

"We intervene not to force social desire, but to build positive neural associations with peer interaction — gradually rewiring the reward signal through structured, enjoyable experiences." — Pinnacle SLP + OT + ABA Consortium

Study | Finding | Grade | |
PRISMA Systematic Review (Children, 2024) PMC11506176 | Peer-mediated + interest-based interventions are evidence-based practices for ASD | Level I | |
Meta-analysis (World J Clin Cases, 2024) PMC10955541 | Social skills + peer interaction outcomes significantly improved with structured interventions | Level I | |
Kasari et al. (J Consulting Clinical Psychology, 2012) | RCT: Peer-mediated social skills group = significant gains in peer engagement | Level II | |
NCAEP Evidence-Based Practices Report (2020) | Peer-mediated instruction + video modeling = evidence-based practices | Level I | |
Padmanabha et al. Indian J Pediatr (2019) | Home-based structured social interventions effective in Indian population | Level II |
"This is NOT about making your child social by neurotypical standards. It IS about expanding their capacity for peer connection, on their terms, at their pace."

- Designs reinforcement schedules for peer interaction
- Structures peer buddy programs
- Data-tracks peer engagement attempts
- Targets social language, scripting, peer communication
- Provides peer interaction scripts
- Addresses theory of mind foundations
- Addresses sensory barriers to peer engagement
- Designs parallel play environments
- Manages sensory overwhelm that blocks peer tolerance
- Facilitates peer buddy programs in school
- Structures classroom peer activities
- IEP social goals integration
"A NeuroDevelopmental Pediatrician first rules out anxiety vs. motivation differences. The FusionModule™ within GPT-OS® then coordinates ABA + SLP + OT inputs into a single converged peer motivation pathway."
Target Domain | Specific Observable Goal | |
Peer Proximity Tolerance | Child tolerates peer within 3 feet for 5+ minutes | |
Peer Orienting | Child glances at peer during peer's action | |
Structured Interaction | Child participates in rule-based activity with 1 peer for 10+ min | |
Interest-Based Contact | Child seeks peer to engage with preferred interest activity | |
Verbal Initiation | Child uses script or spontaneous words to approach peer | |
Reciprocal Exchange | Child takes 3+ conversational turns with peer |


Peer Video Modeling
Material 2 of 9 ABA Lead | NCAEP EBP | Exposure Graduation A safe, predictable preview before facing unpredictable real peers The Science (ABA + OT) Video modeling is classified as a Tier 1 Evidence-Based Practice by NCAEP (2020) for children with ASD. The critical advantage for peer-avoidant children: videos offer pausable, rewindable, predictable peer exposure. The child learns what peer play LOOKS LIKE before experiencing its unpredictability. Neural peer-recognition pathways activate without sensory overwhelm. How It Works Watch videos of peers playing cooperatively (culturally relevant, age-matched) Pause and discuss: "See how Aarav shared the ball? That's what sharing looks like" Gradually introduce same activity in real life AFTER video previewing Video preview reduces the novelty threat of real peer interaction DIY Protocol: "Record 2-minute videos of cousins, neighbors, or school friends playing together — activities your child finds interesting. Watch together daily. Pause and label: 'They're taking turns. That looks fun, doesn't it?' Make real peer play predictable by watching it first." 🛒 Canon Product: Dyomnizy Educational Memory Game — Lights & Sound — ₹519 | amazon.in/d/0iwJwOiH — Use alongside video modeling to demonstrate peer cause-effect play sequences ⚠️ Safety Note: Video is preparation, NOT replacement for real peer exposure. Ensure videos feature culturally appropriate, demographically similar peers. | Citation: NCAEP EBP Report (2020) — Video modeling EBP classification

- Start with 2-player games with simple, crystal-clear rules
- Adult mediates the first 3–5 sessions (referee + reinforcer)
- Short sessions (10 minutes maximum initially)
- Predictability IS the therapeutic mechanism — don't improvise rules
DIY Protocol: "Ludo. Snakes & Ladders. Simple card games. Uno. These require minimal language, have clear rules, defined turns. The peer becomes safe because they are rule-bound. Start here before anything more complex."

- Set up identical activities at adjacent stations (2 children, same materials, separate spaces)
- No interaction required or prompted — just shared space
- Parent narrates: "You're both building. You're in the same room. That's great."
- Gradually reduce distance between stations over weeks
DIY Protocol: "Two children painting at adjacent tables. Two children building Lego at opposite ends of the same mat. Same activity. Adequate personal space. No pressure to interact — just tolerate the presence. This IS therapy."

- Set up toy where PEER activates the exciting effect
- Point to peer immediately: "Priya pressed it — look what happened!"
- Child must attend to peer to anticipate the exciting outcome
- Gradually increase peer's role in generating interesting events
DIY Protocol: "Control a light-up toy or sound toy from one side — child watches from the other. 'Look! [Peer name] makes it light up!' Then let child take turns. The peer becomes the source of interesting things. This is the foundation of social reward."

Situation | Script | |
Joining play | "Can I play?" | |
Showing interest | "What are you building?" | |
Requesting turn | "Can I have a turn?" | |
Sharing | "Do you want some?" | |
Ending play | "I need to stop now. Bye." |
DIY Protocol: "Make 5 laminated index cards with approach phrases. Practice with parent as 'pretend peer' daily for 1 week. Then use in real peer situations with the card as backup. Fade the card over 4 weeks."
- Identify 2–3 tolerant, patient neurotypical peers
- Train them: how to approach, what to expect, how to persist without pressure
- Buddy sessions: 15–20 minutes, structured activity, adult nearby
- Debrief with buddies: what worked, what didn't, celebrate their patience
DIY Protocol: "Talk to your child's cousin, neighbor, or classmate (with parent permission): 'My child finds it hard to start playing with others. Would you help by going to him and saying Can I play too? — and then just starting to play near him?' Brief the willing peer. Most children are kinder than we expect."

DIY Protocol: "Draw a 10-box reward chart. Each box = one successful peer interaction attempt (does not need to be perfect). Fill all 10 boxes = child chooses tonight's movie. Simple. Achievable. Works."

- Child shows active fear or panic at peer presence (may indicate anxiety disorder — consult professional first)
- Child has had a significant distress episode in last 2 hours
- Child is unwell, hungry, or overtired
- You are planning to force physical proximity or touch without consent
- Peer partner is known to be rough, loud, or unpredictable
- Child is mildly dysregulated — use simpler, shorter version
- Only one peer available and they are unfamiliar
- Environment is noisy or overstimulating
- Child refuses materials — switch to parallel only, no demands
- Child is calm, fed, rested
- Peer partner is familiar, patient, and has been briefed
- Environment is quiet, predictable, space is adequate
- Materials ready and session is planned

- ✅ Remove competing distractions (screens off, other toys out of sight)
- ✅ Lighting: natural or warm lamp light (not fluorescent)
- ✅ Sound: quiet background (no TV, low ambient noise)
- ✅ Temperature: comfortable (not hot/stuffy)
- ✅ Materials pre-positioned (not searching mid-session)
- ✅ Timer visible to both children
- ✅ Positive reinforcement items ready nearby
Week | Session Length | |
Week 1–2 | 10 minutes maximum | |
Week 3–4 | 15 minutes | |
Week 5–8 | 20–25 minutes | |
Week 9+ | 30 minutes as tolerated |
Check | Observation | Score | |
🍽️ | Fed? Last meal within 2 hours | ✓ / ✗ | |
😴 | Rested? Not overtired, no meltdown in last hour | ✓ / ✗ | |
🎯 | Regulated? Calm baseline, not in escalation | ✓ / ✗ | |
😷 | Well? No signs of illness, fever, pain | ✓ / ✗ | |
👂 | Sensory? No visible sensory distress in current environment | ✓ / ✗ | |
⏱️ | Time? At least 30 minutes of uninterrupted time available | ✓ / ✗ |
"Postponing is not failure — it is clinical wisdom. The best session is one that starts right."
- Position yourself diagonally — not between children
- Kneel to child's level — never tower over
- Soft, warm voice — no urgency
- Wait 10 full seconds for response before repeating
- Child glances at peer or peer's item ✓
- Child moves slightly toward peer ✓
- Child takes the offered item ✓
- Child doesn't actively move away ✓ (this is enough)
- Child ignores completely → Re-present with preferred item directly
- Child moves away → Don't pursue; run parallel play only today
- Child shows distress → Stop, return to Readiness Gate and Postpone
- Present material at child's preferred distance (not forced into hands)
- Allow 5–10 seconds of observation before offering
- Match material to child's sensory profile (avoid overwhelming textures/sounds initially)
Response | Meaning | Action | |
Approaches material | Engagement | Continue — reinforce immediately | |
Watches from distance | Tolerance | Good enough! Narrate positively | |
Touches own materials only | Parallel play | Accept — narrate "You're both playing" | |
Backs away | Avoidance | Reduce proximity, parallel only |


- Verbal: "Yes! You looked at [peer name]! Beautiful!"
- Physical (if appropriate): high-five, shoulder pat
- Token: place star on reward chart immediately
- Preferred item access: "Good playing — you can have [preferred item] now"
- ❌ "Why aren't you talking to [peer name]?"
- ❌ Comparing to peers who play more naturally
- ❌ Ending session on a failure
- ❌ Making reinforcement unpredictable

- Did child seem more or less tense during cool-down vs. start? (data point)
- Any spontaneous behavior toward peer during wind-down?
- Child's regulation state post-session (for readiness calibration next time)

What Gets Measured Gets Improved — Track These 5 Data Points
Step 6 of 6 Duration: 5 minutes post-session Data Point What to Record Example Peer orientation events How many times did child look at/toward peer? "3 glances" Proximity tolerance Minimum distance maintained comfortably "5 feet" Interaction type Parallel / Near-parallel / Structured / Spontaneous "Parallel" Reinforcement taken Did child accept tokens/praise? "Yes — 4 tokens" Session length completed How long before first resistance? "12 minutes" 📊 GPT-OS® Tracking: Enter these data points into your GPT-OS® EverydayTherapyProgramme™ tracker to sync with your child's Social Participation Index. TherapeuticAI® will adjust protocol recommendations based on weekly trend data. pinnacleblooms.org/track/C-301 "You don't need clinical precision — a voice memo in the car is enough. 'Today he looked at the peer twice. 12 minutes before he moved away.' That's your data." 📞 9100 181 181 — Ask about our FREE AbilityScore® tracking setup
Challenge | Likely Cause | Solution | |
Child leaves the room entirely | Overwhelm, wrong readiness state | Run parallel only tomorrow. Check the Readiness Gate more carefully. | |
Peer becomes too loud/physical | Unpredictable peer | Pre-brief peer better (Material 8). Choose quieter peer. | |
Child fixates on solo activity, ignores peer | Normal — this IS the presenting challenge | Introduce cause-effect element: make peer necessary for preferred activity | |
Child takes peer's materials aggressively | Social script deficit — no 'asking' pattern | Pause. Teach the "Can I have it?" script. Role play. | |
Child seems more distressed post-session | Possible anxiety component, not just motivation deficit | Consult professional — may need anxiety assessment | |
No progress after 4 weeks | Protocol may need individualization | Call 9100 181 181 — ABA specialist will review your log | |
Peer refuses to continue as buddy | Buddy burnout | Rotate peers. Ensure peer is also having fun (not just serving) |
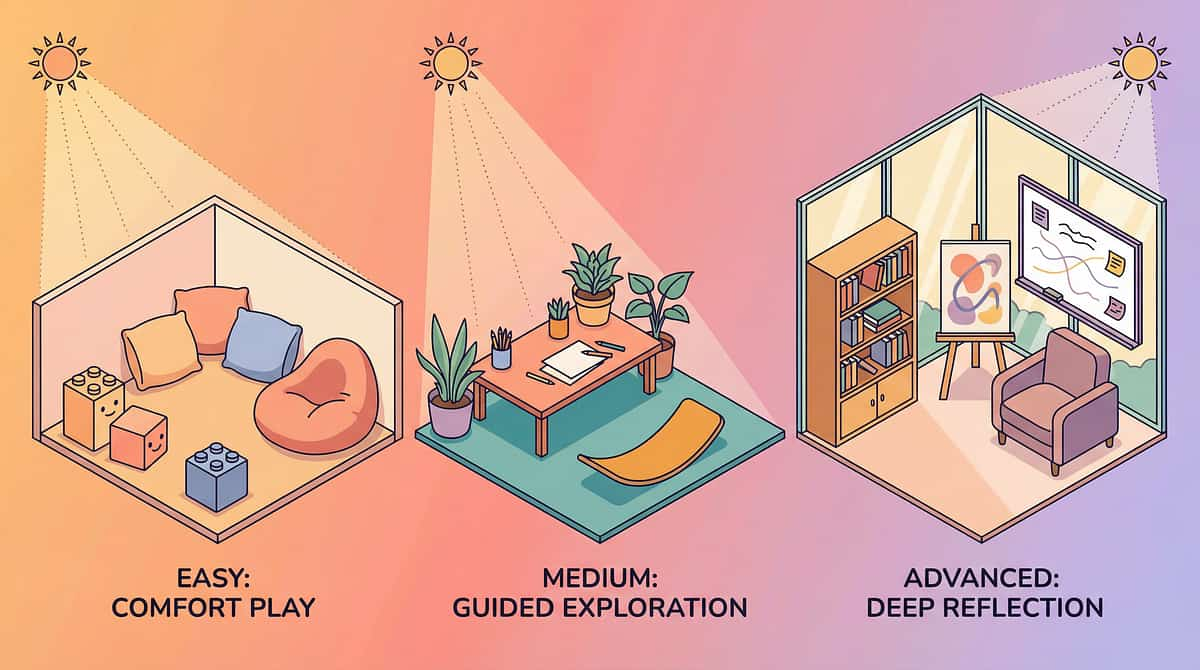
One Protocol, Infinite Personalizations — Find Your Child's Version
Difficulty Calibration Easier 10 min parallel only | No interaction required | Single familiar peer | Strongest interest only Standard 15–20 min structured | Prompted interaction | 1–2 familiar peers | Preferred interest Harder 30 min full cooperative | Scripted peer dialogue | Small peer group | Flexible interests Sensory Profile Adaptations Profile Adaptation Sensory Avoider Maximum personal space, minimal peer sound, very short sessions, gradual proximity increase Sensory Seeker High-energy cause-effect toys, physical games, movement-based peer activities Auditory Sensitive Quiet indoor setting, whisper-voice peers, avoid noisy toys Visual-Spatial Strength Block building, puzzle completion, visual-heavy structured games Age Modifications Ages 3–5 Parallel play emphasis, parent as mediator, 10-minute maximum Ages 6–8 Structured games, script cards, buddy program introduction Ages 9–12 Interest clubs, script internalization, gradual peer group expansion
Your Home Protocol — Save This Card
Fill in this personalized protocol card and post it on your refrigerator. Consistency across all caregivers multiplies therapeutic impact significantly. Child Profile Child Name: ____________ | Age: ______ | Start Date: ________Strongest Special Interest: ________________________Primary Material (from 9): ________________________Peer Partner Name: ____________ | Session Time: ________ Session Parameters Session Length: _____ minutes | Reinforcer: _____________Tracking Method: _____________________ Week-by-Week Goals Week 1–2: Child tolerates peer in same room for 10 minWeek 3–4: Child glances at peer 3+ times per sessionWeek 5–6: Child participates in structured game 10 minWeek 7–8: Child uses approach script spontaneously once My Helpline 📞 9100 181 181Free consultation available 24×7 | 18+ languages ⚕️ Protocol template developed by Pinnacle Blooms Consortium — CRO, BCBA, SLP, OT, SpEd, NeuroDev Pediatrics
- Child tolerates peer in room without leaving → PROGRESS
- Child glances at peer even once → PROGRESS
- Child allows session to reach 8–10 minutes → PROGRESS
- Child accepts reinforcement for peer-adjacent behavior → PROGRESS
- No increase in distress compared to first session → PROGRESS
- Spontaneous initiation toward peer
- Verbal exchange with peer
- Sharing materials voluntarily
- Requesting peer by name
"In Weeks 1–2, you will question whether anything is happening. It is. Neural exposure pathways are forming. Tolerance is being built. If your child tolerates the peer's presence for 3 seconds longer than last week — that is real, measurable neurological progress."

Weeks 3–4: The Neural Pathways Are Strengthening — Watch for These Signs
Phase: Consolidation Progress: 40% Anticipation Signal Child ANTICIPATES peer arrival — looks toward door or moves toward play area before peer arrives. The brain is forming stable representations of "peer = expected/safe." Session Duration Growth Child accepts 12–15 minute sessions without resistance. Peer presence no longer triggers visible avoidance — peer has become a neutral, familiar stimulus. First Vocalizations ANY spontaneous vocalization in peer's direction — even a single sound, word, or comment not directed at you — is a significant synaptic consolidation signal. When to Increase Intensity Child reaching session length without resistance → Extend by 5 minutes Distance comfort established → Reduce distance between children by 1 foot Structured game tolerance shown → Introduce second game option "You may notice YOU are more confident too. Your calibration is improving. You are reading your child's signals more accurately. That is co-regulation — and it matters."

"Mastery for this child may mean Level 2 — and that is clinically valid success. We do not set neurotypical friendship as the only acceptable outcome. We set the child's own developmental growth as the benchmark." — GPT-OS® Clinical Note
- Complete regression in previously present social interest (sudden increase in avoidance)
- Active distress (panic, self-harm, aggression) specifically triggered by peer presence
- No positive response to ANY of the 9 materials after 10 consistent sessions
- Signs of depression (loss of interest in special interests, sleep/appetite changes)
- No attachment to any person including primary caregivers
- Stagnation at same level for 4+ weeks with consistent implementation
- Peer buddy showing frustration or reluctance
- Parent reporting extreme difficulty maintaining sessions
- Child showing anxiety symptoms (not just motivation deficit)
- 🔗 C-300: Joint Attention
- 🔗 C-302: Imaginative Play
- 🔗 C-310: Making Friends
- 🔗 B-198: Conversation Initiation
- 🔗 C-322: Building Empathy

After: At his cousin's birthday, approached another child building with Lego — his special interest — and said: "Can I build too?" First peer initiation ever witnessed by parents.
After: Now seeks out her neighbor's daughter specifically when she wants to play the matching game. Asks for her by name. She has a friend — by her own definition.
"These outcomes are not extraordinary — they are the expected result of consistent, structured implementation. The brain's capacity to build social reward associations does not disappear in autism — it requires a different pathway to activate." — Pinnacle BCBA Consortium

"You found this page because you noticed. Because you are paying attention. Because you refuse to accept that your child must remain isolated while the world connects around them. That attention — that refusal — is where every breakthrough starts."
Get a free social development consultation with a Pinnacle specialist
pinnacleblooms.org/ability-score
techniques.pinnacleblooms.org/download/C-301
Preview of 9 materials that help when child shows no peer interest Therapy Material
Below is a visual preview of 9 materials that help when child shows no peer interest therapy material. The pages shown help educators, therapists, and caregivers understand the structure and content of the resource before use. Materials should be used under appropriate professional guidance.






techniques.pinnacleblooms.org