9 Materials That Help When Your Child Seeks Deep Pressure
"He crashes into everything. Squeezes between the cushions. Wraps himself so tight I can barely unwrap him. He asks me to squeeze harder, harder — and I'm already squeezing as hard as I can."
This is not aggression. This is not defiance. This is not a behavior problem. Your child's body is genuinely, physiologically hungry for a type of sensory input called deep pressure. The crashing, the wedging, the burrowing, the squeezing that never satisfies — these are your child's nervous system trying to feed itself what it desperately needs. You are not failing. Your child's nervous system is speaking. And now you'll learn how to listen.
Sensory Solutions Series — A-025
Proprioceptive Processing + Self-Regulation
Ages 2–12

ACT I: THE EMOTIONAL ENTRY
You Are Not Alone — The Numbers
Before we dive into the science and the materials, let's establish something important: this experience is far more common than you think. Millions of families across the globe are navigating the exact same challenge you are right now.
80%
Sensory Difficulties
of children diagnosed with autism experience sensory processing difficulties, including proprioceptive under-responsivity
1 in 6
Children Affected
children worldwide display sensory processing challenges significant enough to affect daily functioning
50–70%
Proprioceptive Seekers
of sensory-processing children display proprioceptive seeking behaviors — crashing, squeezing, heavy pressure demands
You are among millions of families across 70+ countries navigating this exact challenge. The child who crashes into the couch, who asks to be squeezed harder, who wraps himself so tight in blankets he can barely breathe — that child exists in homes across every continent, culture, and language. This is not rare. This is not unexplainable. And there are materials — clinically validated, scientifically understood, and home-executable — that meet this need.
Sources: PRISMA Systematic Review, Children (2024) — PMC11506176 | SPD Foundation | Sensory Processing Measure normative data; AOTA clinical guidelines

What's Happening in Your Child's Brain
The Proprioceptive System
Your child has a sense you might never have heard of — proprioception. It's the sense that tells the brain where the body is in space and how much force the muscles are using. Receptors in muscles, joints, and tendons send constant signals about body position, movement, and pressure.
The Under-Responsive Pattern
In your child, this system requires MORE intense input than typical to register. Think of it like a volume dial — for most children, everyday activities provide enough proprioceptive "volume." Your child's dial is set higher. Everyday activities are too quiet. The brain doesn't hear the signal.
The Seeking Behavior
So your child turns up the volume. Crashing provides impact. Squeezing provides compression. Burrowing provides all-around pressure. Heavy work provides resistance. These aren't random behaviors — they are your child's brain demanding the input volume it needs to know where its body is.
This is a wiring difference, not a behavior choice. Your child is not being defiant or aggressive. Their nervous system is simply calibrated differently — and that calibration can be supported with the right tools.
Reference: Frontiers in Integrative Neuroscience (2020) — DOI: 10.3389/fnint.2020.556660 | Ayres Sensory Integration Theory
Where This Sits in Development
Understanding where your child is on the developmental timeline helps you recognize that this is a waypoint, not a deficit — with a clear forward path.
0–12 Months
Proprioceptive system begins developing through crawling, pulling to stand, and grasping. Craving movement is entirely normal at this stage.
1–2 Years
Body awareness emerges. High activity and crashing is developmentally typical — but intensity and frequency matter.
2–4 Years ⬅ CRITICAL
Proprioceptive processing differences become visible. Seeking behaviors escalate beyond typical rough play. This is where most parents first notice: "Something feels different."
4–7 Years
School demands reveal regulation challenges — sitting still, force modulation, difficulty with transitions between activities.
7–12 Years
Social consequences emerge. Peers notice roughness. Self-regulation strategies become essential. Child can begin learning to self-identify needs.
Co-occurring patterns to watch: Vestibular seeking (spinning, swinging), oral sensory seeking (chewing non-food items), motor planning challenges, and attention difficulties. These frequently travel together because they share neural infrastructure.
References: WHO Care for Child Development (CCD) Package | PMC9978394 | UNICEF MICS developmental indicators
The Evidence Behind Deep Pressure Intervention
EVIDENCE GRADE: LEVEL I–II
Systematic Reviews + Randomized Controlled Trials
1
16 Studies Confirm
Sensory integration intervention — including deep pressure protocols — meets criteria for evidence-based practice for children with autism spectrum disorder (PRISMA Systematic Review, Children 2024 — PMC11506176).
2
24-Study Meta-Analysis
Demonstrates sensory integration therapy effectively promotes social skills, adaptive behavior, sensory processing, and motor skills (World Journal of Clinical Cases 2024 — PMC10955541).
3
Indian RCT Validated
Padmanabha et al. (2019): Home-based sensory interventions demonstrated significant outcomes in Indian pediatric population. This technique is validated in your context (DOI: 10.1007/s12098-018-2747-4).
4
Grandin's Foundational Research
Temple Grandin's Squeeze Machine research: Controlled deep pressure calms the autonomic nervous system. Deep pressure to parasympathetic activation has been replicated across multiple studies.
Clinically validated. Home-applicable. Parent-proven.

ACT II: THE KNOWLEDGE TRANSFER
Deep Pressure Proprioceptive Input — Materials-Based Sensory Regulation
Parent-Friendly Name:"Feeding Your Child's Body Hunger"
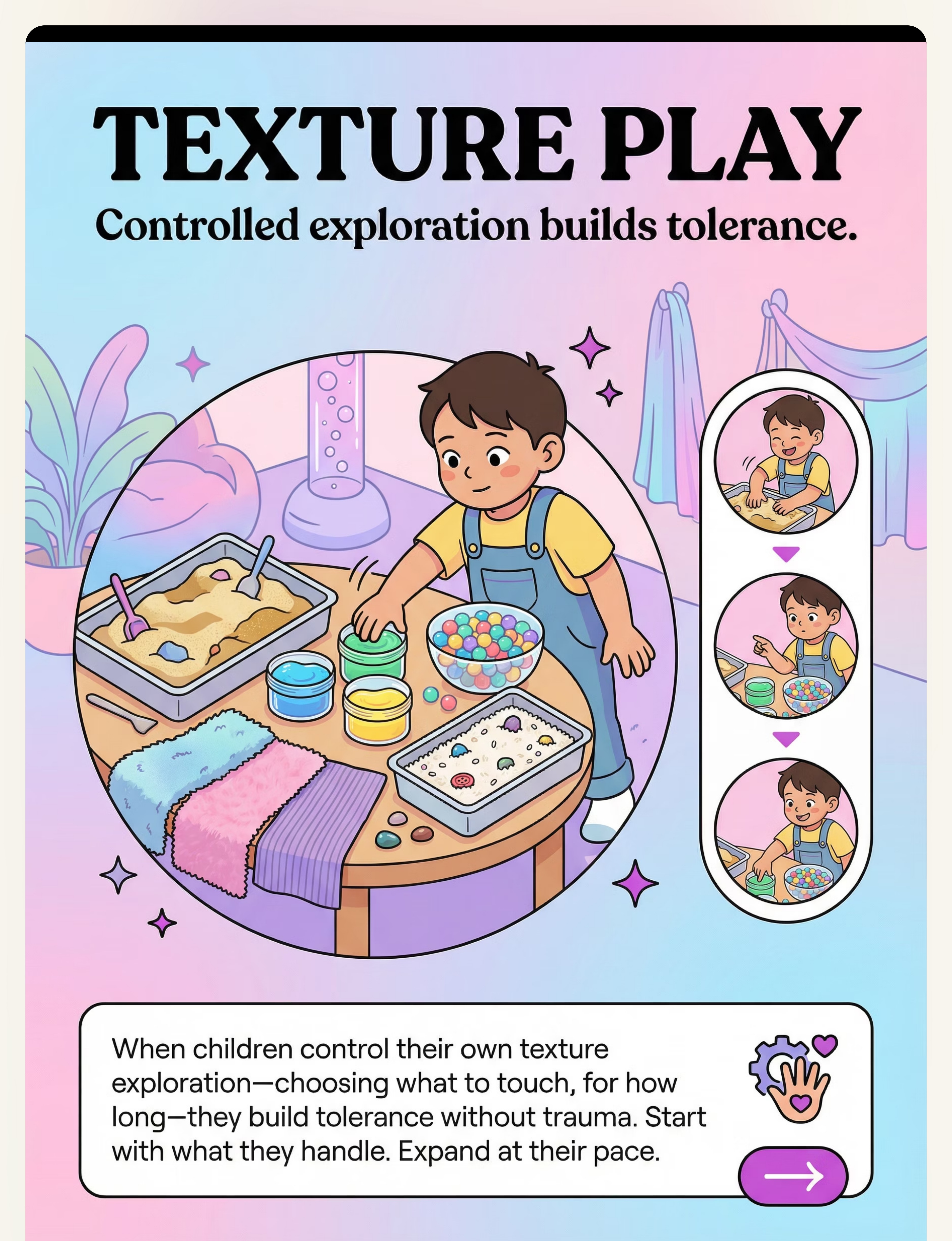
A structured approach to meeting your child's proprioceptive sensory needs through 9 clinically validated materials that deliver deep pressure — the type of intense, sustained, compressive input your child's nervous system requires to feel organized, grounded, and regulated. Instead of fighting the crashing, squeezing, and burrowing, you provide appropriate outlets that satisfy the same neurological need safely and sustainably.
Sensory Processing — Proprioceptive
Weighted Materials, Compression, Resistance
Ages 2–12 Years
Home / School / Therapy
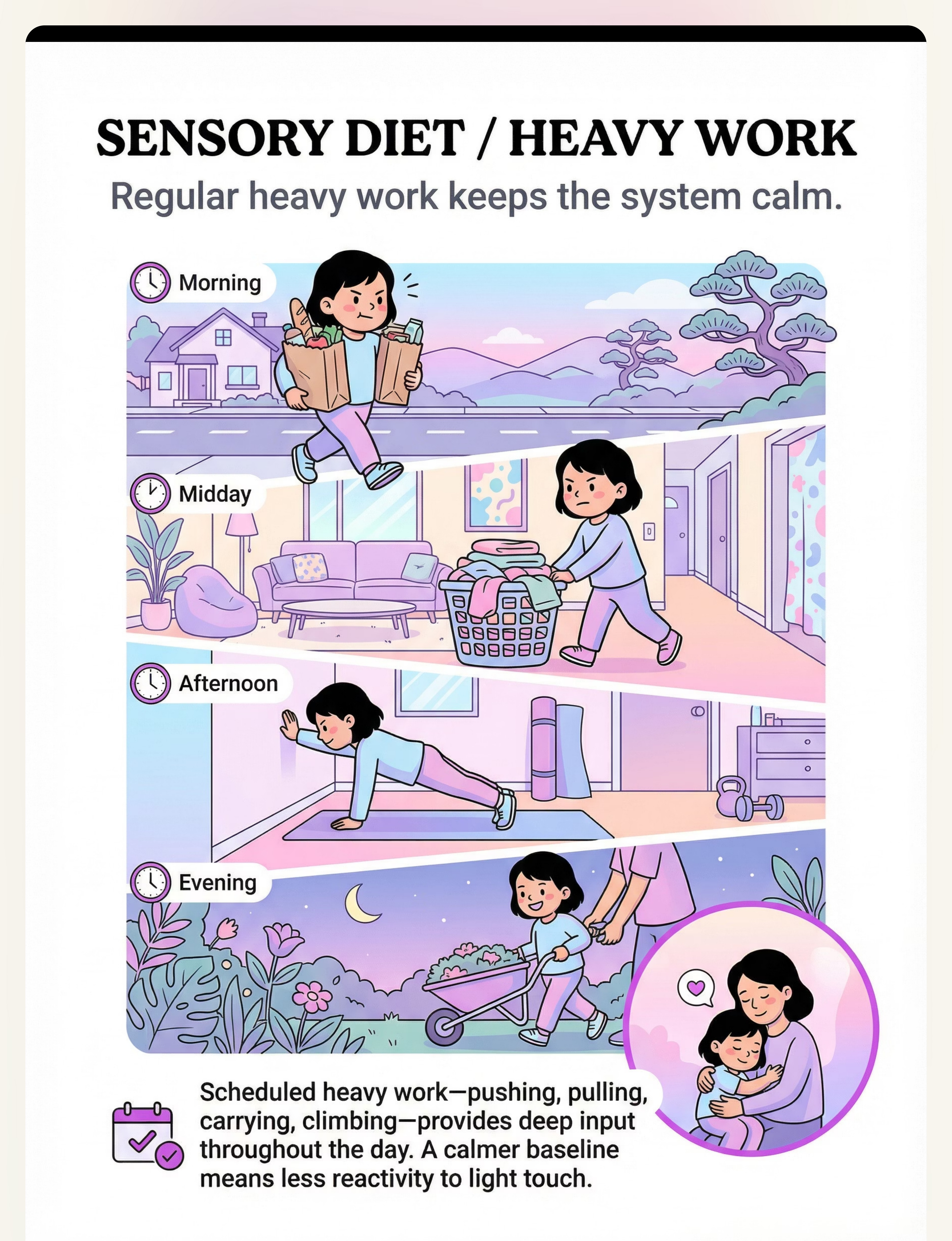
Daily Sensory Diet Integration
10–20 Minute Sessions

Who Uses This Technique — The Consortium Behind the Protocol
This technique crosses therapy boundaries because the brain doesn't organize by therapy type. Here's how each discipline contributes to the deep pressure protocol.
Occupational Therapy (Primary Lead)
OTs design the individualized sensory diet, select specific materials based on the child's proprioceptive profile, establish wearing/use schedules, and monitor sensory regulation progression. The Wilbarger Protocol, weighted material prescriptions, and crash zone design are OT-led.
Applied Behavior Analysis (ABA)
BCBAs use deep pressure materials as antecedent interventions to prevent dysregulated behavior, design reinforcement schedules around material use, and teach the child to self-identify needs and independently access tools — the self-regulation pathway.
Speech-Language Pathology (SLP)
SLPs deploy oral proprioceptive tools (chew tools, resistive foods) for children whose deep pressure seeking extends to the jaw. Oral motor regulation supports feeding therapy, articulation, and attention during language tasks.
Special Education
Special educators integrate heavy work activities into classroom routines, implement compression and weighted tools during academic tasks, and coordinate sensory breaks within the school schedule.
Reference: Adapted UNICEF/WHO Nurturing Care Framework for SLPs (2022) — DOI: 10.1080/17549507.2022.2141327
What This Targets — Precision, Not Guesswork
Deep pressure intervention isn't a vague "calming strategy." It addresses specific, measurable targets organized by priority level.
Observable Indicators of Success: Child uses crash pad instead of walls. Child requests weighted blanket independently. Child completes homework with lap pad without leaving seat. Child's "bear hug" grip strength becomes modulated with peers.
Reference: Meta-analysis (World J Clin Cases, 2024) — PMC10955541
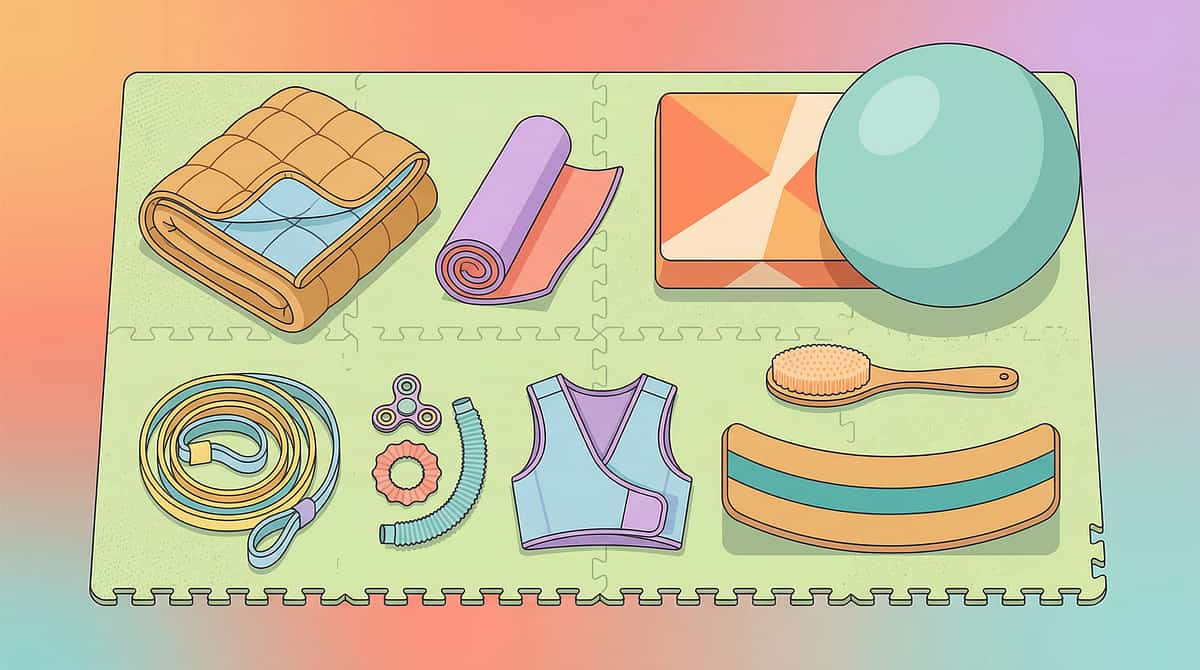
What You Need — The 9 Materials
Here are the 9 clinically validated materials that form the foundation of deep pressure proprioceptive intervention. Each serves a specific purpose within your child's sensory regulation toolkit.
# | Material | Price Range (INR) | Canon Category | |
1 | Weighted Blanket | ₹2,500–8,000 | Sensory Regulation Tools | |
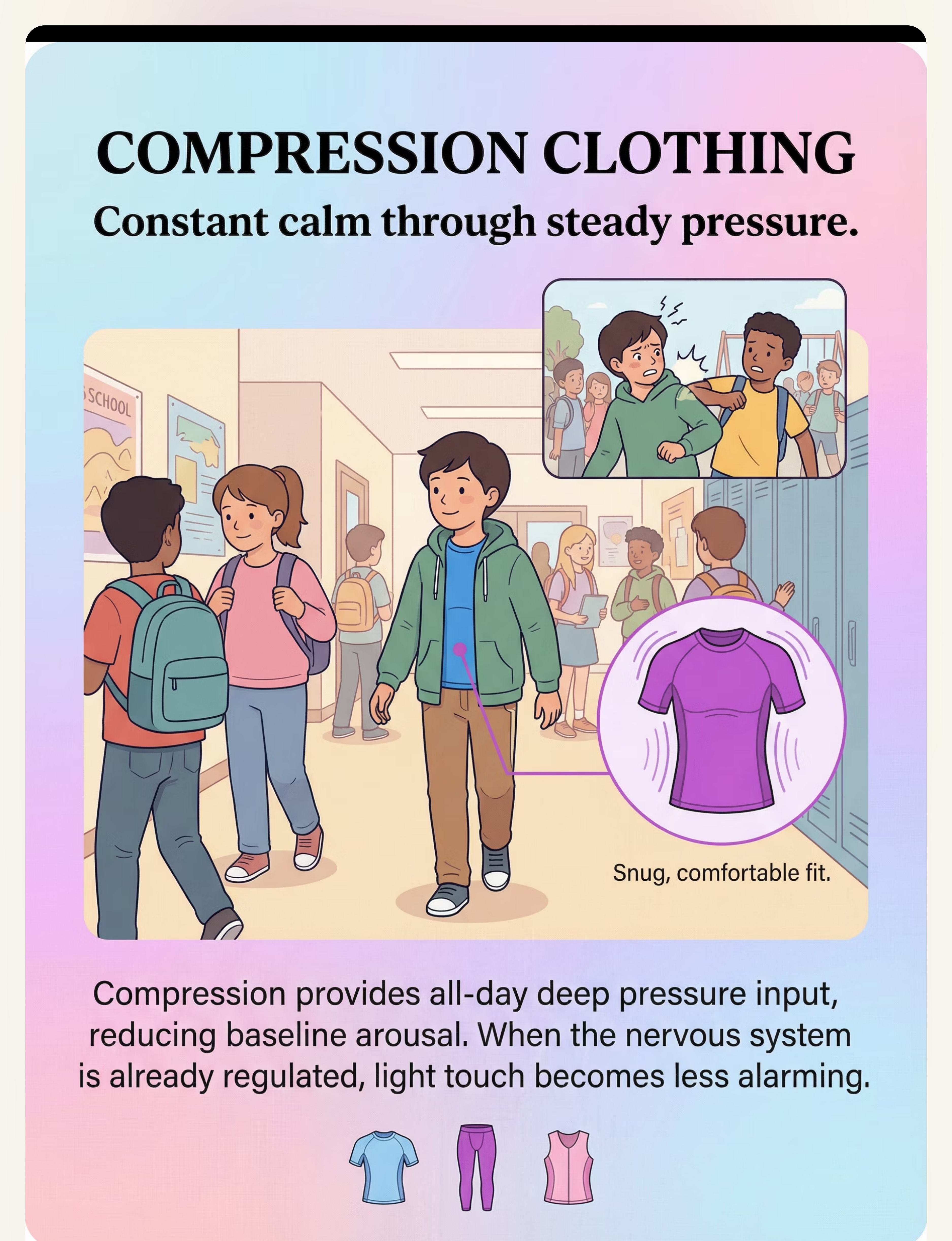
2 | Compression Vest / Pressure Vest | ₹1,500–5,000 | Compression & Proprioceptive | |
3 | Body Sock / Sensory Sack | ₹800–2,500 | Compression & Proprioceptive | |
4 | Crash Pad / Crash Mat | ₹3,000–12,000 | Gross Motor & Movement | |
5 | Weighted Lap Pad / Weighted Animals | ₹600–2,500 | Sensory Regulation Tools | |
6 | Therapy Ball / Peanut Ball | ₹600–2,000 | Gross Motor & Movement | |
7 | Resistance Tunnel / Squeeze Machine | ₹2,000–50,000+ | Compression & Proprioceptive | |
8 | Heavy Work Activities Kit | ₹0–2,000 | Household Items | |
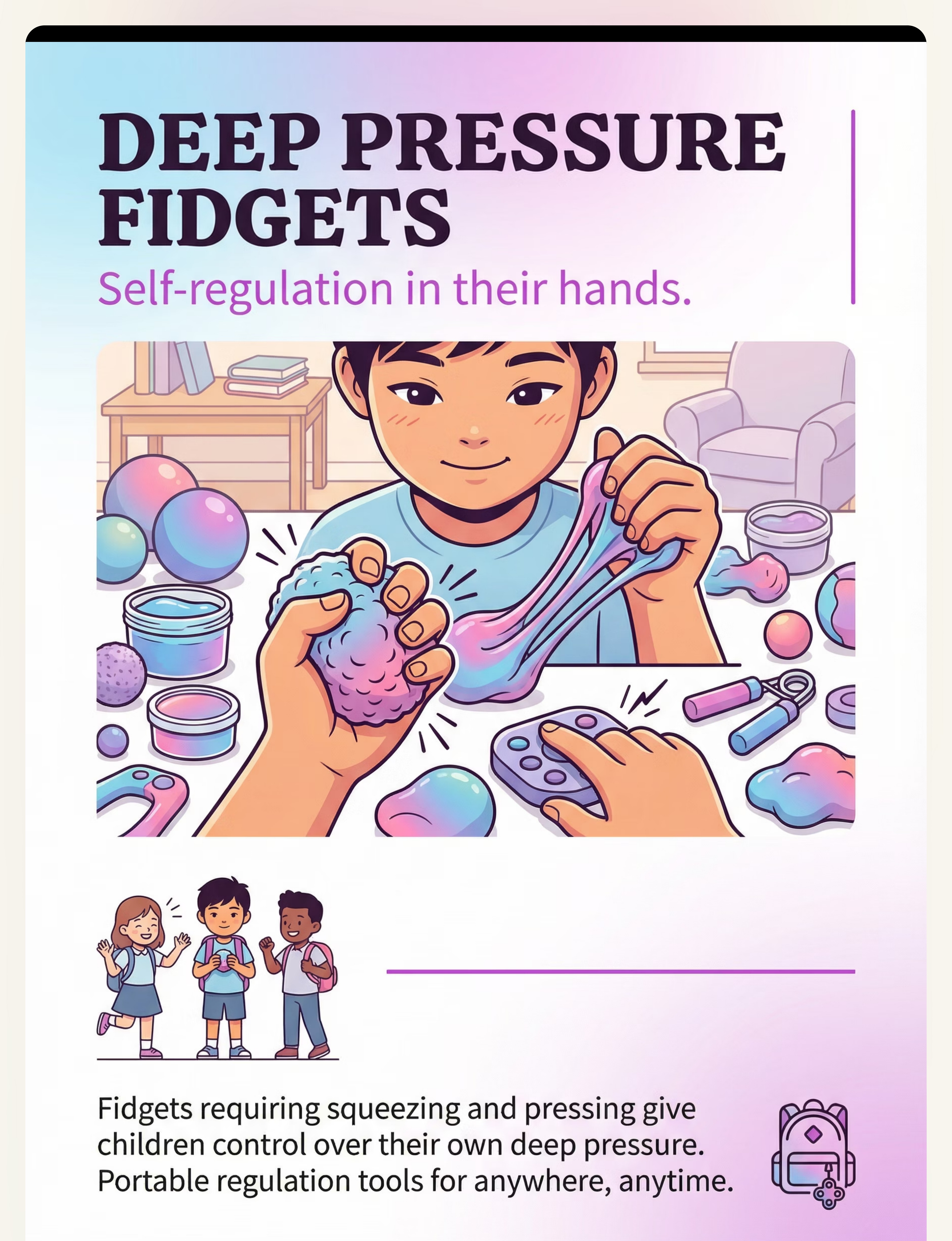
9 | Chew Tools / Oral Proprioceptive | ₹200–1,000 | Oral Motor Tools |
🔖 Pinnacle Recommends — Start With These 3: (1) Weighted blanket appropriate for your child's weight, (2) Crash pad or cushion crash zone, (3) Heavy work activities — free, using household items.

DIY & Substitute Options — Every Family Can Start Today
WHO Nurturing Care Framework: Equity-focused, context-specific interventions. Not every family can order online. Not every village has delivery. This card ensures every parent can begin TODAY.
1
Weighted Blanket → DIY
Sew a pillowcase with pockets. Fill with dried rice or poly pellets in a grid pattern. Start with a lap-sized version to test response before making a full blanket.
2
Compression Vest → DIY
Tight-fitting athletic compression shirts, layering snug undershirts, or tight swimsuits and dance leotards worn under everyday clothing.
3
Body Sock → DIY
Large stretchy pillowcase or lycra/spandex fabric sewn into a sack with a head opening. Stretchy fitted sheet with head opening. Ensure breathable fabric always.
4
Crash Pad → DIY
Large beanbag filled with foam scraps, stacked couch cushions in a corner, a pile of pillows in a designated "crash zone," or an old mattress laid flat on the floor.
5
Lap Pad / Squeeze / Heavy Work / Chew
Lap Pad: Fabric rectangle filled with dried rice/beans, sewn closed. Squeeze: Stretch lycra across chairs, burrito roll in heavy blanket. Heavy Work: Carry laundry, push furniture, pull wagons — free. Chew: Crunchy carrots, chewy dried fruit, bagels.
Zero-cost versions exist for 7 of 9 materials. Economic status does not determine therapeutic access. This is the WHO/UNICEF inclusion principle in action.

⚠️ Safety First — Before You Begin
Deep pressure materials are powerful therapeutic tools. Like any tool, they require proper safety guidelines. Review this traffic light system before introducing any material to your child.
🔴 DO NOT PROCEED IF
- Child is under 2 years (weighted blankets contraindicated for infants)
- Child has respiratory, cardiac, or circulatory conditions (medical clearance required)
- Child cannot remove weighted blanket independently
- Child shows panic or distress in enclosed materials — do NOT force
- Head-banging causing visible injury — seek immediate OT evaluation
🟡 MODIFY AND PROCEED WITH CAUTION
- Never used weighted or compression materials — start lightest, shortest duration
- Compression vest: firm but NOT restrictive. 20–30 minute intervals with breaks
- Crash pad: place AWAY from walls and sharp furniture. Non-slip surface underneath
- Weighted blanket: 10% of body weight + 1-2 pounds MAXIMUM
🟢 SAFE TO PROCEED WHEN
- Child is fed, rested, not in post-meltdown state
- Materials are sized and weighted appropriately for THIS child
- Adult supervision is available for initial use of all materials
- Child shows willingness or curiosity (not resistance)
RED LINE: Stop immediately if child shows respiratory difficulty, skin irritation, panic, persistent distress, or any sign of injury.
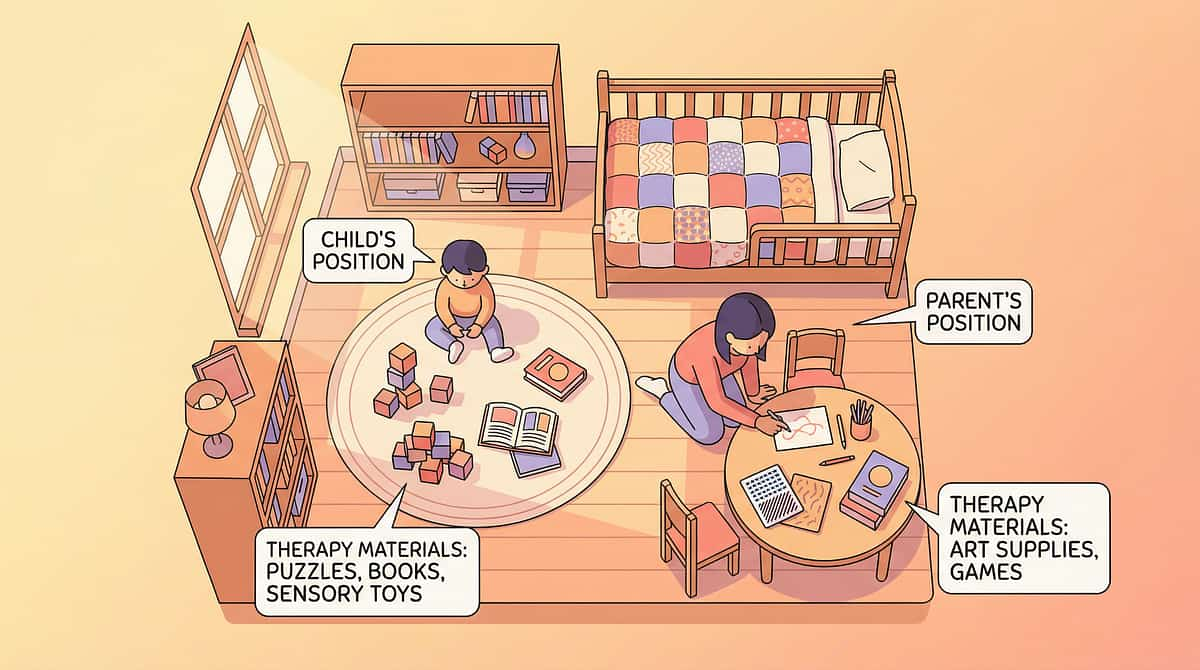
Set Up Your Space — The Proprioceptive Regulation Zone
A well-organized environment is foundational to successful deep pressure intervention. Here's how to create your child's regulation zone at home.
What to Include
- ① Crash Zone: Crash pad, 1.5m clearance, non-slip mat
- ② Calm Pressure Station: Weighted blanket, body sock, beanbag
- ③ Seated Area: Weighted lap pad, therapy ball, chew tools
- ④ Heavy Work Path: Open floor, wall push-up surface
- ⑤ Parent Position: Nearby, within arm's reach
What to Remove
- Breakable items near crash zone
- Sharp-edged furniture
- Distracting screens and toys
- Cluttered floor surfaces
Environment: Moderate lighting, reduced background noise, comfortable temperature. The space should feel inviting, not clinical.

ACT III: THE EXECUTION
Is Your Child Ready? — 60-Second Pre-Session Check
Before starting, run through this quick readiness checklist. The best session is one that starts right — forcing a session when the child isn't ready teaches them that sensory tools equal demands. We want the opposite association.
Fed & Rested
Child is not hungry (hunger mimics dysregulation) and not overtired (fatigue escalates seeking)
Emotionally Stable
No meltdown in the last 30 minutes. Post-meltdown state is too fragile for structured input.
Physically Well
Child is not ill — fever, pain, and infection alter sensory thresholds significantly.
Willing or Curious
Child shows some willingness — even curiosity counts. Not in full shutdown or avoidance.
Materials Ready
Materials are set up and accessible. No scrambling mid-session. You have 15–20 uninterrupted minutes.
All ✅ → GO
Begin with Step 1: The Invitation
3-5 ✅ → MODIFY
Offer weighted blanket only, no demands, just availability
0-2 ✅ → POSTPONE
Not today. Offer a calming alternative. Try again tomorrow.

Step 1 — The Invitation
⏱️ 30–60 seconds
"Hey, I got something for your body. You know how your body loves squeezing and crashing? I found some things that give your body exactly what it wants. Want to check them out with me?"
Your Body Language
Sit at the child's level. Open posture. Relaxed face. Touch or pick up a material yourself — model curiosity, not instruction. You're exploring together, not assigning a task.
Acceptance Looks Like
Child approaches. Child touches a material. Child looks interested. Child moves toward the crash pad. Even a single glance toward the materials is acceptance.
Resistance Looks Like
Child walks away. Child says no. Child appears anxious. That's okay. Leave materials visible and available. Walk away calmly. Many children will approach on their own within 10–30 minutes when the demand is removed.
Every protocol begins with an invitation, not a command. The difference between therapeutic engagement and compliance-based instruction starts here.

Step 2 — The Engagement
⏱️ 1–3 minutes
The child has approached. Now deepen engagement by introducing ONE material at a time. Present it within reach, not on the child. Let the child initiate contact.
Weighted Blanket
Drape gently over legs first, not full body. Let the child feel the weight gradually and decide how much they want.
Crash Pad
You jump first — show it's fun, safe, and satisfying. Your modeling removes uncertainty and builds trust in the material.
Body Sock
Hold it open and let the child choose to climb in. Never pull it over them. Frame it as: "This is a superhero cocoon."
Compression Vest
Offer it like a "superhero jacket" or "power suit." Let them put it on themselves if they're able.
"This is a [weighted blanket / crash pad / body sock]. It gives your body the squeezing/crashing/pressure it likes. Try it — you're in charge of how much."
Reinforcement cue: The moment the child makes contact with the material: "Your body is getting what it needs. That's awesome."

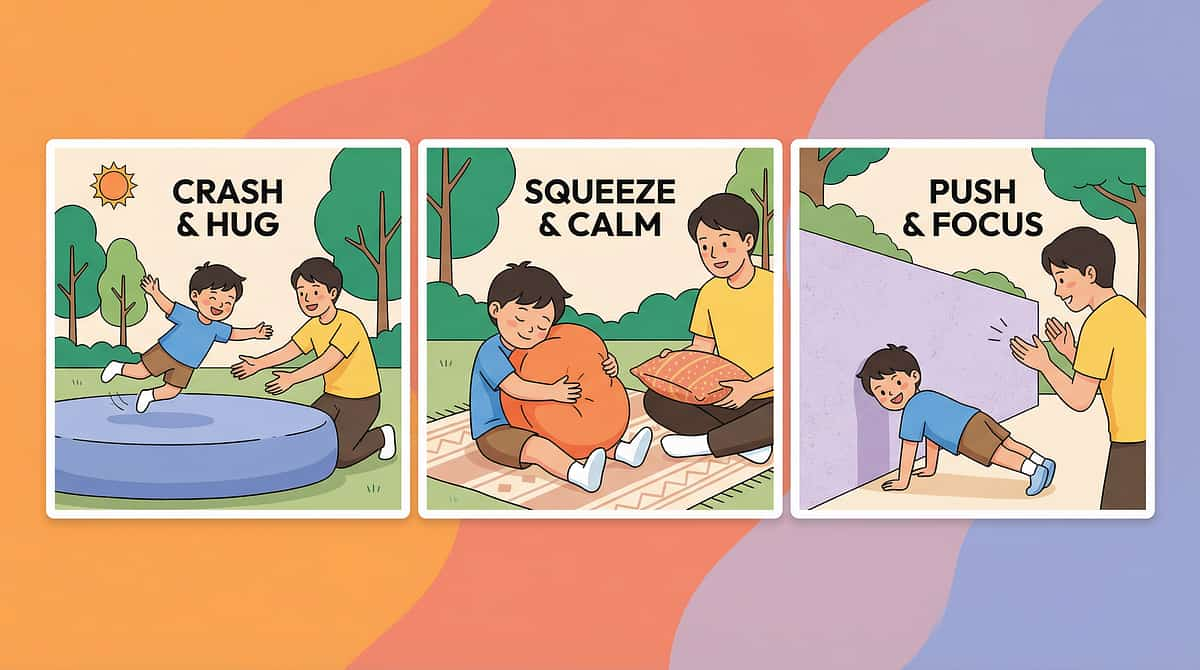
Step 3 — The Therapeutic Action
⏱️ 5–10 minutes — the active proprioceptive input phase

Weighted Blanket
Child lies under blanket or has it across lap for 5–10 minutes. The sustained weight provides deep proprioceptive input. Watch for slower breathing, relaxed muscles, and reduced fidgeting.

Compression Vest
Child wears for 20–30 minutes during activities. Observe for improved focus, reduced crashing behaviors, and calmer transitions between tasks.

Body Sock
Child stretches, pushes, and makes shapes inside. Every movement creates resistance feedback. Guide: "Can you push your arms out? Can you make a star shape?"

Crash Pad
Child jumps, falls, and throws body onto pad. Allow repetition. Count crashes if the child enjoys it: "That was crash number 5! Your body is getting FULL of input."
Also effective: Weighted lap pad across thighs during seated tasks, therapy ball for sit-bounce and balance, heavy work (push laundry, carry books, wall push-ups), and chew tools during focus tasks.
Common execution error: Forcing the child to stay with a material they've disengaged from. If the child moves on — let them. The session isn't failed. The nervous system got what it needed for now.
Step 4 — Repeat & Vary
⏱️ 3–5 minutes
Repetition Guidance
- Crash pad: 5–15 crashes per session (child-led)
- Body sock: 3–5 minutes of sustained use
- Weighted blanket: 10–20 minutes continuous
- Heavy work: 5–10 minutes of effort-based activities
- Therapy ball: 5–10 minutes of bouncing/balance
Introduce Variety
- Crash pad → "Crash like a superhero? A frog? Backwards?"
- Body sock → "Tall shape. Tiny shape. Wiggly shape."
- Heavy work → Rotate carrying, pushing, pulling, squeezing
- Therapy ball → Bounce, lie over, roll, sit and catch
Satiation Indicators — When Enough Is Enough
Watch for these signs that the child's nervous system has received what it needs:
Voluntarily moves away from the material
Body visibly relaxed and calm (mission accomplished)
Interest shifts to a non-sensory activity
Yawning — parasympathetic activation is working
Says "all done" or equivalent
"3 good repetitions with a calm, engaged child are worth more than 10 forced repetitions with a resistant child."

Step 5 — Reinforce & Celebrate
Reinforcement is what builds the bridge between "parent gave me this tool" and "I know what my body needs." Every attempt, no matter how small, deserves recognition.
"Your body needed that pressure and you found exactly what it needed. That's incredible body awareness."
"Look at how calm your body is now! You used your crash pad and your body is settled."
"You know what your body needs and you're learning to give it what it needs. That's a superpower."
Timing
Immediate — within 3 seconds of the desired behavior
Specificity
Name what they did, not just "good job"
Focus
Celebrate the ATTEMPT, not just the outcome
Natural Consequence
Help child notice: "See how your body feels different now?"
Reference: ABA Reinforcement Principles | BACB Ethical Guidelines

Step 6 — The Cool-Down
⏱️ 1–2 minutes
No session ends abruptly. The cool-down transitions from therapeutic input back to baseline, teaching your child that sensory regulation has a beginning, middle, and end.
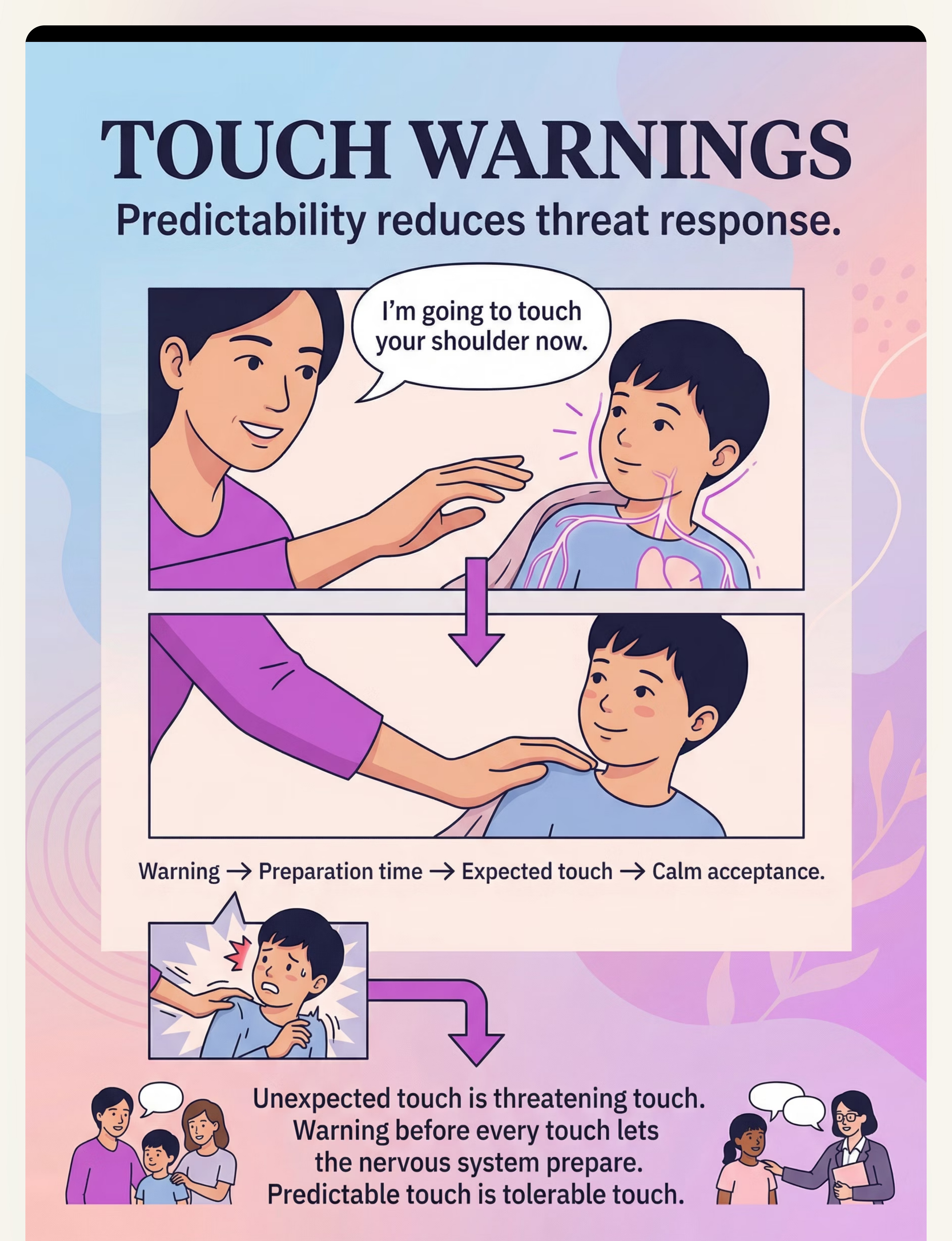
Transition Warning
"Two more crashes on the pad, then we're all done with crash time." Give the child's nervous system a predictable ending point.
Cool-Down Activity
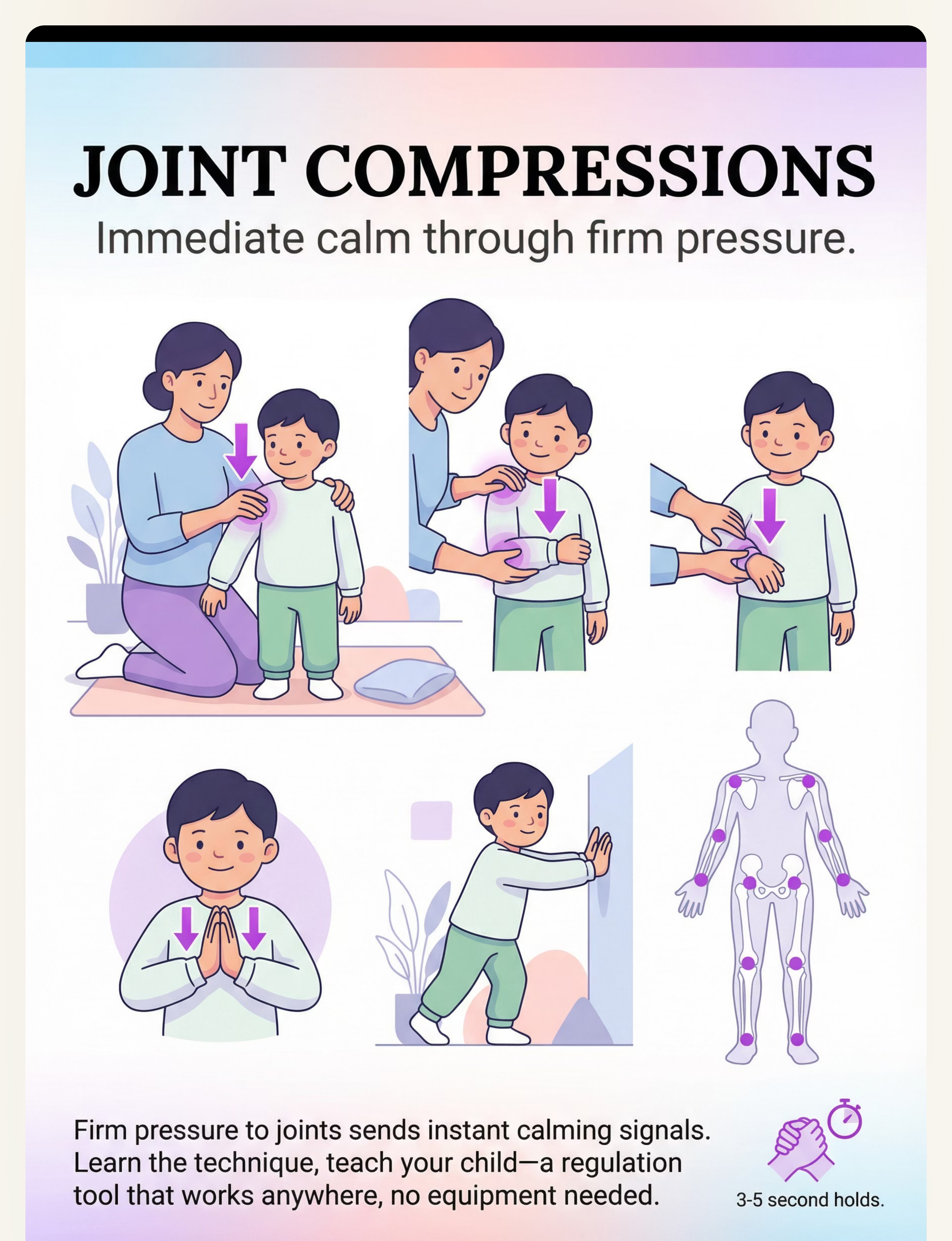
Slow, deep pressure: gentle hand squeezes down each arm. Weighted blanket across lap while sitting quietly. 5 slow wall push-ups. Deep breathing with hands pressing together (joint compression).
Material Put-Away Ritual
"Let's fold your blanket together. It'll be right here for when your body needs it again." The child participates — folding provides additional heavy work!
Transition to Next Activity
"Your body is nice and settled now. What would you like to do next?"
If the child resists ending: This is GOOD data. It tells you the child needs more proprioceptive input than one session provides. Don't extend indefinitely, but acknowledge: "Your body wants more. That's okay. We'll do this again at [next scheduled time]."
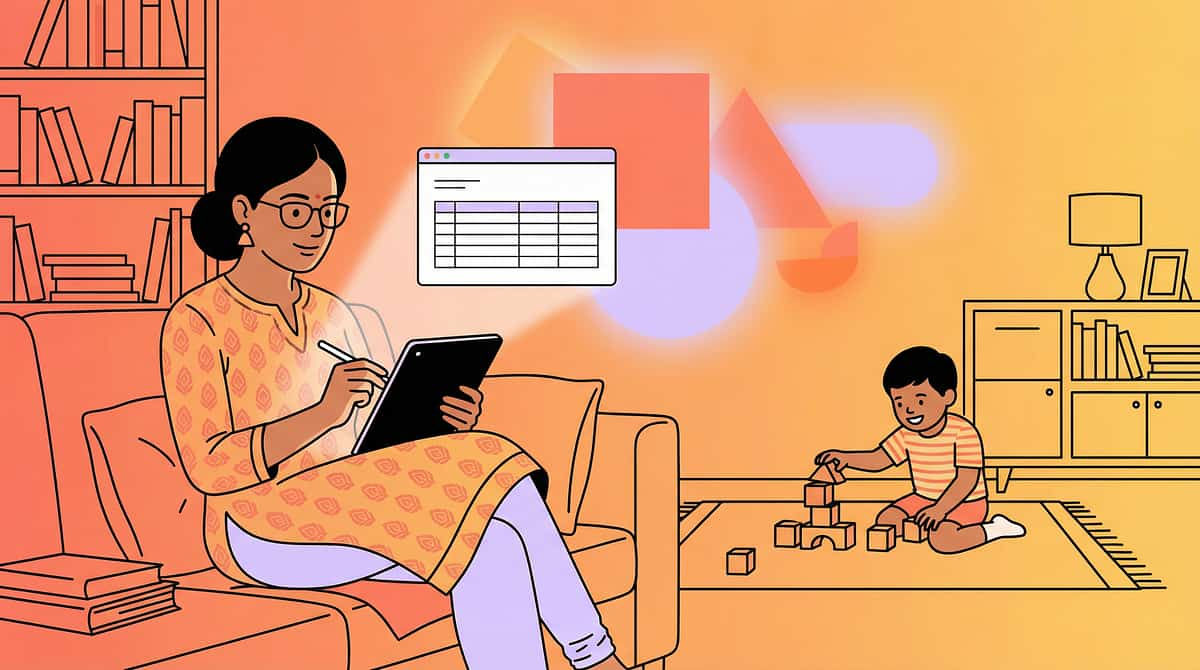
Capture the Data — Right Now
Within 60 seconds of session end, record these three simple data points. This tracking is what transforms isolated sessions into a coherent, progressive therapeutic strategy.
1. Which Materials Used Today?
☐ Weighted Blanket ☐ Compression Vest ☐ Body Sock ☐ Crash Pad ☐ Lap Pad ☐ Therapy Ball ☐ Squeeze/Tunnel ☐ Heavy Work ☐ Chew Tools
2. Engagement Level
🟢Enthusiastic — sought out materials, stayed engaged
🟡Tolerant — used briefly, needed encouragement
🔴Resistant — refused or showed distress
🟡Tolerant — used briefly, needed encouragement
🔴Resistant — refused or showed distress
3. Post-Session State
🟢Visibly calmer
🟡Same as before
🔴More agitated
🟡Same as before
🔴More agitated
Optional notes: Time of day, duration of engagement, specific material that worked best, any material rejected.
"60 seconds of data now saves hours of guessing later."

What If It Didn't Go As Planned?
Session abandonment is not failure — it's data. Here are the most common challenges families encounter, with specific solutions for each.
Child refused all materials
Remove demand completely. Leave materials in the environment. Many proprioceptive seekers will self-approach when not pressured. Try again tomorrow — same setup, zero demand. If refusal persists 5+ days, consult OT for sensory profile refinement.
Child became MORE agitated
Material may have been over-stimulating (too heavy, too tight, too enclosed). Reduce intensity: lighter blanket, shorter body sock time, lower crash height. If agitation persists, the seeking behavior may have a different function — consult your professional team.
Child crashed dangerously
Establish clear crash rules: "We crash body-first, feet toward the pad." Model safe crashing. Add visual boundary markers. If head-impact seeking persists, seek urgent OT evaluation — this may require specialized intervention.
No change in regulation
The material may not provide enough input for this child's threshold. Try heavier blanket (within safety guidelines), more intense heavy work, longer compression time. Some children need a combination of materials simultaneously.
Child loved one, refuses all others
This is data, not failure. The child has identified what their body needs most. Build from there. Gradually introduce variety once the primary material becomes a trusted tool.
Family thinks you're "spoiling" the child
Share Card 3 (neuroscience). This is meeting a physiological need — identical to giving a hungry child food. The need doesn't go away by ignoring it. Share this page with family.

Adapt & Personalize — No Two Children Are Identical
Easier Version
For bad days, initial introduction, or younger children. One material only (weighted blanket). No demands — material just available. Shorter duration (2–5 min). Parent models use first. Lightest weight.
Standard Version
As described in Steps 1–6. 2–3 materials per session. Guided but child-led. 10–20 minutes. Regular daily schedule. Appropriate weight/resistance.
Advanced Version
Full sensory diet with all 9 materials across the day. Child self-selects independently. Combined materials simultaneously. Heavy work challenges with increasing resistance. Self-monitoring and self-reporting.
Age-Based Modifications
1
Toddler (2–3)
Weighted blanket, crash pad, heavy work play. Keep it playful. Short bursts only.
2
Preschool (3–5)
Add body sock, therapy ball, structured heavy work. Games and characters motivate engagement.
3
School Age (6–12)
Add compression vest for school, weighted lap pad for desk, chew tools for class. Teach self-identification.
Sensory Seeker vs. Sensory Avoider: This technique is for SEEKERS. If your child AVOIDS pressure, see → A-001: 9 Materials for Touch Sensitivity at techniques.pinnacleblooms.org.

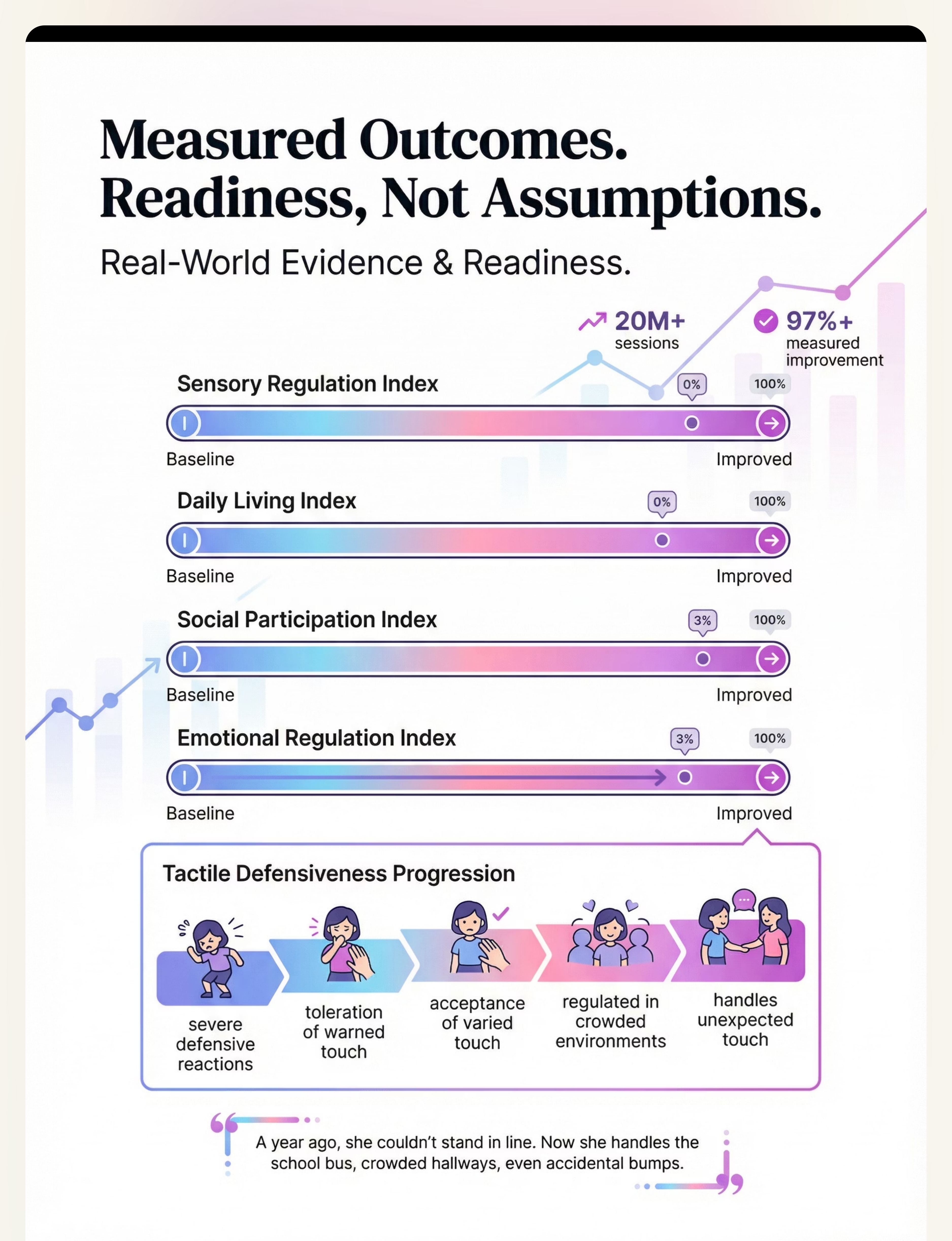
ACT IV: THE PROGRESS ARC
Week 1–2: What to Expect
15%
Progress Bar
You're at the beginning — building the foundation
What "Progress" Looks Like
- Child tolerates weighted blanket for 3 seconds longer than last week — that's real progress
- Child approaches the crash pad independently (even once)
- Crashing intensity on the pad increases — they're USING the tool
- Child allows compression vest for 5 minutes without removing
- Any reduction in unsafe crashing locations (walls → pad even once)
What Is NOT Progress Yet
- Complete elimination of seeking behaviors (unrealistic)
- Child independently selecting tools every time
- Full 20-minute structured sessions without redirection
- Calm throughout the entire day
Parent emotional preparation: Weeks 1–2 feel messy. The neurological change is happening beneath what you can see. Proprioceptive neural pathways are forming. Trust the process.

Week 3–4: Consolidation Signs
40%
Progress Bar
Neural pathways are forming — consolidation is underway
Consolidation Indicators
Child begins to anticipate sensory time — runs to crash pad, requests blanket
Unsafe seeking behaviors noticeably decrease (fewer wall crashes, less tackling)
Child shows material preference — you now know WHICH tools are most effective
Post-input calm periods lengthen from 5 minutes to 15–30 minutes
Child may spontaneously seek weighted blanket at bedtime
Behavioral Changes Signaling Neural Pathway Formation
Child starts doing heavy work without being prompted (carrying things "just because"). Child wraps self in blanket before challenging activities — this is self-regulation emerging. Force modulation begins improving — slightly gentler with peers and objects.
When to increase: If consolidation signs are emerging, increase heavy work frequency from 2x to 3-4x daily. Consider compression vest during school hours. Extend weighted blanket time if child requests it.

Week 5–8: Mastery Indicators
75%
Progress Bar
Approaching mastery — self-regulation emerging
Mastery Criteria — Specific, Observable, Measurable
Independent Access
Child independently requests or accesses deep pressure tools when dysregulated — without prompting from adults
Behavior Reduction
Unsafe seeking behaviors reduced by 50%+ from baseline. Wall crashes, tackling, and head-banging significantly decreased.
Verbal Self-Advocacy
Child can verbalize or gesture body needs: "I need my blanket" / "I need to crash" — naming the internal experience
Generalization
Child uses strategies outside the home — school, grandparents' house. Modifies strategy for context (chew tool at school, crash pad at home).
Mastery doesn't mean the need disappears. It means the child knows how to meet it. If you remove tools for 2–3 days and seeking behaviors return, the child still needs them — this is not dependency. It's meeting a persistent neurological need.
🎉 Celebrate This Win
You did this.
Five to eight weeks ago, you arrived at this page scared, confused, and exhausted. Your child was crashing into walls. You were squeezing as hard as you could and it was never enough. Other people thought your child was aggressive. You weren't sure what was happening.
Now your child has tools. Your child's body is getting what it needs. The crashes go to the crash pad. The squeezing comes from the vest, the blanket, the body sock. The heavy work is built into the day. The seeking hasn't disappeared — but it doesn't need to. It's met. Appropriately. Safely. On your child's terms.
You gave your child the language of their own body.
📸Document this milestone. Take a photo of your child's regulation zone. Write down the moment you first noticed the change. This is yours to keep.
🚩 Red Flags — When to Pause and Seek Guidance
Even in the celebration zone, certain signs mean PAUSE. Trust your instincts — if something feels wrong, stop and ask for professional guidance.
Head-Banging Causing Injury
Despite crash pad availability, child continues head-impact seeking causing bruising, swelling, or skin breakage. → Immediate OT evaluation. Safety planning required.
Escalating Intensity
Instead of stabilizing with materials, child requires progressively more intense input — heavier blankets, harder crashes, squeezing never satisfying. → Consult OT for threshold reassessment.
Self-Injurious Behavior
Biting self, pinching self, hitting face — seeking that crosses into self-harm. → Urgent multidisciplinary evaluation (OT + ABA + NeuroDev Pediatrics).
No Calming Effect After 4+ Weeks
Zero change in regulation despite consistent use. Sensory profile may be more complex. Comprehensive evaluation needed.
New Behaviors Emerging
Proprioceptive seeking addressed but new patterns appearing (auditory distress, visual avoidance, feeding regression). Expanding profile — full evaluation indicated.
Sleep Worsening
Despite weighted blanket, sleep deteriorates. Medical evaluation needed to rule out sleep disorder, anxiety, or medication effects.

The Progression Pathway — Your Developmental GPS
This technique doesn't exist in isolation. It's part of a carefully mapped progression pathway designed to build your child's regulation skills systematically.
Long-Term Developmental Goal: Independent sensory self-regulation — your child recognizes, communicates, and independently meets proprioceptive needs across all settings.
Related Techniques — Sensory Processing Domain
Your child's deep pressure materials overlap with many other sensory processing techniques in the Pinnacle system. Here are the most closely related protocols.

A-001: Touch Sensitivity Materials
Tactile Defensiveness | Intro Level. 9 materials for children who are over-responsive to touch.

A-009: Sand Play Avoidance
Tactile Processing | Intro Level. Graded exposure and desensitization for texture avoidance.

A-024: Hair Brushing Battles
Tactile Processing | Core Level. Structured approach to desensitizing scalp touch sensitivity.

A-026: Child Avoids Movement
Vestibular Processing | Core Level. For children who are under-responsive to movement input.

A-027: Clumsy & Bumping
Proprioceptive-Motor | Core Level. Addressing body awareness and spatial orientation challenges.

A-035: Chews on Everything
Oral Sensory Seeking | Core Level. Deep dive into oral proprioception and safe chew alternatives.
💡You already own materials for techniques #1, #3, and #4 — many Canon materials apply across the sensory processing domain.
Your Child's Full Developmental Map
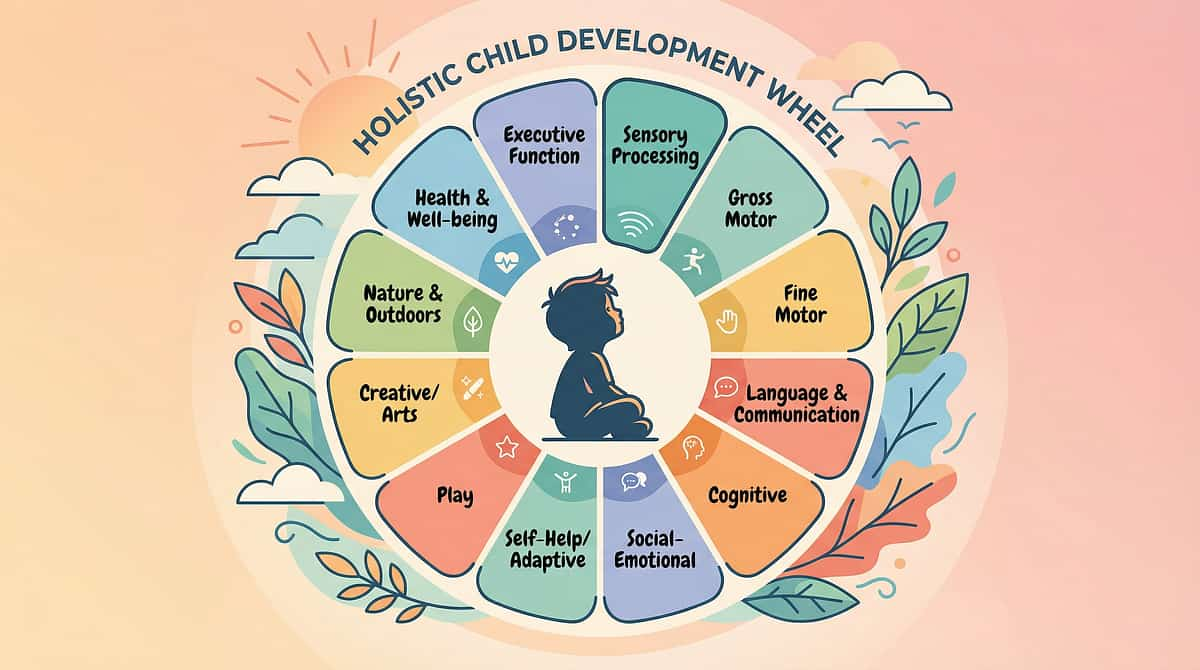
This technique sits in Domain A: Sensory Processing — but its effects ripple across behavior, motor skills, daily living, sleep, and social skills. Proprioceptive regulation is foundational infrastructure that supports everything built on top of it.
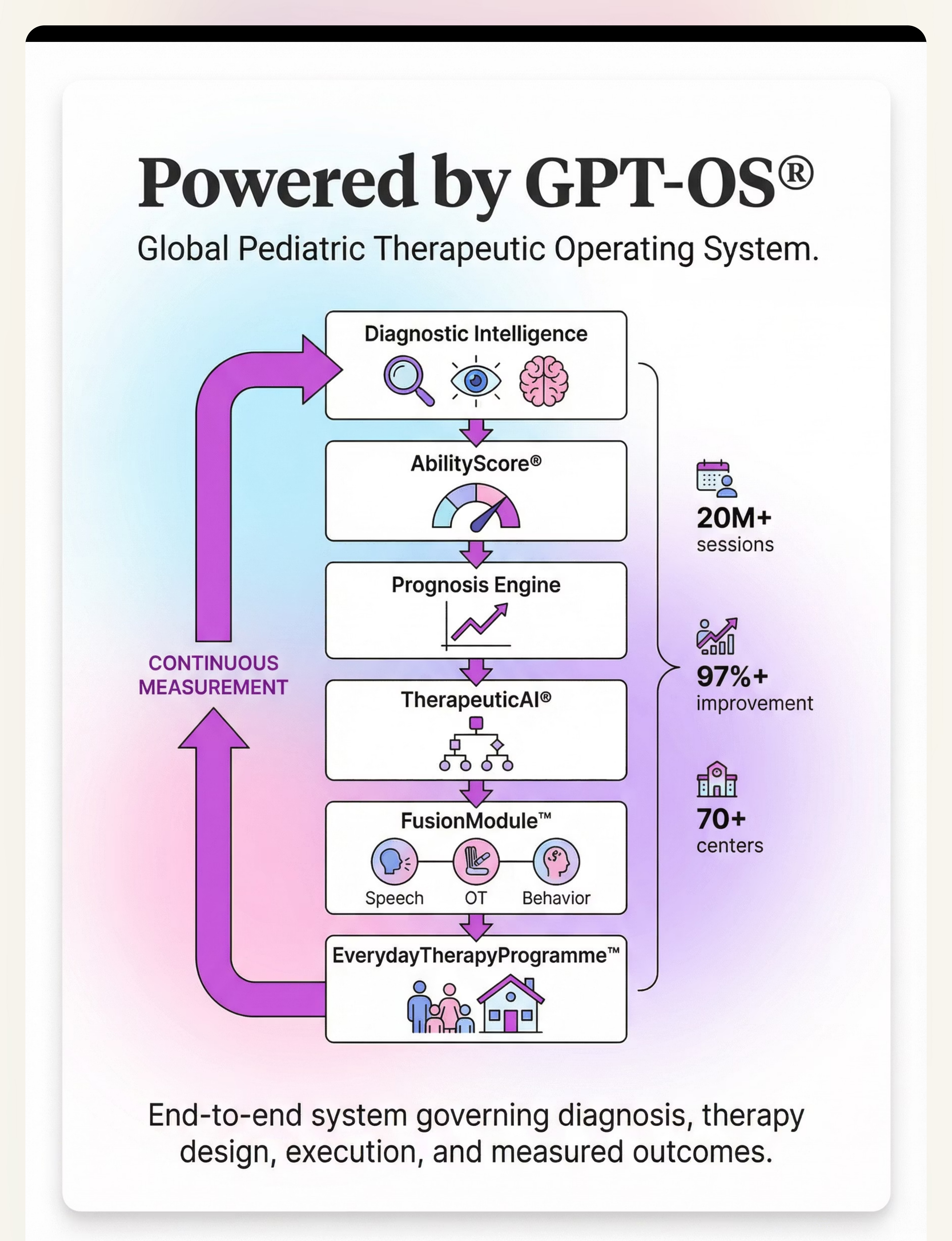
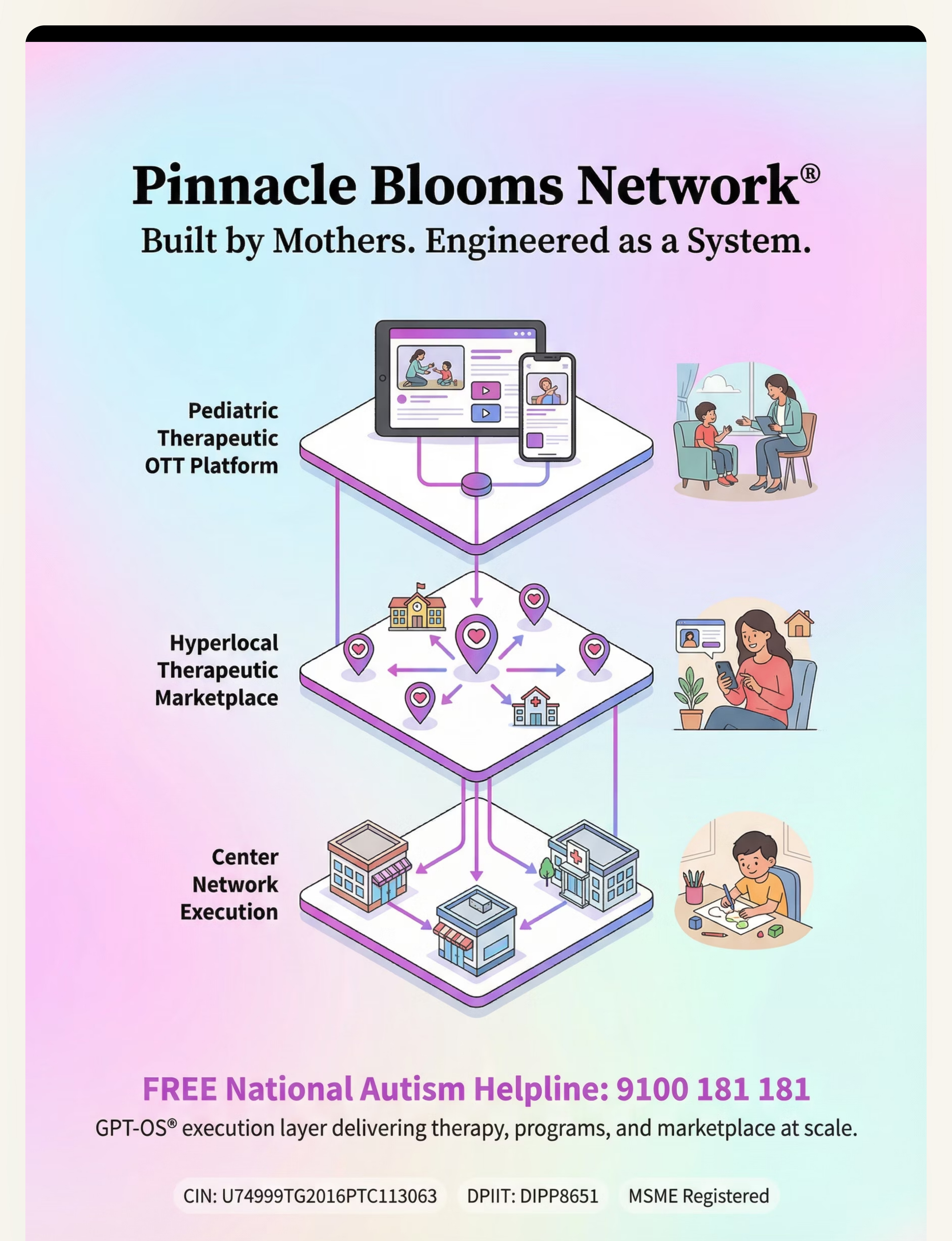
"This technique is one piece of a larger plan. Your child's development is a 12-domain system. GPT-OS® helps you see the full picture."
ACT V: THE COMMUNITY & ECOSYSTEM
Families Who've Been Here
Family Story 1
Before: "My 4-year-old would crash into every wall, every person, every piece of furniture. Other parents pulled their children away at the playground. He'd tackle other kids — not angry, just hungry for contact. I was ashamed and exhausted."
After (8 weeks): "The crash pad changed everything. He has a place now. He runs to it when he feels the need building. Wall crashes are down to almost zero. He told me last week: 'Mama, my body needs a crash.' He NAMED it."
Family Story 2
Before: "She'd wrap herself in blankets so tight I worried she'd suffocate. Every night was a battle — she couldn't settle without being squeezed. I'd squeeze her for 30 minutes until my arms gave out."
After (6 weeks): "The weighted blanket gave her what my arms couldn't. She puts it on herself. She sleeps through the night now. Last week she said 'I need my heavy blanket' before I even suggested it."
From the Therapist's Notes:"Both families presented with proprioceptive under-responsivity profiles. Once appropriate outlets were provided, the dysregulated behaviors decreased not because the need went away — but because it was being met."
Note: Anonymized cases from Pinnacle Network. Illustrative; outcomes vary by child profile.
Connect With Other Parents
You are not a solo operator. Thousands of families are navigating proprioceptive seeking challenges right now, and connecting with them can transform your journey from isolation to shared strength.
💬 WhatsApp Community
Sensory Processing Parent Community — share strategies, ask questions, celebrate wins in real time with families like yours.
🌐 Online Forum
Pinnacle Parent Forum — deeper discussions, organized by technique and domain, with therapist participation and moderation.
📍 Local Meetups
In-person gatherings organized by your nearest Pinnacle center. Meet families in your community navigating the same challenges.
🤝 Peer Mentoring
Connect one-on-one with an experienced parent who has walked this path and can offer guidance, empathy, and practical tips.
Your Professional Support Team
Home-based intervention works best when supported by professional guidance. You don't have to figure this out alone. Here's how to connect with the right specialists for your child's needs.
Primary: Occupational Therapist
Sensory Integration specialist who designs individualized sensory diets, selects materials based on your child's specific profile, and monitors progression.
Supporting: Board Certified Behavior Analyst
Designs regulation protocols, reinforcement schedules, and teaches the child to self-identify needs and independently access tools.
If Oral Seeking: Speech-Language Pathologist
Evaluates oral motor patterns, designs chew tool protocols, and addresses feeding and articulation challenges connected to jaw proprioception.
What to Ask at Your First Appointment
- "Can you conduct a comprehensive sensory processing evaluation?"
- "Can you design an individualized sensory diet for my child's proprioceptive needs?"
- "Which specific materials and weights are right for my child's body and profile?"
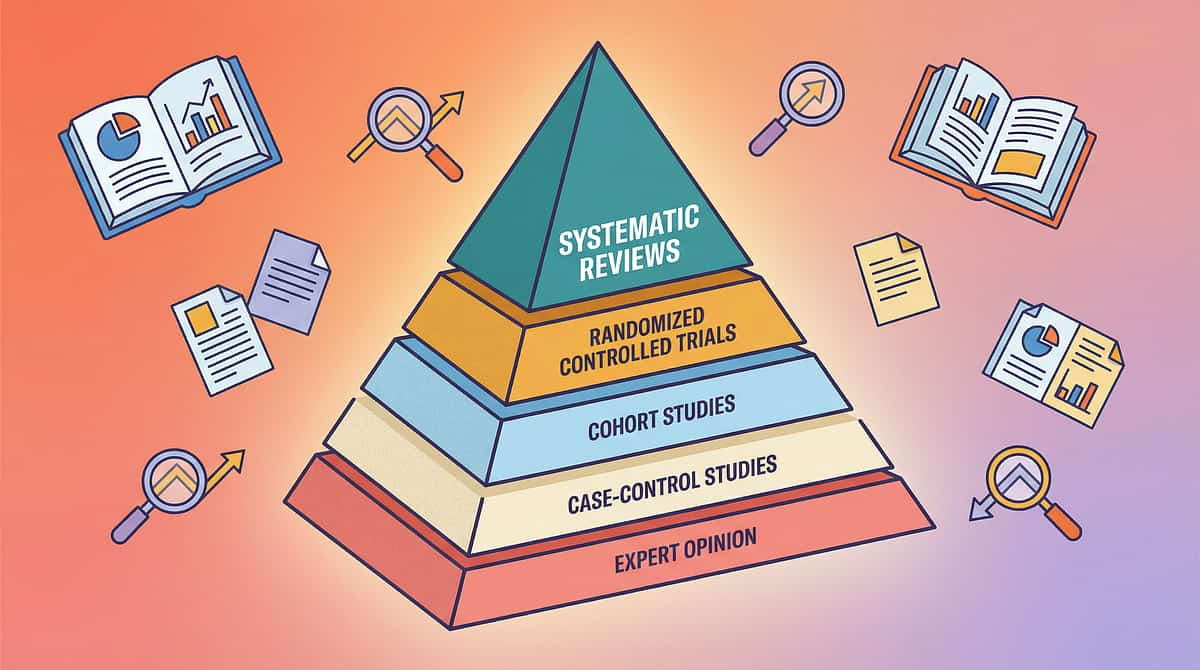
The Research Library — For the Curious Parent
Every recommendation on this page is grounded in peer-reviewed research. Here are the key studies that inform this protocol, organized by evidence level.
1
Systematic Reviews
2
RCTs & Meta-Analyses
3
Cohort Studies
4
Case Studies & Expert Opinion
PRISMA Systematic Review (2024)
16 articles (2013-2023) confirm sensory integration as evidence-based practice for children with ASD. PMC11506176
Meta-Analysis: SI Therapy (2024)
24 studies — effectively promotes social skills, adaptive behavior, sensory processing, motor skills. PMC10955541
Indian RCT — Home-Based (2019)
Padmanabha et al. — Significant outcomes with parent-administered protocols in Indian pediatric population. DOI: 10.1007/s12098-018-2747-4
WHO Nurturing Care Framework (2018)
Caregiver-mediated, context-specific, equity-focused developmental interventions across 54 LMICs. nurturing-care.org
WHO CCD Package (2023)
Household-material-based intervention efficacy. Implemented in 54 countries. PMC9978394
Frontiers in Integrative Neuroscience (2020)
Comprehensive framework for evaluating sensory integration treatment in ASD. DOI: 10.3389/fnint.2020.556660
Additional Foundations: Ayres, A.J. — Sensory Integration Theory | Grandin, T. — Deep pressure & squeeze machine research | AOTA Clinical Guidelines | SPD Foundation: spdfoundation.net
How GPT-OS® Uses Your Data
Your tracking data doesn't just sit in a file. GPT-OS® processes it to deliver increasingly personalized recommendations for your child's sensory regulation journey.
What GPT-OS® Learns from This Technique's Data
- Which of the 9 materials produce the strongest regulation effect for YOUR child
- Optimal time of day for proprioceptive input sessions
- Duration threshold before diminishing returns
- Material combinations that compound effectiveness
- Progress velocity compared to similar profiles
Encrypted Storage
Data stored within sovereign Indian infrastructure
Never Sold
No data sold to third parties — ever
You Own It
Request deletion at any time
Watch the Reel — A-025
Reel ID: A-025 | Series: Sensory Solutions — Episode 25 | Duration: ~75 seconds
This 60-second Reel walks you through all 9 materials with visual demonstrations — what each material looks like in use, the before-and-after regulation effect, and how to introduce them to your child. Seeing the materials in action reinforces everything you've read on this page and gives you the visual confidence to begin.
Coming next in the series: A-026 — 9 Materials That Help When Child Avoids Movement
Share This With Your Family
If only one caregiver understands these tools, the impact is limited. Consistency across caregivers multiplies impact. Every person who interacts regularly with your child should understand why these materials matter and how to support their use.
Family Guide (1-page PDF)
Simplified overview of all 9 materials, safety rules, and daily schedule. Print-friendly for refrigerator posting.
"Explain to Grandparents" Version
Plain language, no clinical terms. Explains WHY the child crashes, WHAT the tools do, and HOW grandparents can support.
Teacher Communication Template
Professional letter explaining sensory needs and requesting accommodations — weighted lap pad, movement breaks, chew tool permission.
Reference: WHO CCD Package — multi-caregiver training critical for intervention generalization | PMC9978394
ACT VI: THE CLOSE & LOOP
Frequently Asked Questions
1
Will my child become dependent on weighted blankets?
Providing appropriate proprioceptive input allows the nervous system to develop and mature. Over time, many children's thresholds shift and they require less intense input. Some children use weighted blankets long-term — and that's perfectly fine. Adults use them too. The goal is regulation, not independence from tools.
2
How heavy should the weighted blanket be?
Approximately 10% of child's body weight plus 1-2 pounds. A 20kg child → 2-2.2kg blanket. NEVER exceed this. Too heavy is a safety risk. Child MUST be able to remove the blanket independently. Consult OT for precise recommendation.
3
My child is only 2 years old. Too early?
Weighted blankets are NOT safe for children under 2. For toddlers 2-3 years, focus on crash pad play, heavy work activities, and gentle compression (tight hugs, snug clothing). Consult OT for age-appropriate protocols.
4
Can compression vests be worn at school?
Yes — many are designed to be worn under clothing invisibly. May require OT recommendation for formal accommodation. Typically 20-30 minute intervals with breaks, not all day continuously.
5
My child chews everything. Is this related?
Yes. Chewing provides intense proprioceptive input through the jaw muscles. Provide safe chew tools. If chewing is intense and persistent, consider an oral motor evaluation with an SLP.
6
The crash pad seems to make my child MORE hyper.
Initial excitement is normal — the child finally has an outlet. Monitor over 1-2 weeks. If true escalation occurs, modify: fewer crashes, more heavy work (carrying, pushing) which provides input through sustained effort rather than impact.
7
Can I use all 9 materials at once?
Start with 2-3. Observe which produce the strongest regulation effect. Add gradually. An OT can design a sensory diet integrating the right combination for your child's unique profile.
8
How is this different from "letting the child be rough"?
This is structured, evidence-based, and teaches self-regulation awareness. Unrestricted roughness doesn't teach the child to identify needs or access tools. This builds lifetime regulation infrastructure.

Your Next Step — Start Now
You've read the science. You've seen the evidence. You've learned the protocol. Your child's body is waiting for the input it needs. Choose your next step below.
🟣 START THIS TECHNIQUE TODAY
Launch GPT-OS® guided session — personalized material selection, real-time guidance, and data tracking built in.
🔵 BOOK A CONSULTATION
Connect with a Pinnacle OT for personalized sensory diet design tailored to your child's specific profile and needs.
⚪ EXPLORE NEXT TECHNIQUE
Continue to A-026: 9 Materials That Help When Child Avoids Movement — the natural next step in the progression pathway.
Validated by Pinnacle Blooms Consortium
OT • SLP • ABA • SpEd • NeuroDev Pediatrics
Preview of 9 materials that help when child seeks deep pressure Therapy Material
Below is a visual preview of 9 materials that help when child seeks deep pressure therapy material. The pages shown help educators, therapists, and caregivers understand the structure and content of the resource before use. Materials should be used under appropriate professional guidance.





Link copied!
The Pinnacle Promise
🧠 OT
🗣️ SLP
🎯 ABA
📚 SpEd
🩺 NeuroDev
🔬 CRO
"From fear to mastery. One technique at a time."
A parent arrived at Card 1 scared, confused, and exhausted. By Card 5, you understood the science and trusted the evidence. By Card 12, you had the materials and the space was ready. By Card 22, you'd executed the technique and adapted it to your child. By Card 30, you saw the full developmental map and your child's journey. By Card 37, you'd shared the knowledge with your family and community. Now — you act. And the loop restarts with the next technique.
Legal Disclaimer: This content is educational. It does not replace assessment by a licensed occupational therapist specializing in sensory processing. Deep pressure seeking can reflect proprioceptive processing differences, sensory modulation challenges, anxiety, or other factors requiring individualized evaluation. Individual results may vary. Weighted products have safety guidelines that must be followed.
© 2025 Pinnacle Blooms Network®, unit of Bharath Healthcare Laboratories Pvt. Ltd. All rights reserved. CIN: U74999TG2016PTC113063 | DPIIT: DIPP8651 | MSME Registered. Powered by GPT-OS® — Global Pediatric Therapeutic Operating System.