
"The screaming starts the moment we walk toward the bathroom."
You are not failing. Your child's nervous system is speaking — loudly — and it is saying: this feels unsafe. What looks like defiance is almost always distress. And distress has answers.
E-495 | Self-Care & Daily Living
Age 2–10 Years
OT-Validated
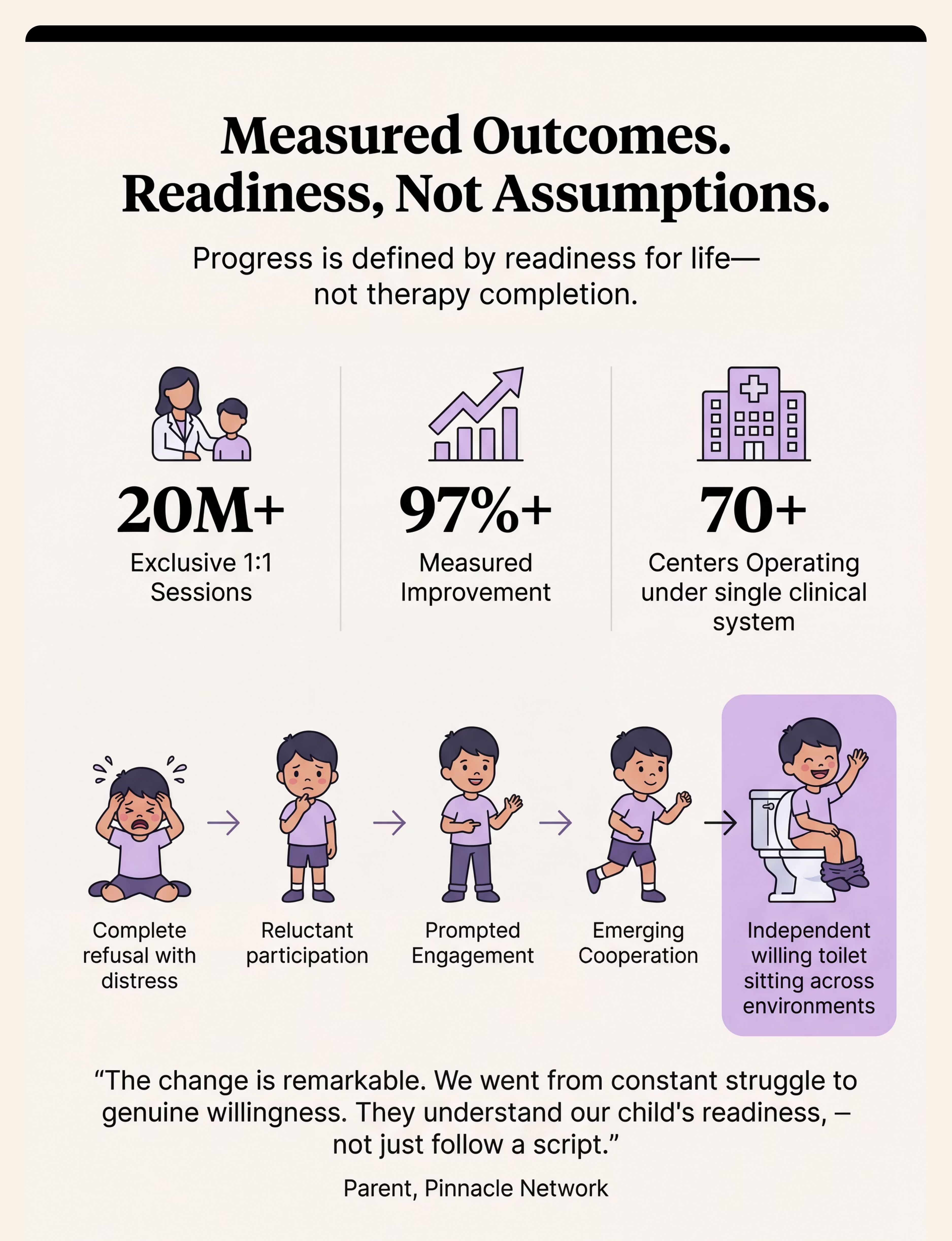
9 Materials That Help When Child Refuses Toilet Sitting — Pinnacle Blooms Network® | OT · SLP · ABA · SpEd · NeuroDev · CRO. "Built by Mothers. Engineered as a System." 97%+ of children in our network with toilet sitting refusal achieved willing, independent sitting — with the right approach.

1 in 3 Children on the Autism Spectrum Faces Significant Toilet Sitting Refusal
You are among millions of families navigating this exact challenge — across India, across 70+ countries where Pinnacle families live. Toilet sitting refusal is not rare, not shameful, not a parenting failure. It is a documented clinical phenomenon with documented clinical solutions.
80%
Sensory Difficulties
Children with ASD experience sensory processing difficulties affecting self-care routines
1 in 3
Face Toileting Challenges
Children with autism face significant toileting challenges — the most underreported self-care barrier
2–4 yrs
Peak Refusal Age
Average age when toilet sitting refusal peaks — and when intervention is most effective
India Context: An estimated 1.8–2 million children on the autism spectrum in India. Toilet independence is among the top 3 parental concerns in every national survey. You are in a vast, struggling, and ultimately succeeding community.
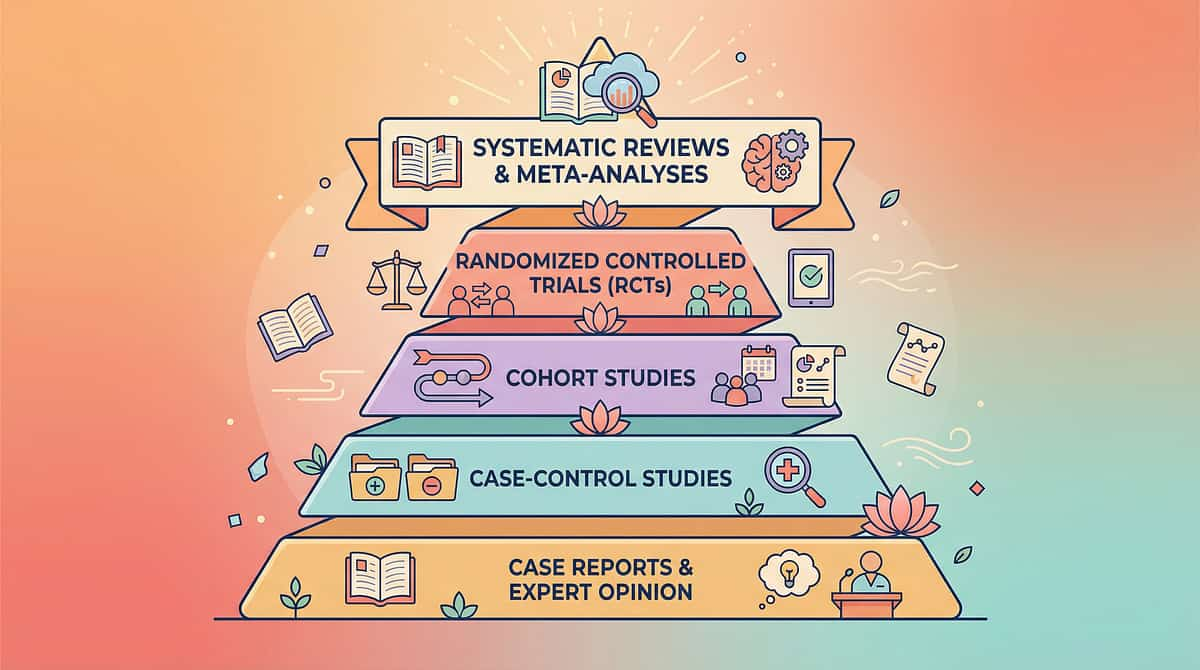
Sources: PRISMA Systematic Review (2024), PMC11506176 | PMC10955541 | DOI: 10.12998/wjcc.v12.i7.1260
This Is Not Stubbornness. This Is Neuroscience.
The Sensory Processing Cascade
Toilet seat contact (tactile input)
Somatosensory cortex: OVER-AMPLIFIES signal
Amygdala: THREAT detected
Fight-or-flight response ACTIVATES → Rigid body · Arching · Screaming
For children with sensory differences, a cold hard toilet seat registers as a GENUINE THREAT — not mild discomfort.
What This Means in Plain Language
Your child's brain receives sensory information differently. The cold, hard seat — or feet dangling in space — or harsh bathroom lights — is not processed as "slightly uncomfortable." It processes as dangerous.
The arching, rigid body, screaming — these are not manipulation. They are the same fight-or-flight responses a frightened animal shows. You cannot force a child through a perceived survival threat and expect learning to happen. You can only change what the toilet represents to their nervous system.
🔵 Tactile System
Cold/hard seat registers as aversive or painful
🟡 Vestibular System
Dangling feet = no ground reference = instability signal
🟢 Proprioceptive
No handles to grip = no body-position security
Frontiers in Integrative Neuroscience (2020): DOI: 10.3389/fnint.2020.556660
Your Child Is Here. Here Is Where We're Heading.
The developmental window for toilet training is wider than most people realize — especially for children with ASD or sensory differences. The timeline extends. The approach changes. The destination remains the same — and it is absolutely reachable.
Age 1–2
Bladder awareness begins
Age 2–3
Toilet introduction window
Age 3–4
Sitting tolerance, routine — E-495 Zone
Age 4–6
Independent toileting in familiar settings
Age 6–10
Generalized mastery — all settings
Toilet sitting refusal commonly co-occurs with: Sensory Processing Disorder (SPD) · Generalized Anxiety · Constipation (creates pain → avoidance → deeper refusal) · Tactile Defensiveness · Vestibular Hypersensitivity. Always rule out constipation first — pain creates aversion that looks identical to sensory refusal.
WHO Care for Child Development (CCD) Package | PMC9978394 | WHO/UNICEF CCD Package (2023)

Clinically Validated. Home-Applicable. Parent-Proven.
Every recommendation in E-495 is drawn from occupational therapy, ABA, behavioral psychology, and sensory science. Each material has a clinical mechanism. Nothing here is guesswork. — Pinnacle Blooms Consortium, OT-SLP-ABA-SpEd-NeuroDev
🏅 Evidence Level I
Systematic Review (2024)
16 peer-reviewed articles (2013–2023) confirm sensory integration intervention is evidence-based practice for children with ASD.
PMC11506176
📊 Meta-Analysis (2024)
24 Studies Confirmed
Sensory integration therapy effectively promoted adaptive behavior, sensory processing, motor skills, and social functioning.
PMC10955541 | World J Clin Cases
🇮🇳 Indian RCT (2019)
Home-Based, Validated
Home-based sensory interventions showed significant, measurable outcomes in Indian pediatric populations — validating parent-administered approaches.
Padmanabha et al., Indian J Pediatr
NCAEP 2020 Evidence-Based Practices
AOTA Pediatric Self-Care Guidelines
WHO NCF 2018
UNICEF CCD Package 2023

E-495 | OT-TSR: What This Technique Is
Technique Code E-495
Toilet Sitting Refusal Intervention — Material-Based Sensory & Behavioral Approach
Parent-Friendly Name: "Making the Toilet Safe Enough to Sit On"
A structured, multi-material approach that systematically addresses the sensory, vestibular, anxiety, and behavioral factors causing children to refuse sitting on the toilet. Rather than overriding the child's nervous system through force or repetition, this approach modifies the environment, materials, and interaction sequence until the toilet is genuinely safe and tolerable for the child's nervous system.
Technique Parameters
Age Range
2–10 years
Session Duration
5–15 minutes per attempt
Frequency
2–4 daily toilet opportunities
Setting
Home bathroom (primary) + school/public generalization
Lead Discipline
Pediatric OT + ABA

This Technique Crosses Every Therapy Boundary
"The brain doesn't organize by therapy type. Neither does toilet training."
Occupational Therapist (Lead)
Identifies sensory triggers. Selects tactile, vestibular, and proprioceptive adaptations. Designs the environmental modification plan. Guides graduated exposure protocol.
ABA / BCBA Therapist
Designs reinforcement systems. Structures gradual exposure ladder as behavior protocol. Analyzes function of refusal behavior. Implements token economy and preference assessment.
Special Education Teacher
Generalizes toilet sitting protocol to school settings. Maintains visual supports in the school bathroom. Communicates progress across home-school environments.
Developmental Pediatrician
Rules out medical causes (constipation, UTI, pain). Assesses anxiety disorder vs. sensory processing disorder. Prescribes pharmacological support for severe anxiety where indicated.
Pediatric SLP
Supports communication around toileting needs. Develops non-verbal communication strategies. Creates visual social stories for bathroom routines.
At Pinnacle, all 5 disciplines review this technique together in a single FusionModule™ session. The OT addresses the seat. The BCBA designs reinforcement. The SLP builds the social story. The result is not 5 different interventions — it is 1 converged approach.

A Precision Tool for a Specific Nervous System Challenge
This technique targets a cascade of outcomes — from the immediate goal of calm toilet sitting, through secondary sensory and trust gains, to tertiary developmental milestones that shape your child's entire trajectory.
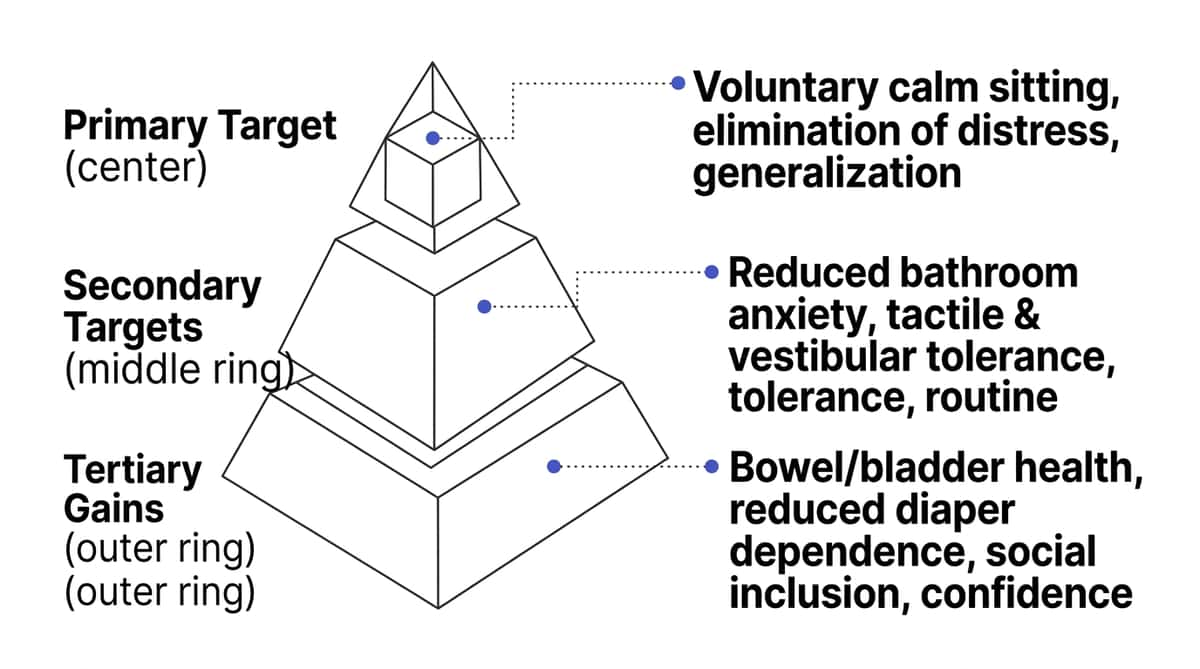
✓ Observable Indicators
Child approaches bathroom without physical resistance · Sits without screaming · Remains seated progressively longer · Communicates toileting needs proactively
Secondary Benefits
Reduced bathroom anxiety · Improved whole-body tactile tolerance · Vestibular security in chairs and swings · Trust between parent and child
Tertiary Gains
School inclusion · Reduced diaper dependency · Dignity & self-esteem · Caregiver burden reduced · Foundation for all self-care skills

9 Materials. Each One Addresses a Different Root Cause.
Before purchasing anything — identify YOUR child's specific trigger. A child scared of falling in needs different materials than a child who cannot tolerate the cold seat. The right material is the one that addresses YOUR child's source of distress.

1. Padded Cushioned Toilet Seat
Category: Tactile Adaptations Mechanism: Eliminates cold/hard tactile shock — the most common sensory trigger. For children with tactile defensiveness, padding transforms first-contact from threat to tolerable. For many children, this single change eliminates refusal. Price: ₹500–2,000 | DIY: Thick towel secured over seat

2. Toilet Seat Reducer with Handles
Category: Stability & Positioning Mechanism: Smaller opening prevents falling-in fear; handles restore child's sense of control. When a child can grip something, they manage their own stability — shifting sitting from passive (done to them) to active (controlled by them). Price: ₹400–1,500 | Non-slip bottom mandatory
3. Step Stool with Non-Slip Surface
Category: Stability & Positioning Mechanism: Grounds feet → vestibular system deactivates alert signal → child feels safe. Dangling feet signal instability to the ancient vestibular system. Grounded children sit longer, with less anxiety, and are more willing to sit. Price: ₹300–1,200 | Spec: knees at ~90 degrees

4. Visual Social Story for Toilet Sitting
Category: Visual Supports Mechanism: Previews the experience in calm context → unknown becomes familiar → anxiety decreases. Use photos of your child's actual bathroom. Read daily in calm moments — not immediately before bathroom time. Price: ₹200–800 | DIY: 8–10 printed photos, laminated

Materials 5–9: Complete the System

5. Bathroom Sensory Modification Kit
Category: Environmental Modification Mechanism: Reduces cumulative sensory load before child reaches toilet — more capacity available for sitting. Dimmer lighting, soft white noise, warm bath mats, unscented products, and quiet-close seat lids transform the bathroom from sensory assault to sensory haven. Price: ₹500–2,500 (or ₹0 with app solutions)

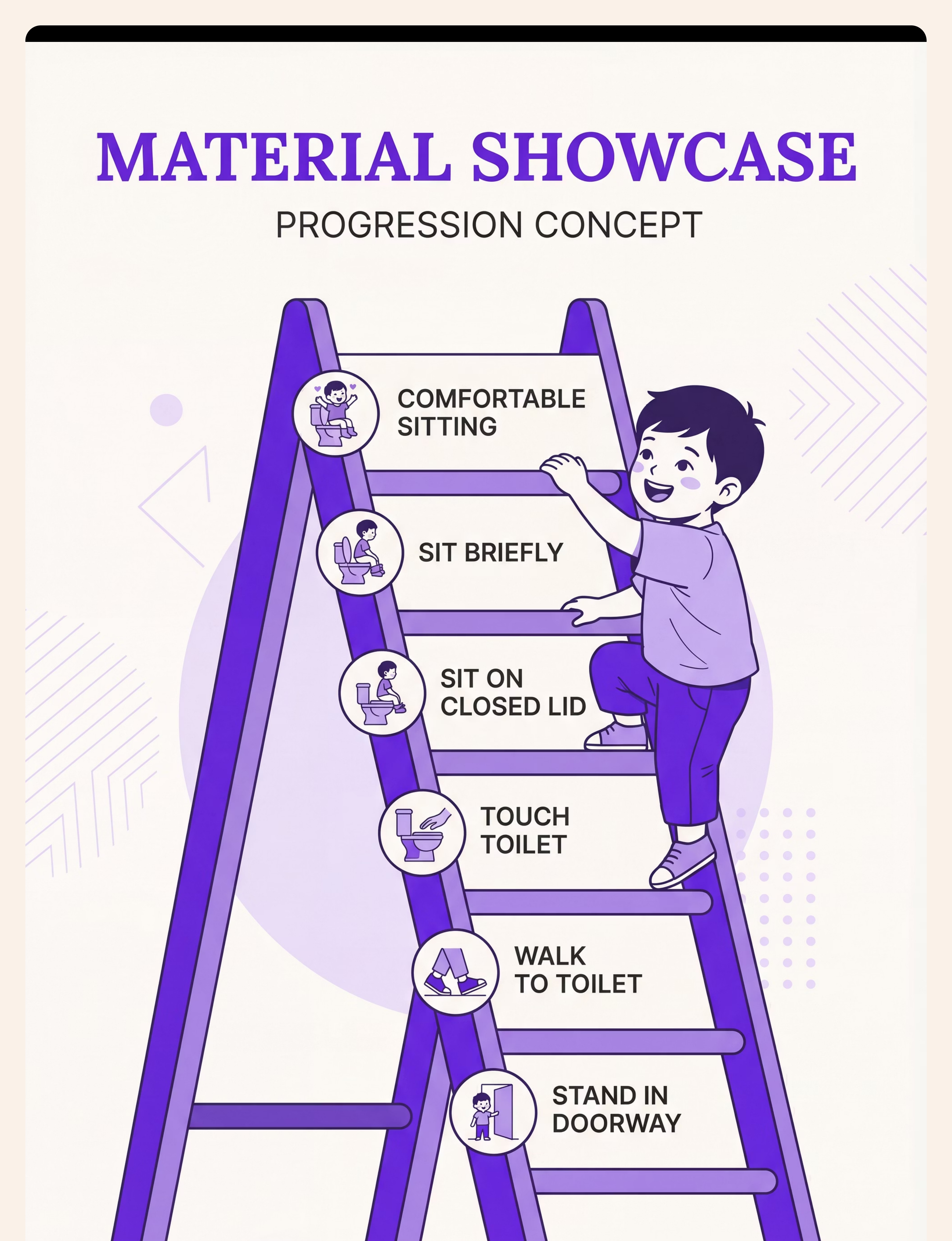
6. Gradual Exposure Visual Ladder
Category: Visual Supports / Desensitisation Mechanism: Breaks impossible journey into achievable steps. Starts at Rung 1 (stand in doorway) through Rung 9 (sitting for progressive durations). Each rung practiced until genuinely comfortable, not just tolerated. Price: ₹200–600 | DIY: Poster board + hand-drawn ladder

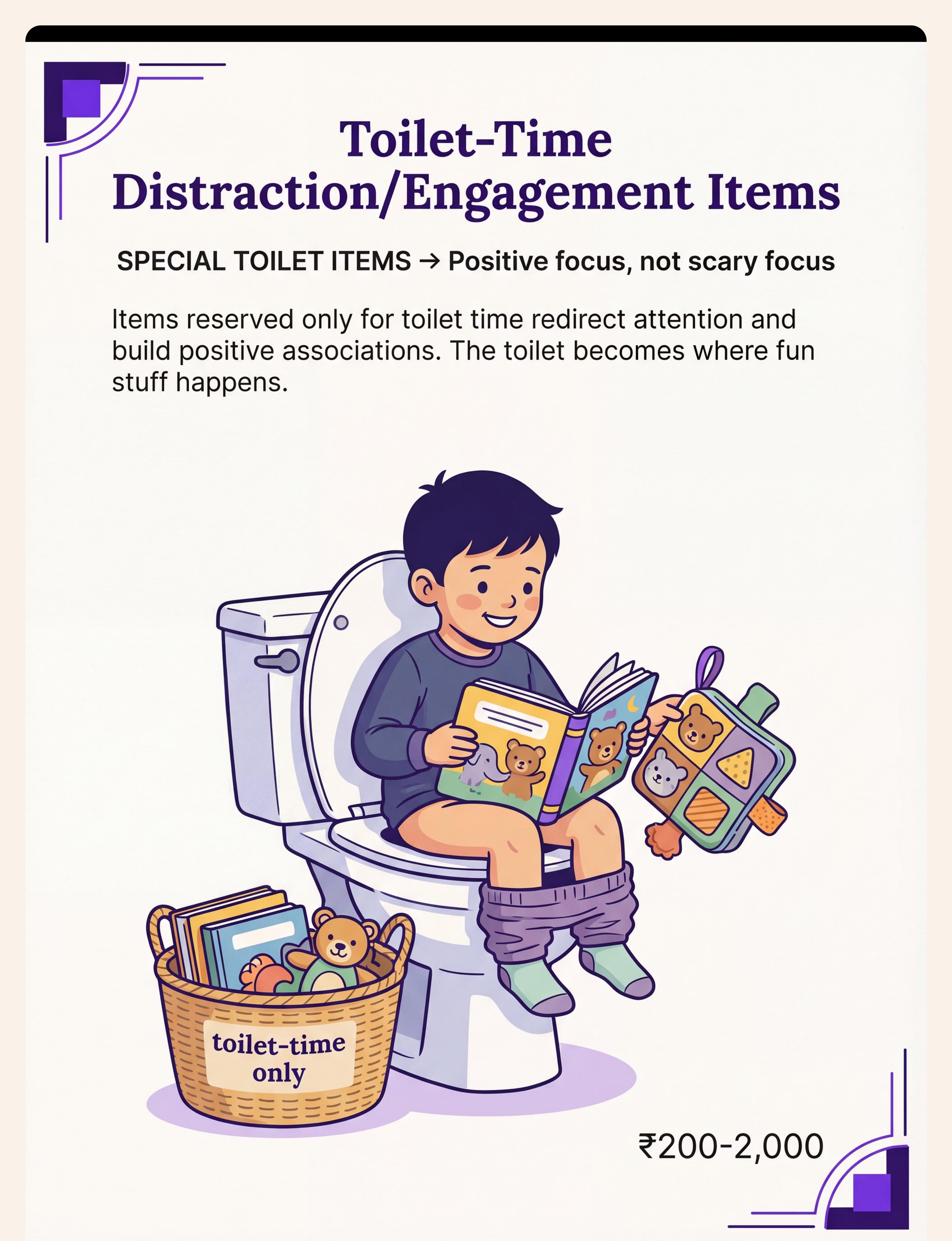
7. Toilet-Time Distraction / Engagement Items
Category: Engagement & Motivation Mechanism: Attention redirected from anxiety to positive stimulus → toilet = positive place. Critical: These items must be exclusive to toilet time only — not available any other time. This creates motivation to sit AND genuine positive conditioning. Price: ₹200–2,000 (items child already loves)
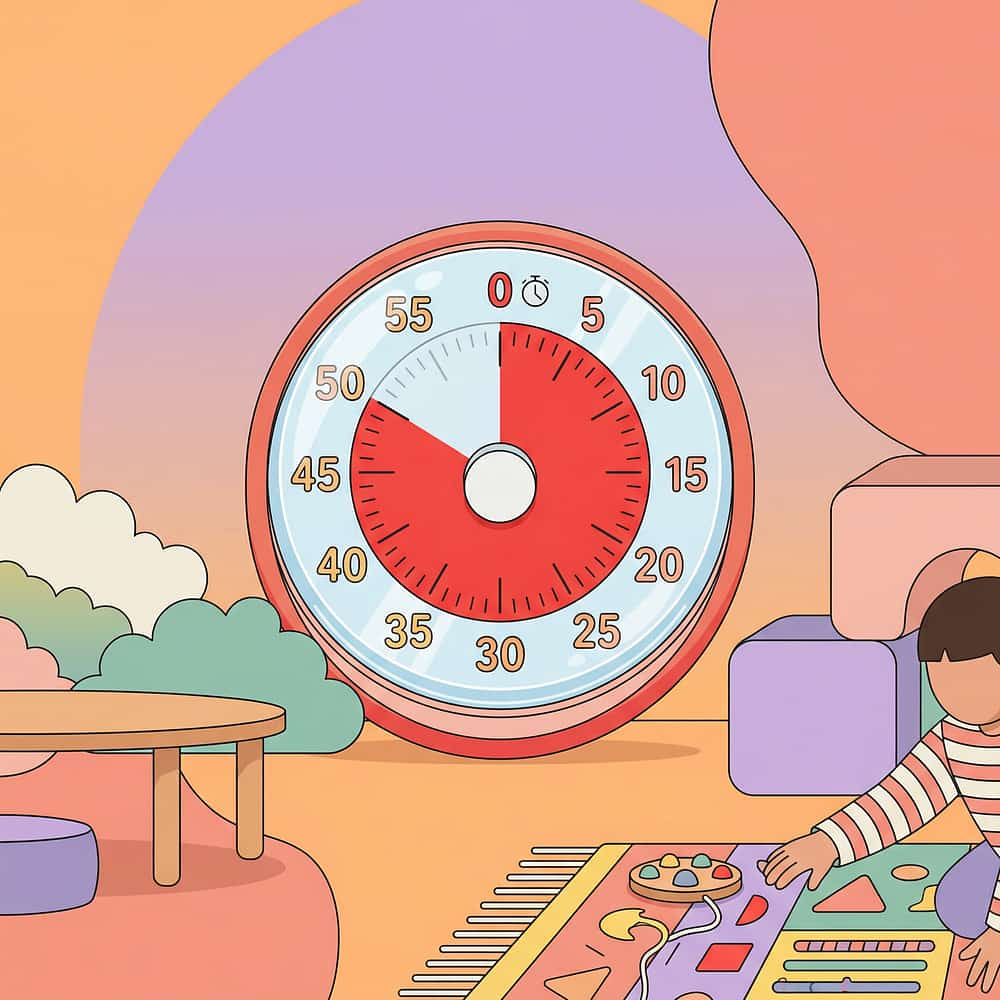
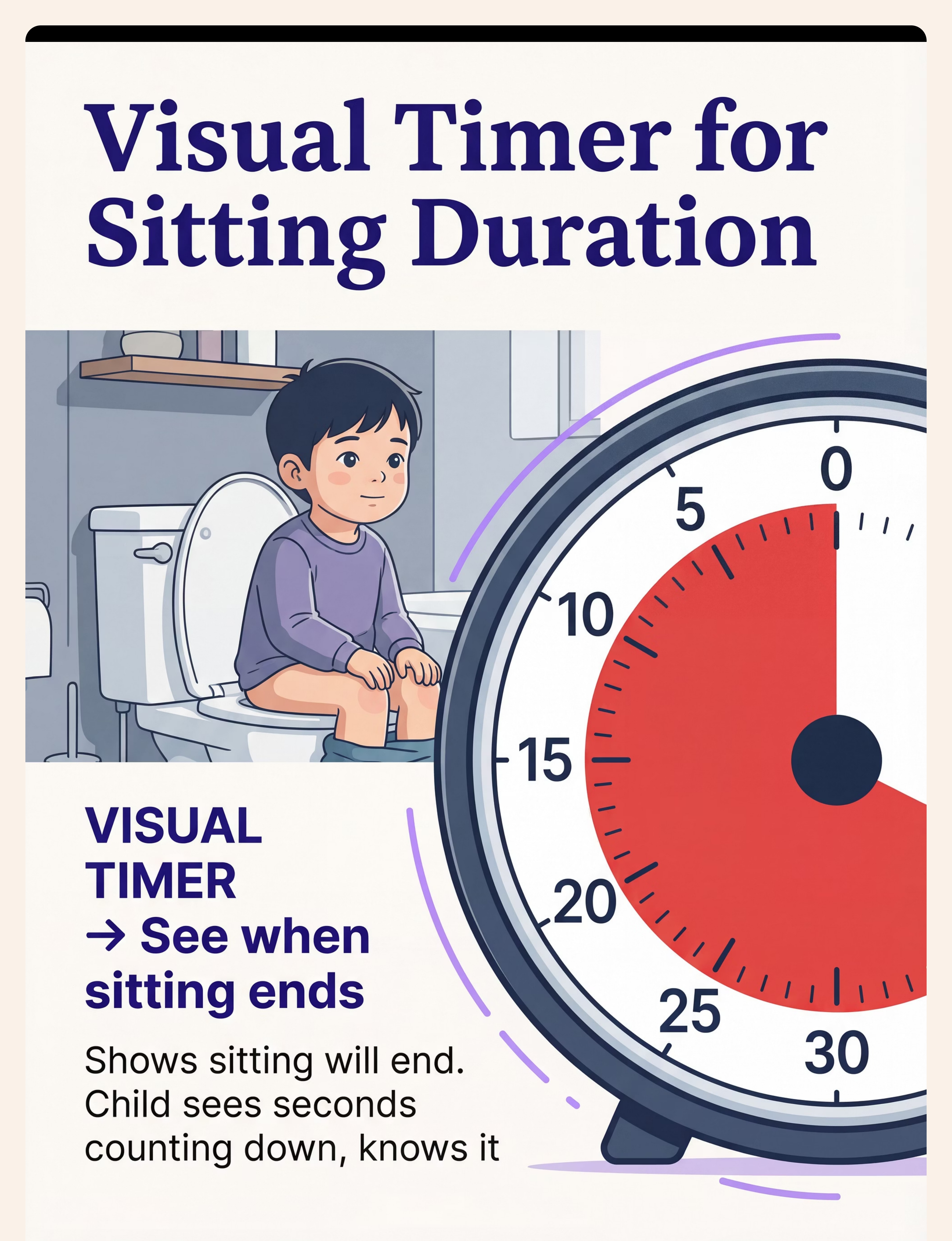
8. Visual Timer for Sitting Duration
Category: Visual Supports / Time Management Mechanism: Makes finite duration visible → removes uncertainty → "I can see when this ends." Start at 10–15 seconds — genuinely brief. Rule: When timer ends, sitting ENDS. Non-negotiable. This consistency builds profound trust. Price: ₹300–1,200
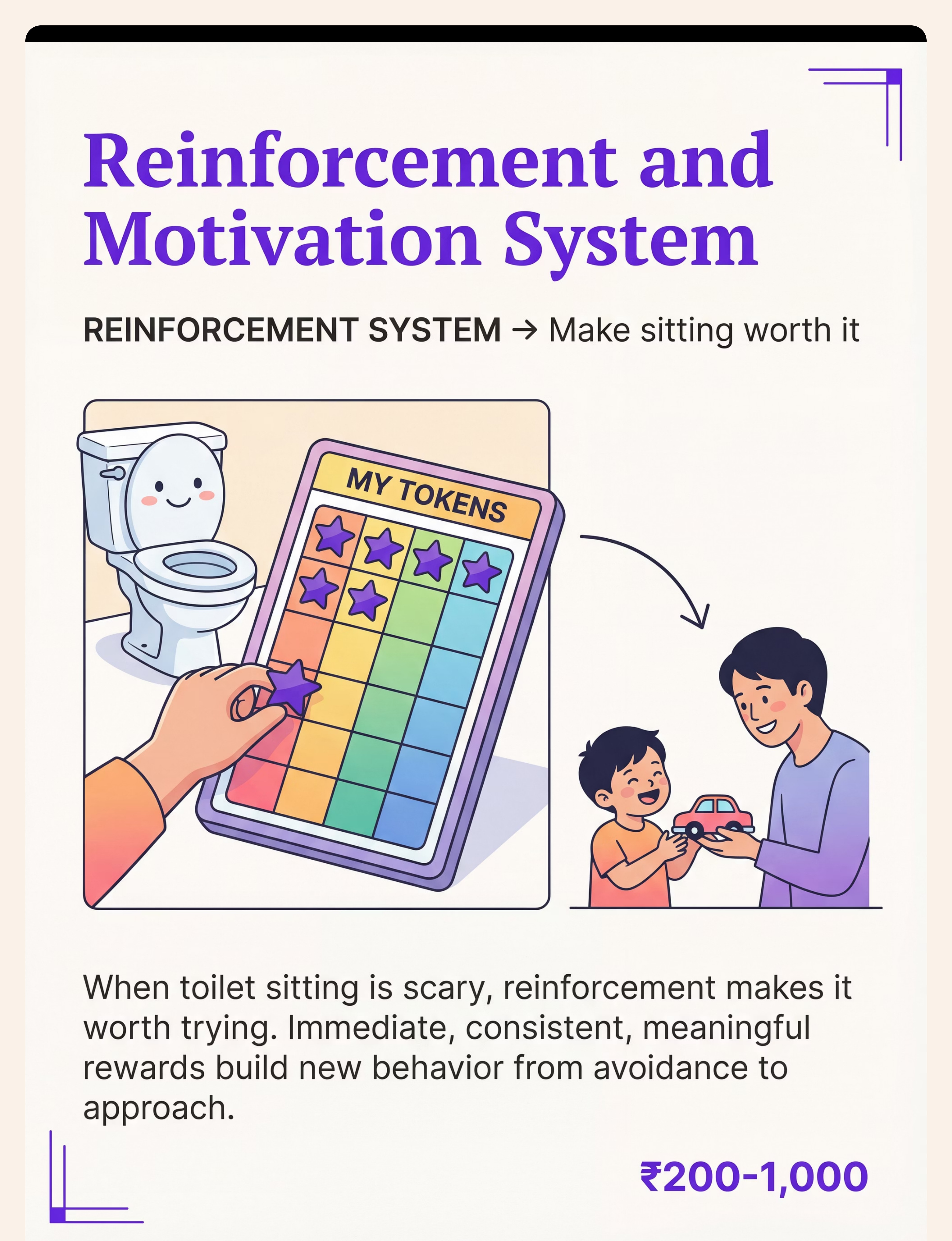
9. Reinforcement and Motivation System
Category: Reinforcement Menus | Mechanism: This is not bribery — it is systematic motivation science. Start reinforcing ANY approach to the bathroom. The system must be immediate (within 3 seconds), consistent (every time initially), and meaningful (what YOUR child actually wants). Options: Token board · Star chart · Immediate small treats · Special activity time · Stickers. Pinnacle Canon Products: Rosette Reward Jar (₹200–500) · 1800+ Reward Stickers Pack (₹150–400) · Animal Soft Toy (₹300–800)
🚀 Starter Kit for Most Families: Padded seat (₹800) + Step stool (₹600) + Seat reducer with handles (₹900) + Visual timer (₹500) = ~₹2,800 total. Addresses tactile, vestibular, postural, and predictability — the 4 most common trigger categories.

Every Material Has a Zero-Cost Version. Every Family Can Begin Today.
WHO/UNICEF equity principle: No child's progress should depend on purchasing power. These household alternatives carry the same clinical mechanism as their commercial counterparts.
Commercial Material | Household DIY Alternative | Same Mechanism | |
Padded toilet seat (₹800) | Thick folded towel secured with rubber bands over seat | Tactile input: soft, warm contact | |
Seat reducer with handles | Plastic bucket/stool beside toilet first; wall grab bar screwed into stud | Containment + grip security | |
Step stool (₹600) | Sturdy wooden box / milk crate / encyclopaedias taped together | Vestibular grounding | |
Visual social story (₹400) | 8 photos printed + laminated with cello tape + stapled booklet | Anxiety preview + familiarisation | |
Bathroom sensory kit | Phone white noise app (₹0) + dim lights + warm floor towel | Sensory load reduction | |
Gradual exposure ladder | Poster board + hand-drawn ladder + child's photo as the "climber" | Systematic desensitisation | |
Visual timer | Phone countdown timer with large display facing child | Finite duration visibility | |
Reinforcement system | Paper star chart + stickers from existing supply | Operant conditioning |
⚠️ Non-Negotiable Upgrade: The step stool is the one item where DIY has real limits. Unstable makeshift stools can slide or tip in a wet bathroom. Invest in a proper non-slip step stool (₹300–600) — it is the highest-impact, lowest-cost permanent solution.

Read This Before Your First Session. Non-Negotiable.
🔴 DO NOT PROCEED IF:
- Child has active constipation or pain during bowel movements — rule out medical cause FIRST
- Child has an active UTI or urinary tract pain
- Child is acutely ill, feverish, or significantly unwell
- Child has experienced a recent traumatic event
- Parent/caregiver is in high frustration or anger — emotional state transfers
- Child shows signs of severe anxiety disorder requiring professional management first
🟡 MODIFY IF:
- Child slept poorly — shorten session, reduce demands
- Child had a meltdown in the previous hour — use only the easiest ladder steps
- Caregiver is new to child — established rapport required first
- Multiple environmental changes happening simultaneously
🟢 PROCEED WHEN:
- Child is calm, fed, rested
- Bathroom environment modifications are in place
- Materials are ready before bringing child to bathroom
- Parent has reviewed today's ladder step and knows the script
- At least 30 minutes have passed since last meltdown
STOP IMMEDIATELY IF: Child shows severe distress escalation beyond initial protest · breath-holding · vomiting · injury-risk behavior · sudden pallor or loss of consciousness. Medical rule-outs to discuss with your pediatrician: Constipation (most common) · UTI · Sensory Processing Disorder (formal evaluation) · Anxiety Disorder.

The Right Environment Is 60% of the Intervention
Spatial precision prevents 80% of session failures before the session begins.
Bathroom Setup: 5 Positions
Toilet
Padded seat and reducer installed before child enters bathroom
Step Stool
In position — child's feet should land on it naturally when seated
Parent Position
Beside and slightly behind child — NOT blocking the door. Child must feel able to leave — this reduces panic.
Timer
At child's eye level, visible from toilet seat without turning
Engagement Item
In your hand, ready to present once child is seated
Sensory Environment Checklist
💡 Lighting
Dim to ~50% if possible. Overhead bathroom lights add to sensory load.
🔊 Sound
White noise running softly OR preferred music playing quietly before child enters.
🌡️ Temperature
Run warm water briefly to raise temperature. Warm bath mat on floor.
👁️ Remove
Harsh cleaning product smells · Loud fans · Visually cluttering items at child's eye level
Parent Body Language: Calm, unhurried posture. No tension in jaw or shoulders — children read this. Make eye contact at child's level. Script for today ready in your mind — no improvising under pressure.
60-Second Readiness Assessment. The Best Session Starts Right.
Before every session, run this 5-point check. It takes less than a minute and prevents wasted sessions — protecting both your child's trust and your energy.
# | Check | ✅ GO | 🟡 MODIFY | 🔴 POSTPONE | |
1 | Sleep | Rested, normal night | Short night, a bit tired | Very poor sleep, overtired | |
2 | Food | Recently fed (30–60 min ago) | Slightly hungry | Very hungry or just ate | |
3 | Emotional State | Calm, regulated, engaged | Mildly elevated, distractible | Actively dysregulated, mid-meltdown | |
4 | Physical Comfort | No signs of discomfort | Mild signs, monitor | Active signs of pain or illness | |
5 | Natural Urge | Signs of needing to go (fidgeting, holding) | Not obvious | Just went (no natural motivation) |
5 Green
Full session — advance one rung on ladder
3–4 Green
Modified session — stay on current ladder rung
1–2 Green
Abbreviated — easiest step only
0 Green
Postpone — walk past toilet, give sticker, leave

Step 1 of 6
The Invitation — Not a Command
The Principle
Every session begins with an invitation, never a command. The child must feel they are going with you, not being taken. This distinction rewires the emotional context of the bathroom approach.
Parent Script: "[Name], it's special bathroom time! I've got your [favourite item] waiting. Come with me?"
Body Language
- Crouch to child's eye level
- Open, relaxed expression — no tensed jaw
- Extend a hand — do not grab
- Slow movement toward bathroom — let child set the pace
What to Do When They Resist
Child backs away
Do not pursue. Neutral response. Try again in 15–20 minutes.
Early distress signs
Reduce demand: "Just come look at the step stool with me?"
Child is clingy
Invite them onto your lap first, walk to bathroom together.
Child says "no" verbally
Honour it. Record in data. Note time of day when refusal was least.
Timing: 30–60 seconds. Outcome: Child is moving toward bathroom, emotional state calm or slightly elevated.

Step 2 of 6
The Engagement — From Door to Toilet
Child enters the bathroom. The door remains visibly accessible — child must be able to see the exit. State today's goal clearly and simply: "Today we're going to [stand next to / touch the seat / sit on the lid — whatever today's ladder rung is]. Then we get your sticker."
🛋️ Padded Seat → Child Touches First
"Feel how soft it is! Touch it." Child touches seat. Praise immediately.
🪵 Step Stool → Demonstrate
"Watch, I put my feet here — they're flat! Your turn." Model foot placement, invite child to copy.
🪑 Seat Reducer → Child Grips Handles
"Hold the handles — see? You're in charge." Child grips handles. Pause. Allow child to feel control.
🟢 Engagement
Child touches, explores, tries materials willingly — continue warmly
🟡 Tolerance
Child complies but shows mild tension — continue with warmth and encouragement
🔴 Avoidance
Child pulls back — pause, praise what they DID do, don't push further today
Timing: 1–3 minutes total for material introduction. Praise every exploratory touch, every step of approach.
Step 3 of 6
The Therapeutic Action — The Core Event
Early Ladder Stages
Child approaches toilet. Touches seat. Holds for 3–5 seconds. This IS the therapeutic event. Praise.
Mid Ladder Stages
Child sits on closed lid with clothing on. Timer set to 15–30 seconds. Holds handles. Feet on step stool. Engagement item in hand. Timer ends. Child gets up.
Advanced Stages
Child sits on open toilet. Timer: 1–3 minutes initially. Increase by 30 seconds per successful week.
❌ Common Execution Errors to Avoid:
- Holding child on toilet if they try to get up — destroys trust
- Saying "just a little longer" after timer ends
- Showing visible frustration if session is brief
- Checking whether child has toileted during sitting — adds performance pressure
Parent Positioning: Beside child, not hovering. Make light conversation — not about toileting — or read the engagement item together. Do NOT watch the child intently — peripheral presence, not surveillance.
Step 4 of 6
Therapeutic Dosage — 3 Good Attempts > 10 Forced Ones
Dosage Guidance
Per Session
1–2 attempts (early stages) · 2–3 maximum (consolidation). Each attempt: timer-controlled, consistent length.
Per Day
2–4 toilet opportunities built into daily routine. After meals (natural gastrocolic reflex = highest biological readiness).
Per Week
3–5 days active protocol + 2 days lighter approach. Never 7 days of pressure — rest days prevent burnout.
Variation Options — Maintain Engagement Across Days
Change one element while keeping core constant:
- Change the engagement item (rotate weekly)
- Change the timer format (hourglass vs. digital vs. app)
- Change the social story page you read together
- Change who accompanies (alternating parent, if appropriate)
- Change time of day (find child's peak regulation window)
Satiation Indicators — STOP when you see:
- Child's engagement item interest drops to zero
- Fidgeting increases without functional direction
- Eye contact decreases markedly
- Vocalizations increase in distress quality
"3 successful seconds are worth more than 30 forced seconds. Success leaves a positive trace in the nervous system. Force leaves a negative one." — Pinnacle OT Consortium

Step 5 of 6
The ABA Reinforcement Event — Timing Is Everything
Reinforcement delivered more than 3 seconds after behavior loses most of its power. This is not negotiable — it is biology. The brain associates reward with the behavior that immediately preceded it. Be ready.
Immediate
Within 3 seconds of the behavior. Not "in a minute." Not after you finish what you're doing. Now.
Specific
Not: "Good job!" But: "You sat on the toilet for 15 seconds AND held the handles. That's exactly what brave looks like."
Enthusiastic
High-affect, genuine celebration. Children read your emotional state — let them feel your pride.
Every Time
During the building phase, reinforce every single qualifying attempt — 100% schedule initially.
Reinforce the Attempt, Not Just Success:
Child walked to bathroom → token
Child touched the seat → token
Child sat for 5 seconds (goal was 15) → token
Child tried but cried → verbal praise + hug → no punishment
Pinnacle Canon Products: Reward Stickers Pack · Rosette Reward Jar · Animal Soft Toy Transition Comfort — all available on Amazon.in

Step 6 of 6
The Cool-Down — No Session Ends Abruptly. The Brain Needs to Land.
Abrupt session endings create dysregulation that transfers to the next attempt. The child's nervous system remembers not just the toilet sitting — but the emotional state they were in when they left the bathroom. Leave on a positive note. Always.
2-Minute Warning
"Two more seconds on the timer, then we're all done!" — Say this before the timer ends, giving the nervous system preparation time.
Immediate Release
"Timer done! All done! You can get up!" — Child gets up immediately. No "just one more second." The system must be trustworthy.
Exit Ritual (30 sec)
"[Name], let's close the bathroom door together." — Child participates in closing. This gives them control of the transition.
Transition Activity (1–2 min)
Lead child to a preferred activity immediately — not straight into another demand. Bathroom time ends; preferred time begins. This builds the association: bathroom → positive things follow.
If child resists ending (a positive sign!): Don't extend — it breaks the system. Say: "We'll do more tomorrow! That means tomorrow comes faster." Redirect to preferred activity. Note in data: "Child showed motivation to continue — positive sign."

60 Seconds of Data Now = Hours of Progress Insight Later
Within 60 seconds of session end. Not tonight. Not "when I remember." Now.
3 Data Points to Capture
1. LADDER STEP ATTEMPTED: Circle: 1 → 2 → 3 → 4 → 5 → 6 → 7 → 8 → 9
2. CHILD RESPONSE: Circle: Refused → Partial → Completed → Exceeded
3. SITTING DURATION: _____ seconds / _____ minutes
NOTES (optional): _______________________
What This Data Does
Shows the pattern — some days, times, conditions better than others
Reveals when to advance the ladder (3 consecutive successes = advance)
Feeds GPT-OS® personalized recommendations
Provides clinical data for therapist review at next appointment
Pattern to look for: 3 consecutive sessions of calm completion at current ladder step → advance to next rung.

Session Abandonment Is Not Failure. It's Data.
Most sessions will not be perfect. This card covers the 7 most common failure modes and what to do next time. Every "failed" session tells you something important about your child's nervous system.
Problem 1: Child refused to enter the bathroom at all
Why: Anticipatory anxiety — the bathroom doorway is itself a trigger from previous forced experiences. Fix: Return to Ladder Rung 1. Today's session = standing in the doorway + immediate reward + leave. Spend 1–2 weeks here. Do not rush.
Problem 2: Child sat briefly then escalated to distress
Why: Timer target was set too high — sensory threshold was reached. Fix: Cut timer target in half. 15 seconds → 7 seconds. Build back up over 2 weeks.
Problem 3: Child had an accident immediately after leaving
Why: Bladder/bowel release happens in the habitual context (diaper/floor) — a functional pattern, not deliberate. This is actually a sign of readiness. Fix: Note accident times for 3 days to identify the pattern. Increase toilet opportunities to coincide with natural timing.
Problem 4: The padded seat made things worse
Why: The child's primary issue may be vestibular (not tactile). Fix: Remove padded seat. Try seat reducer with handles + step stool first. Address vestibular grounding before revisiting seat material.
Problem 5: Doing well at home but refuses at school
Why: Stimulus control — the child's "safe" toilet is the home toilet. Different environment = nervous system restart. Fix: Send portable kit to school: travel padded seat cover + mini step stool + familiar engagement item.
Problem 6: Progress reversed after illness/holiday/disruption
Why: Normal. Expected. Temporary. Fix: Return to 2–3 rungs earlier on the ladder. Progress returns faster than it was first gained — the neural pathways exist; they just need reactivation.
Problem 7: No progress after 6+ months of consistent protocol
Why: Materials don't match the child's specific cause, or clinical need exceeds parent-led intervention. Fix: Call 9100 181 181. Request OT + BCBA joint assessment. Do not continue alone.
No Two Children Are Identical. Your Version Is the Right Version.
The protocol adapts to your child — not the other way around. Use sensory profile and age-based modifications to find the right fit, then gradually shift toward greater challenge as confidence grows.
⬇️ EASIER Modifications
- Return to 2 rungs earlier on the exposure ladder
- Reduce timer to 5–10 seconds
- Use two preferred engagement items simultaneously
- Parent sits on closed toilet lid together with child first (modelling)
- Conduct bathroom desensitisation with toilet lid closed throughout
- Start session at child's calmest time of day
⬆️ HARDER Modifications
- Advance one rung on the exposure ladder
- Increase timer by 15–30 seconds
- Introduce mild distractions (shows real-world tolerance)
- Shift reinforcement from immediate to variable (every 2–3)
- Begin practicing at second toilet in the home (early generalization)
Sensory Profile Variations
🔵 Tactile-Sensitive
Priority: Padded seat → heated seat option → seat cover fabric
🟡 Vestibular-Sensitive
Priority: Step stool (first) → seat reducer with handles → back support
🟣 Anxiety-Dominated
Priority: Social story → gradual exposure ladder → visual timer → powerful reinforcement
🔴 Behavioral Entrenchment
Priority: Reinforcement system → visual timer → gradual exposure → consistency protocol
Age-Based Modifications
- 2–4 years: Very short sessions (30 sec max), maximum novelty, high-affect praise
- 5–7 years: Can understand the ladder concept, can help decide next step
- 8–10 years: Involve in goal-setting, discuss the science, build self-advocacy

Week 1–2: Laying the Foundation (Not Seeing Results Yet)
15%
Foundation Phase
Where you are in the journey — internal nervous system change is happening even when external behavior appears unchanged
✓ What You Will Likely See
- Child's distress when approaching bathroom decreases slightly
- Child tolerates brief bathroom exposure without immediate escape
- Child begins to recognize the routine (predictability emerging)
- One or two sessions go better than expected
✗ What You Will NOT Yet See
- Voluntary willingness to sit
- Consistent calm across all attempts
- Elimination on the toilet
- Generalization to other toilets
"If your child's distress during bathroom approach decreases from a 9/10 to a 7/10 — that is genuine, measurable progress. You may not be able to see it yet. Your data can."
Parent Emotional Preparation: This phase is the hardest. The external behavior change is minimal. The internal nervous system change is significant. Trust your protocol. Track your data. Do not increase pressure when progress feels slow — this is when pressure does the most damage.
Week 3–4: The Neural Pathways Are Forming
40%
Consolidation Phase
Behavioral patterns are consolidating — look for these specific indicators this week
✓ Consolidation Indicators
- Child approaches bathroom with noticeably less resistance — 3+ sessions this week
- Child asks where the special toilet item is
- Child sits for 30+ seconds without escalating distress
- Child mentions toilet or bathroom voluntarily in conversation
- Occasional spontaneous approach to bathroom
When to Increase Intensity
- 3 consecutive sessions completed calmly at current rung → advance one rung
- Timer tolerance stable at 30 seconds → increase to 45 seconds
- Do NOT advance more than one element per week
Neural Pathway Formation Signs
- Child begins walking toward bathroom without being fully guided
- Self-stimulatory behavior (if present) decreases during bathroom time
- Child's body is less rigid during bathroom approach
The Parent Milestone: By Week 3–4, most parents report: "I'm more confident in the protocol now." This matters. Your calm confidence transmits directly to your child's nervous system. You are part of the sensory environment.

Week 5–8: The Evidence of Real Change
75%
Mastery Phase
Observable, specific, measurable change — the nervous system has genuinely reorganized its assessment of safety
🏅 Mastery Criteria — What Mastery Looks Like:
✅ Approach
Child approaches bathroom without physical resistance on 8/10 occasions
✅ Sitting
Child sits on toilet for 2–5 minutes calmly (ladder top rungs)
✅ Independence
Uses handles and step stool appropriately without prompting
✅ Generalization
Tolerates sitting at a second toilet in the home
✅ Function
Child begins to eliminate on toilet at least occasionally
✅ Regulation
Distress behavior ratings consistently below 3/10 during bathroom approach
🏅 Mastery Badge Unlocked: "Toilet Approach & Sitting: Achieving" — GPT-OS® Self-Care Readiness Index. When child sits independently for functional durations consistently → move to E-496 (Fear of Flushing). Do NOT rush past mastery to next technique. Consolidation matters.
You Did This. And Your Child Grew Because of Your Commitment.
"[Child's name] went from complete toilet refusal — from screaming and arching and fighting — to sitting willingly. You made that possible. Every early morning attempt when it didn't work, every session you tried again when you were exhausted — it added up to this."
What This Achievement Means
This is not just about the toilet. Toilet independence is the gateway to so much more:
School Inclusion
Most schools require independent toileting. This achievement opens the door.
Community Participation
Trips, events, camps — the world opens up when toileting is no longer a barrier.
Dignity & Self-Esteem
Peer normalization, reduced diaper dependency — your child's own sense of capability grows.
Family Freedom
Reduced caregiver burden. A family that can go places, do things, live fully.
📓 Journal Prompt: "Today, [date], [child's name] sat on the toilet calmly for [duration]. They used [materials]. They were brave. We are proud."
Trust Your Instincts. If Something Feels Wrong, Pause and Ask.
🔴 Zero progress after 6+ weeks of consistent protocol
Possible signal: Misidentified cause (treating sensory when behavioral, or treating behavioral when medical). Needs professional reassessment.
🔴 Constipation developing or worsening
Possible signal: Withholding behavior evolving. Stool withholding creates pain → deeper refusal → medical complication spiral. Medical intervention needed.
🔴 Anxiety generalizing beyond bathroom
Possible signal: Anxiety disorder (not just toileting anxiety) requires psychological evaluation.
🔴 Child shows regression in other areas during protocol
Possible signal: Protocol is creating generalized stress. Reduce intensity. Seek guidance on pacing.
🔴 Physical pain signs during toilet approach
Possible signal: Medical cause not yet identified. Pediatric evaluation required.
🔴 Parent-child relationship deteriorating over toilet battles
Possible signal: Intervention approach needs professional restructuring. Relationship preservation is more important than toilet training speed.
Level 1: Self-Resolve
Consult Cards 21–22 on this page. Adjust protocol, try 2 more weeks.
Level 2: Teleconsultation
Call 9100 181 181. Request OT teleconsultation (30 min, FREE initial assessment). Available 24×7, 16 languages.
Level 3: Clinic Assessment
Pinnacle center near you. OT + BCBA + Developmental Pediatrician joint assessment. AbilityScore® evaluation.
You Are Not Done. You Are On a Journey.
E-495 is one technique within a complete Self-Care & Daily Living progression. Where you go next depends on what your child shows you — mastery here opens multiple pathways forward.
E-493
Nonverbal Toilet Training
E-494
Hygiene Routines (prerequisite domain)
► E-495
YOU ARE HERE — Toilet Sitting Refusal
E-496
Fear of Flushing — Next Logical Step
Next-Level Options
Child sits well but fears flushing
→ E-496: Fear of Flushing — next logical step
Sensory issues extend beyond toilet
→ E-510: Sensory Processing & Self-Care
Bowel withholding has developed
→ E-497: Bowel Withholding — medical + behavioral combined (consult pediatrician)
Lateral Alternatives
ABA-Led Discrete Trial
BCBA-guided approach — if E-495 approach didn't fully resonate
Reward-Only Protocol
Reinforcement-heavy, minimal sensory focus — for primarily behaviorally motivated children
E-498 Regression Support
If child regresses after initial mastery
Other Techniques in Self-Care & Daily Living
Materials you already own from E-495 are reused across multiple techniques. The step stool, visual timer, and reward system appear in 40+ techniques across Domain E — your investment compounds.
E-493 · Intro
Nonverbal Toilet Training
Visual Supports, Communication-Based Approach
E-494 · Core
Hygiene Routines for Sensory-Sensitive Children
Visual Schedules, Sensory Adaptations
E-496 · Core
Fear of Flushing
Gradual Exposure, Sound Desensitisation
E-497 · Advanced
Bowel Withholding
Medical + Behavioral Combined Approach
E-498 · Core
Toilet Training Regression
Behavior Support, Environmental Analysis
E-510 · Advanced
Sensory Processing & Self-Care
Sensory Integration, Broader Self-Care Skills
Toilet Sitting Is One Piece. Here Is Your Child's Complete Map.
Domain E — Self-Care & Daily Living — is one of 12 developmental domains tracked by GPT-OS®. Understanding how these domains connect helps you see the full picture of your child's growth.
Domain E — Active Domain
Toilet Sitting (E-495) is one technique within 500+ techniques in the Self-Care series. Connected domains commonly co-active:
- Domain A (Sensory): if sensory processing is underlying cause
- Domain C (Emotional Regulation): if anxiety is primary driver
- Domain D (Behavior): if learned avoidance is primary driver
GPT-OS® Full Profile
With GPT-OS®, your child's developmental profile across all 12 domains is tracked via AbilityScore® — showing not just what they're working on today, but where they're heading across their entire developmental journey.

From Complete Refusal to Willing Sitting — Real Families, Real Journeys
Anonymised. Behaviorally specific. From the Pinnacle Network.
Family Story 1
Rahul, Age 4 — Hyderabad
Before: Two years of toilet training attempts, all ending in screaming, arching back, kicking the toilet seat away. Diaper-dependent. Preschool entry uncertain.
Identified: Vestibular hypersensitivity (dangling feet were the primary trigger) + cold seat tactile aversion. Inconsistent reinforcement across parents and grandparents.
Materials Used: Step stool + padded seat + token board with immediate small reward.
"Once we got the step stool and the padded seat, the first calm sitting happened within 3 days. We cried. Nobody had told us about the dangling feet."
Therapist Note: "The step stool is a ₹400 item with a ₹40,000 outcome."
After (10 weeks): Sits willingly for 3–4 minutes. Asks to use bathroom proactively. Started preschool on schedule.
Family Story 2
Priya, Age 7 — Chennai
Before: Anxiety-dominated refusal beginning around age 4 following a traumatic flushing experience. Generalised to ALL toilets in all settings. Could not attend school camps or relatives' homes.
Identified: Anxiety-based refusal with entrenched avoidance. Visual social story and gradual exposure ladder selected as primary approach. Reinforcement built around screen time (highly preferred).
"The social story was the breakthrough. She had built up this enormous fear in her imagination. Once she could read about it and understand she was in control — the fear started to dissolve."
Therapist Note: "For anxiety-led refusal, predictability interventions matter more than physical adaptations."
After (14 weeks): Using home toilet independently. Tolerating school toilet with familiar adaptations. Attended first family vacation.
Illustrative cases. Outcomes vary by child profile, underlying condition, and intervention consistency.

Isolation Is the Enemy of Progress. Join the Community.
You are not the only parent lying awake wondering if your child will ever be toilet independent. There are millions of you. Many have already crossed this bridge. They want to help.
📱 WhatsApp Parent Group
India's largest parent community for toileting support. 16,000+ parents · Expert moderated · Regional language sub-groups available.
💻 Online Community
pinnacleblooms.org/community → Toilet Training Discussion Forum. Search "E-495" to find posts about toilet sitting refusal specifically.
👥 Local Parent Meetups
Organised by Pinnacle centers — monthly in 70+ cities across India. Find a meetup near you → pinnacleblooms.org/meetups
🤝 Peer Mentoring
Connect with an experienced parent who has navigated toilet sitting refusal with their own child. Monthly matching available through Pinnacle centers.
Your experience helps others. If you are reading this after your child has achieved sitting — please share your journey. The parent currently on Card 01 of this page needs your story.
Home Intervention + Clinical Backing = Maximum Impact
This page gives you tools to begin. A Pinnacle therapist gives you tools that are personalised to YOUR child's specific nervous system.
Therapist Matching for E-495
For toilet sitting refusal, request:
Pediatric OT
Sensory + environmental assessment. The lead discipline for material selection.
BCBA / ABA Therapist
Functional behavior analysis + reinforcement system design.
FusionModule™ Joint Session
OT + BCBA together — most efficient approach for complex, entrenched refusal.
Insurance/Funding: Ask about CGHS coverage, state disability welfare support, and Pinnacle's sliding-scale fee structure for qualifying families.
Get Started Now
Teleconsultation (remote families): Available in 16+ languages. Book a 30-minute OT teleconsultation from anywhere.
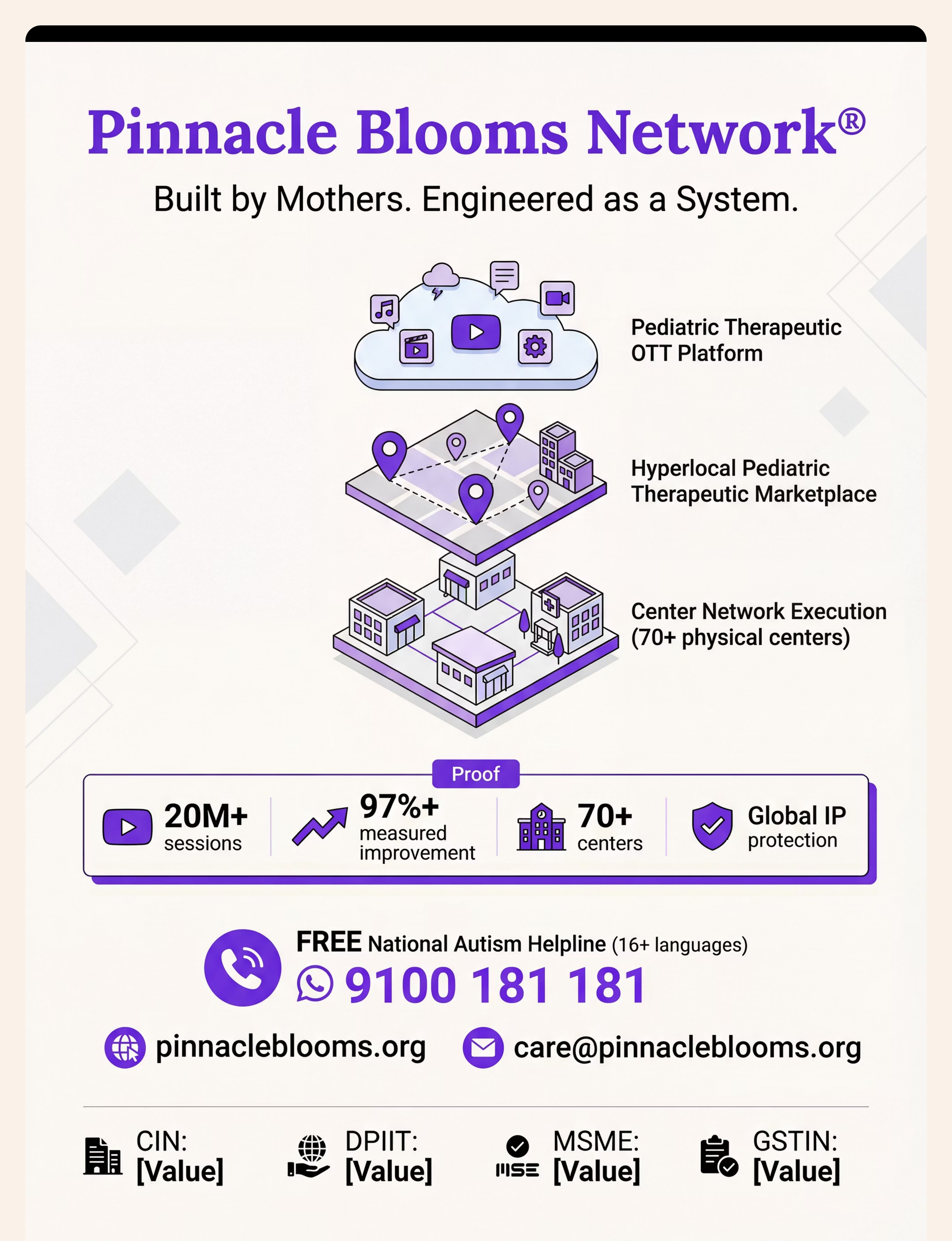
FREE First Call:📞 9100 181 181 — Call, describe your child's toilet refusal. Our triage team connects you to the right professional within 24 hours. No cost. No obligation.
"Home + Clinic = Maximum Impact" — The families achieving fastest progress combine home protocol (this page) with 2× monthly clinical review. The therapist adjusts. The parent executes daily. The child benefits from both.
Deeper Reading for the Curious Parent and Clinician
Every recommendation in E-495 is anchored in peer-reviewed research. Here are the five foundational studies behind this technique.
📄 PRISMA Systematic Review (2024) — PMC11506176
16 peer-reviewed articles (2013–2023) confirm sensory integration intervention is evidence-based practice for ASD. Effect sizes: Social skills (d=0.61), Adaptive behavior (d=0.58), Sensory processing (d=0.71).
📄 Meta-Analysis, World J Clin Cases (2024) — PMC10955541
24 studies: Sensory integration therapy effectively promoted adaptive behavior, sensory processing, motor skills, and social functioning. DOI: 10.12998/wjcc.v12.i7.1260
📄 Indian RCT, Indian J Pediatr (2019)
Home-based sensory interventions showed significant outcomes in Indian pediatric populations — validating parent-administered approaches for Pinnacle families. Padmanabha et al. DOI: 10.1007/s12098-018-2747-4
📄 NCAEP Evidence-Based Practices Report (2020)
Visual supports, reinforcement systems, video modeling, and gradual exposure all classified as EBP for autism. Every material category in E-495 is covered. ncaep.fpg.unc.edu
📄 WHO Nurturing Care Framework (2018)
Comprehensive global framework for ECD across 197 countries. All techniques must align with this framework for global applicability. nurturing-care.org
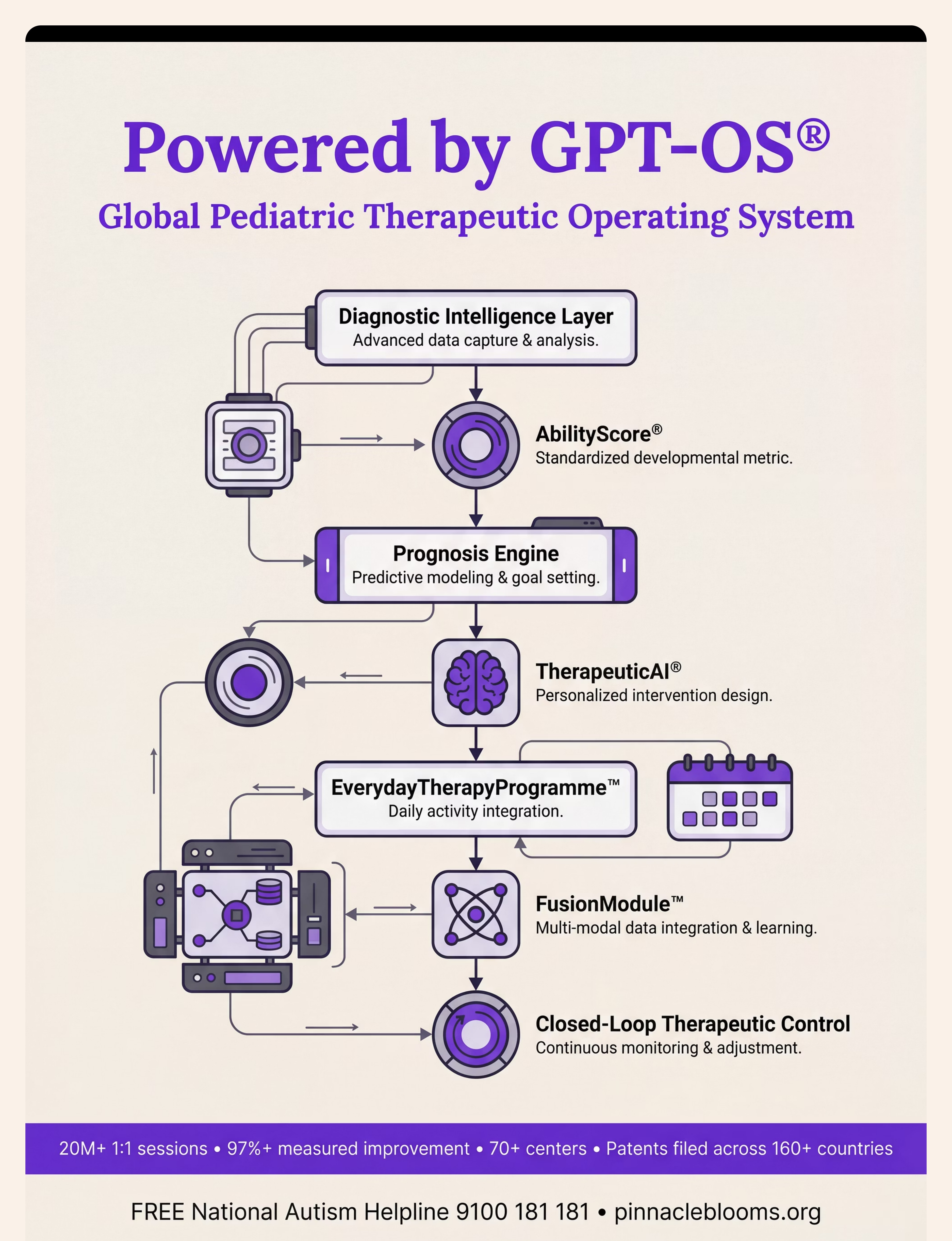
Pinnacle Clinical Data: 20M+ exclusive 1:1 therapy sessions · 97%+ measured improvement · 70+ centers · Population data across every center informs every protocol on this page.
Your Data Helps Your Child. And Every Child Like Them.
When you record session data, it flows through the GPT-OS® intelligence layer — updating your child's profile, recalculating their trajectory, and improving recommendations for every family in the network.
What GPT-OS® Learns from E-495 Data
- Which materials created breakthrough moments (population-level pattern)
- What ladder rung most children stall at (protocol improvement)
- Which caregiver profiles achieve fastest progress (parent guidance optimization)
- Which child sensory profiles respond to which material combinations (personalisation)
🔒 Privacy Assurance
- Data encrypted at rest and in transit
- No identifying information shared with third parties
- DPIIT-registered, MSME-certified, GSTIN-compliant entity
- CIN: U74999TG2016PTC113063 — fully regulated Indian entity
"The families before you who tracked their data are the reason this protocol works as well as it does today."

E-495 | Watch the Reel — 9 Materials in 90 Seconds
A Pinnacle OT therapist walks through all 9 materials in under 90 seconds — demonstrating exactly how each one works and why it helps your child's nervous system.
Reel ID: E-495 | Series: Self-Care & Daily Living Skills | Episode: 495 of 999 | Duration: ~75–85 seconds
Padded seat — soft contact, not cold shock
Seat reducer with handles — security they can hold
Step stool — feet grounded, fear reduced
Visual social story — preview safety before experience
Bathroom sensory modification kit — make the whole bathroom tolerable
Gradual exposure ladder — small steps, real progress
Distraction items — positive focus, not scary focus
Visual timer — see when sitting ends
Reinforcement system — make sitting worth it
"Toilet sitting refusal is one of the most misunderstood challenges in toilet training. What looks like defiance is almost always distress. These materials change what the toilet represents to your child's nervous system — safely, gradually, and permanently." — Pinnacle OT Therapist
Consistency Across All Caregivers Multiplies Impact by 3×
If only one parent executes the protocol, progress happens. If ALL caregivers — both parents, grandparents, school teachers — execute consistently, progress is 3× faster and 5× more likely to generalise.
Explain to Grandparents (Simplified)
"[Child's name] is working on sitting on the toilet."
✅DO: Say "[name], timer is ready. Come sit." Put on the padded seat. Start the timer. Give the sticker when done.
❌DON'T: Force them onto the toilet. Say "just a little longer." Show frustration.
"The toilet has a soft cover now and a step for their feet. Please use them every time. Questions: Call 9100 181 181."
Teacher / School Communication Template
"[Child's name] is following an OT-designed toilet sitting protocol at home. To generalise this to school, we are requesting:
- A portable padded seat cover on the school toilet
- A step stool if available
- 3–5 scheduled bathroom opportunities per day (not demand-based)
- Consistent reinforcement using [child's preferred reward]
Please contact us to coordinate."

The Questions Pinnacle Parents Ask Most
Q1: How long will this take? My child has been refusing for 2 years.
For long-standing refusal (1–2 years), expect 8–16 weeks of consistent protocol before mastery. Initial responses often appear within 2–4 weeks. The first 2 years built deeply entrenched associations — they won't disappear in 2 weeks, but they will disappear. 97%+ of children in our network achieved willing, independent sitting.
Q2: My child sits on the potty chair but refuses the big toilet. Which materials?
Physical size + postural insecurity issue. Priority: Seat reducer (makes opening proportional to potty chair size) + step stool (replicates foot grounding) + padded seat (if texture harder/colder). Most children transition well with these three changes.
Q3: We tried a padded seat and it made no difference. What next?
Tactile aversion may not be the primary driver. Add a step stool — if child suddenly sits more calmly, vestibular insecurity was the primary issue. Also check: is the bathroom itself overwhelming? Environmental modification may need to come before any seat modification.
Q4: My child sits but never produces on the toilet. Is E-495 still relevant?
Yes. Toilet sitting and toilet using are two different skills. E-495 addresses sitting. Once sitting is mastered, the next challenge is learning to release — see E-497 (Bowel Withholding). E-495 is the essential first foundation.
Q5: Is it okay to use a tablet/screen during toilet sitting?
Yes — as a toilet-time-only distraction item — with conditions. Screen must be exclusively available at toilet time (removed immediately after) and not used to trick/force a terrified child. Use for children with some tolerance who need positive association building.
Q6: How do I handle this at school when teachers don't know the protocol?
Use the teacher communication template from Card 37. Request: portable padded cover from home, scheduled bathroom times (not demand-based), visual timer, consistent reinforcer. Most teachers are willing with a clear, simple protocol. Involve the special educator if available.
Q7: My child is 9 years old. Is it too late for these techniques?
No. The sensory and vestibular mechanisms don't have an age cutoff. The materials are identical — adapt by involving the older child in selecting reinforcers, choosing engagement items, and tracking their own progress. Self-determination increases motivation significantly.
Q8: Should I consult a professional or try this myself first?
Both simultaneously is ideal. This page gives you enough to begin tomorrow. A professional assessment (OT + BCBA) identifies which of the 9 materials are most relevant to YOUR child's specific profile — preventing months of trial and error. Call 9100 181 181 while implementing the starter kit from Card 09.
Preview of 9 materials that help when child refuses toilet sitting Therapy Material
Below is a visual preview of 9 materials that help when child refuses toilet sitting therapy material. The pages shown help educators, therapists, and caregivers understand the structure and content of the resource before use. Materials should be used under appropriate professional guidance.













Link copied!
You Have Everything You Need. Begin Today.
Three actions. One priority. Choose yours.
🚀 Start This Technique Today
Access the GPT-OS® Session Launcher for E-495. Personalized session protocol generated in 3 minutes.
📞 Book a Professional Assessment
9100 181 181 · FREE Initial Consultation · 24×7 · OT + BCBA joint assessment available in 70+ centers + teleconsultation
➡️ Explore the Next Technique
E-496: Fear of Flushing — the next logical step once toilet sitting is mastered.
✦ VALIDATED BY THE PINNACLE BLOOMS CONSORTIUM ✦🔵 OT · 🟡 ABA · 🟢 SpEd · 🟣 NeuroDev · 🔴 SLP · CRO WHO-Aligned · UNICEF-Aligned · NCAEP 2020 · 20M+ Sessions · 97%+ Improved · 70+ Centers From Fear to Mastery. One Technique at a Time."We exist to transform every home into a proven, scientific, 24×7, personalised, multi-sensory, multi-disciplinary pediatric therapy ecosystem — for every child, regardless of geography or economic status."📞9100 181 181 · FREE · 24×7 · 16 Languages · WhatsApp same number pinnacleblooms.org · care@pinnacleblooms.org © 2025–2026 Pinnacle Blooms Network®, unit of Bharath Healthcare Laboratories Pvt. Ltd. · CIN: U74999TG2016PTC113063 · DPIIT: DIPP8651 · MSME: TS20F0009606 · GSTIN: 36AAGCB9722P1Z2 This content is educational. It does not replace individualised assessment and intervention from licensed occupational therapists, behavioral therapists, or developmental specialists. Always consult your child's healthcare team before beginning or modifying toileting approaches. Individual results may vary. ← E-494: Hygiene Routines · E-496: Fear of Flushing →