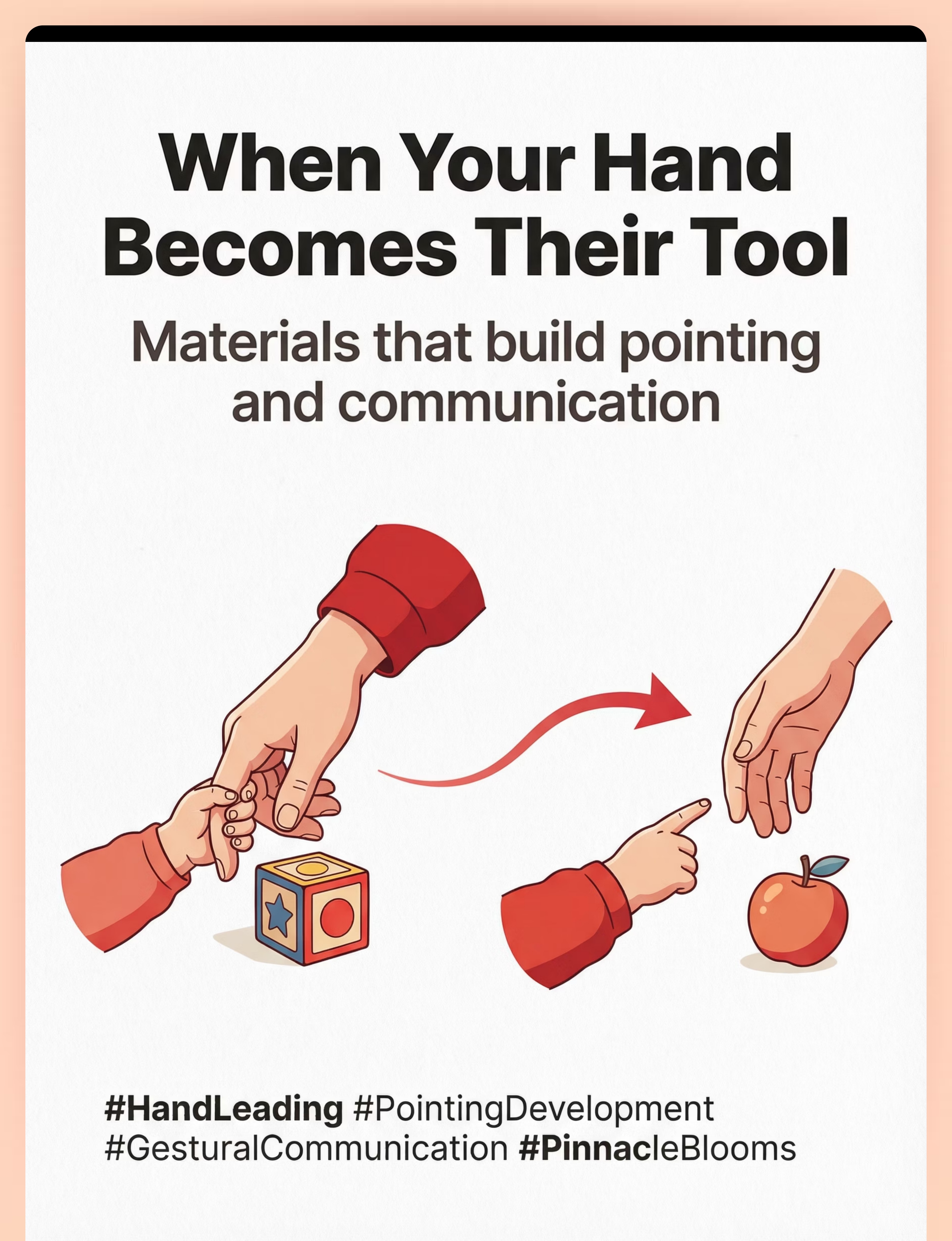
She Doesn't Point. She Grabs My Hand.
When your child wants something, they don't point or ask — they take your hand and place it on the object. Like you're a tool, not a person they're communicating with. You've noticed this. And noticing is where transformation begins.
"When she wants something, she doesn't point or ask — she grabs my hand and puts it on the object. Like I'm a tool, not a person she's communicating with."
Domain: Joint Attention & Gestural Communication
Ages: 12–48 months
Technique: B-132
Series: Communication Differences — Episode 132

This Is One of the Most Common Early Signs Parents Notice
Hand-leading — using an adult's hand as a tool instead of pointing or using gestures — is reported by families in every country, every culture, every socioeconomic background. Research published in the Journal of Autism and Developmental Disorders identifies absent or reduced pointing as one of the earliest observable markers of autism spectrum differences, typically noticeable between 12–18 months.
You are not failing. Your child has found a way to get needs met. They are communicating — just through a different route. And that route can be redirected toward conventional communication.
80%
Joint Attention Differences
Present in children later diagnosed with ASD (Mundy & Newell, 2007)
9–12mo
Pointing Emerges
Protodeclarative pointing by 12–14 months (Baron-Cohen, 1989)
8–12wk
Measurable Gains
Early intervention for gestural communication shows significant improvement (WHO NCF, 2018)
"Across 70+ Pinnacle Blooms centers, hand-leading is one of the top 5 concerns parents report at first consultation. You've already taken the most important step — you noticed."

Why Your Child Uses Your Hand Instead of Pointing
In typical development, a child learns three deeply interconnected things by age 12 months. When a child uses your hand as a tool, they may not yet fully grasp that you are a separate person with your own perspective who can be communicated with. Your hand is simply the most efficient reaching device they know. This is not a rejection of you — it is a developmental difference in understanding agency and communication.
1
Self–Other Distinction
"I am a separate person from you" — sense of self and other
2
Shared Attention
"You can see what I see" — shared attention and theory of mind foundations
3
Communicative Intent
"If I point, you'll look — and that means something" — gestures carry meaning
Hand-leading is positioned at the junction between concepts one and two. Baron-Cohen (1989), Tomasello et al. (2007), and Mundy & Newell (2007) all confirm this as a well-documented developmental pathway — one that responds powerfully to structured intervention.
The Pointing Development Timeline
Pointing isn't one skill — it's a developmental cascade. Understanding where your child is on this timeline helps you meet them exactly where they are, without skipping steps or expecting mastery before the foundation is ready.
1
6–9 Months
Reaching toward desired objects — the motor foundation for all future gesturing
2
9–12 Months
Protoimperative pointing emerges — pointing to REQUEST ("I want that")
3
12–14 Months
Protodeclarative pointing emerges — pointing to SHARE INTEREST ("Look at that!")
4
12–18 Months
Consistently following where others point — joint attention becomes bidirectional
5
18+ Months
Pointing integrated with vocalization and emerging speech — communication expands
"Hand-leading typically occurs when a child has the motor ability to reach but hasn't yet connected that gestures — like pointing — can communicate meaning to another person. The motor pathway is present. The communicative bridge needs building."

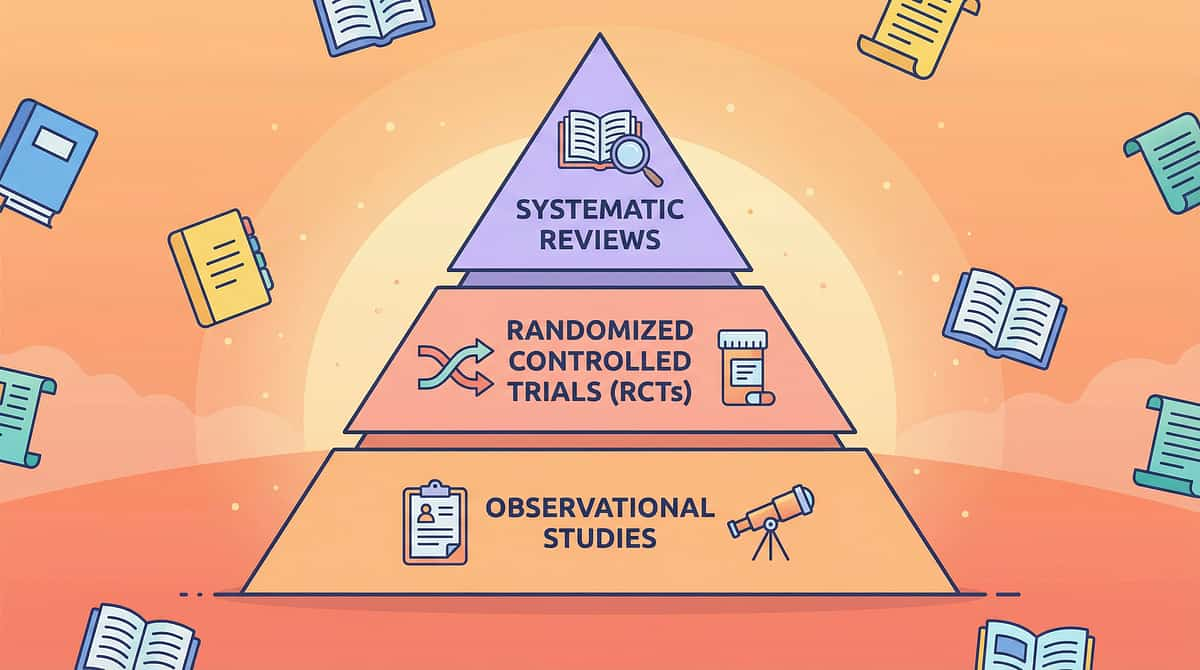
Clinically Validated. Home-Applicable. Parent-Proven.
Evidence Grade: Level II — Multiple Controlled Studies
The research is clear: gestural communication — including pointing — can be developed through structured intervention, and parents are among the most effective intervention agents when properly guided. Four landmark findings anchor the evidence base for this technique.
Finding 1 — PRISMA Systematic Review (2024)
A review across 16 studies (2013–2023) confirms structured communication intervention meets criteria for evidence-based practice. (PMC11506176)
Finding 2 — Parent-Mediated Interventions
Parent-delivered joint attention interventions show effect sizes comparable to clinician-delivered services, with superior generalization to natural environments. (PMC10955541)
Finding 3 — WHO/UNICEF CCD Package
Home-based, caregiver-delivered developmental interventions across 54 countries produce measurable communication gains. (PMC9978394)
Finding 4 — Indian Pediatric RCT
Padmanabha et al. (2019) demonstrated significant outcomes from home-based structured interventions. (DOI: 10.1007/s12098-018-2747-4)
At Pinnacle Blooms Network, across 20M+ therapy sessions, 97%+ of children show measurable improvement on standardized communication readiness indexes.
Communication Temptation & Pointing Development Protocol
Parent-Friendly Name: "Building Pointing Through Motivation"
This technique uses environmental arrangement, motivating materials, and structured communication opportunities to transition a child from hand-leading to conventional gestural communication — pointing, reaching toward the person, and eye contact during requests. Instead of physically manipulating the adult, the child learns that communicating with the adult is more effective, faster, and more rewarding.
Technique Specifications
Domain: B — Behavioral/Developmental
Sub-Domain: Joint Attention & Gestural Communication
Ages: 12–48 months
Duration: 10–15 minutes
Frequency: Multiple times daily
Setting: Home & Therapy
Lead Discipline: Speech-Language Pathology
Sub-Domain: Joint Attention & Gestural Communication
Ages: 12–48 months
Duration: 10–15 minutes
Frequency: Multiple times daily
Setting: Home & Therapy
Lead Discipline: Speech-Language Pathology
Canon Materials Covered
- Communication Boards & Visual Supports
- Cause-and-Effect Toys
- Picture Books & Literacy Materials
- Bubbles & Motivating Activities
- AAC Devices & Communication Apps
- Fine Motor & Sensory Materials

Your Child's Entire Team Uses This — Here's How
This technique crosses therapy boundaries because the brain doesn't organize itself by therapy type. Pointing development involves communication, motor control, social cognition, and behavioral learning — all at once. Each discipline contributes a unique lens.
Speech-Language Pathologist (SLP) — Primary Lead
Designs the communication temptation hierarchy. Targets pointing as a pre-linguistic gesture. Shapes hand-leading toward conventional requesting. Introduces AAC if appropriate.
BCBA / ABA Therapist
Structures reinforcement contingencies. When pointing produces better outcomes than hand-leading, pointing increases. Designs discrete trial and natural environment teaching protocols.
Occupational Therapist (OT)
Addresses finger isolation — the motor prerequisite for pointing. If the child can't isolate their index finger, pointing is physically difficult. Develops fine motor foundations.
Special Educator (SpEd)
Integrates pointing practice into learning activities. Uses visual supports and structured choice-making. Generalizes communication gains to classroom contexts.
NeuroDevelopmental Pediatrician
Evaluates whether hand-leading reflects a broader developmental profile. Rules out motor, neurological, or sensory contributions. Monitors trajectory across all domains.
At Pinnacle Blooms, the FusionModule™ coordinates all five disciplines into one converged therapeutic pathway — so your child's pointing development is addressed from every angle, in every session.
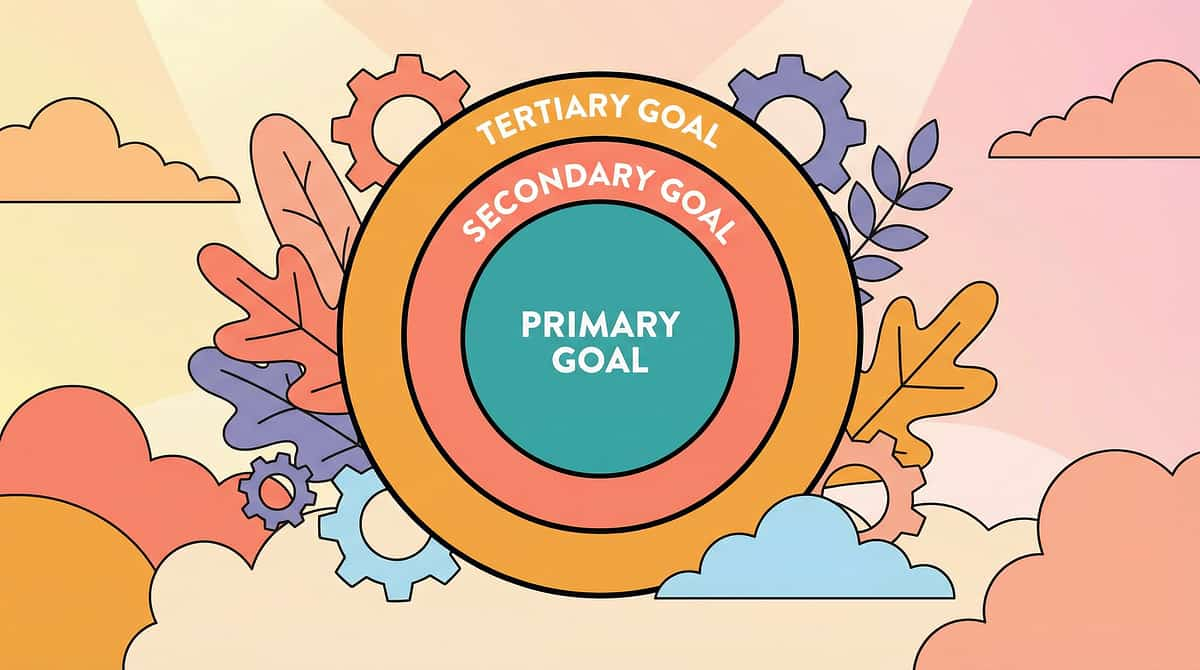
Precision Targets — This Isn't a Random Activity
Every exchange in this technique is aimed at measurable, observable communication milestones. The bullseye structure below shows how primary, secondary, and tertiary targets layer on top of each other to build a complete communication foundation.
🎯 Primary Target
Transition from hand-leading to pointing, reaching toward the person, and gaze-shifting during requests
Secondary Targets
Joint attention, communicative intent, self-other distinction — the scaffolding around the primary skill
Tertiary Targets
Pre-linguistic foundation, social cognition, motor planning for gestures, requesting and protesting skills
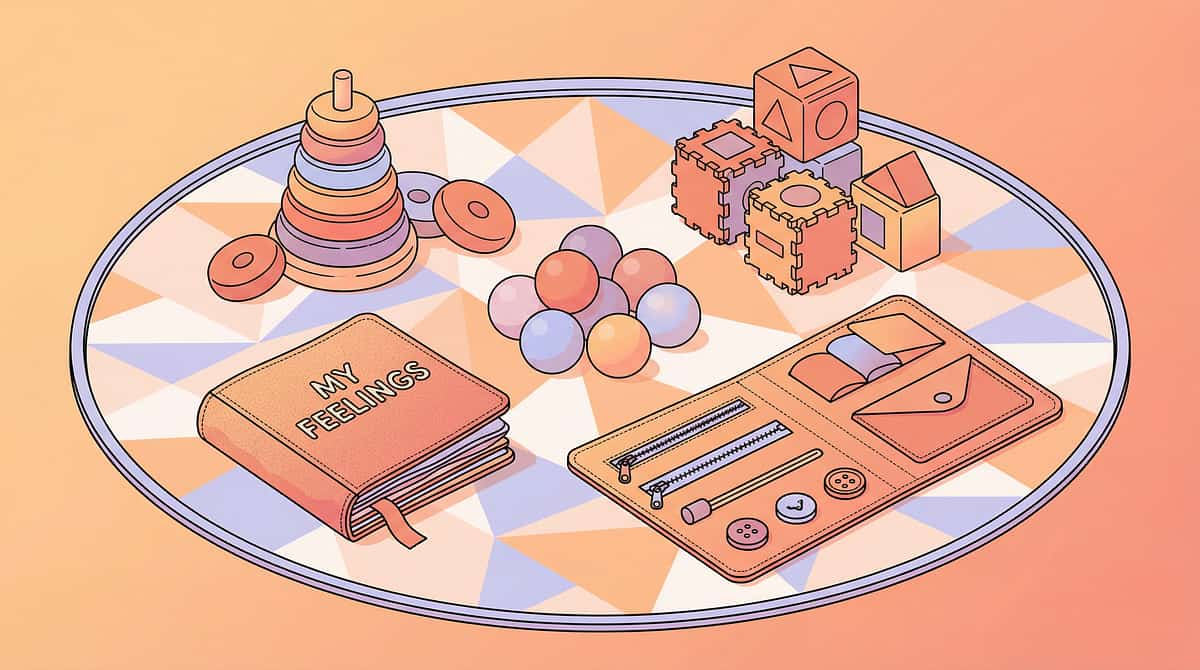
Your 9-Material Communication Building Kit
Everything you need, mapped to the Pinnacle 128 Canon Materials system. Each material serves a specific function in building pointing and communication. You don't need all 9 — start with the ⭐ Essentials listed below.
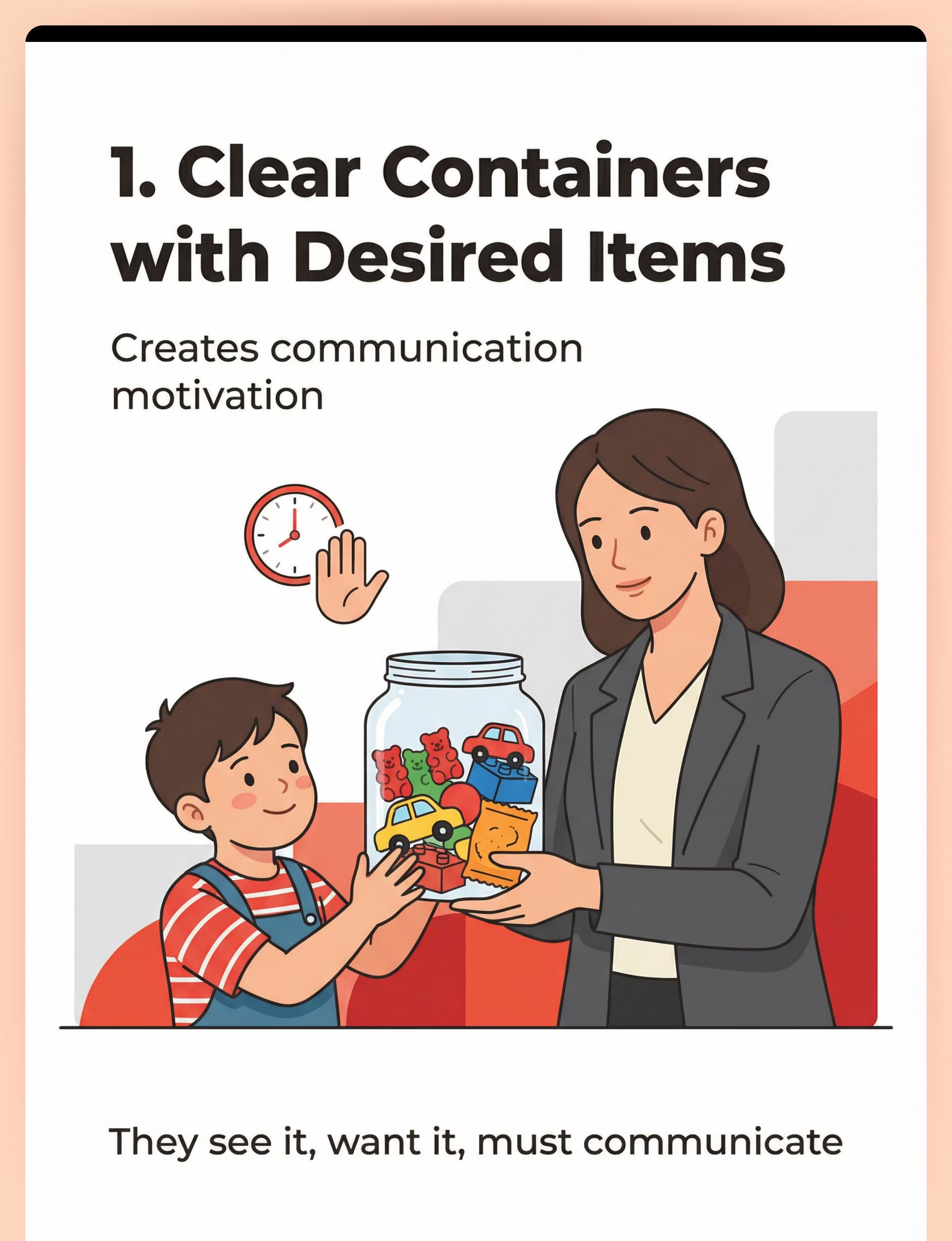
1
⭐ Clear Containers With Desired Items
Canon Category: Environmental Arrangement Tools
Function: Creates communication motivation — child sees desired item, can't access independently, must communicate to get it
Function: Creates communication motivation — child sees desired item, can't access independently, must communicate to get it
2
⭐ Choice Boards & Visual Supports
Canon Category: Communication Boards & Visual Supports
Function: Gives pointing a clear, functional target — point to picture, get the item
Function: Gives pointing a clear, functional target — point to picture, get the item
3
Pointing Practice Toys (Cause-and-Effect)
Canon Category: Cause-and-Effect Toys
Function: Makes pointing powerful and fun — press a button, something exciting happens
Function: Makes pointing powerful and fun — press a button, something exciting happens
4
Picture Books for Joint Attention
Canon Category: Books & Literacy Materials
Function: Natural context for shared pointing — "Look at the dog! Point to the dog!"
Function: Natural context for shared pointing — "Look at the dog! Point to the dog!"
5
⭐ Bubbles & Motivating Activities
Canon Category: Bubbles & Sensory Play
Function: Repositions adult from "tool" to "source of wonderful things"
Function: Repositions adult from "tool" to "source of wonderful things"
6
Reaching & Requesting Objects
Canon Category: Child's Existing Preferred Items (Cost: ₹0)
Function: Creates reaching-toward-person opportunities using what you already own
Function: Creates reaching-toward-person opportunities using what you already own
7
Social Games & Routines
Canon Category: No Materials Required (Cost: ₹0)
Function: Teaches people are partners, not tools — connection without objects
Function: Teaches people are partners, not tools — connection without objects
8
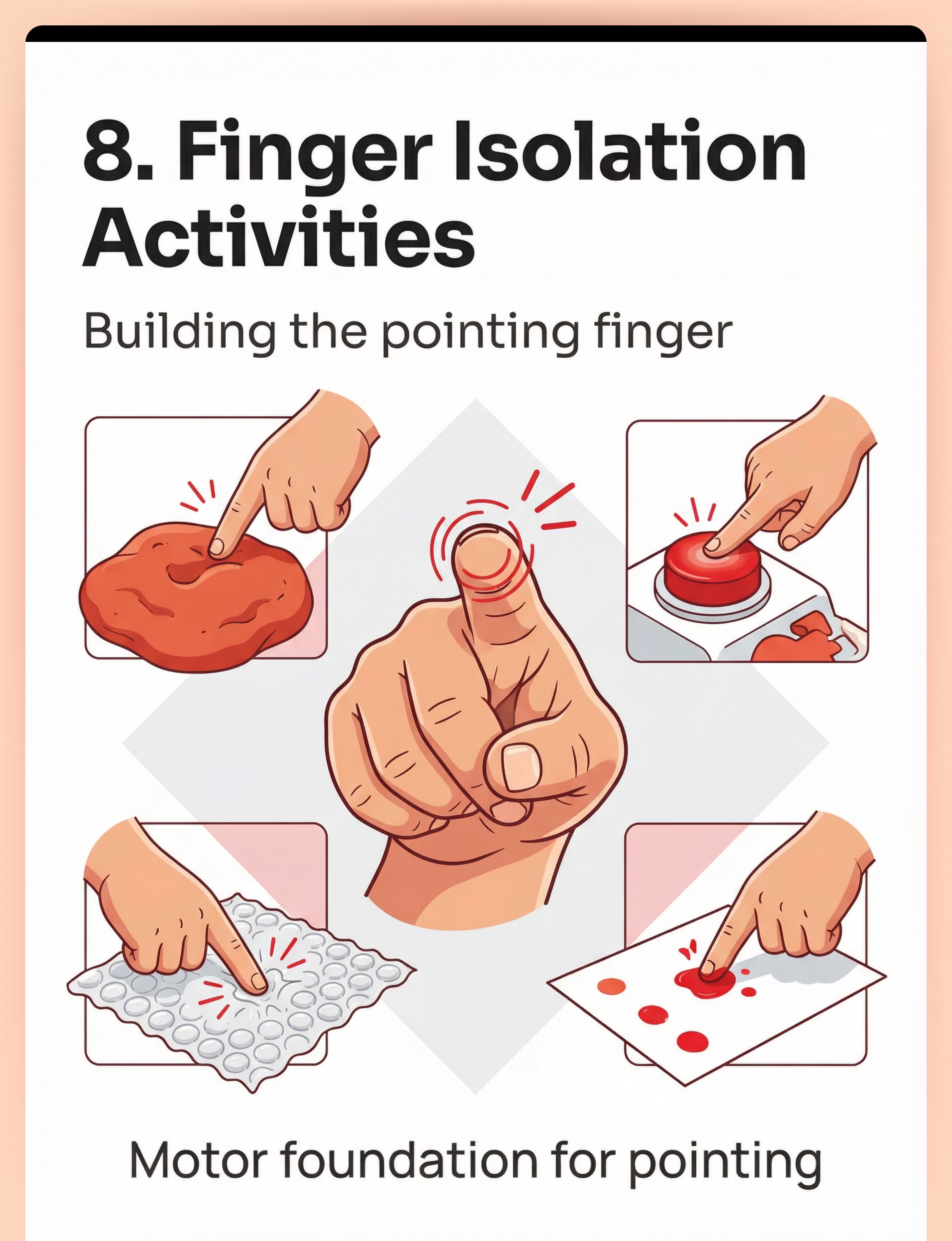
Finger Isolation Activities
Canon Category: Fine Motor Materials / Playdough & Sensory
Function: Builds the motor foundation for the pointing gesture itself
Function: Builds the motor foundation for the pointing gesture itself
9
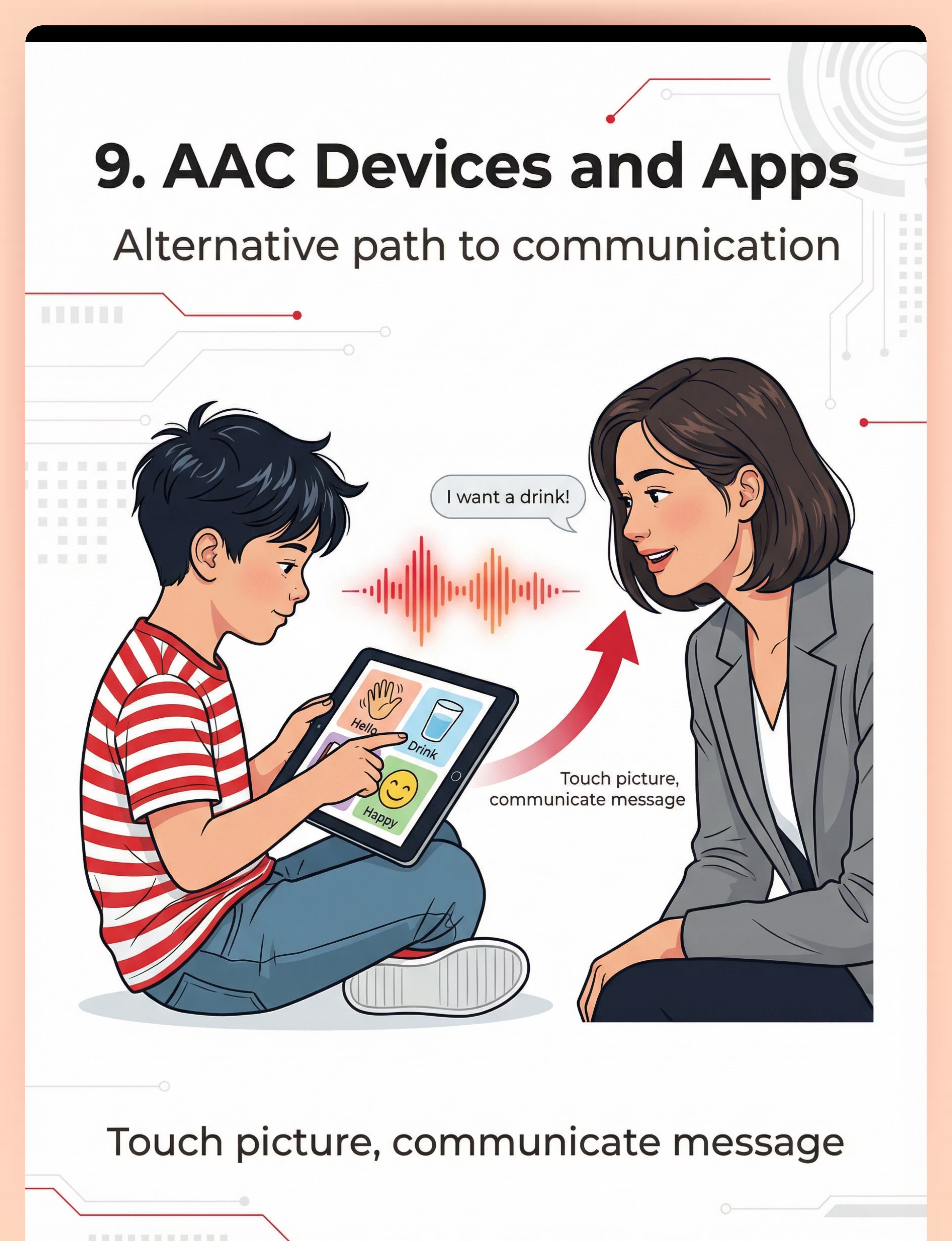
AAC Devices & Communication Apps
Canon Category: AAC & Assistive Communication
Function: Alternative communication pathway when gestural development needs additional support
Function: Alternative communication pathway when gestural development needs additional support
Total Investment: ₹550–₹9,800+ for comprehensive setup (many items free/DIY). Essential starters (marked ⭐): Under ₹1,000. Browse the full Canon Materials library at materials.pinnacleblooms.org

Zero-Cost Versions — Start Today With What You Have
Not every family can order from Amazon. Not every village has same-day delivery. The WHO/UNICEF Nurturing Care Framework emphasizes equity-focused, context-specific interventions. Most of these materials can be created from household items — and work just as well for building pointing and communication.
Buy: Clear Container Set
Make it: Any transparent jar, plastic container, or zip-lock bag the child can see through but can't open. Mason jars, old spice containers, clear pencil cases all work perfectly.
Buy: Choice Board
Make it: Print photos of 2–3 favorite items on paper. Laminate with tape. Mount on cardboard. Use actual photos from your phone — printed at any shop for ₹5 each.
Buy: Pointing Practice Toys
Make it: Any toy with buttons: old TV remote (batteries removed), doorbell, light switches, musical greeting cards. Point/press → something happens.
Buy: Picture Books
Make it: Homemade photo album of family, pets, food, and favorite toys. Staple together. The best pointing books star people and things your child already loves.
Buy: Bubbles
Make it: 1 cup water + 2 tablespoons dish soap + 1 tablespoon glycerin (or sugar). Wire loop from any household wire. Works perfectly — often better than store-bought.
Buy: Finger Isolation Materials
Make it: Playdough (2 cups flour + 1 cup salt + water). Bubble wrap from any delivery package. Pudding or yogurt for finger painting. Stickers for peeling practice.
⚠️When clinical-grade is non-negotiable: If your child's SLP recommends a specific AAC device or system, the professional-grade version may be necessary. Always follow your therapist's guidance for AAC selection.

Safety Gate — Read This Before Your First Session
Before beginning any home-based communication practice, run through this traffic-light safety framework. Your child's emotional safety and your own regulated state are prerequisites — not afterthoughts.
🟢 GREEN — Proceed When:
- Child is calm, alert, and fed (not hungry, tired, or overstimulated)
- Environment is quiet with minimal distractions
- You have 10–15 minutes of uninterrupted time
- Motivating items are prepared and within YOUR reach (not child's)
- You feel patient and calm — your emotional state matters
🟡 AMBER — Modify When:
- Child is mildly fussy — shorten session to 3–5 minutes
- Child shows mild resistance — use higher-value motivators
- Child has had a difficult day — prioritize connection over targets
- You're feeling frustrated — take a break, return later
🔴 RED — Stop Immediately If:
- Child is in distress, crying, or showing signs of meltdown
- Child is ill, in pain, or recovering from a medical procedure
- You are withholding necessities — NEVER use food, water, or comfort as temptation
- Child shows aggression toward self or others
- Frustration escalates beyond 30 seconds of de-escalation
Material Safety: All containers must be shatterproof. Small items must be larger than a toilet paper tube diameter (choking prevention). Bubbles: non-toxic only, keep away from eyes. Balloons require constant adult supervision. Stop immediately if you see prolonged crying (>2 min), self-injurious behavior, complete shutdown, or physical distress. Call 1800-123-7838 for guidance.
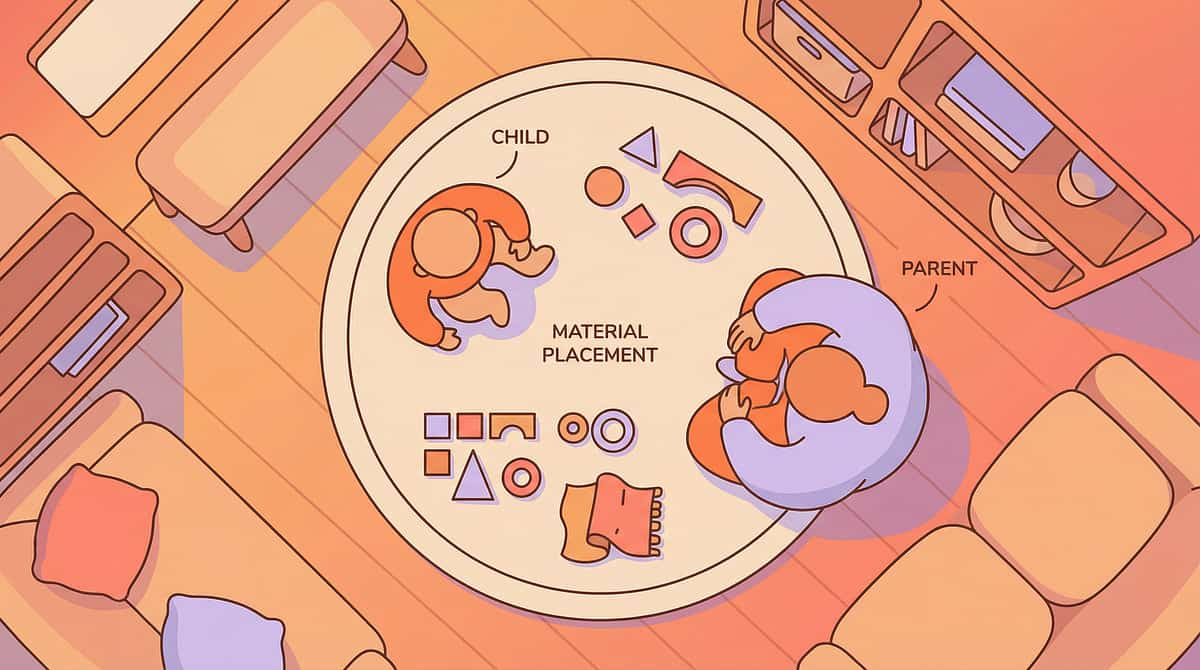
Your Home Communication Therapy Zone
You don't need a therapy room. You need a communication-rich corner of any room you already use. The physical setup is part of the intervention — it's not just preparation, it's practice.
The Communication Zone
A 2m × 2m space is plenty. Use floor-level seating so you and your child are face-to-face, at eye level. Ensure clear sight lines — child can see your face, your hands, and the motivating items. Natural light preferred so facial expressions are visible. TV off, phone silenced.
Time Recommendation
Dedicated practice: 10–15 min, 2–3× daily
Naturalistic embedding: Every meal, every play session, every transition
Daily target: 30+ embedded communication opportunities
Naturalistic embedding: Every meal, every play session, every transition
Daily target: 30+ embedded communication opportunities
Material Positioning — Critical
- Motivating items: Within YOUR reach, OUT OF child's reach (high shelf, clear container, your closed hand)
- Choice boards: Between you and child, at child's eye level
- Bubbles/toys: Ready but not yet activated — YOU control when the fun begins
What to Remove
- Free-access toys (no motivation to communicate if items are always available)
- Screens (compete for attention)
- Siblings during dedicated practice (involve them later for generalization)

Before You Begin — Quick Readiness Check
Run through this checklist before every session. It takes 60 seconds and dramatically improves outcomes. A fully prepared parent in a fully prepared space is itself a therapeutic variable.
Child is calm, alert, and not hungry or tired
Space is set up with motivating items out of child's reach
You have 10–15 minutes of uninterrupted time
Your phone is silenced and face-down
You've identified 2–3 highly motivating items for this session
You're emotionally ready — patient, warm, and playful
Safety checklist completed (no choking hazards, shatterproof containers)
"I am not drilling my child. I am creating opportunities for communication. Every look, every reach, every sound my child makes toward me is progress. I will celebrate approximations. I will not force. I will wait, model, and respond."

Step 1 — Create the Communication Opportunity
Session Phase: 1–2 Minutes
The session begins before the child knows it's begun. You're not announcing "therapy time." You're creating an irresistible situation where communication is the natural next step. The setup IS the intervention.
Child reaches for item
Hold it just out of reach. Wait for them to look at your face — that glance is the breakthrough.
Child grabs your hand
Gently take your hand back. Point to the item yourself. Say the name. Wait 3–5 seconds.
Child looks at you
CELEBRATE immediately. Eye contact during a request is pure gold — deliver the item right away.
Child makes any sound
CELEBRATE immediately. Any vocalization + any gesture = success. Deliver the item enthusiastically.

Step 2 — Meet Their Response With Yours
Session Phase: 3–5 Minutes
Your child has shown interest. Now shape the communication. The engagement hierarchy below moves from easiest (accept any communication) to most refined (pointing to choices). Always start at the level where your child is succeeding, then gently stretch upward.
Level 1 — Accept Any Communication
Child reaches toward you → deliver item immediately + "You want [item]!" Child looks at face → deliver + "You're telling me!" Child makes any sound while reaching → immediate delivery + enthusiastic response
Level 2 — Shape Toward Pointing
Hold item. Point to it yourself: "Point to [item]!" Gently guide child's hand into pointing position. The INSTANT their index finger extends → deliver. Fade physical prompts as quickly as possible.
Level 3 — Pointing to Choices
Present choice board with 2 pictures (one motivating, one neutral). "Which one? Point to what you want!" Accept any touch or point toward a picture. Gradually require more precise pointing over time.
SLP Guidance: "Don't wait for perfect pointing. A reach toward you instead of through you is progress. A glance at your face is progress. A grunt while looking at the item is progress. Celebrate every step on the communication ladder."

Step 3 — The Core Communication Exchange
Session Phase: 5–7 Minutes — 3 to 6 Cycles
This is the active ingredient — the moment where communication replaces hand-leading. When your child reaches for your hand to use it as a tool, follow this five-step sequence every single time. Consistency across repetitions is what builds the neural pathway.
🟢 Ideal
Child points to item independently → Immediate delivery + "You pointed! You told me what you want!"
🟢 Good
Child looks at your face while reaching → Immediate delivery + "You looked at me! That's communication!"
🟡 Acceptable
Child makes any sound while oriented toward you → Delivery + "I heard you!"
🟡 Emerging
Child reaches toward you (not through you) → Delivery + "You're reaching to me!"
🔴 Stop If
Escalating distress, self-injury, or complete shutdown → Comfort. Give item freely. Try again later with higher-value motivator and shorter wait time.
Common Execution Errors: Waiting too long (creates frustration, not motivation) • Physically forcing pointing hand position • Withholding necessities • Making every interaction a "therapy drill" — keep it playful
Step 4 — 3 Good Exchanges > 10 Forced Ones
Session Phase: 3–5 Minutes
Therapeutic dosage matters — but quality always beats quantity. Aim for 3 to 6 genuine, successful communication exchanges per session. When interest wanes, it's time to vary the stimuli or close the session on a high note.
Repetition Target
3–6 communication exchanges per session. Each successful exchange builds the pathway. Forced exchanges undermine trust and reduce future motivation.
Satiation Indicators
- Turning away from motivating items
- Reduced interest or enthusiasm
- Increased fussiness or distraction
- Looking for an exit from the interaction
Variation Options — Keep It Fresh
- Rotate motivating items every 2–3 exchanges
- Switch materials: container → bubbles → choice board
- Change your position: floor → table → standing at shelf
- Involve different activities: snack → play → book
- Use different rooms to build generalization
"If your child is still engaged and happy after 15 minutes — wonderful. But if attention wanes after 5 minutes, that's a complete, successful session. End on success, not exhaustion."
Step 5 — Celebration Is the Intervention
Reinforcement: Immediate — Within 1–2 Seconds
From ABA science: reinforcement timing matters more than magnitude. Celebrate immediately, specifically, and enthusiastically. Every time pointing produces a faster, better result than hand-leading, the brain learns: communication works better than manipulation.
Natural Reinforcement — Preferred
Child points to cracker → Gets the cracker. Child points at bubbles → You blow bubbles. Child touches picture on choice board → Gets that item. The pointing itself WORKS — that is the reward.
Social Reinforcement — Always Add
"You POINTED! You told me what you want!" • "I love how you looked at my face!" • "You used your finger — that's talking with your body!" Clapping, high-fives, hugs (if child enjoys touch).
What NOT to Do
Don't say "Good job" without specifying what was good. Don't delay reinforcement. Don't reinforce hand-leading with the same enthusiasm as pointing. Don't withhold reinforcement to "make them try harder."

Step 6 — End With Connection, Not Correction
Cool-Down: 1–2 Minutes
The session ends before the child wants it to end. Leave them wanting more. The cool-down ensures your child associates communication practice with positive feelings — not frustration or relief that it's over.
Total Session Breakdown
Setup: 1–2 min
Engagement: 3–5 min
Core Action: 5–7 min
Repetition: 3–5 min
Reinforcement: Ongoing throughout
Cool-down: 1–2 min
Total: 10–15 minutes
Engagement: 3–5 min
Core Action: 5–7 min
Repetition: 3–5 min
Reinforcement: Ongoing throughout
Cool-down: 1–2 min
Total: 10–15 minutes
Why Closing Ritual Matters
A consistent closing phrase ("All done! Great talking today!") and gesture (wave, clap) builds predictability. Your child learns the routine has a beginning, middle, and end — which increases tolerance for structure in all areas of life.

30-Second Session Log — Your Data Drives Progress
After each session, capture these five data points. It takes 30 seconds and transforms anecdotal impressions into trackable evidence. Your child's therapist uses this data in real time to adjust the intervention plan.
📊 Date & Time
Log the session date and time of day. Patterns (morning vs. evening performance) inform when sessions are most effective for your child.
📊 Motivating Items Used
Which item produced the most communication attempts this session? Track across weeks to identify your child's highest-value motivators.
📊 Number of Communication Exchanges
Circle: 1 | 2 | 3 | 4 | 5 | 6+. Even one genuine exchange is a complete, successful session.
📊 Best Response Achieved
Circle one: Hand-leading | Reaching toward me | Eye contact | Vocalization | Approximate point | Clear point | Point + vocalization
📊 Child's Mood at End
Circle: 😊 Happy | 😐 Neutral | 😟 Frustrated. Consistently negative end-moods indicate the approach needs modification.
GPT-OS® Integration: Log your data in the Pinnacle GPT-OS® system and your child's Communication Readiness Index updates automatically. Your therapist sees this data in real time at pinnacleblooms.org/gptos
Stuck? Here's What to Try
Every parent hits a wall. Every child has days (or weeks) where nothing seems to click. These targeted solutions address the most common obstacles families encounter when building pointing and communication at home.
"My child gets too frustrated and melts down"
Shorten wait times to 1–2 seconds, not 5. Use higher-value motivators. Accept ANY communicative attempt. Some children need hundreds of "easy wins" before tolerating longer waits. Check: are you accidentally withholding essentials?
"My child just walks away and gets the item themselves"
Environmental arrangement needs tightening. Ensure ALL motivating items are truly out of reach. Use items only YOU can activate — bubbles, wind-up toys, music. Make yourself the gateway to fun.
"They keep grabbing my hand no matter what I do"
This takes time. Gently redirect every time during practice sessions. Model pointing hundreds of times. The neural pathway is forming even when you can't see results yet — trust the process.
"I don't know if they CAN point — their hand stays in a fist"
This may be a motor issue, not a communication issue. Start with finger isolation activities (Material #8). If index finger isolation is difficult, consult your OT before expecting pointing.
"This works in therapy but not at home"
Use the SAME materials in BOTH settings. Ask your therapist to demonstrate exactly what they do. Practice in multiple home locations. Involve all family members for generalization.
If after 4 weeks of consistent daily practice you see no change — not even a slight shift from hand-leading toward looking at your face — book a reassessment. Your child's intervention may need professional modification.
Your Child Is Unique — Adapt the Protocol
No two children respond identically to the same approach. Use the difficulty slider and profile-based variations below to calibrate the protocol to exactly where your child is today — and adjust as they grow.
← Easier (Early Stages / Younger Children)
- Accept hand-leading as a starting point — add a pause before complying
- Use extremely high-value motivators only
- 1-second waits maximum
- Physical prompting for pointing is completely fine
- 2–3 exchanges per session maximum
→ Harder (Breakthrough Stage / Older Children)
- Require pointing or vocalization before delivery
- Extend wait times to 5–10 seconds
- Choice boards with 3–4 options
- Expect pointing + eye contact + vocalization combined
- Practice in noisy environments, during outings
Profile-Based Variations
🔵Sensory Seeker: Use highly stimulating motivators — spinning toys, musical instruments, textured items. Communication earns sensory input.
🔴Sensory Avoider: Use calming motivators — soft toys, preferred quiet activities. Keep sessions low-stimulation. Don't add pressure.
🟡Motor Challenges: Prioritize finger isolation work. Accept approximate pointing. Use large touch-targets on choice boards.
🟢Verbally Emerging: Pair pointing with any vocalization attempts. Model single words during every exchange.
Age Adaptations
- 12–18 mo: All communication attempts accepted. Heavy modeling. Physical prompting.
- 18–30 mo: Shape toward clear pointing. Introduce choice boards.
- 30–48 mo: Expect pointing + vocalization. Multiple-choice boards. Social games with verbal requests.
Weeks 1–2: The Foundation Is Forming (Even If You Can't See It)
Progress: ~15%
Neural pathways are forming beneath the surface during these first two weeks. Visible progress may be subtle — and that's completely normal. What you're watching for are micro-indicators, not milestones.
What Progress Looks Like
- A half-second pause before grabbing your hand (emerging awareness)
- A glance at your face during hand-leading — the glance IS the breakthrough
- Increased interest in motivating items when you control access
- Tolerating the "wait" period slightly longer than before
Not Expected Yet
- Independent pointing (this comes later — be patient)
- Consistent eye contact during requesting (still building)
- Using choice boards without prompting (too early to expect)
Metric to track this week: "How often does my child look at my face during a request?" Count this. It's the earliest leading indicator of progress — and it usually appears before any pointing emerges.
"If your child tolerates the communication setup for 30 seconds longer than last week — that's real progress. Trust the process."

Weeks 3–4: The Shift Becomes Visible
Progress: ~40%
By weeks three and four, consistent daily practice begins to produce observable behavioral changes. These are signs that neural pathways are consolidating — the communication map is being drawn. Behavioral changes also signal that your child is becoming aware of the interaction pattern.
1
Child anticipates the exchange
They know the routine. Anticipation is a cognitive milestone — your child is learning sequences.
2
Hand-leading frequency decreases
Even slightly — track it in your session log. A downward trend is everything.
3
Eye contact during requesting increases
They're checking whether you're a person with a perspective — this is theory of mind emerging.
4
Reaching TOWARD you instead of THROUGH you
This distinction is the core behavioral shift this technique is designed to produce.
5
Gaze shifting between you and the desired item
Looking from the item to your face and back — this IS joint attention emerging.
"You may notice you're more confident too. You've developed an intuition for when to wait and when to help. That clinical instinct? It's forming in you, just like the communication pathway is forming in your child."

Weeks 5–8: Communication Replaces Manipulation
Progress: ~70%
This is the phase families describe as transformative. The behavioral shift from hand-leading to pointing becomes consistent, generalized, and emotionally charged — for parent and child alike.
Pointing Emerges
Index finger isolation with intentional direction. Protoimperative pointing to REQUEST preferred items.
Choice Board Mastery
Functional, voluntary choice board use. Eye contact + gesture combinations appear simultaneously.
Generalization
Pointing appears in new contexts — at the store, with grandparents, during book reading. Untaught environments, untaught people.
Protodeclarative Pointing
Child begins pointing to SHARE INTEREST — "Look at that!" — not just to request. This means they understand you have a mind they can influence.
"The first time your child points at something just to show you — not to request it — you will cry. That protodeclarative point means they understand you have a mind, you can see what they see, and sharing that experience matters. That's theory of mind. That's connection."

Every Point Is a Victory. Here's What You've Built.
Each milestone below represents a genuine neurological and communicative achievement. Print this page. Check them off as they arrive. Share them with your Pinnacle team. Celebrate every single one.
1
🏅 First Look
Child looked at your face during a request
Week 1–2
Week 1–2
2
🏅 First Reach Toward
Child reached toward you, not through you
Week 2–3
Week 2–3
3
🏅 First Approximate Point
Whole hand extended toward desired item
Week 3–4
Week 3–4
4
🏅 First Clear Point
Index finger pointing at item to request
Week 4–6
Week 4–6
5
🏅 First Point + Look
Pointing while looking at your face simultaneously
Week 5–7
Week 5–7
6
🏅 First Sharing Point
Pointing to show you something interesting — protodeclarative
Week 6–8+
Week 6–8+
7
🏅 Generalized Point
Pointing in a new environment or with a new person
Week 7+
Week 7+
"You did this. Not the materials. Not the app. Not the therapist alone. YOU — the parent who noticed the hand-leading, who sat on the floor day after day creating communication opportunities. Your child's pointing exists because of your patience and persistence."

When Home Practice Isn't Enough — Know the Signs
Recognizing when to escalate is not a sign of failure — it's clinical wisdom. These observable indicators are your signal to seek professional modification of the intervention plan. Early escalation is always better care.
🟡 Amber Flags — Book a Reassessment
- No change in hand-leading frequency after 4 weeks of daily practice
- Child's frustration during sessions is increasing, not decreasing
- No eye contact during requests after 3 weeks
- Child has stopped engaging with motivating items entirely
- Regression: skills that emerged are disappearing
🔴 Red Flags — Seek Immediate Professional Evaluation
- Complete absence of any communicative intent beyond age 18 months
- Loss of previously acquired communication skills at any age
- Self-injurious behavior during communication attempts
- No response to name, no social smiling, no shared enjoyment — in combination
- New medical symptoms: seizures, sudden behavioral changes, pain indicators
"These flags don't mean you failed. They mean your child needs more support — possibly a modified approach, more intensive therapy, or medication review. Early escalation is better care."
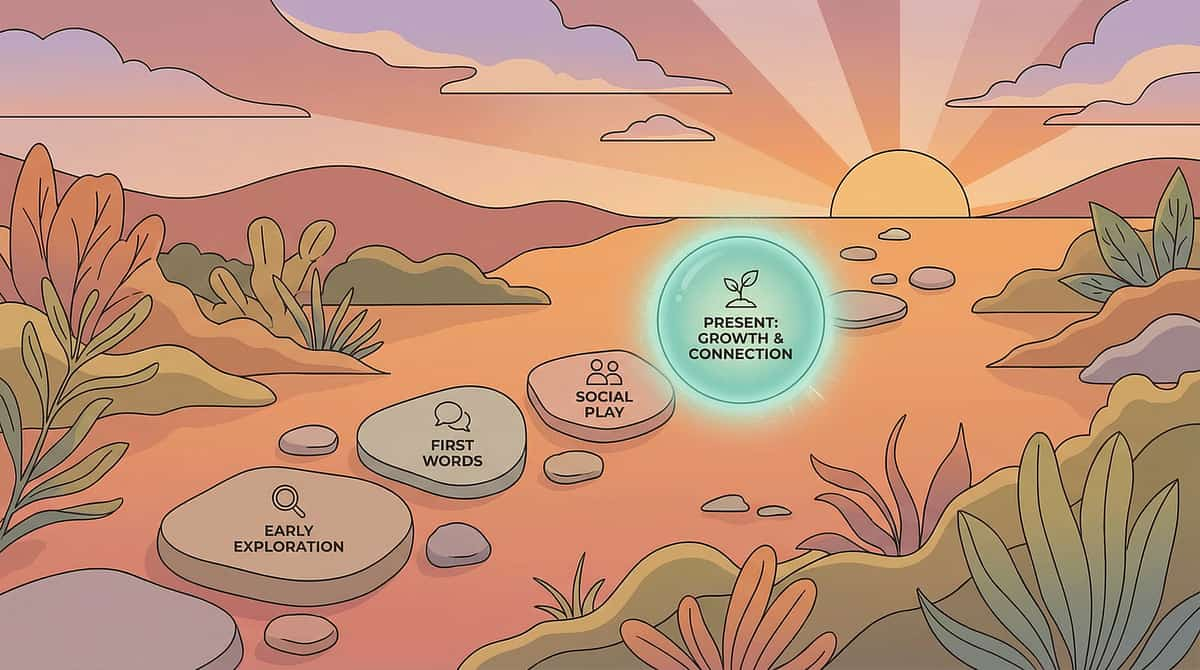
You're on a Journey — Here's the Map
Technique B-132 does not stand alone. It sits within a carefully sequenced progression of communication and joint attention interventions, each one building on the last and opening the door to the next. Here is your place on that map.
Prerequisite Techniques (Before B-132)
B-131: Limited Pretend Play — techniques.pinnacleblooms.org/B/limited-pretend-play
B-005: Reduced Eye Contact — techniques.pinnacleblooms.org/B/reduced-eye-contact
B-005: Reduced Eye Contact — techniques.pinnacleblooms.org/B/reduced-eye-contact
📍 YOU ARE HERE — B-132
Hand-Leading / Uses Hand as Tool — Communication Temptation & Pointing Development Protocol
If Pointing Is Emerging →
B-006: Limited Pointing or Gesturing (advanced pointing development)
techniques.pinnacleblooms.org/B/limited-pointing-gesturing
techniques.pinnacleblooms.org/B/limited-pointing-gesturing
If Eye Contact Is Improving →
B-134: Doesn't Respond to Name
techniques.pinnacleblooms.org/B/doesnt-respond-to-name
techniques.pinnacleblooms.org/B/doesnt-respond-to-name
If Communication Is Expanding →
B-133: Limited Functional Play
techniques.pinnacleblooms.org/B/limited-functional-play
techniques.pinnacleblooms.org/B/limited-functional-play
Lateral Alternatives: K-920: Communication Facilitation Strategies | K-915: Building Joint Attention — for families where this specific approach needs a different entry point.
More Communication & Joint Attention Techniques
These six techniques form the core of the Joint Attention & Gestural Communication domain. Notice how many use materials you've already gathered for B-132 — your kit is already building the foundation for the whole domain.
🟢 INTRO | B-005: Reduced Eye Contact
Materials: Social games, bubbles | You already own: ✅
🟡 CORE | B-006: Limited Pointing or Gesturing
Materials: Choice boards, pointing toys | You already own: ✅ (from this technique)
🟡 CORE | B-007: Not Following Where Others Point
Materials: Motivating items, pointing games | You already own: ✅
🟡 CORE | B-131: Limited Pretend Play
Materials: Pretend play sets, role-play props | You may need: some
🟡 CORE | B-134: Doesn't Respond to Name
Materials: Motivating items, name games | You already own: ✅
🔴 ADVANCED | K-915: Building Joint Attention
Materials: Complex social games, multi-person activities | Progressive build
This Technique Is One Piece of a Larger Plan
Communication doesn't develop in isolation. Pointing connects to motor development, social-emotional growth, cognitive understanding, and language. When you build pointing, you're building pathways across your child's entire developmental landscape.
Why All 12 Domains Connect
Pointing bridges motor development (Domain C), social-emotional growth (Domain E), cognitive understanding (Domain F), and language (Domain D). The WHO/UNICEF Nurturing Care Framework confirms that holistic, integrated developmental monitoring produces superior outcomes to siloed, discipline-specific approaches.
GPT-OS® Full Profile
Connect to GPT-OS® to see your child's personalized developmental profile across all 12 domains. Your therapist uses this same map to coordinate care — so every session in every discipline is pulling in the same direction.

Families Who Walked This Path Before You
These illustrative cases reflect the collective clinical experience of Pinnacle Blooms therapists across 70+ centers. Individual outcomes vary based on severity, consistency of intervention, and each child's unique developmental profile.
Hyderabad Family
"She used to grab my hand for everything — like I was a tool. After three months of speech therapy focusing on pointing and communication, she now points to what she wants and looks at my face. She's communicating WITH me, not through me."
— Parent, Pinnacle Network, Hyderabad [Illustrative case; individual outcomes vary]
— Parent, Pinnacle Network, Hyderabad [Illustrative case; individual outcomes vary]
Bangalore Family
"We started with clear containers and bubbles. That's it. Within two weeks, my son was looking at my face when he wanted bubbles. Within six weeks, he was pointing. The simplest materials made the biggest difference."
— Parent, Pinnacle Network, Bangalore [Illustrative case; individual outcomes vary]
— Parent, Pinnacle Network, Bangalore [Illustrative case; individual outcomes vary]
Vizag Family
"The choice board changed everything. He didn't point at first — he just slapped the whole board. But we counted that. Slowly, his hand got more specific. Now he uses his index finger. He has a voice, even without words."
— Parent, Pinnacle Network, Vizag [Illustrative case; individual outcomes vary]
— Parent, Pinnacle Network, Vizag [Illustrative case; individual outcomes vary]
You Don't Have to Do This Alone
Raising a child with communication differences is not a solo journey. Pinnacle Blooms has built a multi-layer support ecosystem specifically so that no family faces this alone — whether they're in a major city, a small town, or navigating limited access to in-person services.
Pinnacle Parent Community
Online parent support community for families working on communication development. Connect with parents navigating the same techniques at pinnacleblooms.org/parent-community
WhatsApp Support Groups
Connect with other parents in your city working on the same techniques. Contact your nearest Pinnacle center for access to the local parent group.
FREE National Autism Helpline
1800-123-7838 | Available 24×7 | 16+ languages. For questions, guidance, emotional support, or crisis intervention — at any hour.
Find Your Nearest Center
70+ centers across India. Find the one closest to you at pinnacleblooms.org/centers
International Resources
ASHA: www.asha.org | Autism Speaks: www.autismspeaks.org | WHO Early Childhood Development: who.int/ecd
When You Need Professional Guidance
Home practice is powerful — and it works best when supported by a professional team. Here's how to know when to step from home practice into structured professional services, and exactly what that path looks like at Pinnacle Blooms.
Speech-Language Therapy
Communication programming and gestural development, delivered by certified SLPs
ABA Therapy
Behavioral communication interventions with systematic data tracking
Occupational Therapy
Fine motor and sensory foundations for gestural development
Parent Training
Hands-on technique coaching — watch, practice, and receive corrective feedback
Teleconsultation
Virtual guidance for families without access to a nearby center
Full Research Index — Every Claim Is Evidence-Linked
Technique B-132 is grounded in a robust, multi-decade research base spanning foundational developmental science, randomized controlled trials, systematic reviews, and international implementation frameworks. Every clinical claim on this page links to a peer-reviewed source.
Baron-Cohen S. (1989)
"Perceptual role taking and protodeclarative pointing in autism." British Journal of Developmental Psychology. Foundational research establishing pointing differences in autism spectrum disorder.
Mundy P, Newell L. (2007)
"Attention, joint attention, and social cognition." Current Directions in Psychological Science. Joint attention as the foundation for social cognitive development.
Tomasello M et al. (2007)
"Understanding and sharing intentions: The origins of cultural cognition." Behavioral and Brain Sciences. Theory of shared intentionality and pointing as a communicative act.
PRISMA Systematic Review (2024) — PMC11506176
16 studies (2013–2023): structured communication intervention meets evidence-based practice criteria. Confirmed benefits for children with ASD.
World J Clin Cases (2024) — PMC10955541
Meta-analysis: parent-mediated interventions show effect sizes comparable to clinician-delivered services. 40-minute session optimal duration confirmed.
WHO Nurturing Care Framework (2018, updated 2022) — PMC9978394
CCD Package across 54 LMICs demonstrates home-based, caregiver-delivered interventions produce measurable communication gains.
Padmanabha H et al. (2019) — DOI: 10.1007/s12098-018-2747-4
Indian RCT demonstrating significant outcomes from home-based structured interventions. Indian Journal of Pediatrics.
Adapted UNICEF/WHO NCF for SLPs (2022) — DOI: 10.1080/17549507.2022.2141327
Multi-disciplinary nurturing care integration for speech-language pathologists. International Journal of Speech-Language Pathology.
Additional Sources: WHO Global Scales for Early Development (GSED) • UNICEF ECDI • ASHA Clinical Practice Guidelines for Joint Attention Intervention • Pinnacle Blooms Network® Clinical Data: 20M+ sessions, 97%+ measured improvement
GPT-OS® — The Operating System Behind This Technique
Every intervention technique on this platform is governed by GPT-OS® — the Global Pediatric Therapeutic Operating System. This isn't software. It is therapeutic infrastructure — the clinical backbone that coordinates your child's entire developmental journey across every discipline, every session, every setting.
Diagnostic Intelligence Layer
Converts 591+ structured observations across 349 skills into standardized diagnostic clarity — no guesswork, no opinion variance.
AbilityScore®
Patented universal developmental score (0–1000) establishing baseline, severity, and longitudinal change — comparable across time, therapists, and centers.
TherapeuticAI®
Determines therapy focus, intensity, sequencing, and reinforcement logic — always under licensed human clinical authority.
EverydayTherapyProgramme™
Translates clinical plans into daily home-executable micro-interventions. This technique page IS part of ETP.
FusionModule™
Coordinates SLP, OT, behavioral, special education, and medical inputs into one converged therapeutic pathway. No silo. One plan.
Closed-Loop Control
Observe → Score → Plan → Execute → Re-measure → Adapt. Plans change only when the child's data changes. Evidence drives every decision.
20M+
Therapy Sessions
97%+
Measured Improvement
70+
Centers Nationwide
160+
Countries — Patents Filed
Watch the 75-Second Video Summary
Everything on this page — condensed into 75 seconds. Share this reel with your partner, your parents, your child's teachers, and anyone else in your child's world who needs to understand why your child grabs hands instead of pointing, and exactly what to do about it.
B-132 Video Summary: "Hand-leading is a communication difference, not a rejection. These 9 materials help build pointing and genuine communication — from clear containers that create motivation to social games that make YOU the source of fun, not just a tool for getting things."
📱 Share on WhatsApp
Send to your family group, your spouse, or your parent community
📸 Share on Instagram
#HandLeading #PointingDevelopment #JointAttention #AutismSigns
👥 Share on Facebook
#EarlyIntervention #CommunicationSkills #SpeechTherapy #PinnacleBlooms
Series Context: Communication and Joint Attention Differences Series — Episode 132 of 150
← Previous: B-131 Limited Pretend Play | Next: B-133 Limited Functional Play →
← Previous: B-131 Limited Pretend Play | Next: B-133 Limited Functional Play →
Everyone in Your Child's Life Needs to Know This
Communication development requires consistency across ALL caregivers — not just during therapy sessions. When every adult in your child's life uses the same approach, generalization happens faster, more completely, and in the environments that matter most.
For Your Spouse / Partner
"I'm learning about why [child's name] grabs our hands to get things instead of pointing. It's called hand-leading, and there's a specific technique to help build pointing. Can you read this page so we can practice together? [Link]"
For Grandparents / Extended Family
"The therapist is teaching us how to help [child's name] learn to point instead of grabbing our hands. Here's what we're doing at home — it would help so much if you could do the same when you're with them. [Link]"
For Childcare / School
"[Child's name] is working on developing pointing and gestural communication. Here are the specific strategies we're using. Could you incorporate these during the day? [Link]"
Available In: English | Hindi | Telugu | Tamil | Kannada | Malayalam | Bengali | Marathi | Gujarati

Your Questions, Answered by the Consortium
These are the questions Pinnacle Blooms SLPs, BCBAs, and OTs hear most often from families working on pointing and hand-leading. Clear, clinically accurate answers — no jargon, no ambiguity.
"Is hand-leading a definite sign of autism?"
Hand-leading is one of many early indicators of autism spectrum differences, but it is not diagnostic on its own. Persistent hand-leading as the primary communication method beyond 12–15 months, especially combined with absent pointing and limited eye contact, warrants professional assessment.
"Will my child ever stop hand-leading?"
With consistent intervention, most children develop conventional communicative gestures that supplement or replace hand-leading. The timeline varies significantly — some children show changes in weeks, others in months. Progress is measured in approximations, not all-or-nothing change.
"Can I do this without a therapist?"
You can — and should — begin these techniques at home today. However, professional guidance ensures the approach is calibrated to your child's specific profile. A combination of professional therapy and home practice produces the best outcomes.
"My child is already 3 years old. Is it too late?"
It is never too late to develop communication. While earlier intervention typically produces faster results, the brain's plasticity supports communication development well into childhood and beyond. Start now — today is always the right time.
"Should I stop complying with hand-leading completely?"
No. During dedicated practice sessions, gently redirect hand-leading toward pointing. During daily life, continue responding to hand-leading while modeling pointing. The goal is to make pointing MORE effective, not to punish hand-leading.
"How do I know which material to start with?"
Start with the three essentials: clear containers with motivating items, bubbles, and a simple 2-picture choice board. These three cover communication motivation, adult-as-source repositioning, and pointing target practice — the three pillars of this technique.
You've Read It. You Understand It. Now — Do It.
Knowledge without action changes nothing. You now have everything you need: the neuroscience, the technique, the materials, the step-by-step protocol, the troubleshooting guide, and the progress timeline. The only thing left is to begin. Your child's first pointing gesture is waiting — and so is the moment you receive it.
🟢 Start This Technique Today
Download the 30-second session tracker + Quick Start Guide. Launch your first session using the GPT-OS® session launcher.
🔵 Book a Communication Assessment
Free screening at your nearest Pinnacle center. Get your child's AbilityScore® baseline and a personalized intervention plan.
🟡 Explore the Next Technique
B-133: Limited Functional Play — the natural next step when communication is expanding.
✅ Validated by SLP
✅ Validated by BCBA
✅ Validated by OT
✅ Validated by SpEd
✅ Validated by NeuroDev
Preview of 9 materials that help when child uses hand as tool Therapy Material
Below is a visual preview of 9 materials that help when child uses hand as tool therapy material. The pages shown help educators, therapists, and caregivers understand the structure and content of the resource before use. Materials should be used under appropriate professional guidance.





Link copied!
The Pinnacle Promise
"From fear to mastery. One technique at a time." — The Pinnacle Blooms Consortium
Explore More Techniques
Next Recommended
B-133: Limited Functional Play
techniques.pinnacleblooms.org/B/limited-functional-play
techniques.pinnacleblooms.org/B/limited-functional-play
FREE Helpline
1800-123-7838 | 24×7 | 16+ languages
For guidance, support, or crisis intervention at any hour
For guidance, support, or crisis intervention at any hour
Medical Disclaimer: This content is for educational purposes only and does not replace professional evaluation or treatment. Hand-leading instead of pointing is an early marker of autism spectrum disorder and warrants comprehensive assessment. Consult a developmental pediatrician, speech-language pathologist, or other qualified professional for individualized guidance. Communication development varies significantly among children. Individual results vary.
© 2025 Pinnacle Blooms Network®, unit of Bharath Healthcare Laboratories Pvt. Ltd. All rights reserved. CIN: U74999TG2016PTC113063 | DPIIT: DIPP8651 | MSME: TS20F0009606 | GSTIN: 36AAGCB9722P1Z2
techniques.pinnacleblooms.org | Powered by GPT-OS® | Built by Mothers. Engineered as a System.
techniques.pinnacleblooms.org | Powered by GPT-OS® | Built by Mothers. Engineered as a System.