
"He squints at the living room light. Not sunlight. The living room."
Your child's nervous system is speaking. The Pinnacle Blooms Consortium — 500+ therapists across Occupational Therapy, Speech-Language Pathology, ABA, Special Education, and NeuroDevelopmental Paediatrics — has built this page to give you exactly what you need: 9 materials that work, the science behind them, and a step-by-step protocol you can start tonight.
Sensory Solutions Series — Episode 57
Ages 2–12
Pinnacle Blooms Consortium

You Are Among Millions
When your child squints at the classroom lights, they are not the only one. Across India alone — with an estimated prevalence of 1–1.5% for autism spectrum conditions in a paediatric population of 400+ million — millions of families navigate light sensitivity every single day. In stores, in schools, at family gatherings: the same confusion, the same isolation, the same search for answers. That isolation ends here.
80%
Sensory Processing Differences
Of children diagnosed with autism spectrum disorder experience sensory processing difficulties, including visual sensory over-responsivity. Source: PRISMA Systematic Review, Children, 2024 — PMC11506176
1 in 6
Children Globally
Show signs of sensory processing differences that impact daily function, with light sensitivity among the most common visual sensory challenges. Source: World J Clin Cases, 2024 — PMC10955541
42
Countries Tracked
By UNICEF use developmental monitoring indicators that include sensory processing markers, validating this as a global developmental priority. Source: UNICEF MICS, WHO Nurturing Care Framework 2018
20M+
Therapy Sessions
Exclusive 1:1 therapy sessions delivered by the Pinnacle Blooms Network across 70+ centres, serving families from 70+ countries.

The Brightness Dial Is Set Differently
The Neuroscience
The visual system includes dedicated pathways for detecting light intensity. In typical development, the nervous system modulates response to varying light levels automatically — pupils adjust, the visual cortex calibrates, and normal indoor lighting registers as baseline.
In visual sensory over-responsivity (photophobia), this modulation is altered. The pupil may constrict normally — the eye hardware works fine. But central processing in the thalamus and visual cortex treats the incoming light signal as noxious, excessive, or threatening. The brain's gain control is turned up too high.
This creates real physiological discomfort. Squinting, headaches, fatigue, and distress are not behavioural choices. They are neurological responses to a sensory signal the brain is misinterpreting as dangerous.
What This Means for Your Child
This is a wiring difference, not a behaviour problem.
Your child is not being dramatic. They are not attention-seeking. The light that feels neutral to you genuinely feels excessive, painful, or threatening to their nervous system. Their protective responses — squinting, shielding, avoiding, crying — are the body's logical response to what the brain perceives as a noxious stimulus.
Understanding this changes everything: we stop trying to convince them the light is fine (it isn't, for their brain), and we start modifying the light, the environment, and their tools so they can function.
Frontiers in Integrative Neuroscience (2020): Comprehensive framework for evaluating sensory integration/sensory processing treatment in ASD. DOI: 10.3389/fnint.2020.556660

Your Child's Light Sensitivity on the Developmental Map
Light sensitivity does not appear overnight — it follows a developmental arc. Understanding where your child sits on this map helps you calibrate your expectations and choose the right intervention intensity.
Birth–6 Months
Visual system develops basic light/dark response. Pupillary reflexes establish.
6–18 Months
Visual cortex matures. Light modulation pathways begin calibrating. Early signs of photophobia may emerge — infant turns away from ordinary light, prefers dim rooms.
18 Months–3 Years ⚡
Common Emergence Window. Sensory processing differences become observable. Child squints at indoor lights, resists bright environments. Often coincides with language emergence — child verbalises that lights "hurt."
3–6 Years
Functional impact peaks as environments expand. School entry exposes child to fluorescent lighting, gymnasium lights, outdoor recess. Light sensitivity becomes a participation barrier.
6–12 Years
Self-awareness develops. Child may develop coping strategies or avoidance patterns. With intervention, tolerance building is possible. Without support, anxiety about bright environments may solidify.
Light sensitivity commonly co-occurs with: auditory sensitivity, migraine, anxiety, and broader sensory processing disorder. Your child is on this map — and intervention has a clear forward trajectory. WHO Care for Child Development Package. Source: PMC9978394

Clinically Validated. Home-Applicable. Parent-Proven.
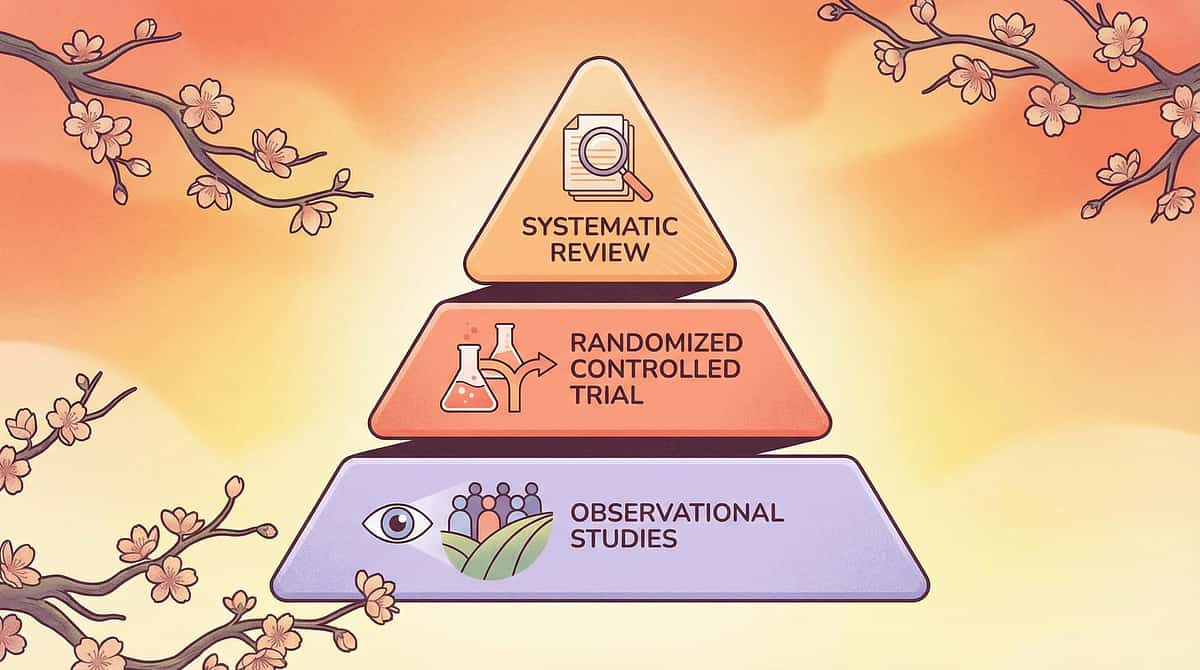
Level II–III Evidence
Systematic Reviews + RCTs + Clinical Consensus
The materials and strategies on this page are drawn from evidence-based practice supported by peer-reviewed research, WHO/UNICEF developmental frameworks, and clinical consensus across the Pinnacle Blooms Consortium's multi-disciplinary team of 500+ therapists. This is not experimental. This is validated, structured, and ready for your home.
16 Studies (2013–2023)
PRISMA-model systematic review confirms sensory integration intervention meets criteria to be considered evidence-based practice for children with ASD. Source: PMC11506176 — Children, 2024
24 Studies
Meta-analysis demonstrates sensory integration therapy effectively promotes social skills, adaptive behaviour, sensory processing, and gross/fine motor skills. Source: PMC10955541 — World J Clin Cases, 2024
Indian RCT (2019)
Home-based sensory interventions demonstrated significant outcomes in a controlled trial involving the Indian paediatric population. Source: DOI: 10.1007/s12098-018-2747-4 — Indian J Pediatr
FL-41 Tinted Lenses
Multiple studies demonstrate reduction in photophobia symptoms, originally validated for fluorescent-light-triggered migraine, now applied broadly to sensory photophobia. Source: Optometry clinical literature

Light Sensitivity Management Through Environmental Modification and Protective Materials
Domain: SEN-VIS-PHOTO
Ages 2–12
Home + School
Parent-Friendly Name: "Light Comfort Toolkit — 9 materials that make the world less bright for your child"
This intervention technique addresses photophobia in children through a structured approach combining three layers: personal protection (tinted lenses, hats, sunglasses), environmental modification (window films, alternative lighting, screen adjustments), and systemic supports (transition strategies, sensory retreats, accommodation plans). The approach is not about avoiding light permanently — it is about filtering, modifying, and managing light so the child can participate in daily life without sensory distress.
Domain
Sensory Processing / Visual System
Age Range
2–12 years
Setting
Home + School + All Lit Environments
Duration
Ongoing daily management with structured introduction protocol
Primary Discipline
Occupational Therapy (Sensory Integration)

Your Consortium Team for Light Sensitivity
Light sensitivity management crosses therapy boundaries because the brain does not organise by therapy type. Effective intervention requires a coordinated multi-disciplinary team, each playing a distinct and essential role.
Occupational Therapist (Primary Lead)
Conducts sensory processing evaluation. Identifies specific light triggers (wavelength, intensity, flicker). Designs environmental modification plan. Guides tinted lens selection. Develops sensory diet addressing visual system modulation. Builds transition protocols and retreat strategies.
Developmental Paediatrician / NeuroDev Specialist
Rules out medical causes of photophobia (migraine, meningitis, ocular conditions). Coordinates with ophthalmology if needed. Monitors comorbid conditions. Provides documentation for accommodations.
Board Certified Behaviour Analyst (BCBA)
Develops systematic desensitisation protocols. Creates data collection systems for tracking tolerance. Designs reinforcement strategies for wearing tinted glasses or using transition techniques. Addresses avoidance behaviours functionally.
Special Educator
Implements classroom accommodations. Coordinates with school staff on lighting modifications. Integrates light sensitivity management into IEP/accommodation plans. Adapts academic activities for visual comfort.
Adapted UNICEF/WHO Nurturing Care Framework (2022): Multiple disciplines contribute to nurturing care. DOI: 10.1080/17549507.2022.2141327
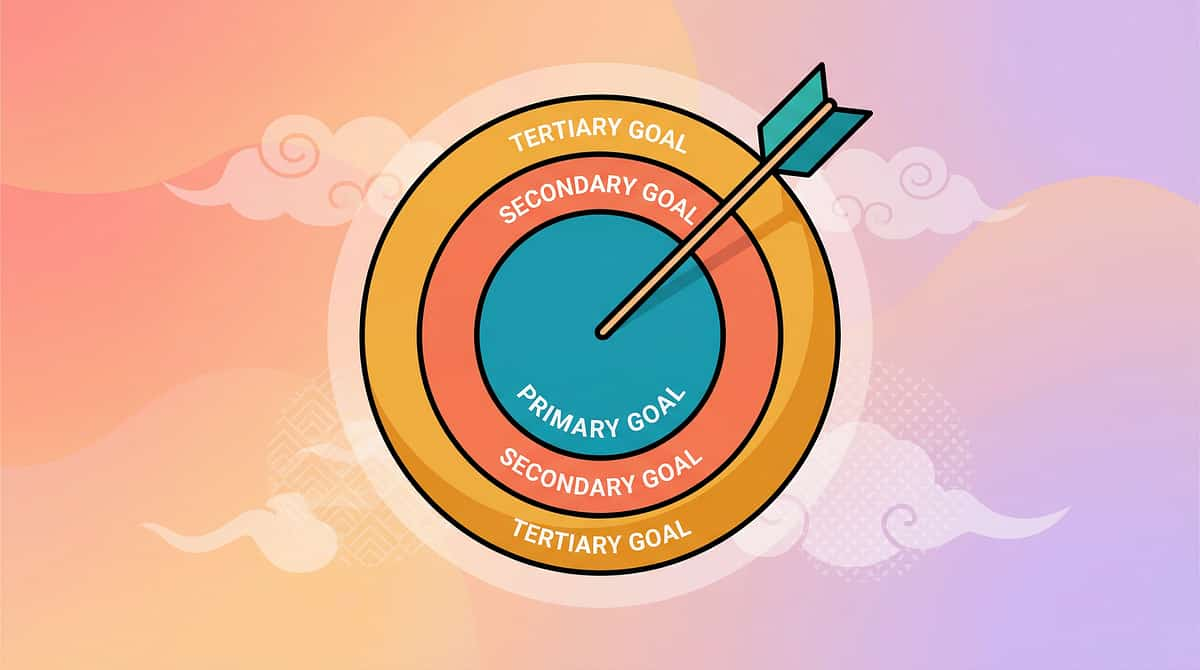
Precision Targets — What This Intervention Changes
Effective intervention targets a hierarchy of outcomes. Understanding the full target spectrum helps you measure progress at multiple levels simultaneously — not just "fewer squints," but broader developmental gains.
Primary Target — Visual Sensory Modulation
Reducing the neurological over-response to typical light levels. Observable indicator: reduction in squinting frequency, eye-shielding duration, and light-avoidance behaviours in daily settings.
Secondary Targets
Environmental participation in stores, classrooms, gyms, and outdoor spaces. Emotional regulation and reduction in light-triggered meltdowns. Autonomic nervous system regulation — reduced stress response when exposed to varied light conditions.
Tertiary Targets
Academic performance, social participation, self-advocacy skills, and sleep regulation. Better circadian rhythm management through controlled light exposure. Meta-analysis (World J Clin Cases, 2024): PMC10955541

Your Light Sensitivity Toolkit — 9 Materials
These nine materials span personal protection, environmental modification, and systemic support. Together, they form a complete, layered approach. Start with what you can access today — even ₹0 and a hat makes a difference.
Total Investment Range: ₹0–15,000
Essential Starters: ₹0 — Hat + Screen Settings + Accommodation Request

1. Tinted Lenses & Specialty Glasses
₹2,000–15,000. FL-41 rose-tinted lenses filter blue-green wavelengths. TheraSpecs, Axon Optics, or prescription photophobia glasses from local optical shops. Canon: Sensory Tools — Visual

2. Hats, Caps & Visors
₹200–1,500. Baseball caps with dark underbrims, bucket hats, wide-brimmed hats. Personal shade zone from overhead light. Canon: Environmental Modification

3. Window Films & Light Covers
₹500–5,000. Solar films for windows, fluorescent light diffuser covers, light-filtering curtains, blackout shades. Canon: Environmental Modification

4. Alternative Lighting
₹300–3,000. Warm LED bulbs (2700K), dimmer switches, table/floor lamps, flicker-free LED options, smart bulbs. Canon: Environmental Modification

5. Transition Supports
₹0–500. Visual transition cards, social stories about brightness changes, timers for adaptation pauses. Canon: Behavioural Tools

6. Sensory Retreat Materials
₹500–5,000. Pop-up sensory tent, canopy, blackout curtains, eye mask, comfortable dim-space seating. Canon: Sensory Environment

7. Screen Modifications
₹0–2,000. Blue light filter settings/apps, physical screen protectors, dark mode activation. Free on every device made after 2016. Canon: Technology Modification

8. Sunglasses (Outdoor)
₹500–5,000. UV-protective wrap-around sunglasses, polarised lenses, sport straps, multiple darkness levels. Canon: Sensory Tools — Visual

9. Accommodation Plans
₹0 (documentation). Written accommodation requests, school 504 plan templates, professional documentation for school and community settings. Canon: Systemic Support
Every Family Can Start Today — Zero Cost Options
The WHO Nurturing Care Framework emphasises context-specific, equity-focused interventions. If you have ₹0 and a hat, a bedsheet, and a phone with Night Mode — you can start managing your child's light sensitivity today. This table gives every family an accessible starting point.
Buy This | Make This (Free / Household) | |
FL-41 Tinted Lenses (₹2K–15K) | Regular sunglasses with lighter tint worn indoors (temporary measure only — consult OT for proper tinting) | |
Specialty Hat (₹500+) | Any brimmed hat from existing wardrobe. Dark fabric taped under the brim reduces ceiling reflection. | |
Solar Window Film (₹500+) | Newspaper temporarily taped on bright windows. Sheer dupatta or fabric draped over curtain rod. | |
Smart LED Bulbs (₹500+) | Move lamps from other rooms to create indirect lighting. Remove some bulbs from multi-bulb fixtures to reduce intensity. | |
Commercial Sensory Tent (₹2K+) | Bedsheet draped over chairs to create a dim fort. Cardboard box with cut opening and blanket interior. | |
Blue Light Screen Filter (₹500+) | Enable built-in Night Shift / Night Light / Eye Comfort — free on every device made after 2016. | |
Written Accommodation Plan | Handwritten letter to teacher explaining light sensitivity with specific requests. Free template at pinnacleblooms.org |
Equity Statement: The Pinnacle Blooms Consortium designs every technique for universal access. You do not need to spend a single rupee to begin. Source: PMC9978394 | WHO NCF Handbook (2022)
Safety Gate — Read Before Starting
Before introducing any light sensitivity materials, work through this safety checklist. Most families will reach Green confidently. If you hit Red — stop and seek medical evaluation first.
🔴 DO NOT PROCEED IF:
Child has sudden onset of severe light sensitivity not previously present — seek immediate medical evaluation (may indicate meningitis, increased intracranial pressure, or acute ocular condition). Child has not had a comprehensive eye exam within 12 months. Sudden vision changes alongside light sensitivity. Light sensitivity accompanied by persistent vomiting, neck stiffness, or altered consciousness — EMERGENCY — seek medical care immediately.
🟡 MODIFY AND CONSULT IF:
Child has diagnosed migraine — coordinate with neurologist. Child is on medications that increase photosensitivity (certain antibiotics, antiepileptics). Child has epilepsy — some lighting modifications require neurologist guidance. Child resists all protective gear — consult OT for gradual introduction strategies.
🟢 SAFE TO PROCEED WHEN:
Eye examination confirms normal vision / current vision correction. Light sensitivity is a consistent pattern (not sudden onset). Child is in a regulated emotional state. Materials are age-appropriate and properly fitted.
Material Safety Notes: Tinted lenses — use lightest effective tint; very dark indoor tints can increase dark adaptation. Hats indoors — ensure hat does not obstruct peripheral vision. Window films — dim ≠ dark; maintain adequate light for reading. Retreat spaces — recovery tool, not total avoidance. Indian J Pediatrics RCT (2019). DOI: 10.1007/s12098-018-2747-4
Prepare Your Home Light Environment
A one-time home audit and setup takes about 90 minutes and creates the foundation for every session that follows. Work room by room, systematically — the goal is to create a gradient from comfort zone to challenge zone.
Step 1: Audit Your Light Sources (30 minutes)
Walk through every room your child uses daily. Identify: type of overhead light (fluorescent, LED, incandescent), window direction and intensity, any flicker (fluorescent tubes), and brightness level. Rate each room 1–5 for your child's comfort.
Step 2: Create the Primary Comfort Zone
Child's room/study area: Replace overhead fluorescent with warm LED (2700K) or add dimmer switch. Place table lamp with warm bulb as primary light source — indirect, not overhead. Apply window film or light-filtering curtain. Designate one corner as sensory retreat (tent, canopy, or curtained area).
Step 3: Prepare Transition Zones
Hallway between dim bedroom and bright living area — add intermediate lighting. Front door entry — place hat and tinted glasses on a hook at child's height. This creates a visual cue and daily ritual.
Step 4: Pack the Portable Kit
Small bag with: hat, tinted glasses, sunglasses, transition card, and eye mask for emergencies. This kit travels to school, stores, and family events.
Remove from Space: Bare fluorescent tubes without diffuser covers. Mirrors or reflective surfaces that create glare points. Direct overhead lighting as the only light source in study area.

Pre-Session Readiness — 60-Second Check
The best session is one that starts right. Run through this checklist before every new material introduction. It takes 60 seconds and prevents a wasted session.
Eye Exam Is Current
Vision tested within 12 months. No medical photophobia diagnosis requiring separate treatment.
Child Is Fed, Hydrated, and Rested
Hunger, dehydration, and fatigue all lower sensory tolerance thresholds significantly.
No Recent Meltdown
At least 30 minutes since last significant dysregulation episode.
Environment Is Prepared
Light modifications from Card 12 are in place. Materials (hat/glasses/tinted lenses) are accessible and fitted.
Child Shows Baseline Regulation
Calm enough to engage — does not need to be happy, just not in active distress.
✅ All Green → GO
Begin the material introduction protocol (Step 1).
🟡 1–2 Amber → MODIFY
Use simplified version: just offer the hat or tinted glasses without full protocol. Let child choose.
🔴 Any Red → POSTPONE
Alternative calming activity instead. Dim the room, offer retreat space, try tomorrow.

Step 1 of 6
Step 1 — Introducing the Light Comfort Tools (The Invitation)
The introduction is the most important moment. Get the framing right — this is a gift, not a treatment. Your body language and tone communicate more than your words.
Script (exact words to say): "Hey [child's name], I got something really cool for you. You know how the lights sometimes bother your eyes? I found some special [glasses/hat/thing] that might make them feel better. Want to see?"
Body Language Guidance
- Sit at child's level, not standing over them
- Hold the material casually, not presenting it like medicine
- Smile. This is a gift, not a treatment.
- If offering tinted glasses: wear a pair yourself first. Model comfort.
What Acceptance Looks Like
- Child reaches for the material
- Child shows curiosity (looking at it, touching it)
- Child allows you to place hat on their head or glasses on their face (even briefly)
What Resistance Looks Like & How to Modify
- Child pushes away: Place the material nearby within reach. Say "It's here whenever you want it." Move on. Try again tomorrow.
- Child shows anxiety: Leave the glasses/hat on the table in their room for 2–3 days. Let familiarity develop before offering.
- Child says "I don't need it": Validate. "That's okay. Some kids like how these feel. If the lights ever bug you, they're right here."
Timing: 30–60 seconds. No pressure. The goal is a positive first impression, nothing more.
Ages 2–3: Play-Based Introduction
Skip verbal explanation. Simply offer the hat during a fun activity. Put it on a stuffed animal first. Make it part of dress-up play, not a therapeutic introduction.
Ages 8–12: Agency-Based Introduction
"I read that these special glasses can help with light sensitivity. Here are three options — which one do you think looks best?" Let them choose. Autonomy increases acceptance significantly.

Step 2 of 6
Step 2 — First Contact With the Material
Once the child accepts the material, you move into the first real test: a brief, positive encounter with the protective tool in a normally challenging light environment. Keep it short. The data matters more than the duration.
For Tinted Lenses / Glasses
Once the child accepts the glasses, walk together into a room that is normally problematic (kitchen with overhead lights). Stay 30 seconds. Ask: "How do the lights feel now?" Accept any answer. Remove glasses if child requests. Even 30 seconds of comfortable exposure to previously distressing light is data.
For Hats
Place hat on child and walk into a bright room together. Point upward: "See how the hat blocks the light from up there?" If child is comfortable, extend time. If child removes hat, note how long they kept it on.
For Environmental Modifications
Invite child into the modified room. "I changed the lights in here. How does this feel?" Compare with child: turn the old lights on briefly, then back to new warm lights. Let them feel the difference directly.
Engagement
Smiles, relaxes brow, stops squinting, voluntarily stays in bright space → reinforce verbally immediately.
Tolerance
Neutral expression, stays but doesn't seem excited → continue, don't push. This is a valid and valuable response.
Avoidance
Squints through the new tool, removes it, asks to leave → stop, retreat, reduce intensity next time. Not failure — data.
Reinforcement Cue: The moment the child shows any comfort in a previously uncomfortable light environment: "Look at you — you're in the kitchen and your eyes look so relaxed! Those glasses are really doing their job!"
Timing: 1–3 minutes.PMC11506176: Sensory integration intervention with structured material introduction meets evidence-based practice criteria.

Step 3 of 6
Step 3 — Using the Light Comfort Tool in a Real Environment
This is the active ingredient: protected exposure to the challenging stimulus. With the chosen material in place, deliberately expose the child to a previously problematic light environment — but now with protection. The activity anchors positive experience in a previously negative space.
Common Execution Errors
- ❌ Starting in the most challenging environment (school gym with full fluorescents). Start mild.
- ❌ Making the light exposure the focus. The ACTIVITY should be the focus; light tolerance is the background gain.
- ❌ Forcing continued exposure when child signals distress. Protection + comfort, not endurance training.
- ❌ Removing the protective tool mid-session to "test" the child. Never remove protection without consent.
Child Response Spectrum
- Ideal: Child is absorbed in activity, doesn't mention lights, appears visually comfortable.
- Acceptable: Child notices lights but continues activity with protective tool.
- Concerning: Child squints through protective tool, asks to leave, shows escalating distress → END session, retreat to dim space.
Meta-analysis (World J Clin Cases, 2024): 40-minute clinic sessions showed maximum effectiveness. Home sessions: 10–20 minutes. Core action: 40–60% of session time. Source: PMC10955541
Step 4 of 6
Step 4 — Building the Pattern
Neuroplasticity is built through repetition across varied contexts. The same protective tool in different environments on different days builds breadth of tolerance, not just depth in a single setting.
1–2
Sessions Per Day
Daily protected exposure sessions. Consistency is more important than session length.
7–10
Sessions Per Week
Weekly target across different environments for maximum neuroplastic benefit.
8–12
Weeks
Typical SI protocol duration for meaningful, measurable tolerance gains.
Sessions 1–3: Living Room
Full lights + tinted glasses. Home base environment. Build baseline comfort.
Sessions 4–6: Kitchen
Overhead fluorescents + hat. One step up in challenge intensity.
Sessions 7–9: Outdoor Morning Walk
Natural light + sunglasses. Variable, natural light environment.
Session 10+: Brief Store Visit
Portable kit (glasses + hat). Community environment. Major milestone.
"3 good sessions > 10 forced sessions." Sensory fatigue is real. When child appears fatigued or cranky — end the session. Quality beats quantity every time.

Step 5 of 6
Step 5 — Celebrate Every Win
Reinforcement delivered within 3 seconds of the desired behaviour increases the likelihood of that behaviour recurring. Be specific, be immediate, and celebrate the attempt — not just the success.
When child wears tinted glasses for a full activity:
"I'm so proud of you for keeping your special glasses on! Look at you — sitting in the kitchen with all the lights on, and your eyes look so comfortable!"
When child tolerates a new environment:
"Wow, we just walked through the whole store and you didn't have to cover your eyes once! Your [glasses/hat] really helped, and you were so brave trying it."
When child self-advocates:
"You told me the lights were bothering you and asked for your glasses. That's exactly what you should do. That was really smart."
Reinforcement Menu
- Verbal praise — always, immediately, within 3 seconds
- High-five or preferred physical gesture
- Preferred activity after the session ("Let's go play in your [dim] room now — you earned some chill time")
- Small tangible reward for major milestones (first full store trip, first school day with accommodation plan working)
- Sticker chart for daily protective tool use (younger children)
"Celebrate the attempt, not just the success." A child who wears the glasses for 2 minutes before removing them made progress. That's data, and that's worth acknowledging. ABA Reinforcement Principles: Immediate, specific reinforcement increases behaviour occurrence.
Step 6 of 6
Step 6 — Transition to Comfort
The cool-down is not an afterthought — it is a structured part of the protocol. How a session ends shapes how the child enters the next one. A smooth, predictable close builds trust in the whole process.
2-Minute Warning
"In two more minutes, we're going to head back to your [dim/comfortable] room. You did great today." Predictability reduces transition resistance significantly.
The Transition
Walk child from the bright/modified environment back to their comfort zone (retreat space, dim room). If outdoors, transition from bright to shaded area. Calm, unhurried movement.
Sensory Recovery
Allow 5–10 minutes in preferred dim environment. Offer eye mask if child enjoys it. Let them self-regulate — this is not punishment, it's recovery. The nervous system needs decompression time.
Material Put-Away Ritual
"Let's put your light glasses in their case. They'll be ready for you next time." Child hangs hat on their hook. Creating a ritual normalises the tool as daily equipment — like shoes.
If Child Wants to STAY in Bright Environment
That's actually the best possible outcome — they're choosing the challenging environment. "That's fantastic. Let's do five more minutes and then transition." Note it in your tracker.
If Child Is Upset About Ending a Preferred Activity
Use "First/Then" — "First we put away, then [preferred next activity]." Visual supports for transitions are classified as evidence-based practice for autism (NCAEP, 2020).

60 Seconds of Data Now Saves Hours of Guessing Later
Your session data flows into GPT-OS® and shapes personalised recommendations for your child. Track immediately after each session — memory fades within minutes. Three fields is all it takes.
1
Field 1: Environment
Where was the session? Living room / Kitchen / Outdoor / Store / School. Record the specific room or location.
2
Field 2: Duration of Comfortable Tolerance
How many minutes did the child remain comfortable with the protective tool in the challenging light environment? Record as a number in minutes.
3
Field 3: Comfort Rating (1–5)
1 = Distressed throughout. 2 = Uncomfortable but managed. 3 = Mostly comfortable. 4 = Comfortable. 5 = Comfortable without protective tool (spontaneously removed glasses/hat and stayed comfortable).
Date | Environment | Tool Used | Duration (min) | Rating (1–5) | Notes | |
"Your data flows into GPT-OS® and shapes personalised recommendations for your child."ABA Data Collection Standards: Continuous measurement as standard practice. Reference: BACB Guidelines

Troubleshooting — When Sessions Don't Go Perfectly
Every family encounters obstacles. These are not signs of failure — they are data points. Each problem below has a researched, tested solution. Work through these systematically before concluding that the technique isn't working.
"My child won't wear the tinted glasses."
Start with hats (less invasive). Let child choose glasses style. Have them in the room for days before offering. Let child decorate the case. Try clip-on tints for existing glasses. Consider OT consultation for desensitisation protocol.
"The environmental changes didn't seem to help."
The wrong light type may have been modified. If you changed bulbs but left fluorescent tubes in an adjacent room, the flicker may still be reaching the child. Audit systematically — one room at a time.
"Child melted down when I tried to remove the glasses."
Don't remove them. The goal is protected function, not unprotected tolerance (yet). That's a later-stage goal. For now, comfort with tools = success.
"Child was comfortable at home but school is still terrible."
Home modification addresses only one environment. School requires formal accommodation (Material #9). Request a meeting. Provide documentation. The child needs the same protections at school.
"Child got worse — more sensitive, not less."
If using very dark tints indoors constantly, dark adaptation may be occurring. Lighten the tint. If sensitivity is genuinely increasing, consult developmental paediatrician — sensory changes can indicate developmental shifts or medical factors.
"Session abandoned — child had a meltdown."
Session abandonment is not failure — it's data. What triggered the meltdown? Light intensity? Duration? Transition? Unfamiliar environment? Record it. Adjust one variable next time.
Personalise for YOUR Child
No two children with light sensitivity are identical. This protocol scales across sensitivity levels, ages, and temperaments. Find your child's current point on the difficulty spectrum and work from there — never from an arbitrary starting point.
Easier Version
For bad days / younger children / high sensitivity. Darkest appropriate tint. Modified home environment only. Sessions of 3–5 minutes. One protective tool. Retreat immediately at any distress signs.
Standard Version
For most sessions. Appropriate tint for the environment. Progress through home rooms, then familiar outside environments. Sessions of 10–15 minutes. Combine tools (glasses + hat). Transition supports between light levels.
Harder Version
For breakthroughs / older children / building tolerance. Lighter tint or just hat. Unfamiliar environments (new store, friend's house). Sessions of 20–30 minutes. Brief periods without protective tools. Self-advocacy practice.
By Sensory Profile
- Light Avoider (most photophobic children): Priority is protection and comfort. Don't push exposure speed. Environmental modification is primary.
- Light-Fascinated but Overwhelmed: Allow brief engagement with controlled light, then transition. Fibre optic light toys in retreat space may help.
By Age
- Ages 2–4: Tool introduction through play, not instruction. Hat during outdoor play. Modified bedroom as sanctuary.
- Ages 5–8: Choice-based. "Which glasses do you want today?" Social stories for school accommodations.
- Ages 9–12: Self-management training. Child carries and deploys own toolkit. Peer education: "I wear these because bright lights bother my eyes — it's a brain thing, not an eye thing."
Progress Arc — Week 1–2
Weeks 1–2 — The Introduction Phase
Neuroplasticity is working from day one. Progress in the first two weeks is subtle and internal. Learn to recognise the real milestones — not the Instagram-worthy ones.
✅ Child accepts wearing tinted glasses for 2–3 minutes
Even if they remove them after. First week tolerance may be seconds. That is normal. That is progress.
✅ Child reaches for hat before entering a bright space
Emerging self-awareness. The nervous system is beginning to connect the tool with comfort.
✅ Reduced squinting in modified home rooms
From constant to intermittent. A measurable neurological shift is occurring.
✅ Child uses "the lights hurt" language
Instead of unexplained meltdowns. This is PROGRESS. Naming the discomfort is a developmental milestone in self-awareness and communication.
What Is NOT Progress Yet: Child voluntarily choosing bright environments (too early). Wearing glasses all day without prompting (most children need 4–6 weeks). No meltdowns in unmodified environments — that takes systemic change.
"If your child wears the tinted glasses for 30 seconds longer than yesterday — that is measurable progress. Neuroplasticity is working. Trust the process."
Progress: ████░░░░░░░░░░░░░░░░ 15%PMC11506176: Sensory integration intervention outcomes emerge across 8–12 week timelines.
Progress Arc — Week 3–4
Weeks 3–4 — Neural Pathways Are Forming
Something shifts around week three. The child stops experiencing the protective tools as novel impositions and starts experiencing them as familiar comfort providers. This is the consolidation phase — the nervous system is building new associative pathways.
Spontaneous use of protective tools
Child puts on glasses/hat without being prompted before entering bright spaces. This is the consolidation landmark milestone.
Extended tolerance duration
From 3–5 minutes to 10–15 minutes in challenging light environments. Duration growth tracks neural pathway strengthening.
Verbal preference statements
"I like the warm light better" or "Can we use the lamp?" The child is now consciously aware of and expressing environmental preferences.
Reduced anticipatory anxiety
Less resistance before entering stores, school, or bright rooms. The threat response is recalibrating.
Transition adaptations internalised
Child begins pausing at thresholds naturally, without verbal cues. Adaptive behaviour is now automatic.
When to increase intensity: If child is comfortable for 15+ minutes with protective tool in home environments → begin adding community environments (brief store visits, friend's house, outdoor walks).
"You may notice you're more confident too." Parent self-efficacy is the strongest predictor of continued intervention implementation.
Progress: ████████░░░░░░░░░░░░ 40%

Progress Arc — Week 5–8
Weeks 5–8 — Functional Mastery Emerging
By week five, you are no longer managing a crisis — you are building a life. The milestones at this stage are functional, social, and participatory. They are the ones that change your family's daily experience.
🏆 Full School Day Navigated
Child navigates full school day with accommodation plan + protective tools with minimal light-related distress.
🏆 Store Visits Completed
Full grocery shopping trip with hat/glasses and no meltdown. Community participation milestone.
🏆 Self-Advocacy Observed
Child tells teacher "The lights are bothering me, can I use my glasses/move seats?" This is a developmental landmark beyond sensory management.
🏆 Tolerance Building Visible
Child tolerates some previously problematic environments WITHOUT protective tool for brief periods.
🏆 Proactive Retreat Use
Child goes to dim space for recovery BEFORE reaching meltdown, demonstrating genuine self-regulation capacity.
Maintenance Check: Does the child maintain tolerance when you stop the structured protocol and move to natural daily use of tools? If yes → Mastery achieved. If tolerance regresses → Return to consolidation-phase protocol for 2 weeks. Source: PMC10955541 | BACB mastery criteria standards
Progress: ███████████████░░░░░ 75%🏅LIGHT SENSITIVITY MANAGEMENT — FUNCTIONAL MASTERY

You Did This. Your Child Grew Because of Your Commitment.
You arrived on this page searching for answers about why your child squints at normal light. You learned it's not a vision problem — it's a neurological difference. You acquired materials. You modified your home. You introduced protective tools with patience. You tracked data. You adapted when things didn't work. You advocated at school.
And now your child walks through the grocery store wearing their tinted glasses, comfortable, regulated, participating. That transformation happened because of you.
"Write down the moment you realised the light sensitivity management was working. What was your child doing? Where were you? How did it feel to see them comfortable?"
Family Celebration Suggestion
Mark this milestone. Take a photo of your child doing something they couldn't do comfortably 8 weeks ago — sitting in a bright restaurant, playing at the park in full sun with their sunglasses, studying at a desk with warm lamp light. Frame it. Date it. That is your family's evidence of progress.
From Fear to Mastery
One technique at a time. The nervous system that once experienced ordinary light as a threat now navigates the world with tools, strategies, and a family who understands. That is everything.

Clinical Guardrails — When to Seek Professional Help
Trust your instincts — if something feels wrong, pause and ask. These red flags are specific to light sensitivity management and require escalation beyond home protocol.
🔴 Increasing Sensitivity Despite Consistent Intervention
If after 4+ weeks of protective tool use and environmental modification, light sensitivity is getting WORSE, not better → Consult developmental paediatrician. Rule out progressive medical cause.
🔴 New Symptoms Appearing
Light sensitivity accompanied by new headaches, nausea, balance issues, or vision changes → Medical evaluation needed. Do not continue protocol until cleared.
🔴 Child Develops Fear of ALL Environments
If accommodation has shifted to avoidance (child refuses to leave dim room), anxiety may be driving behaviour beyond sensory processing → Behavioural consultation needed.
🔴 Protective Tools Causing Social Isolation
If child refuses to attend events even with full protective toolkit, peer relationship impact may require additional social skills support.
🔴 Skin Symptoms Around Eyes
Tinted glasses or hats causing irritation, pressure marks, or allergic reaction → Change materials, consult allergist if needed.

Your Child's Journey Forward — Where to Go From Here
Every technique in the Pinnacle Blooms library is a node in a connected pathway. Understanding where A-057 sits in your child's broader developmental journey helps you plan intelligently for what comes next.
← PREREQUISITE
A-045: Sensory Overload in Public Spaces — General overwhelm management. The foundational technique before targeted light sensitivity work.
⭐ CURRENT TECHNIQUE
A-057: 9 Materials That Help When Child Squints at Lights — You are here. Light sensitivity management through environmental modification and protective materials.
Path A — Deeper Visual Sensory Work
→ A-058: Visual Clutter Overwhelm — if child also struggles with busy visual environments
→ A-059: Pattern and Movement Sensitivity — if ceiling fans or scrolling screens are also triggers
→ A-059: Pattern and Movement Sensitivity — if ceiling fans or scrolling screens are also triggers
Path B — Broader Sensory Integration
→ A-052: Auditory Sensitivity — if light sensitivity co-occurs with sound sensitivity
→ A-048: Meltdowns Triggered by Sensory Input — if meltdowns persist despite light management
→ A-048: Meltdowns Triggered by Sensory Input — if meltdowns persist despite light management
Path C — Functional Participation
→ K-985: Advocating for Sensory Accommodations at School — deepen the accommodation strategy
→ K-990: Creating a Sensory-Friendly Home — whole-home environmental design
→ K-990: Creating a Sensory-Friendly Home — whole-home environmental design

More Sensory Processing Techniques You Can Explore
"You already own materials for 4 of these 6 techniques." Your investment in light sensitivity management creates a foundation for broader sensory support across overlapping domains.
Technique | Difficulty | Materials You Already Own | |
A-045: Sensory Overload in Public Spaces | Intro | ✅ Hat, tinted glasses, retreat strategies | |
A-048: Meltdowns Triggered by Sensory Input | Core | ✅ Retreat space, transition supports | |
A-052: Auditory Sensitivity | Intro | Partially — retreat space transfers | |
A-058: Visual Clutter Overwhelm | Core | ✅ Window films, environmental modification skills | |
A-059: Pattern and Movement Sensitivity | Advanced | Partially — tinted lenses may help | |
K-990: Creating a Sensory-Friendly Home | Intro | ✅ All environmental modification tools transfer |
This Technique Is One Piece of a Larger Plan
Light sensitivity management does not exist in isolation — it opens doors across your child's entire developmental profile. Understanding these connections helps you see the full value of every session you complete.
Domain J: Emotional Regulation
Unmanaged light sensitivity → meltdowns → emotional dysregulation cycle. Managing light breaks this cycle at its source.
Domain L: Community Participation
Light sensitivity management → store visits, school attendance, social events → direct participation gains.
Domain I: Cognitive / Academic
Classroom comfort → attention → learning gains. Reducing visual distress is a prerequisite for academic engagement.
Domain F: Social Communication
Self-advocacy for accommodations is a communication skill. Every time your child asks for their glasses, they are practising functional communication.
WHO/UNICEF Nurturing Care Framework: Five components of nurturing care require holistic developmental monitoring. Source: WHO NCF (2018)
Real Families. Real Results.
Family Story 1
Before: "School was torture because of the fluorescent lights. He'd come home with headaches every day and meltdowns every week. The classroom felt like it was attacking him."
Intervention: FL-41 glasses, school accommodation plan (seating away from windows, hat permission), teacher switched to lamps when possible, sensory room access for breaks.
After (8 weeks): "He still wears his glasses every day. He still takes breaks when needed. But he's not in pain anymore, and that changed everything."
— Parent, Pinnacle Network. Illustrative case; outcomes vary by child profile.
Family Story 2
Before: "Birthday parties were impossible. The moment someone used a camera flash, she'd scream and bury her face. We stopped going."
Intervention: Tinted glasses for events, social story about flash photography, advance communication to hosts about minimising flash, designated dim recovery corner at events.
After (6 weeks): "She wore her glasses to her best friend's party and stayed for two hours. She even asked if there would be 'the flashy camera' beforehand — that's self-advocacy. She asked."
— Parent, Pinnacle Network. Illustrative case; outcomes vary.
"Light sensitivity is one of the most responsive sensory challenges to environmental modification. When we stop arguing with the child's experience and start modifying the world to meet their neurological reality, progress is often rapid and dramatic." — Pinnacle Blooms Occupational Therapist
You Are Not a Solo Operator — Join Your Community
Isolation is the enemy of adherence. Every family that shares their light sensitivity management journey gives another family the courage to start. The Pinnacle community is built by parents, for parents — real questions, real answers, real understanding.
Sensory Solutions Parent Group
Join the dedicated WhatsApp group for families navigating light sensitivity. Share wins, ask questions, and get peer support from families who understand exactly what you're going through.
Pinnacle Parent Community Forum
In-depth discussions, technique comparisons, accommodation letter templates, and school navigation advice. community.pinnacleblooms.org
Peer Mentoring Programme
Connect with a parent who has been through this journey. Pinnacle's Peer Mentor Programme matches new families with experienced families navigating the same challenge.
WHO NCF: Community engagement is a core principle. Parent support networks improve intervention outcomes.
Home + Clinic = Maximum Impact
The protocol on this page is designed for home implementation. Pairing it with professional OT support at a Pinnacle centre produces measurably better outcomes — the clinic extends what you build at home, and what you build at home extends what the clinic achieves.
Find Your Nearest Pinnacle Centre
70+ centres across India. Each centre operates under GPT-OS® standards with measurable accountability. Sensory Integration-trained Occupational Therapists at every location.
Therapist Matching
For light sensitivity, your primary discipline match is an Occupational Therapist with Sensory Integration specialisation. Secondary: NeuroDevelopmental Paediatrician for medical coordination.
Teleconsultation (Remote Families)
Can't visit a centre? Teleconsultation available in 16+ languages. Free initial guidance through the National Autism Helpline.
FREE National Autism Helpline: 9100 181 181 | Available 24/7 | 16+ Languages | No cost
Services Relevant to Light Sensitivity:
- Occupational Therapy (Sensory Integration)
- Comprehensive Developmental Evaluation
- School Consultation and Accommodation Support
- EverydayTherapyProgramme™
- AbilityScore® Assessment
The Science Behind Every Recommendation on This Page
Every claim on this page traces back to peer-reviewed research. This is the reference library — for the parent who wants to understand the evidence, the therapist who needs citations, and the educator who needs to justify accommodations to an administrator.
PRISMA Systematic Review (2024)
Sensory integration intervention as evidence-based practice for ASD. 16 articles, 2013–2023. PMC11506176 — Children, 2024
Meta-Analysis (2024)
Sensory integration therapy effectiveness across 24 studies — social skills, adaptive behaviour, sensory processing, motor skills. PMC10955541 — World J Clin Cases, DOI: 10.12998/wjcc.v12.i7.1260
Indian RCT (2019)
Home-based sensory interventions with significant outcomes in Indian paediatric population. DOI: 10.1007/s12098-018-2747-4 — Indian J Pediatrics
WHO Nurturing Care Framework (2018)
Foundation for early childhood development interventions. https://nurturing-care.org/ncf-for-ecd/
Frontiers in Integrative Neuroscience (2020)
Framework for evaluating SI/SP treatment in ASD. DOI: 10.3389/fnint.2020.556660
NCAEP Evidence-Based Practices Report (2020)
Visual supports and video modelling as evidence-based practices. National Clearinghouse on Autism Evidence and Practice.

Your Data Shapes Personalised Recommendations
The tracking sheet from Card 20 is not just a paper record — it feeds a learning system that gets smarter about your specific child with every session you log.
GPT-OS® Core Stack Connection
Diagnostic Intelligence Layer → AbilityScore® → Prognosis Engine → TherapeuticAI® → EverydayTherapyProgramme™ → FusionModule™ → Closed-Loop Therapeutic Control
This technique page feeds the Sensory Regulation Index and Environmental Tolerance Index within the GPT-OS® architecture.
Privacy Assurance
All data is governed under Pinnacle's ISO/IEC 27001 Information Security framework. Individual data is never shared, sold, or exposed. Only anonymised population-level patterns feed the recommendation engine.
"Your data helps every child like yours."
Digital health intervention evidence: 21 RCTs, 1,050 participants per 2024 meta-analysis.

Watch: 9 Materials That Help When Child Squints at Lights
Reel ID: A-057
Sensory Solutions Series — Episode 57
60 seconds
A Pinnacle therapist walks you through all 9 materials in 60 seconds — tinted lenses on a child's face, hat blocking overhead light, warm lamp replacing fluorescent, the sensory retreat tent, the transition pause at a doorway. Visual demonstration of everything this page explains in text.
Video Embed Placeholder: Embed A-057 Reel from Pinnacle OTT Platform or Instagram/YouTube. Reel ID: A-057 | Domain: Sensory Processing / Visual System | Duration: 60 seconds. Presented by a Pinnacle Blooms Network Occupational Therapist specialising in Sensory Integration.
"Video + text + demonstration = maximum parent skill acquisition." Video modelling is classified as evidence-based practice for autism (NCAEP, 2020).
Consistency Across Caregivers Multiplies Impact
A child who wears their tinted glasses at home but encounters unchanged fluorescent lights at school — and no hat at grandma's house — receives an inconsistent therapeutic message. Every caregiver your child spends time with needs to understand and apply the same approach.
Family Guide (1-Page PDF)
Simplified version for spouses, grandparents, and babysitters. Clear, non-clinical. Printable and shareable. Everything the non-primary caregiver needs on a single page.
Teacher Communication Template
Letter explaining light sensitivity + specific accommodation requests. Ready to customise with your child's name and send to the class teacher or SENCO.
'Explain to Grandparents' Guide
Short, non-clinical explanation: "Why [child's name] wears special glasses indoors." Plain language, no jargon, no stigma.
WhatsApp-Formatted Summary (Copy-Paste Ready): "Hi! I found this really helpful page about managing light sensitivity in children. [Child's name] has been struggling with bright lights, and this has 9 materials and a step-by-step plan that's working for us. Here's the link: techniques.pinnacleblooms.org/sensory-processing/light-sensitivity-materials. It's from Pinnacle Blooms Network (India's largest autism therapy chain). Take a look when you have a minute!"
WHO CCD Package emphasises multi-caregiver training as critical for intervention generalisation. Source: PMC9978394
Your Questions, Answered
These are the questions Pinnacle therapists hear most often from families navigating light sensitivity. Every answer is grounded in the same evidence base as the rest of this page.
Will my child always be light-sensitive?
Light sensitivity may improve with neurological maturation, consistent environmental management, and tolerance building. Some children grow into significantly reduced sensitivity by adolescence. Others maintain it as a permanent trait they learn to manage effectively. Either way, with the right tools, light sensitivity does not have to limit your child's life.
Should I let my child wear sunglasses indoors?
Yes — with the right type. Properly tinted indoor glasses (lighter than outdoor sunglasses, ideally FL-41 or similar) protect without causing dark adaptation. Very dark sunglasses indoors can make sensitivity worse over time. The key is the lightest effective tint for indoor use.
Is this the same as migraine photophobia?
Related but distinct. Sensory processing photophobia is a consistent pattern across light exposures. Migraine photophobia intensifies during migraine episodes. FL-41 tints help both. If your child also has headaches, consult a neurologist — the two conditions often co-occur and benefit from coordinated management.
Will these materials be needed forever?
Some children phase out protective tools as tolerance builds. Others use them lifelong, like someone who wears reading glasses. There's no failure in needing tools. The goal is function and participation, not performing normalcy.
How do I get the school to cooperate?
Start with a written request citing your child's sensory processing evaluation (from OT or developmental paediatrician). Request a meeting. Specify accommodations: seating location, hat/glasses permission, retreat access, lighting modifications. Get everything in writing. The Pinnacle School Consultation service can support this process.
Is this covered by insurance?
Sensory processing evaluations and OT sessions are covered under many health insurance plans in India. Tinted lenses may be covered if prescribed by an ophthalmologist. Contact your insurer with ICD code for photophobia (H53.14) and sensory processing disorder.
What if my spouse/family doesn't believe this is real?
Share this page. Show them Card 03 (the neuroscience). Show them Card 05 (the evidence). Light sensitivity is documented in peer-reviewed literature, recognised by WHO developmental frameworks, and treatable. It's not about belief — it's about evidence.
Can I combine these materials with each other?
Absolutely. Most effective management uses multiple layers: tinted glasses + hat + modified home lighting + school accommodations. The materials are designed to work together, not in isolation.

You've Read the Evidence. You've Seen the Plan. Start.
Every day without light sensitivity management is a day your child's nervous system is working harder than it needs to. The protocol is ready. The materials are accessible. The evidence is clear. The only remaining step is yours.
Validated by the Pinnacle Blooms Consortium
OT • SLP • ABA • SpEd • NeuroDev | 500+ Therapists | 70+ Centres | 20M+ Sessions | 97%+ Measured Improvement
Preview of 9 materials that help when child squints at lights Therapy Material
Below is a visual preview of 9 materials that help when child squints at lights therapy material. The pages shown help educators, therapists, and caregivers understand the structure and content of the resource before use. Materials should be used under appropriate professional guidance.




















Link copied!

From Fear to Mastery. One Technique at a Time.
The Pinnacle Blooms Consortium — 500+ therapists across Occupational Therapy, Speech-Language Pathology, Applied Behaviour Analysis, Special Education, and NeuroDevelopmental Paediatrics — built this page so that every parent, everywhere, can transform their home into a scientifically grounded, personalised, multi-sensory therapy environment for their child.
Powered by GPT-OS®
AI-driven personalised therapeutic recommendations built on 20M+ sessions.
Built by Mothers
Designed for parents by a team that understands what it means to search for answers at 11pm.
Engineered as a System
Every technique connects to a larger network of 70,000+ evidence-linked interventions.
Pinnacle Blooms Network®🌸 OTT Platform | 🌸 Marketplace | 🌸 70+ Centre Network
FREE National Autism Helpline: 9100 181 181 | 16+ Languages | 24/7
pinnacleblooms.org | care@pinnacleblooms.org
FREE National Autism Helpline: 9100 181 181 | 16+ Languages | 24/7
pinnacleblooms.org | care@pinnacleblooms.org
Medical Disclaimer: This content is educational. It does not replace evaluation by a physician, ophthalmologist, or occupational therapist. Light sensitivity can be associated with various medical conditions — persistent or severe photophobia should be evaluated to rule out underlying causes and identify appropriate intervention. Individual results may vary. Statistics represent aggregate outcomes across the Pinnacle Blooms Network.
Legal: © 2025 Pinnacle Blooms Network®, unit of Bharath Healthcare Laboratories Pvt. Ltd. All rights reserved. CIN: U74999TG2016PTC113063 | DPIIT: DIPP8651 (Govt. of India). GPT-OS®, AbilityScore®, TherapeuticAI®, EverydayTherapyProgramme™, FusionModule™ are registered trademarks/patents filed across 160+ countries.
40 cards × 70,000+ techniques = 2,800,000 evidence-linked, parent-empowering, GPT-OS®-powered knowledge units. The largest structured paediatric intervention knowledge base on Earth.