
Everyone else's kid loves slime. Mine runs away screaming.
It's the birthday party where all the kids are elbow-deep in slime and your child is pressing against the wall, hands behind their back, eyes wide with terror. It's Tuesday morning when the preschool teacher says "finger painting today" and your child's face crumbles. It's the hundredth trip to the sink because a single grain of rice stuck to their palm.
You are not failing. Your child's nervous system is speaking a language most people cannot hear. This page will teach you to speak it back.
Tactile Desensitization for Slime and Texture Aversion — 9 materials, a 7-phase progression, and a protocol you can run from your kitchen table.
Ages 2–10
Sensory — Tactile Defensiveness
Technique ID: A-008
Pinnacle Blooms Consortium Validated
Pinnacle Blooms Network® | Built by Mothers. Engineered as a System. | GPT-OS® Therapeutic Intelligence
You Are Not Alone — The Numbers
Millions of families around the world are navigating exactly what you're experiencing. What your child feels has a name, a neurological basis, and a proven intervention pathway.
80%
Children with autism experience sensory processing difficulties
Source: PRISMA Systematic Review, Children (2024) | PMC11506176
1 in 6
Children worldwide show clinically significant tactile over-responsivity
Source: SPD Foundation prevalence data
~4M
Families in the US navigating tactile defensiveness in their child
Extrapolated from ASD prevalence × 80% sensory involvement, CDC pediatric data
You are among millions of families navigating this exact challenge. What your child experiences has a name, a neurological basis, and a proven intervention pathway.
Research: PRISMA systematic review (2024) — 16 articles from 2013–2023 confirm sensory integration intervention meets evidence-based practice criteria for children with ASD. References: PMC11506176 | PMC10955541 | DOI: 10.12998/wjcc.v12.i7.1260
What's Happening in Your Child's Brain
The Signal Path
The Wiring Difference
Your child's somatosensory cortex — the brain's touch-processing center — over-amplifies tactile signals. When slime touches their palm, their brain doesn't register "interesting texture." It registers "DANGER."
Light Touch vs. Deep Pressure
Light, unexpected touch (sticky, slimy, wet) activates your child's protective alarm system. Firm, deep pressure (tight hugs, heavy blankets) activates the calming system. This is why the same child who screams at slime may crave tight squeezes.
The Habituation Gap
In typical development, repeated exposure to a texture reduces the brain's response. In tactile defensiveness, this habituation process is impaired — each exposure can feel as intense as the first.
This is a wiring difference, not a behavior choice. The distress is real. The avoidance is protective.
Research: Frontiers in Integrative Neuroscience (2020): Comprehensive framework establishing neurological basis for sensory-based interventions in ASD. Reference: DOI: 10.3389/fnint.2020.556660
Where This Sits in Development
Tactile defensiveness doesn't appear in a vacuum — it intersects with your child's developmental journey at key moments. Understanding when it matters most helps you understand why you're here now.
6–12 Months
Begins exploring textures orally and with hands
12–18 Months
Tolerates messy eating; begins sensory play
18–24 Months
Finger painting, sand play emerge as normative
⚠️ 2–3 Years
CHALLENGE ZONE — Tactile defensiveness most commonly identified here
3–5 Years
Sensory play becomes critical for school readiness — art, crafts, science
5–8 Years
Social impact increases — peer play, birthday parties, school art
8–10 Years
Self-awareness and self-advocacy skills become primary targets
Tactile defensiveness commonly co-occurs with: auditory sensitivity (A-003), visual overwhelm (A-005), food texture aversion (A-012), clothing sensitivity (A-009), and grooming difficulties (A-010).
Your child is here. Here is where we're heading: From texture avoidance → to texture tolerance → to texture participation → to texture enjoyment (at their own pace).
Research: WHO Care for Child Development (CCD) Package — Age-specific evidence-based recommendations for caregivers. Implemented in 54 countries. References: PMC9978394 | WHO/UNICEF CCD Package (2023)
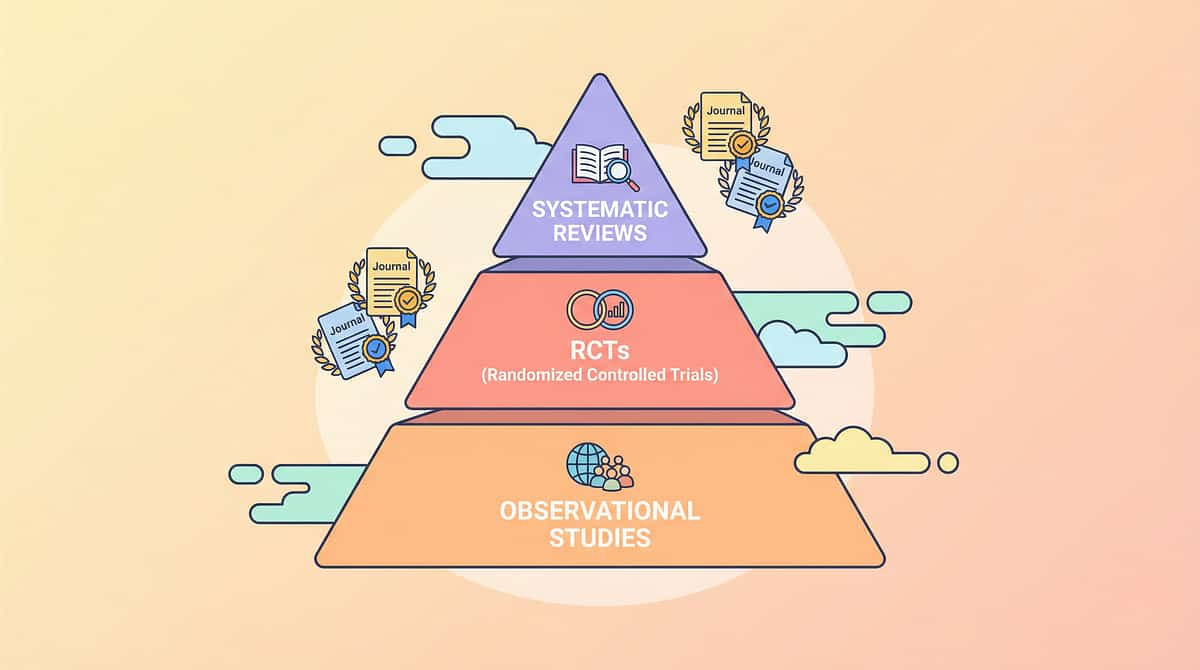
The Evidence Behind This Technique
This isn't an experimental approach. Tactile desensitization through graduated sensory exposure has rigorously been studied, systematically reviewed, and internationally validated.
Evidence Grade
LEVEL I
Systematic Review + Meta-Analysis — the highest standard of clinical evidence
EVIDENCE-BASED PRACTICE
What the Research Shows
- 16 studies (2013–2023) reviewed under PRISMA systematic review criteria
- 24 studies in meta-analysis confirming effectiveness across social skills, adaptive behavior, sensory processing, and motor skills
- Home-based delivery validated in RCT (Padmanabha et al., 2019)
- WHO/UNICEF endorsed through Nurturing Care Framework implementation across 54 countries
Sensory integration intervention, delivered through graduated material exposure with child-led pacing, meets criteria for evidence-based practice in pediatric autism intervention.
85%
Evidence Confidence
Strong evidence base with multiple systematic reviews supporting this technique
Clinically validated. Home-applicable. Parent-proven. References: PMC11506176 | PMC10955541 | DOI: 10.1007/s12098-018-2747-4 (Padmanabha et al., Indian J Pediatr, 2019)

The Technique — What It Is
Formal Name: Graduated Tactile Desensitization Protocol for Texture Aversion
Parent-Friendly Alias: "Teaching hands the world is safe to touch"
A structured, child-led approach that introduces tactile textures in a carefully graded sequence — from completely dry and predictable materials to progressively wetter, stickier, and more challenging textures. The child controls the pace. Every session includes escape options (wipes, water, stopping). Progress is measured in seconds of tolerance, not in "playing like other kids."
Nine specific therapeutic materials serve as the vehicles for this progression, each targeting a different point on the texture spectrum.
Domain
A — Sensory Processing (Tactile Defensiveness)
Age Range
2–10 years
Session Duration
10–20 minutes
Frequency
3–5 sessions per week
Timeline
8–12 weeks per progression phase
Canon Materials: Sensory Bins, Theraputty, Water Beads, Kinetic Sand, Tactile Brushes, Shaving Cream, Finger Paint Bags, Gloves/Tools, Edible Sensory Materials

Who Uses This Technique
Tactile desensitization crosses therapy boundaries — because the brain doesn't organize by therapy type. Your child's OT, BCBA, SLP, and teacher may all use variations of this approach, and that's by design.
Occupational Therapist (OT) — Primary Lead
Designs the sensory diet, selects materials, establishes the desensitization progression ladder, trains parents on correct techniques. The Wilbarger Protocol brushing component must be OT-initiated and supervised.
Applied Behavior Analyst (BCBA/RBT) — Secondary
Structures the reinforcement schedule, designs the data collection protocol, analyzes session data for decision-making, implements systematic desensitization using ABA pairing principles.
Speech-Language Pathologist (SLP) — Contributing
Addresses oral tactile defensiveness (food textures), links tactile tolerance to feeding therapy goals, collaborates on edible sensory play protocols.
Special Educator (SpEd) — Contributing
Adapts classroom sensory activities, implements IEP accommodations for art/science/messy play, bridges clinic-to-school generalization.
Research: Adapted UNICEF/WHO Nurturing Care Framework for SLPs (2022): Multiple disciplines contribute to nurturing care components. Reference: DOI: 10.1080/17549507.2022.2141327
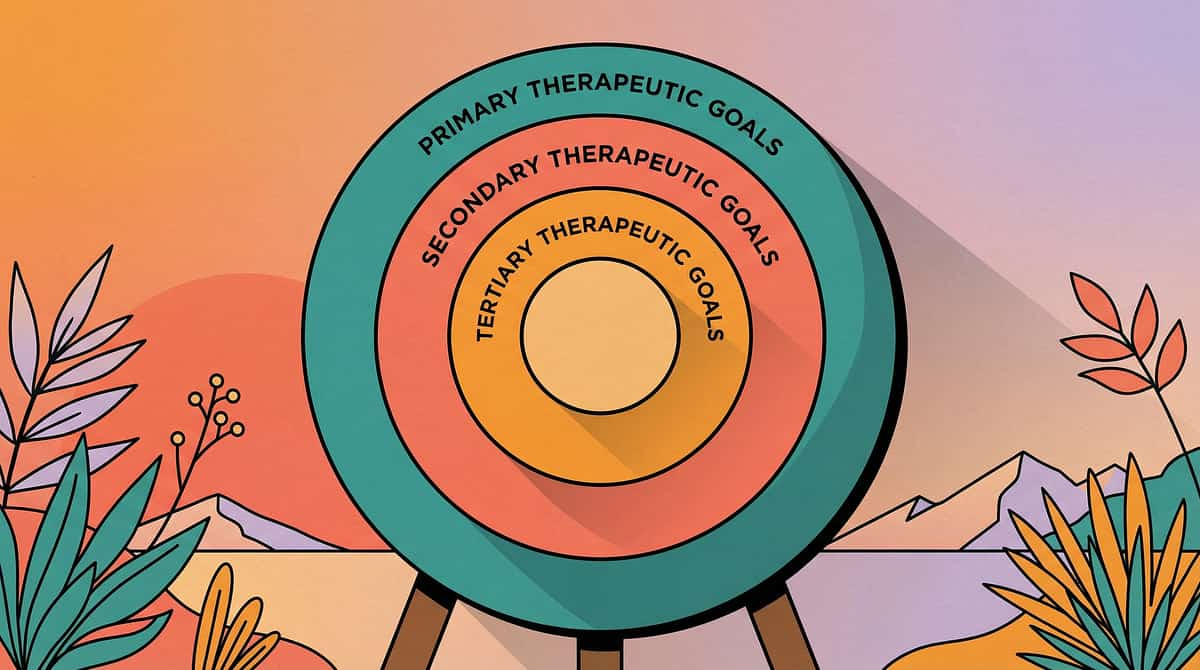
What This Technique Targets
The primary goal of tactile desensitization is building tolerance — but the ripple effects extend far beyond the fingertips. Every session touches multiple areas of your child's development simultaneously.
Observable Primary Indicators
Duration of contact increases, distress level decreases, voluntary touch attempts emerge in structured and unstructured settings
Secondary Growth Areas
Fine motor engagement through material manipulation builds hand strength and coordination alongside emotional regulation capacity
Long-Term Life Impact
Self-care independence, academic participation in hands-on learning, self-advocacy around tactile needs and preferences
Research: Meta-analysis (World J Clin Cases, 2024): Sensory integration therapy effectively promoted social skills, adaptive behavior, sensory processing, and motor skills across 24 studies. Reference: PMC10955541
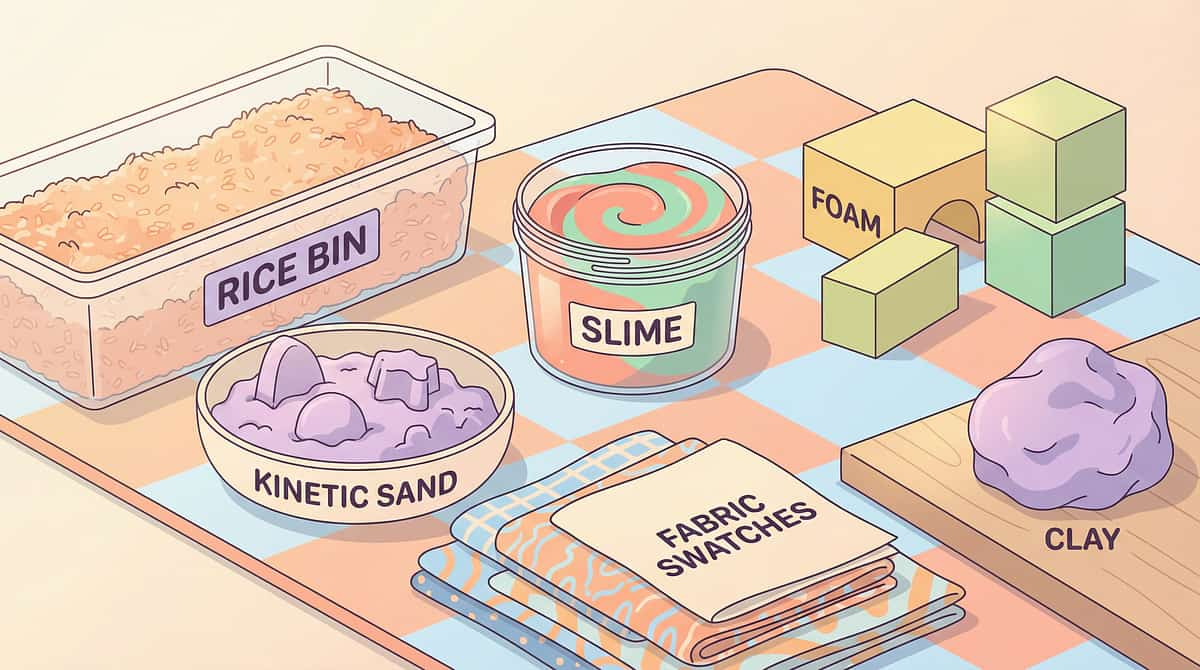
The 9 Primary Materials — What You Need
These nine materials form the complete tactile desensitization toolkit, each targeting a different point on the texture spectrum — from completely dry and predictable to wet, sticky, and challenging.

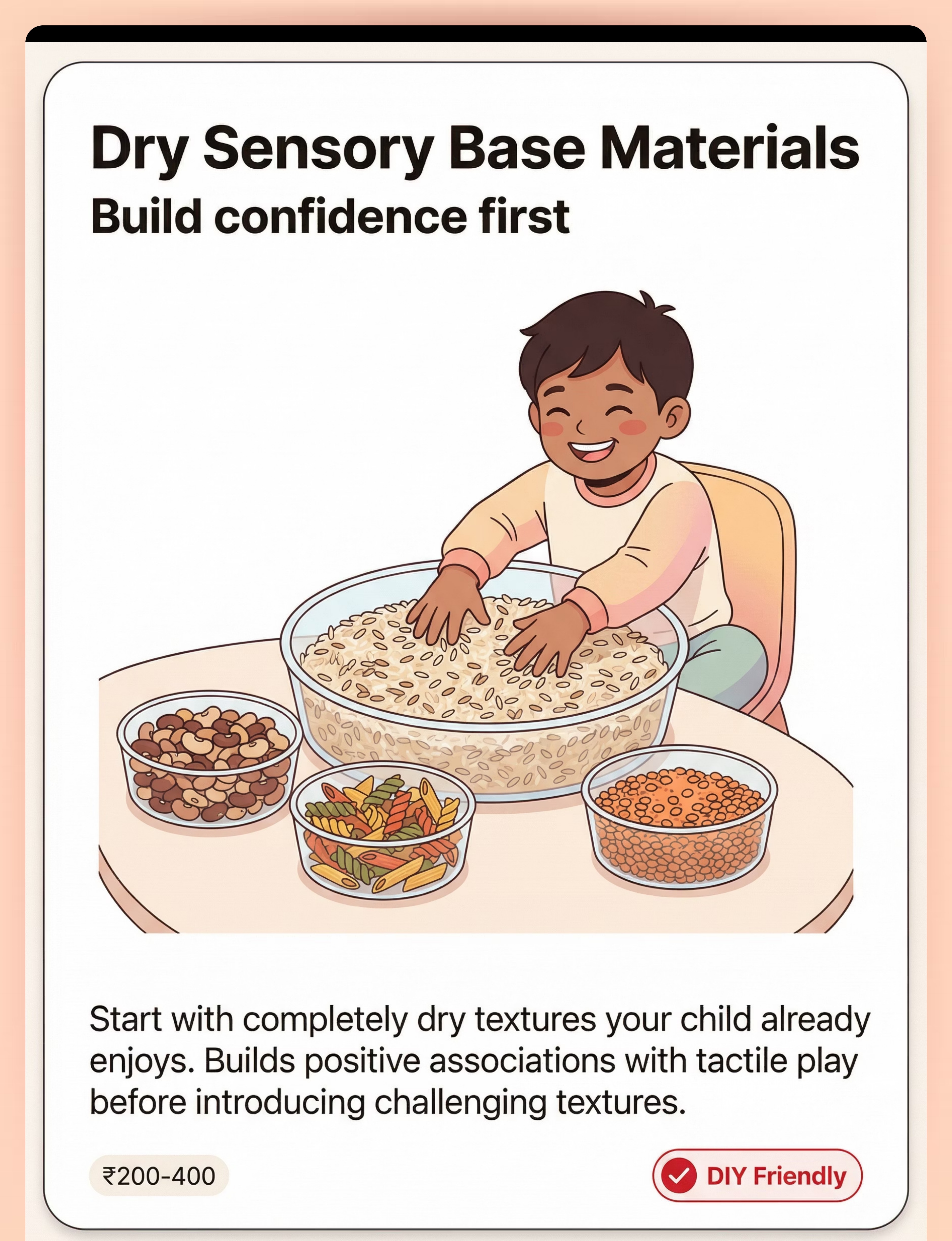
1. Dry Sensory Bins (Rice, Beans, Pasta)
Starting point for nearly every child. Completely dry, predictable, and familiar from the kitchen. Perfect first-phase material.
DIY Friendly

2. Theraputty / Therapy Dough
Moldable, non-sticky, resistive. Builds hand strength while providing controlled tactile input. Professional recommendation.
⭐ Professional Recommendation

3. Water Beads (Contained System)
Introduces wet, smooth, slippery properties in a controlled way. Bridge material from dry to wet textures.
⚠️ Ages 3+ Only

4. Kinetic Sand
Feels dry but molds like wet sand. Non-sticky. Deeply satisfying. One of the most successful bridge materials on the ladder.
DIY Alternative Available
5. Tactile Brushes (Wilbarger Protocol)
Surgical-grade soft brushes used for proprioceptive input. Activates the calming system. OT training required — no substitutes.
🔴 OT Training Required

6. Shaving Cream (Controlled Introduction)
First wet-and-light-messy material on the ladder. Wipeable, non-staining, visually accessible. Easy to control quantity.
DIY Friendly

7. Finger Paint in Bags (No-Touch Option)
Child experiences color and movement without direct contact. Barrier-protected entry point to messy art materials.
DIY Friendly

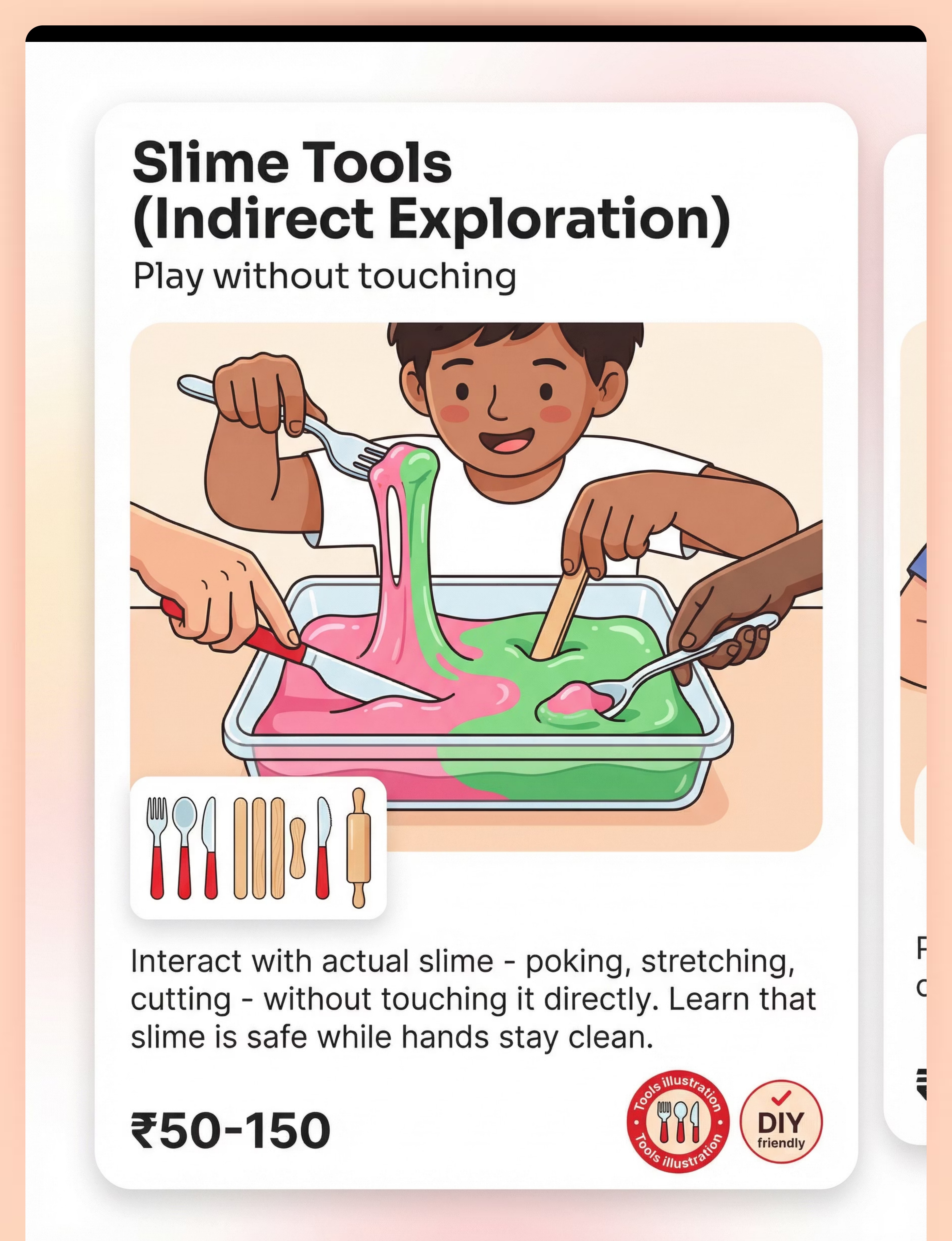
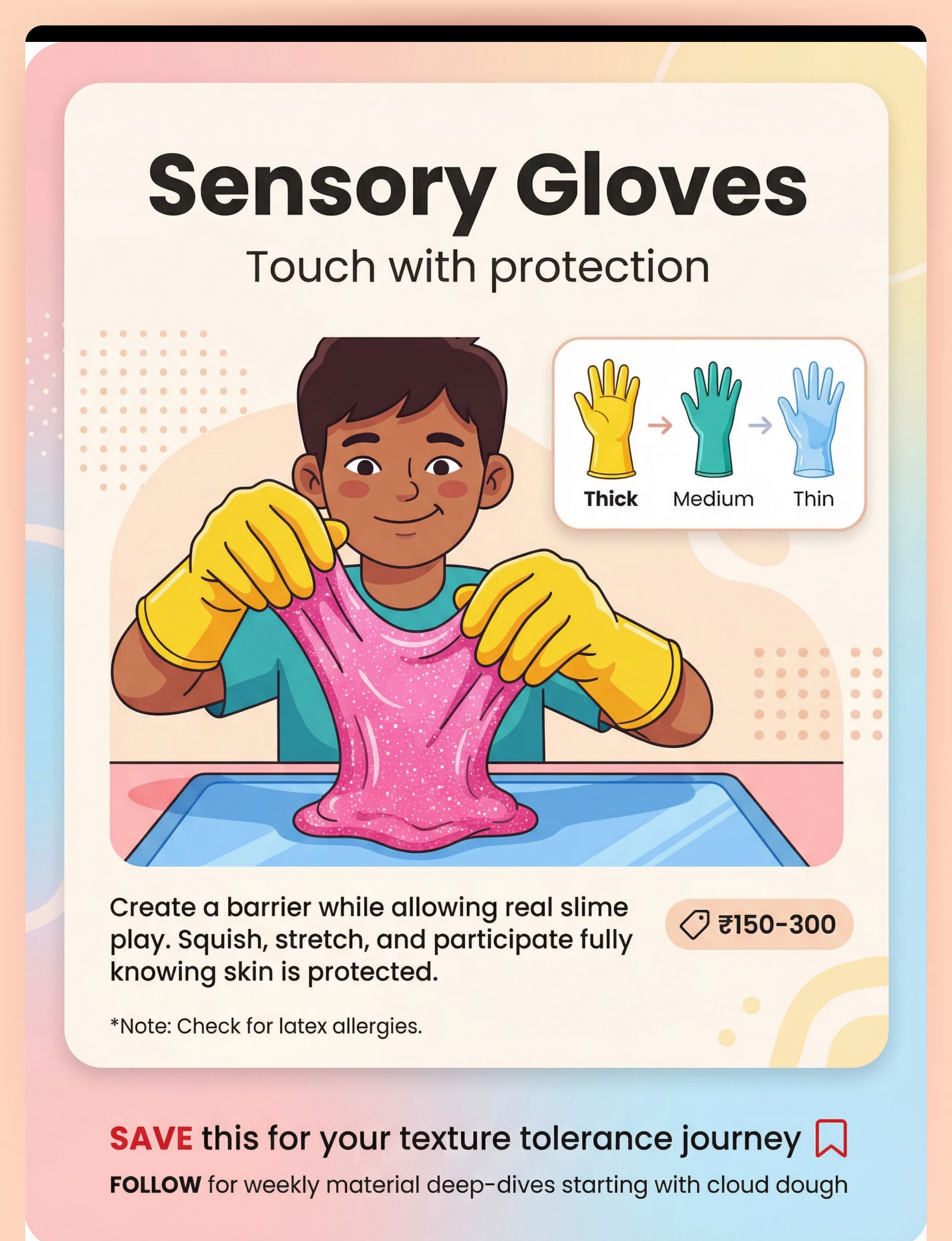
8. Gloves and Tools (Barrier Options)
Enables immediate participation in sensory activities while maintaining tactile safety. Gloves, spoons, scoops — all valid tools.
Immediate Participation

9. Edible Sensory Play Materials
Safe for mouthers. Pudding, whipped cream, cooked pasta. Bridges hand-based tolerance to oral tolerance. Ideal for ages 2–3.
Kitchen Ingredients
Essential Starters: Dry Sensory Bins + Theraputty + Gloves — the safest, lowest-barrier entry point to the protocol. Total investment for essentials: very low. Full toolkit: moderate.

DIY & Substitute Options
"Every parent can start TODAY. Zero cost."
The therapeutic principle is the texture property (dry, moldable, wet, sticky) — not the brand. Any material matching the target sensory property delivers the same neurological input. Here's how to replicate every material from your kitchen and pantry.
Buy This | Make This (Zero-Cost DIY) | |
Commercial Kinetic Sand | 4 cups fine sand + 2 cups cornstarch + 1 cup oil → mix until moldable | |
Theraputty | Cornstarch + conditioner → knead to non-sticky dough consistency | |
Cloud Dough | 8 cups flour + 1 cup oil → feels dry, molds like wet sand | |
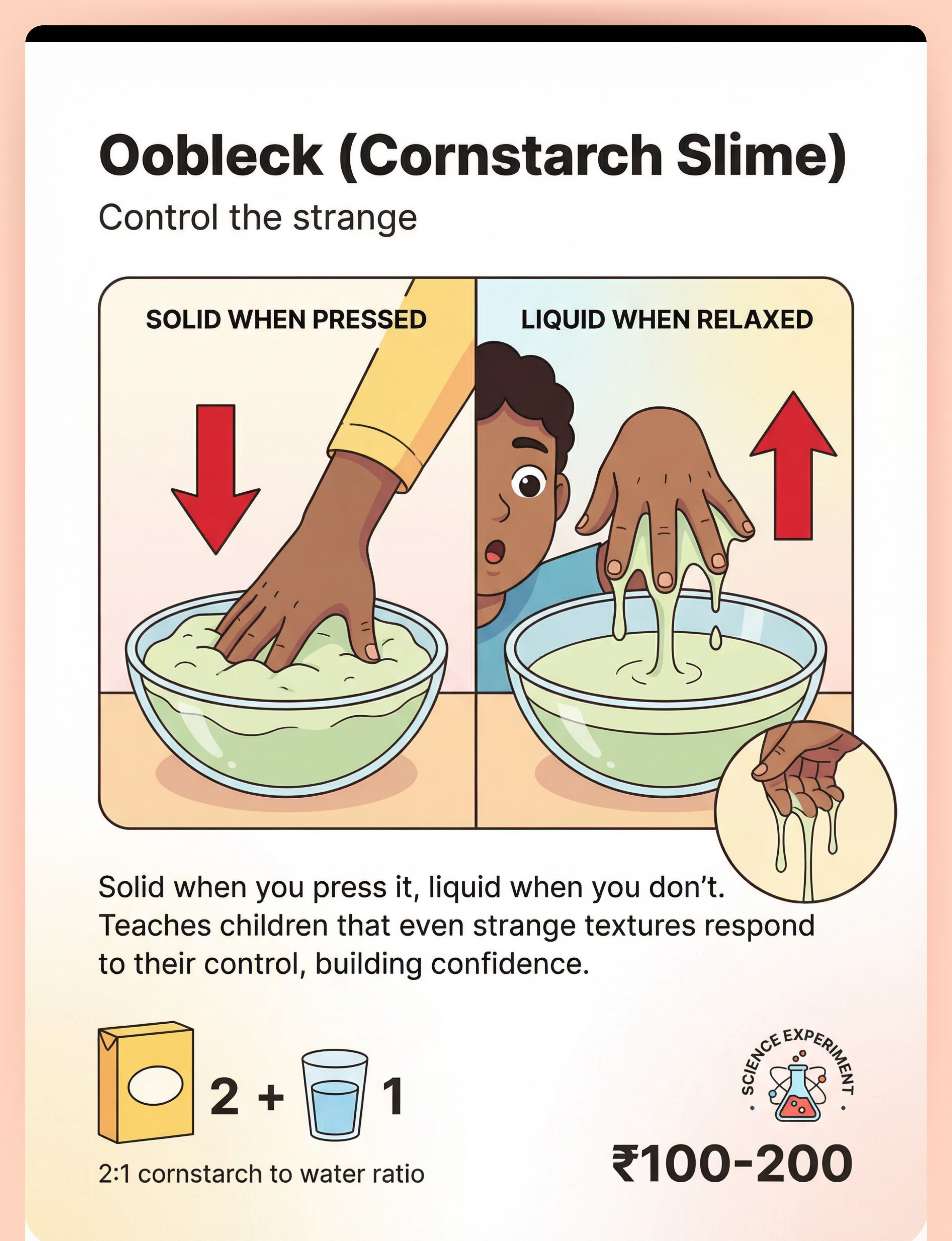
Oobleck/Cornstarch Slime | 2 parts cornstarch + 1 part water → solid when pressed, liquid when relaxed | |
Water Beads | Ice cubes, frozen grapes, or cooked tapioca pearls (safer for younger children) | |
Sensory Bin Fill | Dried rice, lentils, pasta from your kitchen pantry | |
Finger Paint Bags | Zip-lock bag + blobs of any paint OR hair gel + food coloring | |
Gloves | Food service gloves, cleaning gloves, or plastic bags over hands |
When Clinical-Grade is Non-Negotiable:⚠️ The Wilbarger Protocol Brush — must be the correct soft surgical brush. No household substitute exists. Must be paired with OT training.
Research: WHO Nurturing Care Framework (2018): Context-specific, equity-focused interventions. CCD Package across 54 LMICs validates household-material-based intervention efficacy. References: PMC9978394 | WHO NCF Handbook (2022)

Safety First — Before You Begin
The protocol is designed to be safe when followed correctly. Understanding what to stop, check, and always do is non-negotiable before your first session.
🔴 RED — Absolute Stop
- NEVER force tactile contact. Forced exposure causes trauma and worsens defensiveness.
- Water beads: serious choking and ingestion hazard. Not for children under 3 or any child who mouths objects.
- Wilbarger brushing: must be taught by trained OT. NEVER brush face, chest, or stomach.
- If child shows extreme distress, self-harm, or prolonged dysregulation — STOP and consult professional.
🟡 AMBER — Check First
- Latex allergies: use nitrile gloves if allergy status unknown.
- Food allergies: check before ANY edible sensory play.
- Small dry items (rice, beans, beads): choking hazard for children who mouth objects. Supervise constantly.
- Shaving cream: not for mouthers. Use whipped cream as edible alternative. Avoid fragranced varieties.
🟢 GREEN — Always Do
- Wipes, towels, and water within arm's reach at ALL times.
- Child can see cleanup supplies — reduces anxiety about being "stuck."
- Child controls duration — they decide when to stop.
- Warn before introducing textures. No surprise touch.
- Deep pressure input before light-touch exposure.
- Praise the ATTEMPT, not just the outcome.
The child must ALWAYS know they can stop, wipe, or leave. This non-negotiable escape option is what makes desensitization safe.
Research: Indian Journal of Pediatrics RCT (2019): Home-based sensory interventions safety protocols for parent-administered sessions. Reference: DOI: 10.1007/s12098-018-2747-4

Set Up Your Space
A predictable environment dramatically reduces your child's baseline anxiety before the session even begins. When the child knows exactly where everything is — especially the escape kit — they can take risks.
Room Positions
Child
Seated comfortably at table or on floor mat. Back supported. Feet grounded.
Parent
Beside the child (not across). Same eye level. Within arm's reach.
Materials
On tray or contained surface. Visible but not touching the child.
Escape Kit
Wipes, towel, water bowl — VISIBLE to child, within child's reach.
Timer
Visual timer showing session duration (optional but recommended).
Environment Settings
- Lighting: Soft, natural. No fluorescents.
- Sound: Quiet. Calm background music if child prefers.
- Temperature: Comfortable. Cold rooms increase tactile sensitivity.
- Surface: Easy-to-clean mat or tray underneath. Reduces parent anxiety about mess.
Remove from Space
- Distracting toys, screens, pets
- Other children (session is 1:1)
- Loud background noise
- Bright or flickering lights
Critical Principle: Predictable space = reduced anxiety. The child's nervous system can only attend to the sensory work when it feels safe in the environment.
Research: Sensory Integration Theory (Ayres): Structured environment is a core principle. Meta-analysis confirms 1:1 individual sessions in structured environment most effective. Reference: PMC10955541
Is Your Child Ready? — The Pre-Session Readiness Check
Sixty seconds of honest assessment before every session determines whether you're setting your child up for success or walking into a preventable meltdown. The best session is one that starts right.
1
Fed Within 2 Hours
Not hungry — hunger amplifies sensory sensitivity significantly
2
Adequately Rested
Not overtired — fatigue dramatically lowers sensory threshold
3
Currently Regulated
No meltdown in the last 30 minutes — child is in a calm baseline state
4
No Physical Discomfort
No illness, pain, or physical distress that would compound sensory sensitivity
5
Not Mid-Activity
Child is not in the middle of a preferred activity — avoid interrupting flow
6
Space Set Up
Environment is prepared per Card 12 checklist — escape kit visible and accessible
🟢 GO — All Checked
Proceed to Step 1: The Invitation
🟡 MODIFY — 1-2 Unchecked
Shorter session, easier material, lower expectations today
🔴 POSTPONE — 3+ Unchecked
Not today. Offer a calming activity instead — weighted blanket, deep pressure, preferred play
A postponed session is NOT a failed day — it's a wise decision. Your child's nervous system will thank you tomorrow.

Step 1: The Invitation
Step 1 of 6
30–60 Seconds
The Invitation is the most important moment in the session. Your tone, your body language, and your non-urgency set the neurological stage for everything that follows. If you feel rushed, your child will feel it too.
"Hey [child's name], look what I have today! Want to come see?" [Place material on tray, visible but 3 feet away. Do NOT bring it to the child.]
Your Body Language
- Relaxed posture. Smile. No urgency.
- Touch the material yourself first. Let them see YOU enjoying it.
- No eye contact pressure. Casual glance.
What Acceptance Looks Like
Child moves toward the material, looks at it, asks about it, reaches toward it, or says "okay." ANY approach behavior counts.
What Resistance Looks Like
Child turns away, says "no," moves backward, covers hands, shows anxiety. This is okay.
If Resistance Occurs
"That's okay! It'll be here if you want to check it out." Leave material visible. Continue with a different activity. Revisit in 5 minutes with even lower demand: "Want to just LOOK at it with me?"
Timing: 30–60 seconds. Do not extend the invitation phase. Lingering creates pressure. Move on naturally, and let curiosity do the work.
Research: ABA Pairing — establishing motivating operations before demand. OT "Just-Right Challenge": matching task demand to child's current capacity.

Step 2: The Engagement
Step 2 of 6
1–3 Minutes
The child is approaching. Now your job is to meet them exactly where they are — not where you hope they'll be. Present the material at their comfort level, using the current phase material from the 9-material progression ladder.
If Dry Sensory Bin
Pour rice through YOUR fingers first. Let child hear the sound. Offer a scoop/spoon (tool first, NOT hands). "Want to try the scoop?"
If Theraputty
Squeeze it yourself. Show how hands stay clean after. Offer to hold it while child pokes with ONE finger.
If Kinetic Sand
Cut it with a plastic knife (satisfying). Let child watch it flow. "It sticks to itself, not to you. Want to try cutting it?"
Speed
Slow. Every movement predictable. No surprises.
Distance
Material on tray. Child decides when to touch.
Position
Beside the child, not across from them.
The MOMENT the child makes any contact — even a fingertip touch lasting half a second — immediate, specific praise: "You touched it! Your finger touched the rice! That was brave."
Research: Systematic review (Children, 2024): Sensory integration intervention with structured material introduction meets evidence-based criteria. Reference: PMC11506176

Step 3: The Therapeutic Action
Step 3 of 6
3–5 Minutes
The child is now touching or interacting with the material. This is the active desensitization window — the moment the nervous system receives the tactile input and begins learning: "This is not dangerous." Your role shifts from inviter to narrator and witness.
What to Do Right Now
- Narrate what the child is experiencing: "The rice feels smooth. It's dry. It falls right off your hand."
- Match the child's pace. If they touch for 2 seconds, celebrate 2 seconds. Do NOT push for 10.
- If child uses tools, that IS participation. Tool use counts as engagement.
- Offer gentle escalation ONLY if child is comfortable: "Want to try with your other hand too?"
Duration of Exposure by Stage
- First sessions: ANY contact counts — even 1 second
- Building sessions: 30 seconds to 2 minutes of active contact
- Advanced sessions: 3–5 minutes of sustained play
Child Response Spectrum
- ✅Ideal: Engaged, curious, reaching for more
- ✅Acceptable: Tolerating with mild discomfort, brief contact then wiping
- ⚠️Concerning: Escalating distress, pulling away repeatedly, crying → Move to Step 5
Research: Meta-analysis (2024): 40-minute clinical sessions showed maximum effectiveness. Home sessions: 10–20 minutes; core action occupies 40–60% of session time. Reference: PMC10955541
Step 4: Repeat & Vary
Step 4 of 6
3–5 Minutes
Repetition is where the neural pathway forms — but forced repetition erases every gain you've made. The goal is rhythm, not volume. Three confident touches that end in a smile matter more than ten reluctant ones that end in tears.
The 3 > 10 Principle: 3 good repetitions where the child feels successful are worth infinitely more than 10 forced contacts that end in tears.
Target: 3–5 Contact Episodes Per Session (Natural Rhythm — Not Forced)
Hide a Toy
"Can you find the dinosaur in the rice?"
Add Color
"Let's add food coloring — pick a color!"
Change Container
"Now let's try it in the big bowl"
Mix Textures
"Want to add pasta to the rice bin?"
Take Turns
"My turn, your turn" — social rhythm builds engagement
Satiation Indicators — When to Move to Step 5
Looking away from the material, pushing material away, saying "all done," decreasing engagement energy, or reaching for wipes/towel. When you see any of these signals — move on. Do NOT push through satiation.
Research: SI therapy dosage: 2–3 sessions/week for 8–12 weeks as typical protocol. Session-level repetition from clinical consensus.

Step 5: Reinforce & Celebrate
Step 5 of 6
Within 3 Seconds
Reinforcement is not about candy or prizes — it's about your child's nervous system learning that bravery is safe and acknowledged. The timing, specificity, and authenticity of your praise are the active ingredients.
"You TOUCHED it! You put your whole hand in the rice! I am SO proud of you. That was really brave."
1
Immediate
Within 3 seconds of the behavior. Not after cleanup. Not after you've tidied the tray. RIGHT NOW.
2
Specific
Name EXACTLY what they did. "You touched the theraputty with three fingers" — NOT "good job." Specificity teaches the child what bravery looks like.
3
Enthusiastic
Match your energy to the child's accomplishment. For a first touch, this is a BIG deal. Your excitement becomes their pride.
Reinforcement Menu
Verbal Praise (Always)
High-Five or Preferred Gesture
Token or Sticker Chart
Choice of Next Activity
Tell a Family Member
Celebrate the ATTEMPT, not just the success. A child who touched for 1 second and then wiped their hand deserves the same celebration as one who played for 5 minutes.

Step 6: The Cool-Down
Step 6 of 6
1–2 Minutes
The cool-down is not the end of the session — it IS the session's final therapeutic act. How you transition out of sensory work shapes your child's memory of the entire experience. A smooth ending builds willingness to return.
"Two more touches, then all done!" → [2 more] → "One more, then all done!" → [1 more] → "All done! Great work. Let's clean up together."
This sequence gives the child control over the ending, activates the calming proprioceptive system after tactile exposure, and anchors the session in positive memory through the transition to something they enjoy.
If Child Resists Ending
Positive sign — they're engaged! "We'll play with this again tomorrow. It'll be right here." Offer one more brief contact: "One last scoop, then it goes to sleep." Never end abruptly. Endings that feel safe make beginnings feel safe too.
Research: Visual timer and transition support — classified as evidence-based practice for autism (NCAEP, 2020).

Capture the Data — Right Now
Data collection is not optional — it's the engine of your child's personalized progression. Within 60 seconds of session end, record these three data points. Approximate is fine. Done is better than perfect.
Data Point 1 — Material Used
Which of the 9 materials? What progression level? Note if a tool or barrier was used.
Data Point 2 — Duration of Contact
How many seconds or minutes of voluntary tactile contact? Approximate is fine — 5 seconds vs. 5 minutes tells the story.
Data Point 3 — Distress Level (1–5)
1 = No distress, engaged happily | 2 = Mild discomfort, continued | 3 = Moderate, needed breaks | 4 = Significant, session shortened | 5 = Unable to engage, ended early
Date | Material | Level | Duration | Distress | Notes | |
___ | ___ | ___ | ___ sec | 1–5 | ___ | |
___ | ___ | ___ | ___ sec | 1–5 | ___ | |
___ | ___ | ___ | ___ sec | 1–5 | ___ |
60 seconds of data now saves hours of guessing later. Your data is what tells GPT-OS® how to personalize your child's next step.
Research: ABA Data Collection — continuous measurement (frequency, duration, latency) as standard for behavior-analytic intervention tracking. Reference: BACB Guidelines + Cooper, Heron & Heward
What If It Didn't Go as Planned?
Every session teaches you something. A session that didn't go as planned is not a failure — it is the most valuable data point you have collected. Here is how to interpret what happened and what to do next.
Problem 1: "My child refused to come near the material."
This IS data, not failure. Start at a greater distance. Let them WATCH you play with it. Even observation is a step. Consider: was the material too advanced on the progression ladder? Try again tomorrow at observation-only level.
Problem 2: "They touched it once and had a meltdown."
They TOUCHED it — that took courage. The meltdown means their nervous system is working; it just needs more time. Next session: shorter exposure, quicker access to wipes, more reinforcement for even looking at the material.
Problem 3: "Fine with dry materials but screamed at wet ones."
Correct — this is the progression working as designed. Insert "bridge textures": cloud dough (feels dry, molds like wet), kinetic sand, then shaving cream with immediate wipe access. Don't skip steps.
Problem 4: "Family thinks I'm 'giving in' or making it worse."
Share Card 03 (the neuroscience). This is a wiring difference, not a behavior problem. Forcing exposure causes trauma. Gradual, child-led desensitization is the evidence-based approach — see Card 05.
Problem 5: "3 weeks in and I see no change."
Check: are you tracking data? Small changes — 1 extra second of contact, one less hand-wash per day — ARE progress. Expect 8–12 weeks for visible shifts. If zero change at 8 weeks, consult your OT for protocol adjustment.
Problem 6: "My child became severely distressed."
Stop immediately. Offer deep pressure (firm hug, weighted blanket). No more attempts today. This tells you the material was too challenging — step back one level. If severe distress occurs repeatedly, consult a professional before continuing.
Session abandonment is not failure — it's data. The technique needs adjustment, not the parent.
Adapt & Personalize
No two children move through this protocol identically. The 9-material progression is a framework, not a rigid script. Use these modifications to match the protocol to your child's profile, age, sensory pattern, and daily readiness.
⬅️ Easier Modifications
For Bad Days / Early Sessions
- Tools only — scoop, pour, no hand contact
- One finger for one second, then wipe
- Material in sealed bag — feel through plastic
- Observation only — watch parent or video
- Shorter sessions (3–5 minutes total)
➡️ Harder Modifications
For Breakthroughs / Advanced Sessions
- Two-handed contact sustained for 2+ minutes
- Transfer between containers with hands
- Playing alongside a sibling or peer
- Mixing two textures simultaneously
- Progressing to next material on the ladder
Ages 2–3
Edible materials prioritized (safe if mouthed). Shorter sessions (5–7 min). Heavy parent modeling. Keep it playful and follow the child's lead completely.
Ages 4–6
Full 9-material protocol. Social motivation ("show Daddy what you did!"). Sticker charts for tracking bravery. Can begin understanding the "why."
Ages 7–10
Self-awareness language ("your brain is learning to feel safe"). Self-tracking with their own data sheet. Peer-based goals — "so you can do art at school."
Mixed Profile (seeks some, avoids others): Use preferred textures as bridges. "You love the rice — want to add some kinetic sand to the rice bin?"

Week 1–2: What to Expect
Progress Phase 1
~15% Complete
The first two weeks are about establishing the pattern, not achieving mastery. Your child's nervous system is learning that the session itself is predictable, safe, and controllable. That learning is happening even when it doesn't look like progress from the outside.
✅ What Progress Actually Looks Like
- Child tolerates being in the SAME ROOM as the material
- Contact time increases from 0 seconds to 2–5 seconds
- Child approaches the material voluntarily (even without touching)
- Fewer hand-washes per day (tracking this matters!)
- Willingness to WATCH parent interact with the material
✗ Not Expected Yet
- Playing happily with messy textures
- Touching all 9 materials
- Enjoying sensory play
- Joining peers in messy activities
If your child tolerates the material for 3 seconds longer than last week — that's real neural pathway formation happening in their somatosensory cortex right now. That is the work.
Research: Systematic review (Children, 2024): Early-phase indicators focus on tolerance and participation, not skill mastery. Reference: PMC11506176

Week 3–4: Consolidation Signs
Progress Phase 2
~40% Complete
Weeks three and four bring the first unmistakable signs that something is shifting — not just in your child's behavior, but in their relationship with the material. Watch for these consolidation indicators.
Anticipates the Session
"Are we doing rice today?" — your child is beginning to look forward to the work. This is enormous. Anticipation without dread means the nervous system is no longer classifying the material as a threat.
Shows Material Preference
Choosing kinetic sand over theraputty, or rice over pasta. Preference requires engagement — they can't prefer what they're still fleeing.
Sustained Contact
Touches for 15–30 seconds without prompting. Distress level drops from 3–4 to 2–3 on your tracking scale. Spontaneous touch outside structured sessions may begin.
Neural Pathway Signals
Reduced hand-washing frequency, less anxiety when warned about upcoming tactile activities, willingness to hold new items with different textures.
When to Increase Difficulty: If your child is consistently at Distress Level 1–2 for the current material, introduce the NEXT material on the 9-material ladder.
You may notice you're more confident too. Your hands are steadier, your voice is calmer, your timing is better. You're becoming a home therapist.
Week 5–8: Mastery Indicators
Progress Phase 3
~75% Complete
Mastery is not perfection — it is consistent, voluntary engagement with a material across settings and conditions. When your child has internalized a material's safety, the nervous system generalizes that learning to adjacent textures.
2+ Minutes Without Distress
Child interacts with the material for at least 2 minutes without significant distress signals
Voluntary Initiation
Child initiates contact — they reach for the material, not just tolerate it when offered
Positive Language
Child can identify the material and talk about it positively — "the rice is smooth," "kinetic sand is cool"
Generalization Across Settings
Tolerance persists at the table, on the floor, at a grandparent's house, and after a 3-day break
Maintenance
The skill holds even when not practiced daily — it has moved into long-term neurological memory
🏆 MASTERY — Progress
All 5 criteria met → Move to the next material on the 9-material ladder
🔄 STRENGTHEN
Stay at current level — add variations, social component, longer sessions, different settings
↔️ LATERAL MOVE
Try a different material at the same texture level — if kinetic sand is mastered, try regular sand

Celebrate This Win
You did this.
Your child started this journey unable to touch a material that seemed ordinary to everyone else. After weeks of consistent, patient, child-led sessions, they can now engage with it voluntarily. This is not luck. This is not coincidence. This is neuroscience responding to structured, loving intervention — delivered by you, at your kitchen table, on days when you weren't sure it was working.
Show Their New Skill
Let your child demonstrate what they can do to a grandparent, sibling, or close friend. Social witness amplifies the child's pride exponentially.
Create a "Brave Hands" Certificate
Write their name, the date, and exactly what they can do now. Frame it. This is a neurological achievement worth documenting.
Take a Photo
Document your child interacting with a material they couldn't touch 8 weeks ago. This is the before-and-after of the nervous system learning safety.
Share with Your Therapist
Bring the data and the moment to your next OT session. They will celebrate with you — and they will know exactly what milestone this represents clinically.
Your child grew because of your commitment. The science made the map. You walked the road with them, every single session.

Red Flags — When to Pause
Home-based protocols are powerful — and they have limits. Knowing when to pause and seek professional input is not a sign of failure. It is the most responsible parenting decision you can make. Trust your instincts.
🚨 Regression Over 2+ Weeks
Tolerance is decreasing despite consistent protocol. The technique may need professional recalibration — not just more repetition of what isn't working.
🚨 Self-Harm in Response to Touch
Child biting, hitting, or scratching themselves after tactile exposure. This exceeds home protocol scope and requires immediate professional evaluation.
🚨 Generalized Anxiety Spreading
Child becomes anxious about ALL activities, not just tactile ones. The sensory work may be triggering broader anxiety that requires additional clinical support.
🚨 Physical Symptoms
Pain reports at touch sites, redness, swelling, or skin reactions. Rule out medical causes — neuropathy, dermatological conditions — before continuing.
🚨 Sudden Complete Refusal
Child who was progressing suddenly refuses all sessions. Explore what changed: new school stress, illness, caregiver change. Something shifted in their environment.
🚨 New Onset — Sudden Appearance
Tactile defensiveness appearing SUDDENLY in a child who previously tolerated textures. This warrants medical evaluation before sensory intervention begins.
1
Self-Adjust Protocol
2
Teleconsult with OT
3
In-Clinic Evaluation
4
Comprehensive Sensory Profile
The Progression Pathway
A-008 is one stop on a carefully mapped developmental journey. Knowing where you've been, where you are, and where this technique leads helps you see the larger therapeutic arc — not just the individual session.
Your Position: A-008
Tactile Desensitization
A-001 (Prerequisite)
Touch Sensitivity — General Introduction
★ A-008 (HERE)
Tactile Desensitization — Slime/Texture Aversion — 7-Phase Internal Progression
A-009 (Next)
Can't Stand Clothing Tags / Fabric Sensitivity
A-010
Grooming Difficulties — Hair, Nails, Face
A-012
Food Texture Aversions — Oral Tactile
The 7-Phase Internal Progression of A-008
Phase 1 — Dry & Predictable
Rice, Beans — zero sticky factor
Phase 2 — Moldable & Non-Sticky
Theraputty, Kinetic Sand
Phase 3 — Wet & Smooth
Water Beads
Phase 4 — Wet & Light Messy
Shaving Cream
Phase 5 — Barrier-Protected
Paint Bags, Gloves
Phase 6 — Edible & Safe
Pudding, Whipped Cream
Phase 7 — Direct Sticky Contact 🏆
Finger Paint, Playdough, Slime
Related Techniques in the Tactile Domain
The materials you've gathered for A-008 are the same materials that power four other techniques in the Tactile Defensiveness series. You're already better equipped than you think.
A-007 — Seeks Messy Play (Opposite Pattern)
For children who crave intense tactile input. Opposite end of the sensory spectrum but overlapping materials. Materials you already own: Dry Sensory Bins, Kinetic Sand.
⚪ Intro Level
A-008 — Won't Touch Slime ★ THIS PAGE
Core tactile desensitization protocol. All 9 materials. The foundational technique for the entire tactile sensitivity domain.
🟡 Core Level
A-009 — Clothing Tag & Fabric Sensitivity
Extends tactile work to clothing and fabric. Primary material overlap: Tactile Brushes. A natural next step after A-008 gains are consolidated.
🟡 Core Level
A-010 — Grooming Difficulties
Hair brushing, nail cutting, face washing. Material overlap: Theraputty, Tactile Brushes. Self-care independence is the goal.
🟡 Core Level
A-011 — Avoids Being Touched Socially
Social touch aversion — hugs, handshakes, crowded environments. Advanced protocol requiring clinical supervision.
🔴 Advanced
A-012 — Food Texture Aversions
Oral tactile defensiveness linked to feeding difficulties. Material overlap: Edible Sensory Play. Gains in hand-based tolerance often transfer here.
🔴 Advanced
You already own materials for 4 of these 6 techniques — the investment you made for A-008 extends far beyond this one protocol.
Your Child's Full Developmental Map
Tactile desensitization is one piece of a much larger developmental picture. Understanding how Domain A connects to every other domain in your child's profile helps you see the full impact of the work you're doing today.
Domain A → Domain F
Fine motor development through material manipulation — hand strength, coordination, bilateral hand use
Domain A → Domain H
Daily living skills — self-care tolerance for grooming, hygiene, food preparation
Domain A → Domain J
Play participation — joining peers in messy play, art, birthday activities, school crafts
Domain A → Domain C
Social engagement through shared sensory play — the tactile world is where childhood friendships are built
This technique is one piece of a larger plan. GPT-OS® connects all 12 domains into your child's personalized developmental pathway.

Families Who've Been Here
Progress is not always linear. It is not always Instagram-worthy. And it often happens in the quietest moments — an approach without crying, a second of contact without wiping, a hand that didn't wash itself after breakfast. These are real families who know exactly where you're standing right now.
Family 1 — Before & After
"He used to scream at the sight of finger paint. The preschool teacher would call us to pick him up every art day."
After: "We started with dry rice. Used bags and gloves. Slowly built up. It took a year, but he plays in the sensory bin now. He asked for playdough for his birthday."
— Parent, Pinnacle Network
Family 2 — Before & After
"She washed her hands 30–40 times a day. Her skin was raw. She wouldn't hug anyone because she couldn't predict what their hands would feel like."
After: "After 6 months of the graduated protocol, hand-washing dropped to 8–10 times. She tolerates shaving cream. She hugged her grandmother voluntarily for the first time."
— Parent, Pinnacle Therapy Center
"Tactile desensitization is a marathon, not a sprint. The families who succeed are the ones who celebrate the micro-victories — the 2-second touch, the approach without crying, the day they didn't wash their hands after breakfast. Those tiny moments are neural pathways forming." — Pinnacle Therapist
Note: Illustrative cases representing composite outcomes. Individual results vary by child profile and severity.

Connect with Other Parents
The protocol is most powerful when you're not running it alone. Other parents who have walked this road — who know what it feels like at 2am to doubt everything — are your most valuable resource alongside the clinical team.
Tactile Defensiveness Parent Community
Connect with families running the same protocol. Share wins. Ask questions. Get encouragement at 2am when you're doubting everything. Real parents, real data, real progress stories.
Pinnacle Parent Community Forum
Topic threads for each of the 9 materials. Real parent photos and videos of their child's progression at each phase. Searchable by child age and material type.
Peer Mentoring Program
Connect with an experienced parent who has completed the A-008 protocol. They've been where you are. They'll tell you it gets better — and they'll mean it.
Local Parent Support Groups
Find your nearest Pinnacle center and join the monthly parent support group. In-person connection with families who understand without explanation.
Your experience helps others. The parent you are today is the peer mentor another family needs six months from now. Consider sharing your journey.
Your Professional Support Team
Home practice amplifies clinical work. Clinical expertise shapes home practice. The two work together — and the combination produces outcomes neither can achieve alone.
🗺️ Pinnacle Center Locator
70+ centers across the country. Find your nearest occupational therapist specializing in sensory integration — including Wilbarger Protocol training.
👩⚕️ Therapist Matching
Get matched with an OT who specializes in tactile defensiveness. They'll supervise your home protocol, review your data, and calibrate progression timing for your specific child.
📱 Teleconsultation
Can't visit a center? Book a video consultation with a Pinnacle OT. Review your session data, adjust your protocol, and receive personalized guidance — from anywhere.
📞 FREE National Helpline
Call or email for guidance in 18+ languages. No referral needed. No waitlist for initial contact. Expert triage to the right resource for your child's needs.
Home + Clinic = Maximum Impact
Research consistently shows that parent-implemented home protocols, supervised by a qualified clinician, produce the strongest and most durable outcomes in pediatric sensory intervention.
Contact Pinnacle
📞 National Helpline (18+ languages)
📧 care@pinnacleblooms.org
The Research Library
Every technique on this platform is grounded in peer-reviewed research. Here is the full evidence base behind A-008 — with direct references for parents who want to go deeper, and for clinicians who need to cite sources in clinical documentation.
PRISMA Systematic Review (2024)
16 articles confirm SI intervention as evidence-based for ASD. PubMed: PMC11506176
Meta-Analysis, World J Clinical Cases (2024)
SI therapy promotes social skills, adaptive behavior, sensory processing, and motor skills across 24 studies. PMC10955541 | DOI: 10.12998/wjcc.v12.i7.1260
Padmanabha et al. RCT (2019)
Home-based sensory interventions demonstrate significant outcomes in pediatric population. DOI: 10.1007/s12098-018-2747-4 | Indian Journal of Pediatrics
WHO Nurturing Care Framework (2018)
Global framework for early childhood development including sensory-responsive caregiving. nurturing-care.org/ncf-for-ecd
WHO CCD Package Implementation (2023)
Caregiver-mediated interventions validated across 54 countries. PubMed: PMC9978394
Foundational Texts for Deeper Reading
- Ayres, A.J. — Sensory Integration and the Child (1979, revised 2005)
- Wilbarger, P. & Wilbarger, J. — Sensory Defensiveness in Children (1991)
- Miller, L.J. — Sensational Kids (2006)
- Dunn, W. — The Sensory Profile Assessment (1999)

How GPT-OS® Uses Your Data
Every data point you record after a session becomes part of your child's personalized clinical profile — and contributes to a growing population database that makes the protocol smarter for every family that comes after you.
What GPT-OS® Learns from Your Sessions
- Which materials your child responds to best (personalizes material sequencing)
- Optimal session duration and frequency for your child specifically
- Distress patterns that predict readiness for progression
- Cross-domain connections (tactile improvement predicting feeding gains)
Privacy & Data Protection
- Your child's data is encrypted and anonymized in population analytics
- Individual data accessible ONLY to you and your authorized clinical team
- Compliant with US HIPAA provisions and applicable data protection law
- ISO/IEC 27001 certified information security
20M+
Therapy Sessions
Feeding GPT-OS® algorithms across the Pinnacle network
97%+
Measured Improvement
Across families who complete the full protocol with consistent data collection
Your data helps every child like yours. The population insights from your sessions today become the personalized recommendations for the family starting their A-008 journey tomorrow.

Watch the Reel — A-008 in Action
A-008 Visual Guide
Sensory Solutions — Episode 008
Reading about materials is one thing. Seeing a trained Pinnacle occupational therapist demonstrate each of the 9 materials — showing what they look like, how to present them, and what child engagement looks like at each stage — is another entirely. This 60-second reel is the visual companion to everything you've read on this page.
🎬 What You'll See
A Pinnacle OT walks through all 9 materials in sequence — correct presentation technique, what distance to start from, how to read the child's response, and what breakthrough engagement looks like.
📱 How to Use It
Watch once before your first session to orient yourself. Watch the relevant material segment before each new material introduction. Share with family members and caregivers who need the visual protocol.
🎓 Why Video Works
Video modeling is classified as evidence-based practice for autism (NCAEP, 2020). Multi-modal learning (visual + text + demonstration) improves parent skill acquisition and session fidelity.
Series: Sensory Solutions | Domain: Tactile Defensiveness — Touch Over-Responsivity | Technique ID: A-008 | Produced by the Pinnacle Blooms Clinical Media Team
Share This with Your Family
Consistency across caregivers multiplies the impact of every session you run. When grandparents understand, when teachers accommodate, when the whole household speaks the same language — your child's nervous system gets to practice safety everywhere, not just at the kitchen table.
Share via WhatsApp
Pre-formatted message with page link — ready to send to family members in seconds
Share via Email
Page link with full summary — appropriate for teachers, school counselors, and extended family
Download Family Guide
1-page simplified A-008 protocol summary. Print-friendly. Fridge-door ready. All 6 steps on one page.
👵 "Explain to Grandparents" Version
"[Child's name]'s brain processes touch differently. When slime or sticky things touch their skin, their brain sends a 'danger' signal — like how some people can't stand nails on a chalkboard, except it happens with every sticky texture. We're using special materials to slowly teach their brain that these textures are safe. Here's how you can help: don't force them to touch things, praise any voluntary touch, and keep wipes nearby."
👩🏫 Teacher and School Communication Template
An adaptable letter template requesting IEP accommodations for tactile defensiveness during art, sensory play, and craft activities — citing the neurological basis and specific classroom accommodations that support your child's participation and safety.

Frequently Asked Questions
The questions parents ask most often — answered with the same clinical honesty and warmth that grounds every technique on this platform.
Q: How long until I see results?
Expect 2–4 weeks for observable tolerance changes with consistent 3–5 sessions per week. Mastery of each texture phase typically takes 5–8 weeks. The full 7-phase progression may take 6–12 months. Your child's pace is the right pace — not the average pace.
Q: Can I do this without an OT?
The graduated material exposure protocol (8 of the 9 materials) can be safely implemented at home following this guide. The Wilbarger Protocol (tactile brushing) MUST be taught by a trained OT. If unsure, start with dry sensory bins — they are the safest starting point by a wide margin.
Q: My child has texture issues with food too. Is that related?
Yes. Oral tactile defensiveness (food texture aversion) is part of the same neurological pattern. See technique A-012 for the feeding-specific protocol. Gains in hand-based texture tolerance often transfer to oral tolerance — but not automatically or immediately.
Q: Is this just for autism?
No. Tactile defensiveness occurs in children with autism, sensory processing disorder, ADHD, anxiety disorders, premature birth, and sometimes with no other diagnosis. The protocol works regardless of the underlying condition because it targets the neurological mechanism, not the diagnosis.
Q: What if my spouse or family doesn't believe this is real?
Share Card 03 (the neuroscience). Show them the PubMed references on Card 34. The evidence base for tactile defensiveness as a neurological difference — not a behavioral choice — is robust, peer-reviewed, and internationally endorsed.
Q: Can I use multiple materials in one session?
In early stages, use ONE material per session for clarity and to isolate the neurological learning. As the child progresses, you can introduce a second material at a lower difficulty level. Never introduce two new materials in the same session.
Q: My child is 8–10. Is it too late?
No. Neural plasticity continues throughout childhood and beyond. Older children often progress faster because they can understand the rationale and participate in goal-setting. The protocol adapts fully for ages 2–10 — older children just get a different vocabulary.
Q: Where can I buy these materials?
Amazon.com, local OT supply shops, or DIY with household ingredients (see Card 10). Each of the 9 materials has a dedicated page at materials.pinnacleblooms.org with direct purchase links and DIY recipes.

Your Next Step — Start Now
You have everything you need.
You understand the neuroscience. You know the 9 materials and how to sequence them. You have the 6-step protocol, the safety rules, the troubleshooting guide, and the data tracking system. Your child's nervous system is ready to learn. And you are ready to teach it.
🟢 Start This Technique Today
Launch a GPT-OS® guided first session. The system will select your starting material, set your session timer, and walk you through all 6 steps with real-time guidance.
📞 Book a Consultation
Connect with a Pinnacle OT for personalized protocol design, Wilbarger brushing training, or a comprehensive sensory evaluation. In-clinic or teleconsult available.
🔄 Explore the Next Technique
A-009: 9 Materials That Help When Child Can't Stand Clothing Tags — the natural next step for most families completing A-008.
✅ OT Validated
✅ SLP Validated
✅ ABA Validated
✅ SpEd Validated
✅ NeuroDev Validated
✅ CRO Validated
Preview of 9 materials that help when child wont touch slime Therapy Material
Below is a visual preview of 9 materials that help when child wont touch slime therapy material. The pages shown help educators, therapists, and caregivers understand the structure and content of the resource before use. Materials should be used under appropriate professional guidance.











Link copied!

The Pinnacle Promise
OT
SLP
BCBA
Special Educator
NeuroDev Pediatrician
Clinical Research
From fear to mastery. One technique at a time.
You arrived on this page scared, confused, and exhausted — wondering if it would ever get better. You now understand the neuroscience of what your child experiences. You have the materials, the protocol, the troubleshooting guide, and a community of families beside you. Your child's nervous system is capable of learning. And you are now equipped to teach it — one patient, consistent, child-led session at a time.
🔝 Return to Top
Card 01 — The Recognition Moment
🔄 Next Technique
A-009: Clothing Tag & Fabric Sensitivity
🗂️ Browse All Techniques
techniques.pinnacleblooms.org
🏠 Pinnacle Home
pinnacleblooms.org
20M+
Exclusive 1:1 Sessions
97%+
Measured Improvement
70+
Centers Nationwide
160+
Countries with Patents Filed
Medical Disclaimer: This content is educational and does not replace assessment by a licensed occupational therapist. Tactile defensiveness and sensory processing differences benefit from professional evaluation. If your child's tactile sensitivity significantly impacts daily functioning, consult a qualified professional. Individual results vary. The Wilbarger Protocol must be administered under trained OT supervision.
© 2026 Pinnacle Blooms Network®. All rights reserved. Content developed by the Pinnacle Blooms Consortium — a multidisciplinary expert body combining Clinical Research, Pediatric OT, SLP, ABA, Special Education, and NeuroDevelopmental Medicine. Powered by GPT-OS® Therapeutic Intelligence.
ISO 13485 Medical Device QMS | ISO/IEC 27001 Information Security | DPIIT Recognized
techniques.pinnacleblooms.org/sensory/tactile-desensitization-slime-texture-aversion