x7, 16+ languages) or book teleconsultation online.
➡️ Explore Next Technique
A-014: Sand Play Avoidance (if progressing well) • A-013: Clothing Tag Sensitivity (if exploring tactile domain) • Browse Full Technique Library at techniques.pinnacleblooms.org
✓ Validated by the Pinnacle Blooms Consortium®
OT • SLP • ABA • SpEd • NeuroDev
Preview of 9 materials that help when child wont walk barefoot Therapy Material
Below is a visual preview of 9 materials that help when child wont walk barefoot therapy material. The pages shown help educators, therapists, and caregivers understand the structure and content of the resource before use. Materials should be used under appropriate professional guidance.









Link copied!

From Fear to Mastery. One Technique at a Time.
Pinnacle Blooms Consortium®
OT • SLP • ABA • SpEd • NeuroDev
A parent arrived on this page scared, confused, and exhausted. Now they understand the science. They have the materials. They know the protocol. They have a community. They have professional backup. They have data-driven guidance from GPT-OS®.
This is what therapeutic infrastructure looks like.
Our Mission
Pinnacle Blooms Network® exists to transform every home into a proven, scientific, 24x7, personalized, multi-sensory, multi-disciplinary, integrated therapy center for pediatric development. Powered by GPT-OS®. Built by mothers. Engineered as a system.
Legal Disclaimer
This content is educational and informational. It does not replace assessment by a licensed occupational therapist or other qualified healthcare professional. If barefoot avoidance is part of broader sensory concerns, please consult a qualified professional. Individual results vary. Sensory tolerance progression should be child-led and never forced.
40M+ Knowledge Units
40 Cards × 70,000+ Techniques = 2,800,000 Evidence-Linked Knowledge Units. The largest structured pediatric intervention knowledge base on Earth.
WHO-Aligned Standards
Every technique validated against WHO Nurturing Care Framework, NCAEP Evidence-Based Practices, and PubMed-referenced research.
Equity First
Zero-cost alternatives for every material. Available in 16+ languages. Accessible to every family, regardless of geography or economic status.
© 2025 Pinnacle Blooms Network®, unit of Bharath Healthcare Laboratories Pvt. Ltd. All rights reserved. CIN: U74999TG2016PTC113063 | DPIIT: DIPP8651 | MSME: TS20F0009606
techniques.pinnacleblooms.org | The Pinnacle Blooms Consortium®