When Your Child Can't Stop Jumping — Their Body Isn't Misbehaving. It's Speaking.
He bounces before breakfast. He jumps off the couch, the table, the back of the sofa. At school, the teacher says he can't sit still. His body is driven by something you can't see — something more powerful than his ability to control it. You are not failing. Your child's nervous system is speaking. And what it's saying is: "I need this input to feel regulated."
Technique A-088
Sensory Solutions Series
Ages 2–12

You Are Not Alone — The Numbers
Millions of families worldwide are watching their child jump, bounce, crash, and climb — wondering if something is wrong. Nothing is wrong. Something is different. And that difference has a name, a science, and solutions.
80%
Sensory Difficulties in Autism
Of children diagnosed with autism display sensory processing difficulties including intense proprioceptive and vestibular seeking behaviours such as compulsive jumping (PRISMA Systematic Review, 2024).
1 in 36
Children Diagnosed with ASD
In the United States. In India, prevalence estimates range from 1 in 68 to 1 in 100 — meaning millions of families navigate sensory seeking challenges every single day.
20M+
Pinnacle Therapy Sessions
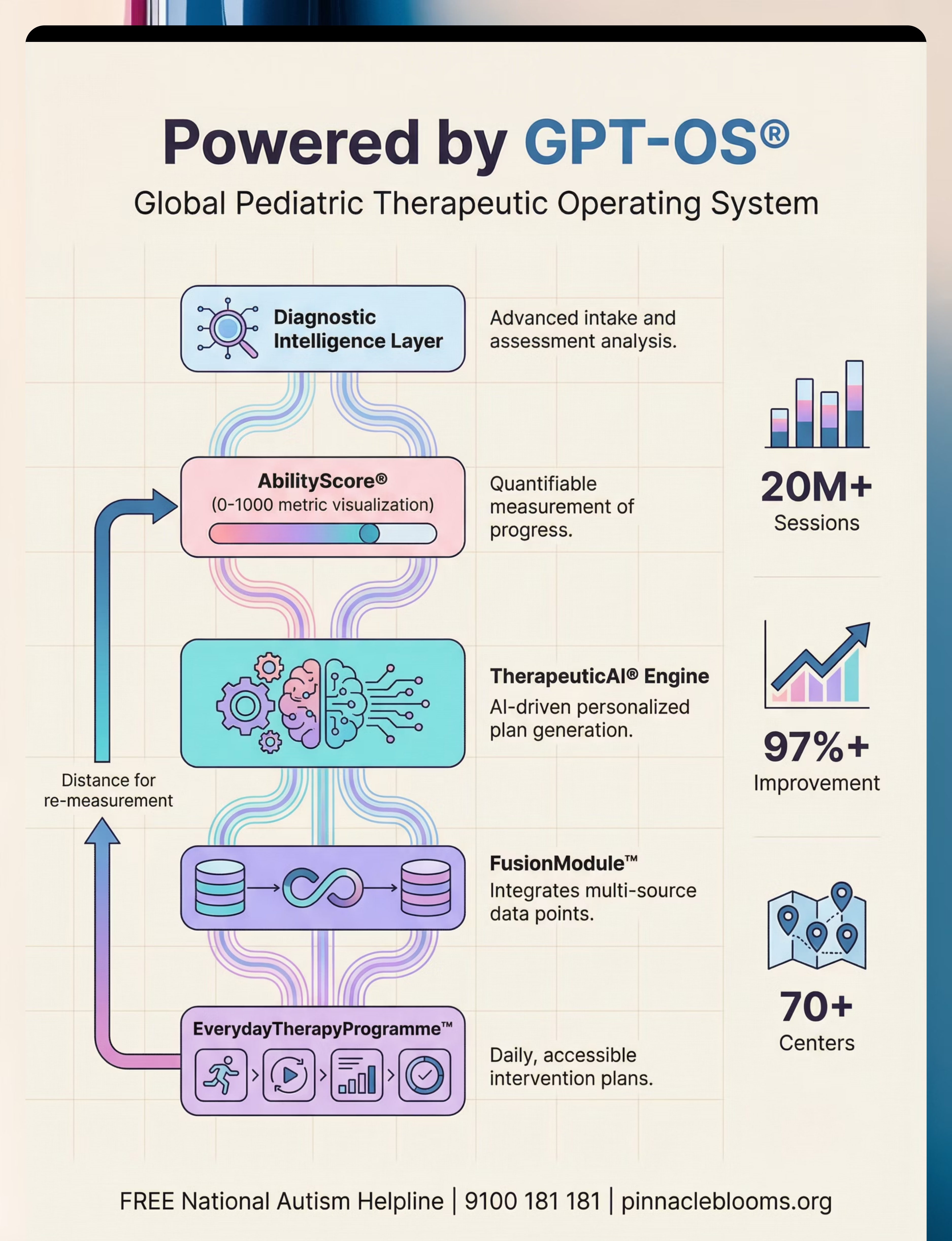
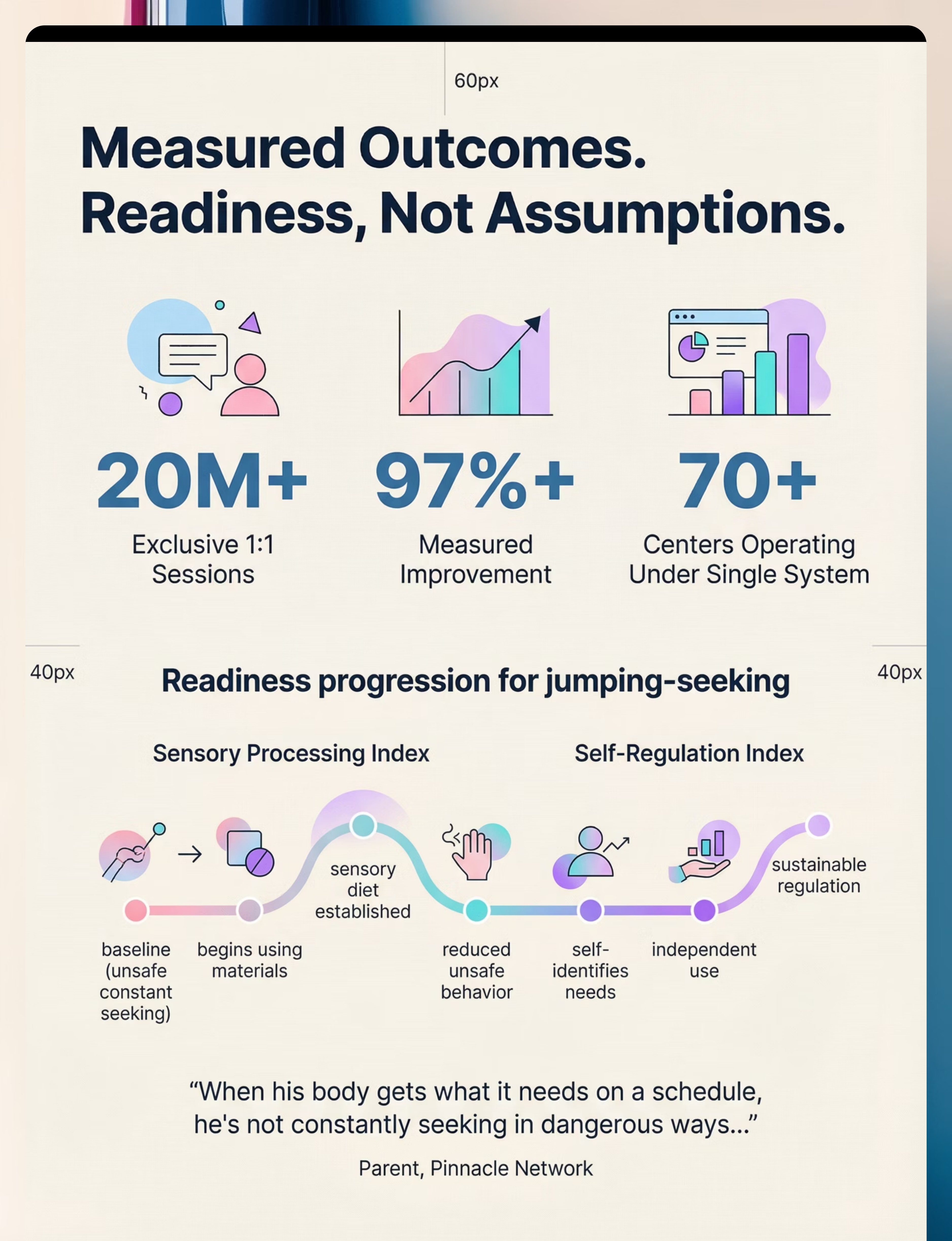
The Pinnacle Blooms Network has delivered 20M+ exclusive 1:1 therapy sessions addressing sensory processing challenges with 97%+ measured improvement rates across 70+ centres.
Proprioceptive seeking — the drive for deep pressure, joint compression, and heavy impact — is among the most common sensory modulation patterns in paediatric populations, affecting both diagnosed and undiagnosed children.

What's Happening in Your Child's Brain
The Proprioceptive System
Tells your child where their body is in space and how much force they're using. Receptors in muscles, joints, and tendons send this information to the brain. When your child jumps, the landing impact sends a massive wave of proprioceptive data — joint compression, muscle loading, tendon stretch — flooding the brain with the input it craves.
The Vestibular System
Lives in the inner ear and detects movement, acceleration, and head position. When your child is airborne, this system activates intensely — position change, acceleration, gravity shifts — all providing the movement sensation the brain requires.
Why Jumping Is So Compelling
Jumping is neurologically efficient because it delivers both proprioceptive AND vestibular input simultaneously. The airborne phase feeds the vestibular system. The landing feeds the proprioceptive system. One activity — two regulatory systems served.
The High Threshold
Your child's nervous system has a higher-than-typical threshold for these inputs. It takes more proprioceptive and vestibular input than average for their brain to register "enough." This is why the jumping seems compulsive — the nervous system is driving the behaviour to meet a genuine neurological need.
This is a wiring difference, not a behaviour choice. Not defiance. Not ADHD alone. Not bad parenting. Neurophysiology.
Where This Sits in Development
Your child is on a clear developmental map. This is not a deficit — it is a waypoint in a journey with a clear forward path. Proprioceptive and vestibular seeking commonly co-occurs with attention differences, motor planning challenges, and anxiety. These are interconnected features of the same neurodevelopmental profile.
1
0–12 Months
Basic proprioceptive awareness develops through tummy time, rolling, and crawling. Foundation of body awareness forming.
2
12–24 Months
Walking, climbing, beginning to jump. Early movement seeking may emerge — bouncing and climbing intensifies.
3
2–3 Years
Jumping-seeking often becomes apparent — constant bouncing, jumping off furniture begins. Peak parental concern window.
4
3–5 Years
Peak identification window — compulsive jumping, crashing, and risk-taking movement behaviours are clearly visible.
5
5–8 Years
Functional impact zone — jumping-seeking conflicts with school demands for stillness and sustained attention.
6
8–12 Years
Self-awareness opportunity — child can begin to understand and self-manage their own sensory needs with guidance.

The Evidence Behind These Materials
Evidence Grade
Level I–II
Systematic Reviews + Randomised Controlled Trials
24+ studies across systematic reviews and meta-analyses confirm sensory integration intervention meets evidence-based practice criteria for children with autism spectrum disorder (PRISMA 2024).
Indian Evidence: Home-based sensory interventions demonstrated significant outcomes in Indian paediatric populations (Padmanabha et al., Indian Journal of Pediatrics, 2019), validating that parent-administered sensory protocols produce measurable developmental improvement.
Key Findings
Sensory integration therapy using proprioceptive and vestibular input materials — including trampolines, crash pads, weighted items, therapy balls, swings, and heavy work activities — effectively promotes:
- Sensory processing and self-regulation
- Social skills and adaptive behaviour
- Motor development (gross and fine)
- Attention and classroom participation
The Sensory Diet Approach
A scheduled, proactive approach to delivering sensory input throughout the day — the "sensory diet" model — has the strongest clinical consensus as the framework for deploying these materials effectively.
Clinically validated. Home-applicable. Parent-proven.

Sensory Materials for Jumping-Seeking Behaviour
Parent-Friendly Name: "Meeting the Jumping Need Safely"
This intervention technique deploys 9 evidence-based therapeutic materials to safely meet the proprioceptive and vestibular input needs that drive compulsive jumping behaviour in children. Rather than attempting to stop the jumping, this approach channels the neurological need through designated safe outlets, scheduled proactively as a "sensory diet" to maintain baseline regulation and reduce unsafe seeking behaviour.
Domain
Sensory Processing | Proprioception | Vestibular Processing | Self-Regulation
Age Range
2–12 years across home, school, therapy, and outdoor settings
Frequency
Daily sensory diet implementation; individual material use as needed throughout the day
Duration
10–30 minutes per material session; sensory diet spans the full day

Who Uses These Materials — The Consortium Disciplines
This technique crosses therapy boundaries because the brain doesn't organise by therapy type. Four disciplines converge to deliver comprehensive support for the jumping-seeking child.
Occupational Therapy (OT) — Primary Lead
OTs are the primary specialists for sensory processing assessment and intervention. They evaluate the child's full sensory profile, design individualised sensory diets, and train parents on correct material usage, environmental setup, and progression protocols.
Applied Behaviour Analysis (ABA)
BCBAs integrate sensory materials into behavioural programming, replacing unsafe seeking behaviours with functional alternatives. Reinforcement schedules support consistent material use and generalisation across settings.
Special Education (SpEd)
Special educators implement classroom-based sensory strategies — therapy ball seating, heavy work classroom jobs, scheduled movement breaks, weighted lap pads — enabling the jumping-seeking child to participate in academic activities.
NeuroDevelopmental Paediatrics
NeuroDev paediatricians assess the broader neurodevelopmental picture — differentiating proprioceptive seeking from ADHD hyperactivity or anxiety-driven movement — ensuring the right systems are targeted and ruling out conditions requiring medical intervention.
What These Materials Target
When proprioceptive and vestibular needs are met safely and proactively, the ripple effects reach every domain of development. Observable indicator for the primary target: reduced frequency and intensity of unsafe jumping-seeking behaviour within 2–8 weeks of consistent sensory diet implementation.

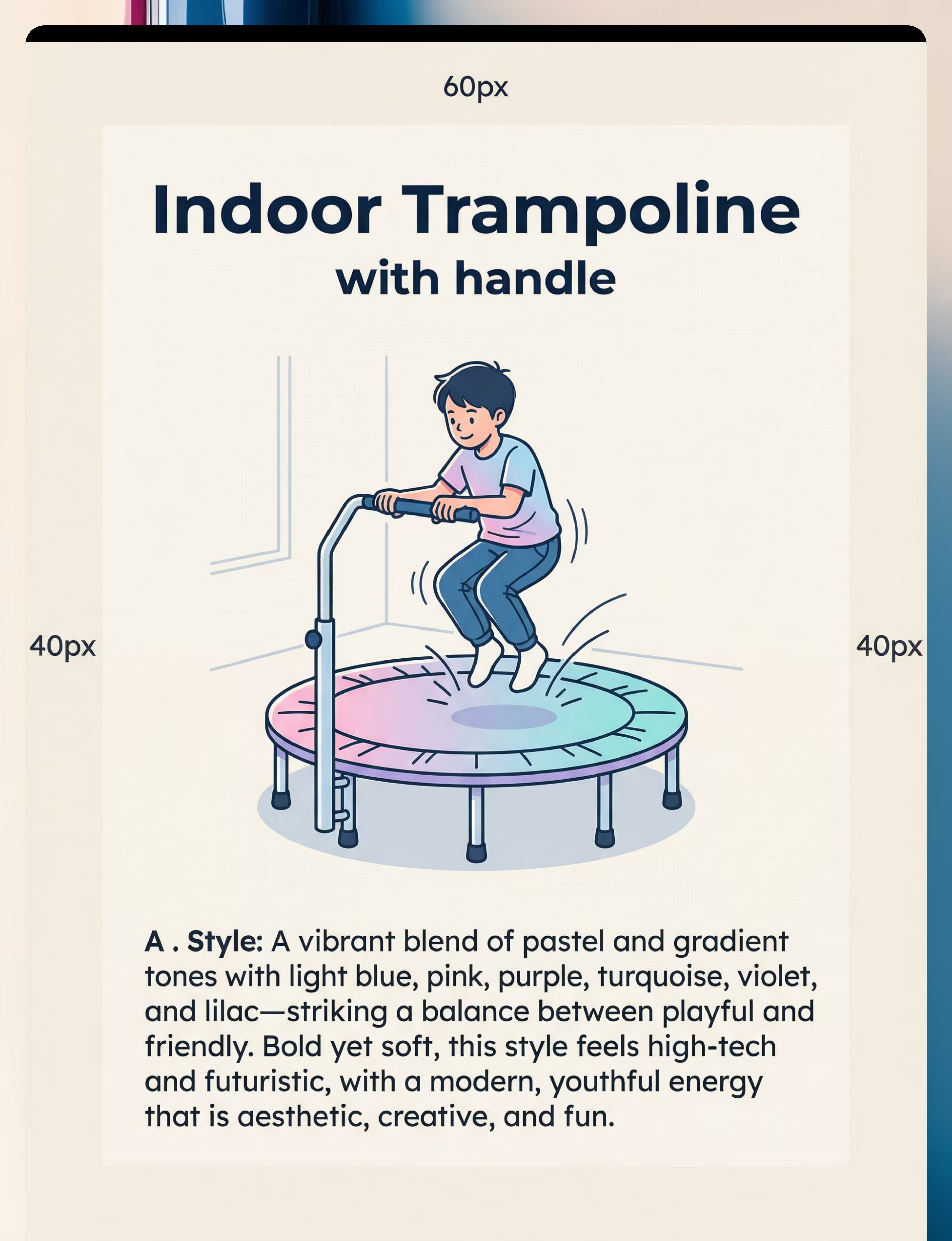
Material 1 — Indoor Trampoline with Handle
Canon Material 1 of 9
Proprioceptive + Vestibular
What It Is
A small indoor trampoline (typically 36–40 inches diameter) with a vertical stability handle, designed for single-child use indoors. Anti-burst construction, non-slip rubber feet, weight-rated for children.
Price Range (INR)
₹2,000–8,000
Best ROI Rating
⭐⭐⭐⭐⭐ — Single best investment for jumping-seekers
Why It Works
The trampoline is the most neurologically complete solution for jumping-seeking behaviour. Every bounce delivers simultaneous proprioceptive input (joint compression on landing) and vestibular input (airborne acceleration and position change). It creates a designated "yes" space for jumping — a legal, safe outlet that begins to replace unsafe furniture jumping when introduced proactively.
How to Use
- Place in a cleared area, minimum 3 feet from walls in all directions
- Handle must be gripped during initial sessions
- 5–15 minutes of rhythmic bouncing per session
- Count jumps together, sing to a bouncing beat, play jump-and-freeze

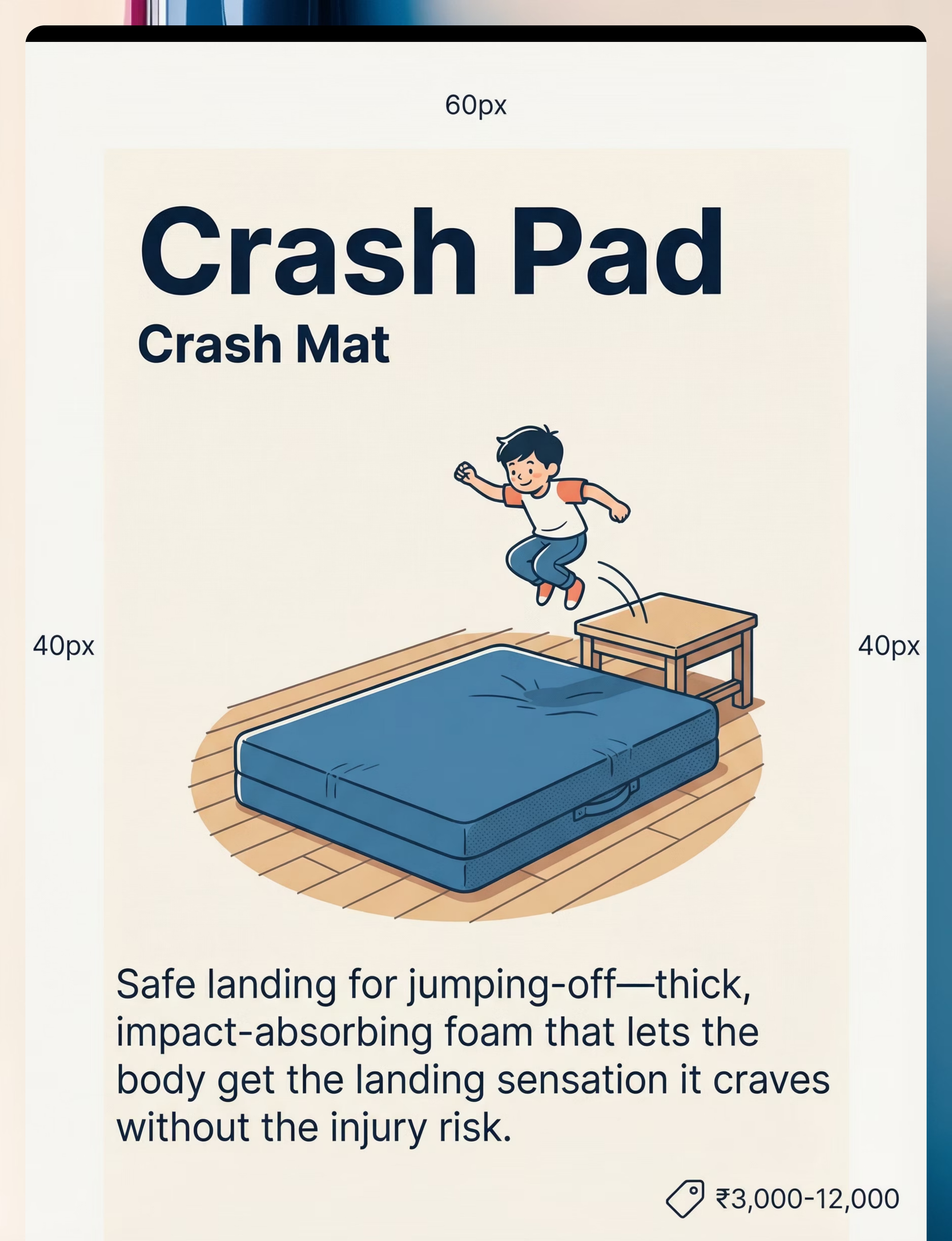
Material 2 — Crash Pad / Crash Mat
Canon Material 2 of 9
Proprioceptive Impact
What It Is
A thick, dense foam mat (4–8 inches depth) with a durable fabric cover, designed to absorb the impact of children jumping or falling onto it safely.
Price Range (INR)
₹3,000–12,000
DIY Alternative
Layer multiple thick mattress toppers, folded comforters, or couch cushions in a corner. Not as dense as commercial pads, but dramatically safer than hard floors.
Why It Works
The crash pad addresses the child's drive to jump from height — one of the most dangerous expressions of jumping-seeking. By positioning the crash pad adjacent to a low, safe surface (such as a sofa or step), you create a designated jump-and-land circuit. The deep foam absorbs impact while delivering intense proprioceptive input through the full-body landing.
How to Use
- Position against a wall corner for containment and safety
- Designate one safe jumping surface (low step, sofa edge)
- 10–20 repetitions per session — forward jump, belly flop, cannonball
- Celebrate the landing: "What a crash! Your body loved that!"

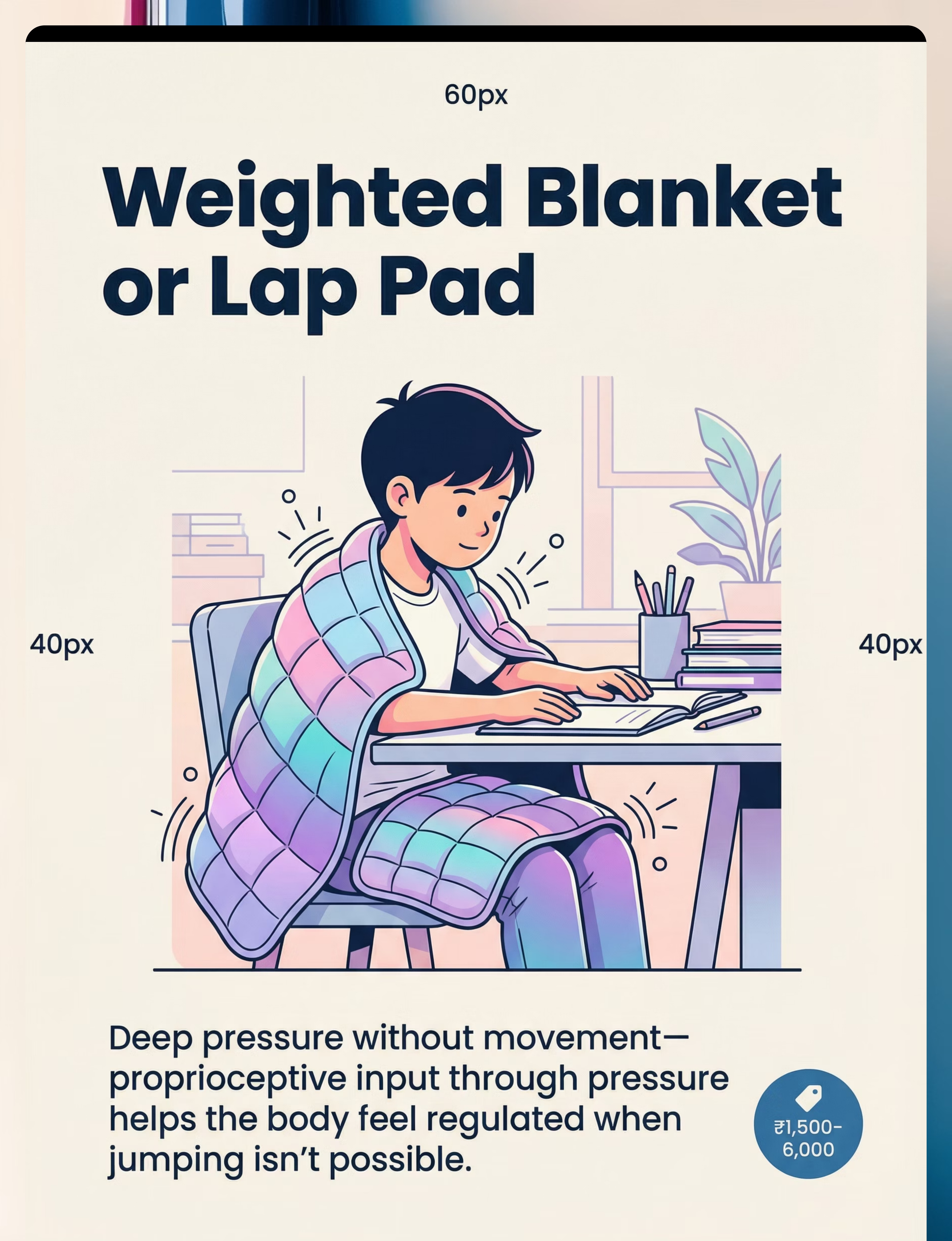
Material 3 — Weighted Blanket or Lap Pad
Canon Material 3 of 9
Deep Pressure Proprioception
What It Is
A blanket filled with glass beads or poly pellets, providing consistent, evenly distributed weight across the body. Lap pad version covers only the lap and thighs for seated use.
Price Range (INR)
₹1,500–6,000
Safety Rule
Weight must not exceed 10% of child's body weight. Child must be able to remove independently. Never cover face or airway.
Why It Works
When jumping isn't possible — during meals, homework, car journeys, or bedtime — the weighted blanket or lap pad delivers proprioceptive input through sustained deep pressure. This activates the same joint receptors and calming neural pathways as jumping, in a socially and situationally appropriate format. Many children who resist sitting for meals or homework will sustain attention significantly longer with a weighted lap pad.
How to Use
- Drape across lap or shoulders during seated activities
- Use for 15–30 minutes during homework, meals, or screen time
- Observe: does the child settle? Fidget less? Sustain attention longer?
- Introduce at bedtime as a sleep-regulation tool

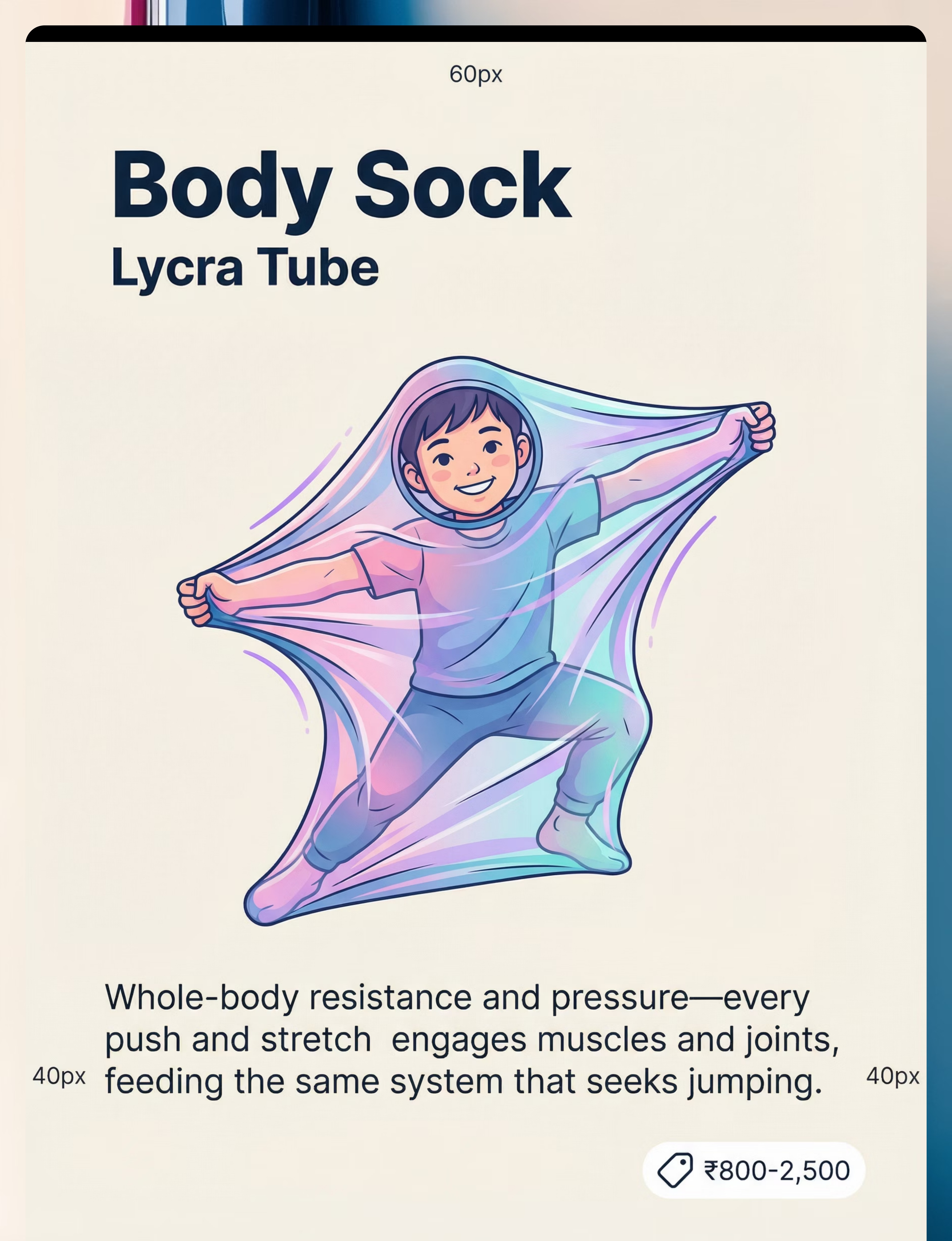
Material 4 — Body Sock / Lycra Tube
Canon Material 4 of 9
Resistance and Containment
What It Is
A large stretchy tube made from Lycra or spandex fabric, open at both ends. The child climbs inside and uses their body to push, stretch, and resist the fabric in all directions.
Price Range (INR)
₹800–2,500
DIY Alternative
A large pillowcase with a head hole cut — upper body resistance play. A stretchy sleeping bag provides similar resistance and containment.
Why It Works
The body sock provides whole-body proprioceptive input through resistance — every movement the child makes is met with the fabric pushing back. This 360-degree deep pressure and resistance is highly organising for the nervous system, particularly for children who seek both impact (jumping) and containment (squeezing into small spaces). Unlike the trampoline, the body sock can be used in quieter, calmer settings — it bridges high-energy and low-energy environments.
How to Use
- Face must remain uncovered — breathing unobstructed at all times
- Child must be able to exit easily — check before starting
- 5–10 minutes of pushing, stretching, and rolling inside the sock
- Combine with music or counting for engagement

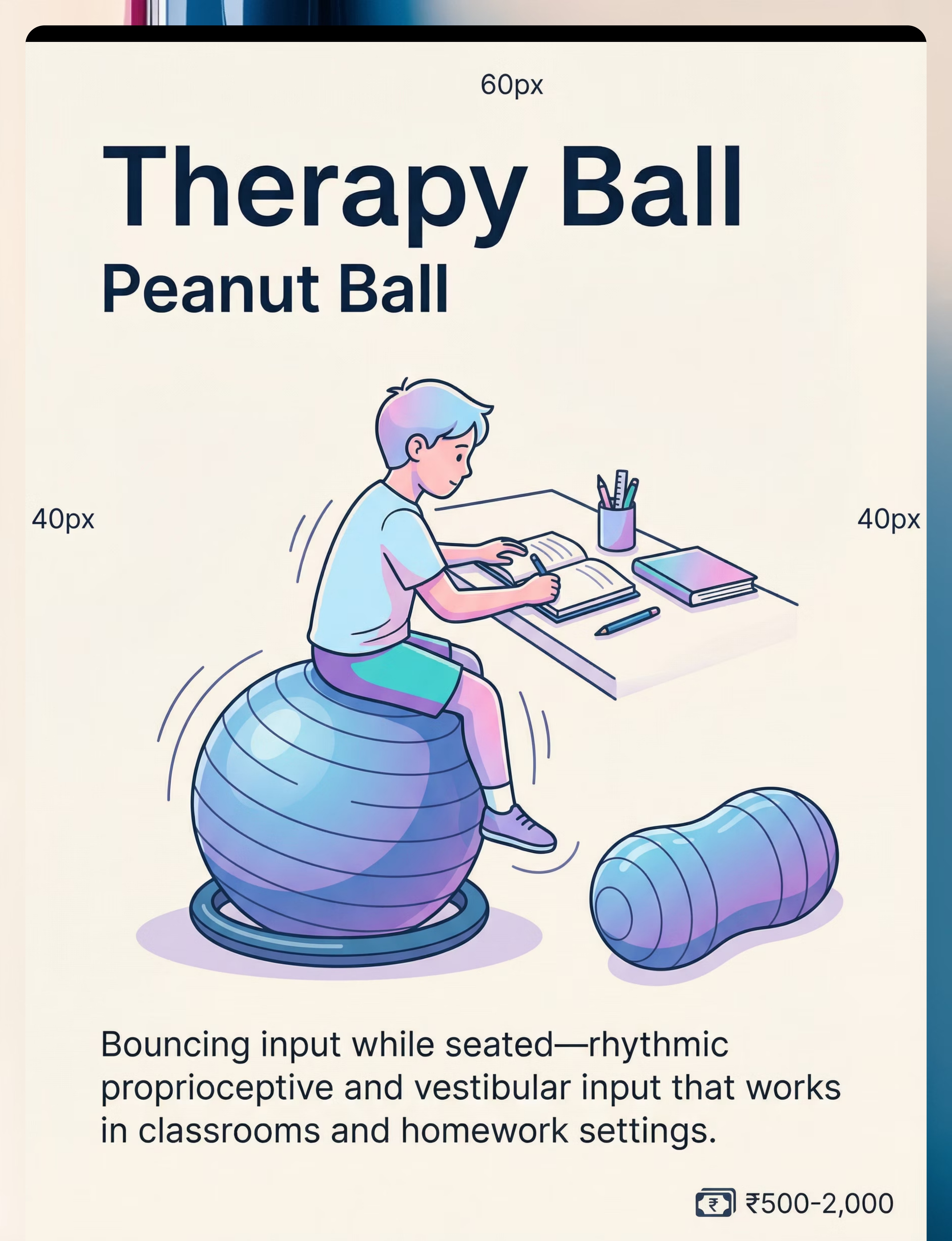
Material 5 — Therapy Ball / Peanut Ball
Canon Material 5 of 9
Active Seating
What It Is
A large inflatable ball (round or peanut-shaped) used as a dynamic seating surface. Size is selected by child's height — hips and knees should be at 90° when seated. Anti-burst construction essential.
Price Range (INR)
₹500–2,000
Size Guide
Ages 2–4: 45cm | Ages 4–8: 55cm | Ages 8–12: 65cm. Use a fabric ring base to prevent rolling when unoccupied.
Why It Works
The therapy ball is the most classroom and homework-compatible material in this toolkit. The unstable surface requires constant micro-adjustments from core muscles — continuous proprioceptive input that keeps the nervous system engaged without requiring the child to leave the table. Children who bounce and fall off chairs while seated on standard furniture often sustain significantly longer periods of table-top work when using a therapy ball. This is not fidgeting — it is proprioceptive fuelling.
How to Use
- Introduce during homework or meals — not free play initially
- Allow gentle bouncing while working — this is the goal, not a distraction
- 10–20 minutes of active sitting per session
- Transition back to standard chair when introducing new, demanding tasks

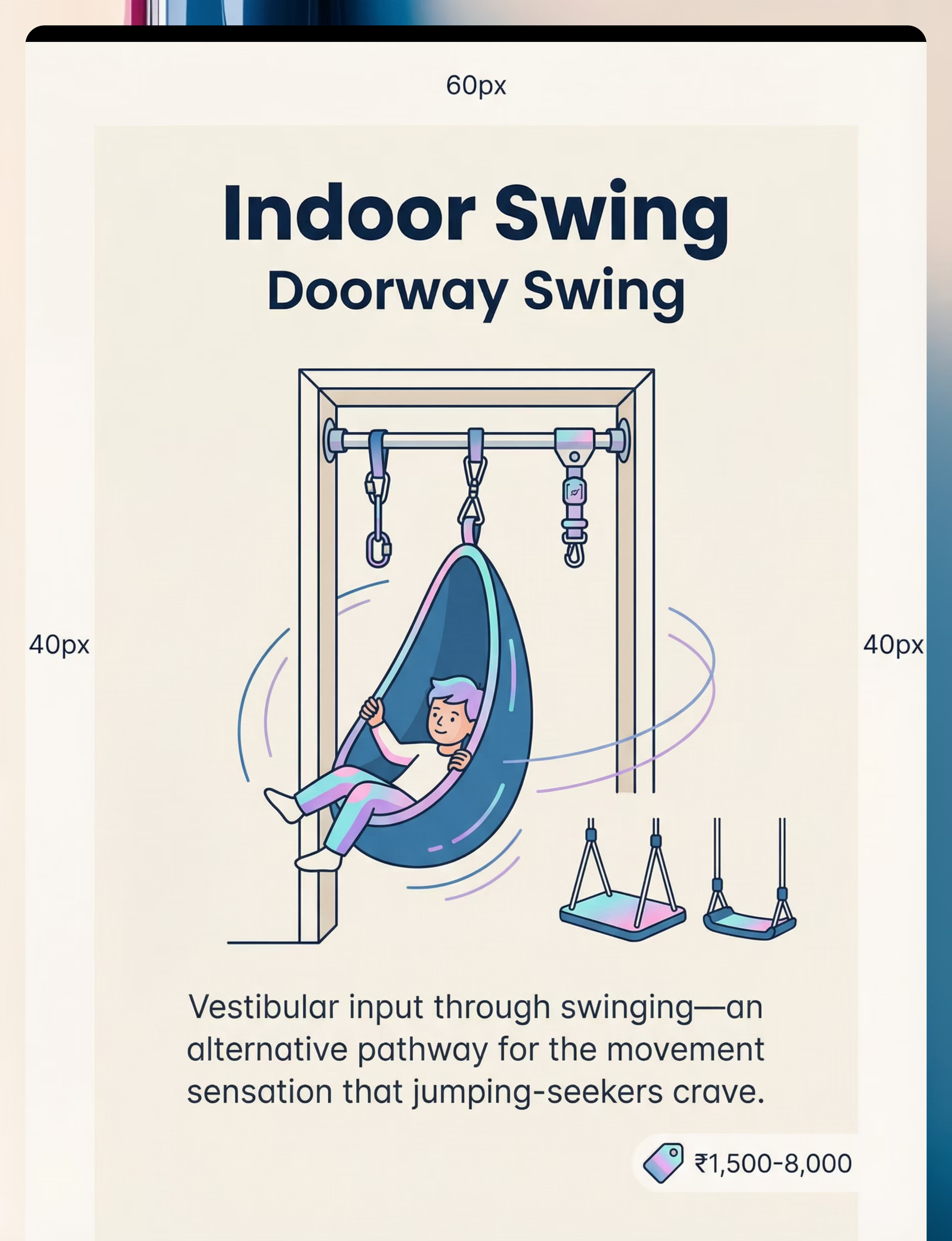
Material 6 — Indoor Swing / Doorway Swing
Canon Material 6 of 9
Vestibular Input
What It Is
A fabric or platform swing mounted in a doorway frame or from a ceiling stud mount. Provides rhythmic, repetitive vestibular input through back-and-forth or side-to-side movement.
Price Range (INR)
₹1,500–8,000
Installation Safety
Ceiling mount into structural studs only — never drywall alone. Verify weight limits before first use. Full swing arc must be clear of furniture.
Why It Works
The indoor swing targets the vestibular component of jumping-seeking specifically. While the trampoline and crash pad emphasise proprioceptive impact, the swing provides linear movement input that is calming and organising to the vestibular system. For children who become over-stimulated by high-impact activities, or whose jumping-seeking has a strong "movement craving" component (rather than impact craving), the swing may actually be more regulating than the trampoline. Linear movement (forward-back) is calmer than rotational — always start there.
How to Use
- 5–15 minutes of rhythmic linear swinging per session
- Parent provides gentle, rhythmic push — let the child set the rhythm
- Avoid spinning — linear only for calming effect
- Use as transition tool before homework or bedtime

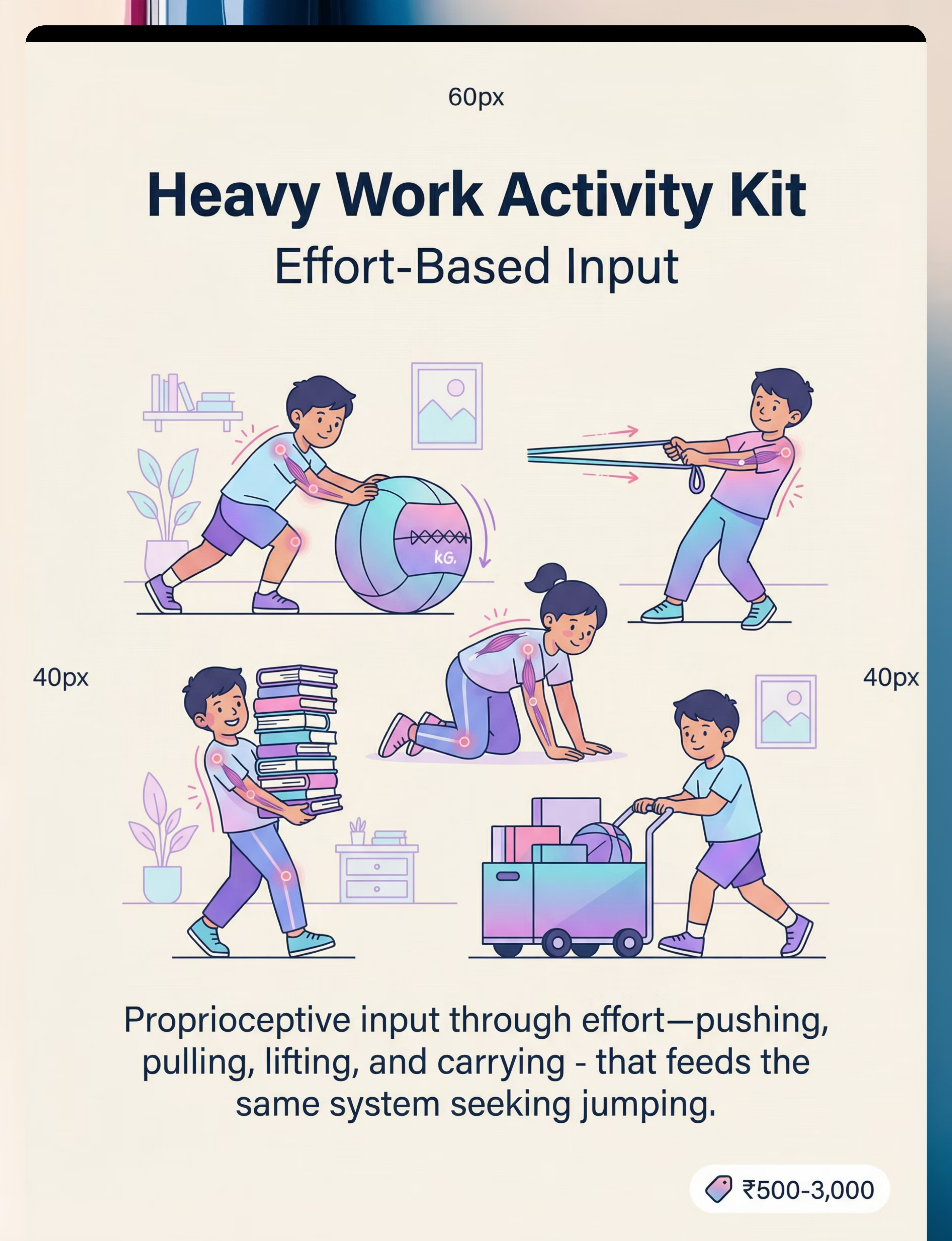
Material 7 — Heavy Work Activity Kit
Canon Material 7 of 9
Proprioceptive Loading
What It Is
A collection of activities and tools requiring sustained muscular effort — pushing, pulling, lifting, and carrying. Can be formalised with resistance bands, medicine balls, and weighted backpacks, or implemented entirely through household activities.
Price Range (INR)
₹500–3,000 (or completely free with household activities)
Zero-Cost Heavy Work
Carrying groceries, pushing furniture, digging in yard, sweeping with heavy broom, moving laundry baskets, filling a backpack with books.
Why It Works
Heavy work delivers proprioceptive input through sustained muscular effort rather than impact — making it uniquely valuable for situations where jumping isn't appropriate. Pushing, pulling, and carrying activate the deep muscle and joint receptors that the nervous system craves, in a format that is socially acceptable, practically useful, and available anywhere. Heavy work also serves as an excellent pre-activity primer — 5 minutes of heavy work before a demanding seated task can extend the child's regulated window significantly. It is the most versatile material in the entire toolkit.
How to Use
- 5–10 minutes of sustained effort activities per session
- Match weight to child's ability — effortful but not straining
- Use before school, before homework, and during sensory diet transitions
- Teach proper lifting technique — back straight, legs driving

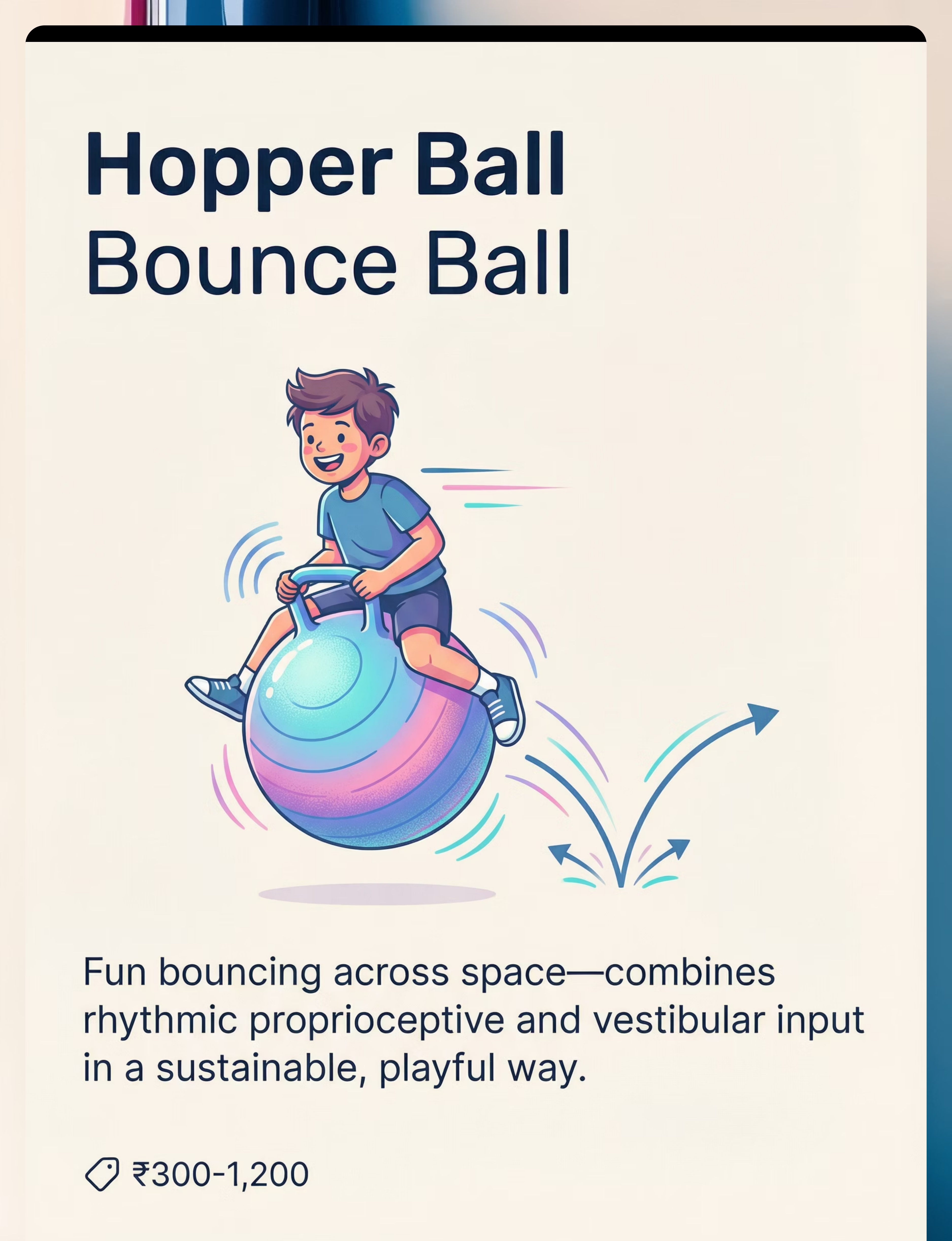
Material 8 — Hopper Ball / Bounce Ball
Canon Material 8 of 9
Movement Play
What It Is
A large inflatable ball with a handle grip, designed for children to sit on and bounce across a space. Provides rhythmic proprioceptive and vestibular input through forward-propelled bouncing movement.
Price Range (INR)
₹300–1,200
DIY Alternative
Bouncing play on a mattress on the floor, or couch cushions laid flat. Any bouncing surface provides similar input through rhythmic movement.
Why It Works
The hopper ball delivers input through fun, child-led play — making it one of the most motivating materials in the toolkit. The rhythmic bouncing while propelling across space combines proprioceptive input (landing impact through the seat and legs) with vestibular input (forward movement and position changes). Unlike the trampoline, the hopper ball allows the child to move through space — satisfying the "movement across the environment" component of vestibular seeking. It is also highly portable and can be used indoors or outdoors, making it ideal for settings where fixed equipment isn't available.
How to Use
- 5–10 minutes of bouncing across a clear indoor or outdoor space
- Create obstacle courses — bounce around cones, through doorways
- Race the parent across the room — social engagement layer
- Use as transition activity between structured tasks

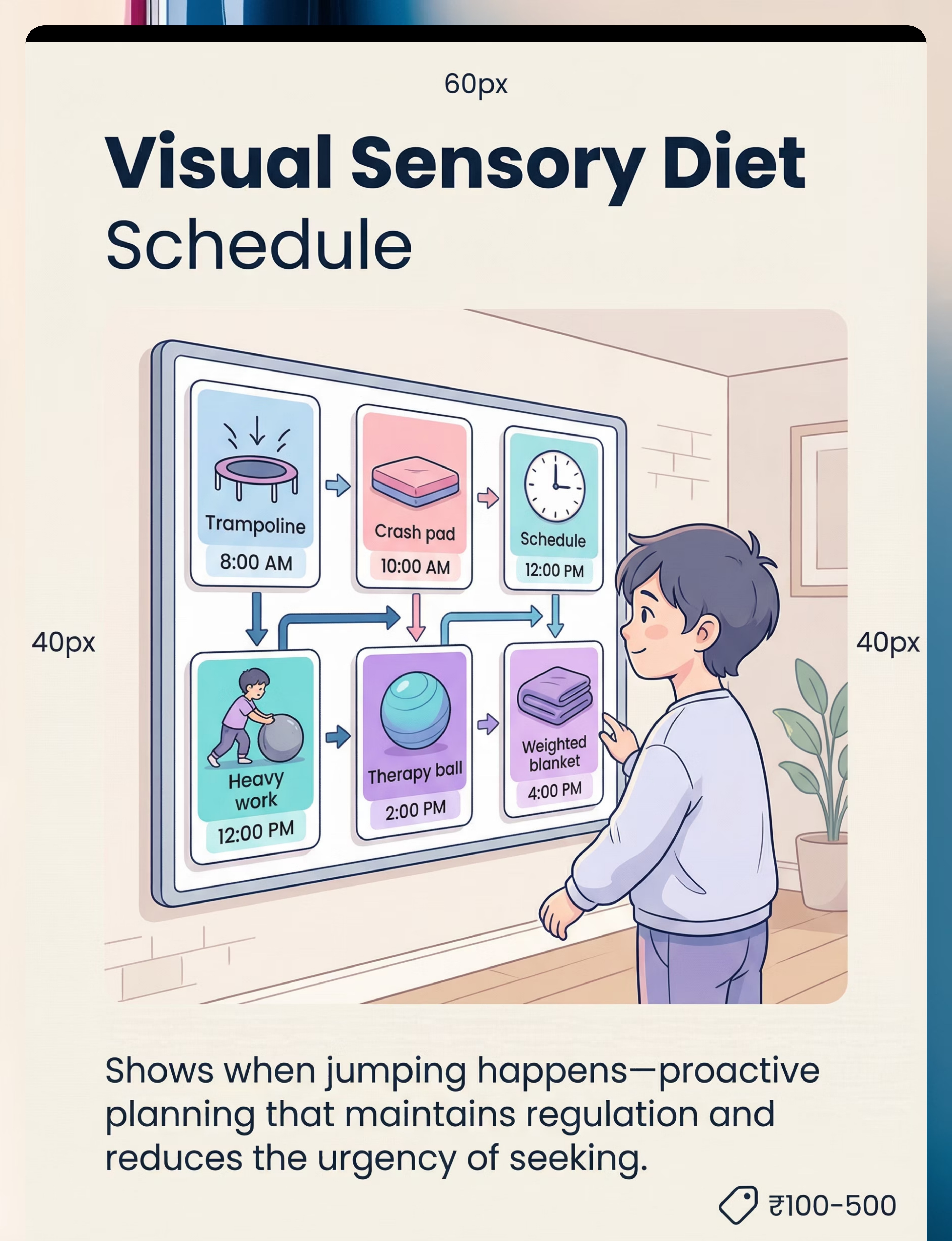
Material 9 — Visual Sensory Diet Schedule
Canon Material 9 of 9
Planning and Structure
What It Is
A visual chart — using pictures, photographs, or icons — that shows the child which sensory activities are scheduled and when throughout the day. Typically displayed at eye level in the movement zone.
Price Range (INR)
₹0–500 (can be homemade immediately)
DIY Option
Hand-drawn pictures on paper taped to the refrigerator. Simple list with checkboxes. Photos of activities in order. Costs nothing and works immediately.
Why It Works
The visual schedule is the architectural framework of the entire sensory diet — it is what transforms a collection of therapeutic materials into a coordinated, proactive system. Without it, sensory input is reactive (parent responds to unsafe jumping when it happens). With it, sensory input is proactive (the nervous system receives input before the seeking drive builds to an unsafe intensity). The schedule also serves as a powerful communication and self-regulation tool — over time, the child learns to anticipate and request their sensory activities, developing nascent self-advocacy skills for their own neurological needs.
How to Use
- Post at child's eye level in the movement zone
- Review schedule together at the start of each day
- Use Velcro or stickers to mark completed activities
- Build in 3–5 sensory sessions distributed across the waking day
DIY and Substitute Options — Start Today With What You Have
Not every family can order online. Not every village has same-day delivery. Every parent can start TODAY. This is the WHO/UNICEF inclusion principle in action.
Buy This | Make This (Zero-Cost) | Why the Substitute Works | |
Indoor Trampoline | Thick exercise mat or folded comforter on the floor as a designated "jumping zone" | Provides a safe, designated space and some impact absorption. The neurological principle — proprioceptive input — remains the same. | |
Crash Pad | Layer multiple mattress toppers, folded comforters, or couch cushions in a corner | Dramatically safer than hard floors. Dense layering approaches commercial foam density. | |
Weighted Blanket | Pillowcase filled with rice or dried beans, sewn shut. Heavy books in a backpack for brief wearing. | Deep pressure input is delivered by mass — household materials achieve this at zero cost. | |
Body Sock | Large pillowcase with head hole cut. Stretchy sleeping bag provides resistance and containment. | Resistance and containment are the therapeutic ingredients — fabric type is secondary. | |
Therapy Ball | Any large inflatable ball, partially deflated for stability. Fabric nest ring to keep in place. | The dynamic seating principle — unstable surface requiring core engagement — is preserved. | |
Indoor Swing | Blanket held by two adults (safe hammock swing). Outdoor playground swings are free and highly effective. | Vestibular input from linear movement is identical whether the platform is commercial or improvised. | |
Heavy Work Kit | Completely free: carrying groceries, pushing furniture, digging, sweeping, filling backpack with books | The therapeutic ingredient is muscular effort. Household activities are neurologically equivalent. | |
Hopper Ball | Bouncing on mattress on floor. Any bouncing surface provides rhythmic input. | Rhythmic proprioceptive input is the mechanism. Surface type is less important than the rhythm. | |
Visual Schedule | Hand-drawn pictures taped to refrigerator. Simple checkboxes. Photos of activities in sequence. | The scheduling and anticipation function is what matters — not the medium. |
When the clinical-grade material is non-negotiable: For children with significant safety risks from high-impact seeking, a proper indoor trampoline with handle provides stability and impact absorption that DIY alternatives cannot match. Consult your OT.
Safety First — Before You Begin
🔴 RED — Do NOT Proceed If:
Child has recent head injury or concussion. Unstable seizure disorder without medical clearance. Trampoline or swing hardware not securely installed. Weighted items exceed 10% of child's body weight. Face or airway could be obstructed by body sock or weighted blanket.
🟡 AMBER — Modify If:
Child has motor coordination difficulties — use handle. Low muscle tone — shorter sessions, more support. Recovering from injury — consult OT first. Signs of over-stimulation (flushing, giddiness) — reduce intensity. Child cannot verbally communicate distress — monitor closely.
🟢 GREEN — Proceed When:
Space is clear of obstacles. Equipment inspected and weight limits verified. Child is fed, rested, and in a regulated baseline state. Parent/caregiver is present and attentive. One child at a time on trampoline and swing.
RED LINE — Stop immediately if: Child shows sudden pallor, loss of consciousness, vomiting, unusual eye movements, or severe behavioural escalation beyond baseline. Seek medical attention.

Set Up Your Sensory Movement Zone
Your sensory movement zone is the physical infrastructure of the sensory diet. Set it up once, maintain it consistently, and it becomes the environmental anchor that helps your child associate their sensory materials with regulation — not restriction.
Environment Essentials
- Lighting: Natural or soft ambient — avoid fluorescent if child has visual sensitivity
- Sound: Low background noise. Some children regulate better with rhythmic music during movement
- Surface: Non-slip flooring or mat. Carpet preferred over hard surfaces for crash pad area
Remove From the Space
- Breakable items and glass surfaces
- Sharp-edged furniture within swing and trampoline radius
- Small objects on the floor
- Low-hanging lights and fixtures
- Pets from the active zone during sessions

Is Your Child Ready? — 60-Second Pre-Session Check
The best session is one that starts right. Run this check before every sensory diet session.
Child has eaten within the last 2 hours
Not too full, not hungry. Blood sugar stability supports regulation during sensory activities.
Child has slept adequately
Not overtired or just woken. Fatigue amplifies dysregulation and reduces sensory input tolerance.
Child is in a relatively regulated state
Not mid-meltdown, not post-crisis. The sensory diet prevents dysregulation; it does not rescue from it.
Equipment inspected and space cleared
Trampoline stable, crash pad positioned, swing hardware checked, hazards removed per setup card.
Parent/caregiver present and attentive
Not multitasking during active sessions. Full presence during trampoline and swing use is non-negotiable.
🟢 All YES → GO
Proceed to Step 1: The Invitation
🟡 1–2 Concerns → MODIFY
Use lower-intensity materials — weighted blanket, therapy ball — rather than high-impact options. Shorter session.
🔴 Dysregulated, Ill, or Distressed → POSTPONE
Offer calming activities: gentle rocking, weighted blanket, quiet space. Try again later today or tomorrow.
Step 1 — The Invitation
Step 1 of 6
Every session begins with an invitation, not a command. The child is brought into the activity through playful, low-demand engagement that matches their current energy and emotional state.
Say this for the trampoline: "Hey! Your body looks like it wants to move. Your trampoline is ready! Want to go bounce?"Say this for the crash pad: "I set up the crash pad. Want to do some big jumps?"Say this for the full sensory diet: "It's movement time! Let's look at your schedule — what's first today?"
Body Language Matters
- Lean toward the child with energy and enthusiasm
- Point toward the equipment with an inviting gesture
- Match the child's energy level — if they're already bouncing, be energetic too
- Keep voice warm and excited, not commanding or directive
Handling Resistance
- Child turns away: Move equipment closer, model bouncing yourself, add a preferred toy to the trampoline
- Child is occupied: Wait for a natural transition, offer movement as the next activity
- Child is distressed: This is not the time — go to calm-down alternatives and postpone
Timing: 30–60 seconds

Step 2 — The Engagement
Step 2 of 6
The child is now approaching the material. Deepen the interaction by introducing the therapeutic input deliberately and joyfully.
For the Trampoline
"Hold the handle and let's count your jumps! Ready? One... two... three..."
- Start with gentle bouncing — let the child find their rhythm
- Encourage hands on handle for safety
- Match their energy: "Big jumps! Your body is getting exactly what it needs!"
For the Crash Pad
"Stand on the cushion. Ready? Jump and CRASH!"
- Demonstrate the landing yourself if needed
- Show the child the safe landing zone: "Land right here — in the middle!"
- Celebrate the landing: "What a crash! Your body loved that!"
For the Weighted Blanket
"Here's your heavy blanket for homework time. Feel how it presses down? That's helping your body stay calm."
- Drape across lap or shoulders — let child adjust positioning
- Don't force — offer and observe response
Reinforcement cue: When you see engagement, label it: "Your body is bouncing so well! You look so regulated!" Specific, enthusiastic, immediate praise. Timing: 1–3 minutes.

Step 3 — The Therapeutic Action
Step 3 of 6
This is the core therapeutic event. The child is now actively receiving the proprioceptive and vestibular input their nervous system requires. Duration: 5–15 minutes of active input.
Trampoline Protocol
Sustained rhythmic jumping for 5–15 minutes, child-paced. Count jumps together. Sing songs with a bouncing rhythm. Play "jump and freeze" to build impulse control. Vary: high jumps, tiny bounces, two-foot and one-foot landings.
Crash Pad Protocol
10–20 repetitions per session. Jump from designated safe surface. Vary: forward jump, running jump, belly flop, cannonball. The landing impact is the therapeutic ingredient.
Therapy Ball Protocol
10–20 minutes of active sitting during homework, coloring, or eating. The instability engages core muscles continuously — gentle bouncing while working is the goal.
Weighted Blanket Protocol
15–30 minutes during seated activities. Child must be able to remove independently. Observe: does the child settle, become more focused, fidget less?
Concerning sign: If the child is escalating — movements becoming wild, unfocused, or showing signs of over-stimulation (flushed, giddy, losing control) — reduce intensity or transition to cool-down immediately.
Step 4 — Repeat and Vary
Step 4 of 6
Therapeutic dosage matters. Quality over quantity — 3 good repetitions are worth more than 10 forced ones. Maintain engagement by changing the game, not the neurological input.
Counting Games
"How many jumps to 50? Can you beat yesterday's number?" Builds numeracy while maintaining the rhythmic proprioceptive input.
Music Integration
Bounce to the beat. Freeze when music stops. The rhythm externalises the regulation — the child's body synchronises to an organising auditory input.
Simon Says Jumping
"Simon says... BIG jump! Simon says... tiny bounce! Simon says... FREEZE!" Builds impulse control within the proprioceptive input delivery.
Obstacle Course Circuit
Trampoline → crash pad → heavy work → therapy ball. Multi-material rotation within a single session for variety and sustained engagement.
Satiation indicators (the child has had enough): Movements slow naturally. Child spontaneously dismounts. Attention shifts to another activity. Yawning, relaxed posture. Child says "all done." When satiation happens, celebrate it: "Your body got exactly what it needed. Great listening to your body!"

Step 5 — Reinforce and Celebrate
Step 5 of 6
"You did amazing jumping today! Your body got what it needed and look how calm and focused you are now!""I love how you used your trampoline instead of the couch. That's such a safe choice!""You crashed SO WELL on the crash pad! Your body is getting so good at finding what it needs."
Immediate
Within 3 seconds of the behaviour you want to see more of. Delayed praise loses its neurological reinforcement value entirely.
Specific
Name the exact behaviour — "You jumped on the trampoline" not just "good job." Specificity builds the neural association you want.
Enthusiastic
Match the child's energy. Celebrate the movement, the effort, the self-regulation — not just the compliance.
Process-Focused
"You listened to your body" rather than "you sat still." Praise the process and the self-awareness, not the behavioural output.
"Celebrate the attempt, not just the success. The child who jumped on the trampoline 3 times instead of furniture is making a profound neurological shift."

Step 6 — The Cool-Down
Step 6 of 6
No session ends abruptly. The cool-down transitions the child from high-energy input back to baseline — preserving the regulated state and making the transition to the next activity smooth.
Transition Warning Script
"Two more big jumps, then we're all done with trampoline!"
"One more crash, and then we do our calm-down."
Give 2-minute and 1-minute warnings. The predictability reduces resistance and builds the child's capacity for transition.
If the Child Resists Ending
- Add 2 more repetitions (honour the request — then firm boundary)
- Use visual timer: "When the timer goes, we're done. Then you choose what's next."
- Offer a calming alternative: "Trampoline is done, but you can use your therapy ball while we do puzzles."
- Avoid power struggles — resistance may itself be seeking behaviour. Offer lower-intensity input as a bridge.

Capture the Data — Right Now (60 Seconds)
The session just ended. Record these 3 data points within 60 seconds. Over weeks, this data reveals whether the sensory diet is reducing unsafe seeking — the core outcome measure.
1
Duration
How many minutes of active input? (Trampoline: ___ min | Crash Pad: ___ jumps | Other: ___ min)
2
Regulation Rating
After the session, how regulated is your child? Rate 1 to 5: (1 = very dysregulated → 5 = calm and focused)
3
Unsafe Seeking Count
How many unsafe jumping incidents today (jumping off furniture, crashing dangerously)? Note the count and the context.
"60 seconds of data now saves hours of guessing later. Over weeks, this data reveals whether the sensory diet is reducing unsafe seeking — the core outcome measure." Track weekly with a simple downloadable sheet or the GPT-OS® in-app tracker which auto-calculates trends and generates progress reports for your OT.

What If It Didn't Go as Planned?
Session abandonment is not failure — it is data. Every attempt teaches you something about your child's sensory profile. Here are the most common challenges and how to address them.
Child won't use the trampoline — still prefers furniture
The trampoline may be less appealing because it's less intense than jumping from height. Try: Place the trampoline near the couch and practice jumping FROM couch ONTO trampoline. Add a crash pad landing zone. Make the trampoline the bridge, not the destination.
Session made child MORE hyper, not calmer
Some children become over-stimulated from too much vestibular input. Reduce session duration. Shift to proprioceptive-only input (heavy work, weighted blanket) which is more organising. Linear movement (back-and-forth) is calmer than rotational.
Child lost interest after 2 minutes
That's data, not failure. 2 minutes of input is 2 minutes of regulation. Build duration gradually. Add games, music, or social engagement. Alternate materials within the session to maintain novelty.
Child won't transition OFF the trampoline
This likely means they haven't gotten enough input yet. Extend the session. Use a visual timer. Offer a calming alternative (weighted blanket, body sock) as bridge. Avoid power struggles — this resistance is likely itself seeking behaviour.
School won't permit sensory materials
Request an OT consultation for classroom accommodations. Therapy ball seating, bouncy bands on chair legs, weighted lap pad, and scheduled movement breaks are all school-compatible. Many teachers are receptive when they understand the neurological basis — share the neuroscience card with them.
Family members think you're encouraging bad behaviour
Frame as medical intervention, not permissive parenting. Consistent language: "This is prescribed sensory input, like medication for the nervous system." Share the neuroscience and evidence sections with them directly.
Adapt and Personalise
Every child's sensory profile is unique. The following modifications allow you to calibrate the protocol to your child's specific needs, age, and current state on any given day.
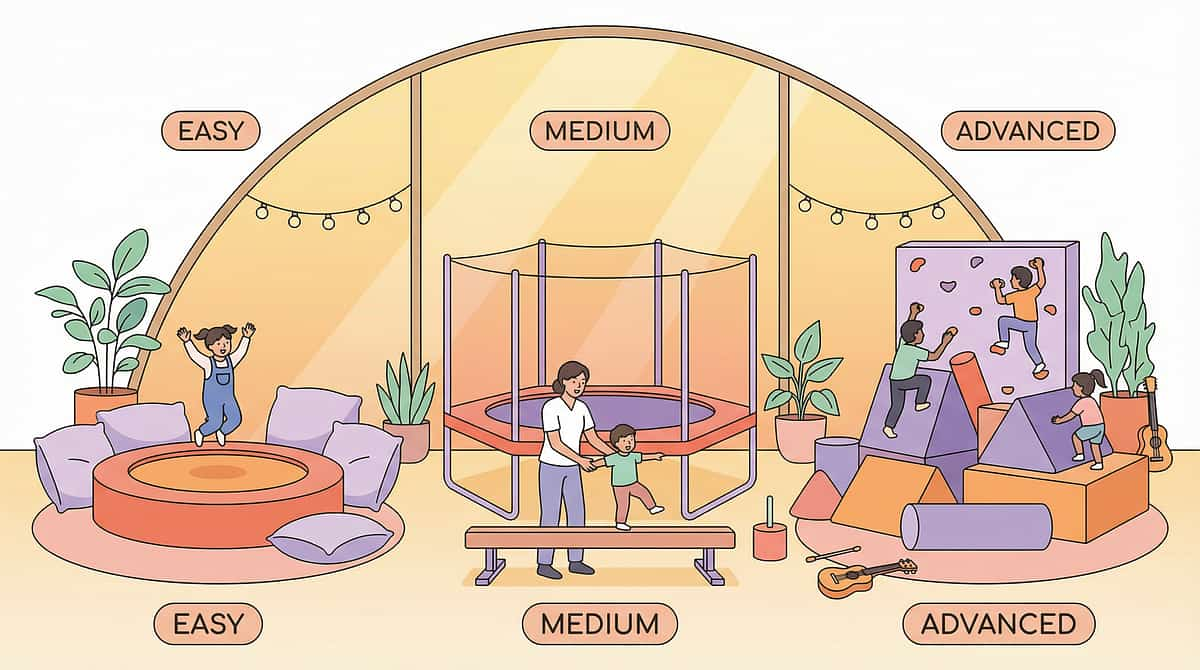
1
Easier (Younger / Sensitive / Hard Days)
Weighted blanket on lap only. Gentle rocking on therapy ball. Slow swinging, linear only. Heavy blanket draped — no active movement required.
2
Standard (Typical Session)
Full sensory diet rotation. Trampoline and crash pad combination. 10-minute trampoline plus heavy work. Multi-material session with visual schedule.
3
Harder (Older / High-Threshold / Breakthrough Days)
Full obstacle course circuit. Timed jumping challenges with goals. 20-minute sustained jumping plus heavy work plus swing. Add resistance: body sock plus trampoline combined.
Age Modifications
- Ages 2–3: Simplified materials, short sessions (2–5 min), high supervision, parent-guided throughout
- Ages 4–6: Full material rotation, growing independence, visual schedule introduction
- Ages 7–9: Self-monitoring emerging, child helps plan sensory diet, school integration begins
- Ages 10–12: Self-advocacy skills, independent material selection, peer-aware modifications
Mixed Sensory Profile
If your child seeks jumping but avoids other sensory input — respect the avoidance in non-jumping domains while meeting the jumping need. Don't force a touch-sensitive child into a body sock. The sensory diet should match the seeking profile, not override the avoidance profile.
Honour what the nervous system is telling you. Always start where the child is comfortable and expand gradually from that foundation of trust.
Week 1–2: What to Expect
Progress Arc
Weeks 1–2
15%
Progress Stage
Foundation building — tolerance and exposure phase
1/10
Redirection Success
Even 1 successful redirection out of 10 attempts is genuine, measurable neurological progress at this stage
30%
Session Consistency
Partial consistency is expected in weeks 1–2. The schedule matters more than perfect execution
What "Progress" Actually Looks Like in Weeks 1–2: Progress is NOT the child stopping furniture jumping. Progress is: the child uses the trampoline at least once when redirected. The crash pad gets used at all. The parent starts implementing a sensory diet with partial consistency.
Parent Emotional Preparation: This phase feels slow. You'll wonder if it's working. Keep the data. Trust the process. Consistency now builds the foundation for the breakthrough coming in weeks 3–4. "If your child tolerates the trampoline for 3 minutes today when they wouldn't touch it last week — that's real, measurable neurological progress."

Week 3–4: Consolidation Signs
Progress Arc
Weeks 3–4
40%
Progress Stage
Neural pathway consolidation — association and preference forming
50%
Redirection Success Rate
By week 4, successful redirection to safe outlets more than half the time is a strong consolidation sign
Child begins anticipating sensory diet times
"Is it trampoline time yet?" — The brain is forming strong associations between materials and the regulated state.
Post-session calm periods extend
30 minutes of post-session regulation becomes 60 minutes. This is synaptic strengthening through repeated structured input.
Child shows preference among the 9 materials
Data reveals which inputs are most regulating for YOUR child specifically. This is your personalisation signal — lean into what works.
Unsafe jumping incidents begin to decrease
Check your tracking data from Card 28. Even a 20–30% reduction in unsafe incidents at this stage is a powerful consolidation indicator.
"You may notice you're more confident too. The techniques are becoming second nature — not just for your child, but for you."

Week 5–8: Mastery Indicators
Progress Arc
Weeks 5–8
75%
Progress Stage
Mastery phase — independent selection and generalisation emerging
🏆 Mastery Criterion 1
Child independently selects appropriate sensory materials when feeling the need to jump — without adult prompting.
🏆 Mastery Criterion 2
Unsafe jumping-seeking behaviour significantly reduced — compare tracking baseline to current frequency data.
🏆 Mastery Criterion 3
Child can verbalise or signal their sensory need: "I need to jump" / moves to trampoline independently.
🏆 Mastery Criterion 4
Sensory diet is routine — happens with minimal parent prompting. Skills persist even when schedule timing is imperfect.
Your child has progressed from unsafe, constant seeking → to independent, safe sensory self-management. The need didn't go away. The strategy for meeting it transformed. That is the goal.

Red Flags — When to Pause and Seek Professional Consultation
Trust your instincts — if something feels wrong, pause and ask. These red flags indicate that professional consultation is needed before continuing the sensory diet.
🚩 Seeking is ESCALATING despite consistent sensory diet
More intense, more frequent, more dangerous seeking despite 4+ weeks of consistent material use. The sensory diet may need recalibration. Book OT consultation.
🚩 No calming response to ANY proprioceptive/vestibular input
After trampoline, crash pad, and heavy work — child is still as dysregulated as before. The sensory profile may be more complex. Full sensory processing evaluation needed.
🚩 Motor regression or new coordination problems
Child was landing safely, now falling. Balance worsening. Movements becoming less coordinated. This may indicate an underlying neurological or motor issue requiring medical evaluation.
🚩 New behaviours appearing alongside jumping (tics, staring, unusual eye movements)
Behaviours that don't fit the sensory seeking pattern warrant NeuroDev paediatric evaluation to rule out seizure or other neurological conditions.
🚩 Child is repeatedly injuring themselves despite safe outlets
Child consistently chooses dangerous jumping over safe alternatives. This may be beyond sensory seeking — behavioural assessment to determine function is needed.
🚩 Parent/caregiver burnout — exhausted, frustrated, losing hope
You can't maintain the sensory diet. Conflict is increasing. This is a valid red flag. You need support. Contact Pinnacle for professional guidance — your wellbeing IS your child's wellbeing.
The Progression Pathway — Your Developmental GPS
Your child's sensory journey doesn't end here. Based on their response to A-088 materials, the following pathways offer the most clinically logical next steps.
Long-term developmental goal: Independent sensory self-regulation — the child recognises their own needs, selects appropriate tools, and maintains baseline regulation across settings without adult prompting. Every technique in this series brings the child one step closer to that goal.
Related Techniques — Sensory Processing Domain
The materials from A-088 overlap significantly with neighbouring techniques — you may already own everything you need to start these too.
Technique | Level | Materials You Already Own | What's New | |
A-086: 9 Materials for Crashing/Bumping | Core | ✅ Crash Pad, Heavy Work Kit, Body Sock | Minor additions only | |
A-087: 9 Materials for Mouthing/Chewing | Core | Partial | Oral motor materials needed | |
A-089: 9 Materials for Spinning Seeking | Core | ✅ Indoor Swing, Therapy Ball | Rotation-specific additions | |
A-090: 9 Materials for Loud Sound Seeking | Core | Limited | Auditory tools required | |
A-091: Sitting Still in Classroom | Applied | ✅ Therapy Ball, Weighted Lap Pad, Heavy Work | Classroom-specific protocols | |
A-092: Sensory Diet Design Masterclass | Advanced | ✅ Visual Schedule — foundation in place | Advanced scheduling tools |

Connect With Other Parents
You are not navigating this alone. Thousands of families across India and beyond are walking this same path — with the same fears, the same wins, and the same deep love for a child whose body speaks differently.
Sensory Seeking Parent Community (WhatsApp)
Join families whose children are sensory seekers — jumping, crashing, spinning, mouthing. Share strategies, ask questions, find support from parents who understand from the inside out.
Pinnacle Parent Forum
Online discussion board organised by sensory challenge. Find the Proprioceptive Seeking thread. Share your wins and your hard days with a community that responds with experience, not judgement.
Local Pinnacle Parent Meetups
Monthly meetups at Pinnacle centres. Sensory-friendly environments. Children welcome. Meet families navigating the same journey in person — because some connections need to be face to face.
Peer Mentoring
Connect with an experienced parent who has already been through the jumping-seeking journey and come out the other side. Because sometimes you need to hear "I've been there, and it gets better" from someone who really has.
"Your experience helps others — consider sharing your journey." Every story shared is a lifeline for a family just beginning theirs.

How GPT-OS® Uses Your Data
What GPT-OS® Learns From A-088
- Which materials produce the strongest regulation response for YOUR child
- Optimal session duration and frequency
- Time-of-day patterns — when seeking is highest, when input is most effective
- Rate of unsafe seeking reduction over time
- Which combinations of materials work best together
Privacy and Population Impact
🔒 Your child's data is encrypted, anonymised in aggregate, and never shared without explicit consent. Pinnacle complies with Indian Data Protection standards.
"Your data helps every child like yours." When thousands of families track jumping-seeking outcomes, GPT-OS® identifies which intervention patterns produce the best results across different sensory profiles, age groups, and severity levels.
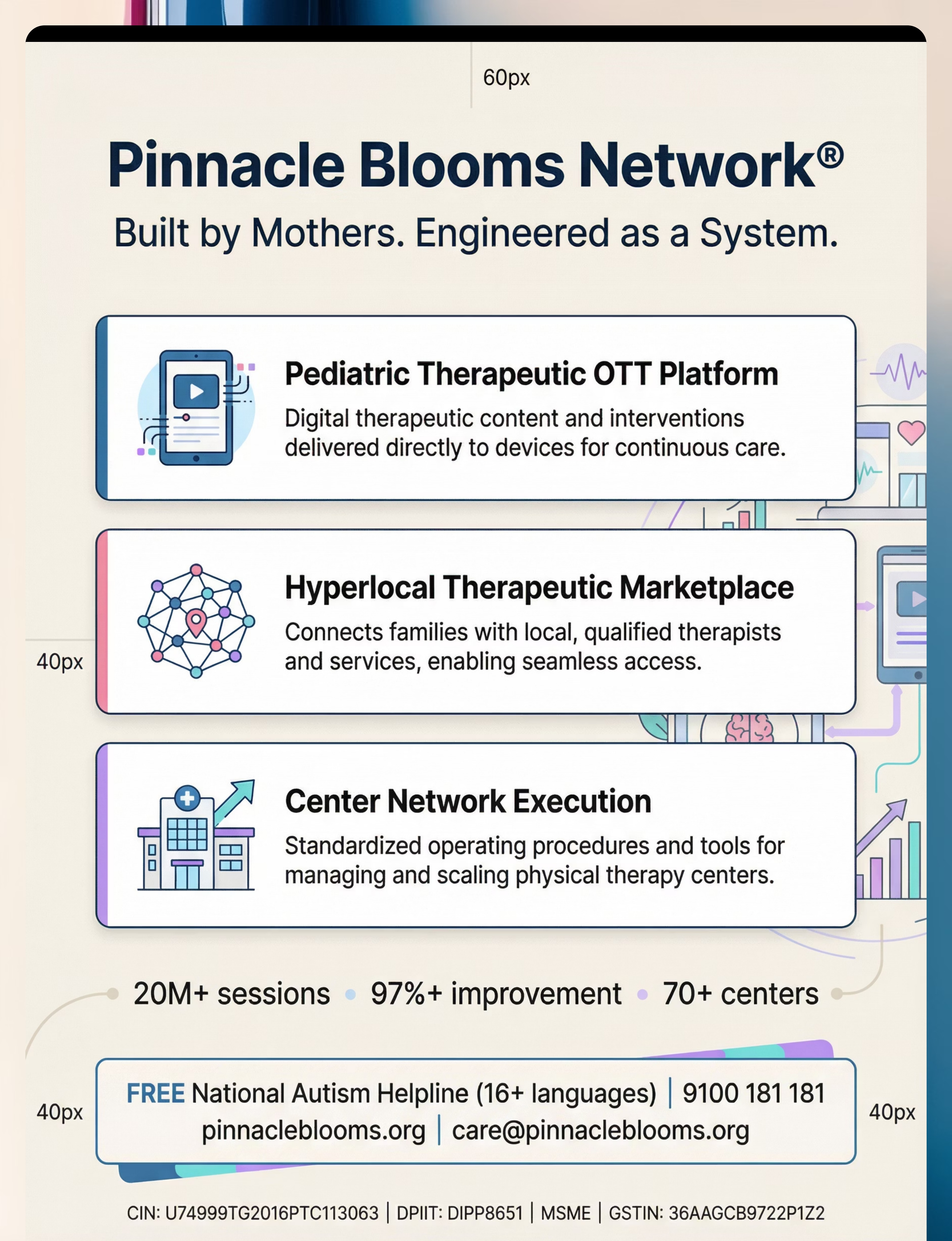
20M+ sessions. 97%+ measured improvement. 70+ centres. One closed, accountable system.

Watch the Reel — A-088
Reel A-088
Sensory Solutions Episode 88
🎬 Reel Title: 9 Materials That Help When Child Seeks Jumping
📋 Reel ID: A-088 | Domain: Sensory Processing
📺 Series: Sensory Solutions — Episode 88
📋 Reel ID: A-088 | Domain: Sensory Processing
📺 Series: Sensory Solutions — Episode 88
In this 60-second Reel, a Pinnacle therapist demonstrates all 9 materials in action — trampoline, crash pad, weighted blanket, body sock, therapy ball, indoor swing, heavy work kit, hopper ball, and visual sensory diet schedule. Watch the child's body receiving the input it needs and the transformation from unsafe seeking to safe, channelled movement.
🎯 What You'll See
All 9 materials demonstrated in clinical practice. The child's body language shifting from dysregulated seeking to calm, organised engagement.
📱 Where to Watch
Available on the Pinnacle Blooms YouTube channel and Instagram (@PinnacleBlooms). Follow for 999 Reels covering the full spectrum of paediatric therapy techniques.
🎓 Why Video Matters
Video modelling is classified as an evidence-based practice for autism (NCAEP, 2020). Multi-modal learning improves parent skill acquisition — see the technique, then do it.
Preview of 9 materials that help when child seeks jumping Therapy Material
Below is a visual preview of 9 materials that help when child seeks jumping therapy material. The pages shown help educators, therapists, and caregivers understand the structure and content of the resource before use. Materials should be used under appropriate professional guidance.






Link copied!

The Pinnacle Promise
From fear to mastery. One technique at a time.
20M+
Exclusive 1:1 Sessions
Delivered across the Pinnacle Blooms Network
97%+
Measured Improvement
Across all therapy disciplines and sensory profiles
70+
Centres Across India
With specialists in sensory integration and neurodevelopmental paediatrics
Pinnacle Blooms Network®
Built by Mothers. Engineered as a System.
GPT-OS® — Global Paediatric Therapeutic Operating System
Diagnosis → AbilityScore® → Prognosis → TherapeuticAI® → FusionModule™ → EverydayTherapyProgramme™ → Re-measurement
Patents filed across 160+ countries.
Navigate
📞FREE National Autism Helpline: 9100 181 181
16+ languages | 24×7
16+ languages | 24×7
CIN: U74999TG2016PTC113063 | DPIIT: DIPP8651 | MSME: TS20F0009606 | GSTIN: 36AAGCB9722P1Z2
© 2026 Pinnacle Blooms Network®, unit of Bharath Healthcare Laboratories Pvt. Ltd. All rights reserved.
Medical Disclaimer: This content is educational and informational. It does not replace assessment by a licensed occupational therapist or healthcare provider. Sensory seeking behaviours, especially when impacting safety, daily functioning, or development, should be evaluated comprehensively to understand the child's full sensory profile and guide appropriate intervention. Individual results may vary. Statistics represent aggregate outcomes across the Pinnacle Blooms Network.