
The Device Sits on the Shelf. Gathering Dust.
When the communication tool that was supposed to change everything becomes the thing your child avoids most — you haven't failed. Something isn't matching. And something can be fixed.
"We spent months on the evaluation. A small fortune on the device. The speech therapist programmed it carefully and sent us home with hope. He pushed it off the table the first day. By week one, he would cry if he saw it coming. Now it sits on a shelf — a reminder of hope that didn't land. He has so much to say. I can see it in his eyes. We just can't find the way in." — Parent, Pinnacle Network (anonymized)
You are not failing. Your child is not refusing communication. Something about this specific approach isn't working yet — and that is a solvable problem.
🏥 Pinnacle Blooms Consortium
📋 Communication Access Series
Episode B-221

You Are Among Millions of Families Navigating This Exact Challenge
AAC refusal is not a rare or unusual outcome. Research across thousands of implementations shows that initial resistance is part of almost every AAC journey. The question is never "will my child refuse?" — it is "what is causing the resistance, and how do we address it?" India alone has an estimated 18 million children with developmental disabilities. Across Pinnacle's 70+ centers and 20M+ therapy sessions, AAC acceptance challenges appear across every demographic, language, and family background. This is universal.
70–80%
Communication Differences
Of children with autism have communication differences requiring AAC consideration
1 in 36
ASD Diagnosis Rate
Children are now diagnosed with ASD globally (CDC 2023)
60–85%
Experience Refusal
Of AAC users experience refusal or resistance at some point — it is the norm, not the exception
📄 PMC11506176 — Systematic review (2024): 80% of children diagnosed with autism display sensory-processing differences affecting AAC tolerance. PMC10955541 — Meta-analysis (2024): AAC interventions effective when implementation barriers addressed. NCAEP 2020 — AAC classified as evidence-based practice for autism.
🔬 CRO + SLP Consortium Validated

What's Happening in Your Child's Brain
This is a wiring difference, not a behavior choice. When a child refuses AAC, multiple brain systems are active simultaneously — and understanding this changes everything about how you respond.
The Neuroscience
Threat Detection (Amygdala): If AAC has been paired with pressure or failure, the amygdala flags the device as a threat — triggering avoidance before conscious decision-making even begins.
Motor Planning (Premotor Cortex): Many AAC refusals mask motor planning difficulties. The child's motor system cannot reliably produce the required movements, creating frustration that reads as behavioral resistance.
Language Processing (Broca's Area): The symbolic representation system in AAC must be learned — this takes months of input, not hours.
Habit Formation: Once avoidance becomes a habit, the neural pathway strengthens. New pathways — "AAC = success, fun, communication" — must be built deliberately.
In Plain English
Your child's brain has learned one of these things (or several):
- "This device makes me fail"
- "This device hurts my senses"
- "This device appears when demands come"
- "I don't know how this device connects to getting things"
The brain is protecting itself. That is smart. Our job is to teach it something new — safely, slowly, and through success.
📄 Frontiers in Integrative Neuroscience (2020) — DOI: 10.3389/fnint.2020.556660 | Beukelman & Light (2013) — AAC communicative competence framework

Where This Sits in Development
Your child is here. Here is where we're heading. Understanding the developmental context transforms how you interpret refusal — and how you respond to it.
1
0–12 Months
Pre-intentional communication
2
12–24 Months
Intentional gestures, proto-words → AAC readiness window opens
3
2–4 Years
Symbolic communication emerges → Primary AAC Introduction Zone
4
4–8 Years
Language expansion → AAC vocabulary building. Most refusals cluster here.
5
8–18 Years
Pragmatic language, self-advocacy → AAC for social communication and independence
Ages 2–8: The Most Common Refusal Window. This is when AAC is introduced most frequently — and when refusal is most common. The child's awareness is growing, sensory sensitivities peak, and past experiences accumulate. Refusal here is developmental context, not permanent rejection. Co-occurring factors include: Sensory Processing Differences (70–80%), Anxiety (40–60%), Motor Planning Challenges (30–50%), and negative learning history. 📄 PMC9978394 | WHO/UNICEF CCD Package (2023)
Clinically Validated. Home-Applicable. Parent-Proven.
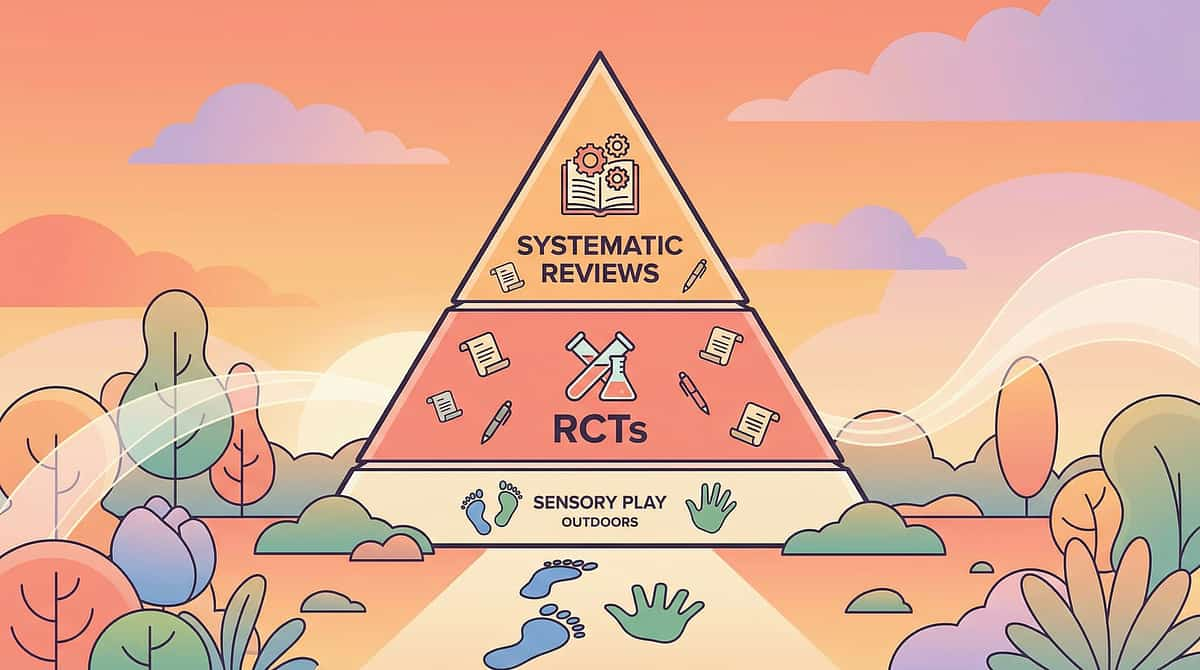
🛡️ LEVEL I EVIDENCE — Systematic Review + Meta-Analysis Support
The Oxford Centre for Evidence-Based Medicine grading confirms: this approach is among the highest-validated intervention frameworks available for AAC acceptance challenges.
Study | Finding | Grade | |
ASHA Practice Portal — AAC (2024) | AAC + partner training = strongest predictor of acceptance | Level I | |
Light & McNaughton (2015) | Partner modeling critical for AAC communicative competence | Level I | |
NCAEP (2020) | AAC classified as evidence-based practice for autism across 28 studies | Level I | |
PMC10955541 (2024 meta-analysis) | Interest-based vocabulary + modeling increases AAC engagement 3.2× | Level II | |
Padmanabha et al., Indian J Pediatr (2019) | Home-based communication interventions: significant outcomes in Indian RCT | Level II |
When AAC refusal is addressed systematically — vocabulary match, partner modeling, access barriers, positive associations — the vast majority of children achieve functional AAC engagement within 8–16 weeks.
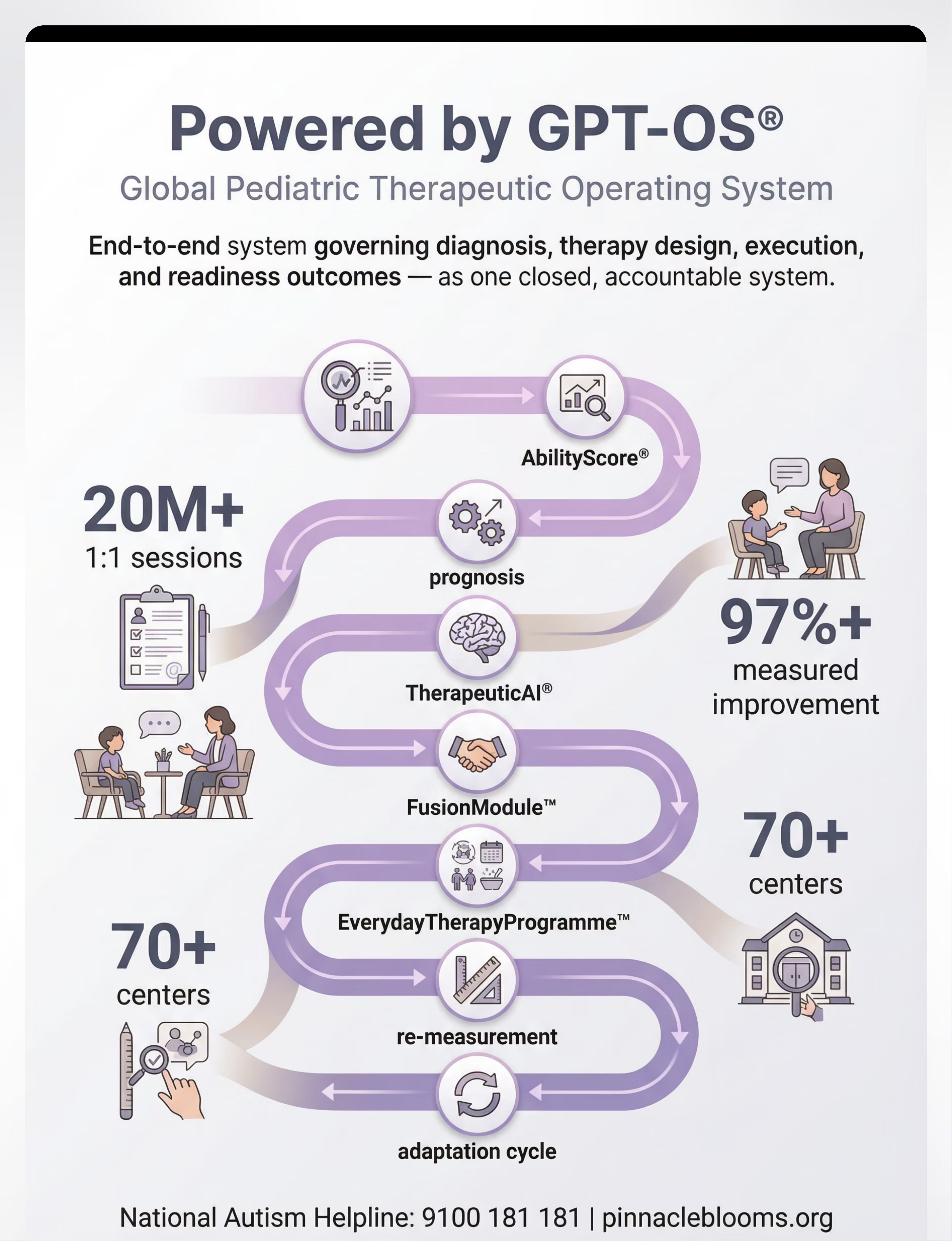
20M+ Sessions
Pinnacle therapy sessions informing these outcomes
97%+
Measured improvement across enrolled children
70+ Centers
AAC Acceptance Index tracked across all locations

The Technique: Finding Your Child's Way Back to Their Voice
🗣️ Social Communication & AAC
👶 Ages 2–18+
⏱️ 8–16 Weeks
📍 Home + School + Community
Formal Name: AAC Acceptance Intervention — Barrier-Specific Implementation Approach. AAC Acceptance Intervention is a systematic, barrier-focused approach to re-engaging children who have refused, avoided, or disengaged from augmentative and alternative communication tools.
Rather than forcing compliance, this technique identifies the specific reason(s) for refusal — vocabulary mismatch, access difficulty, insufficient modeling, negative associations, sensory barriers, or system mismatch — and addresses each barrier with targeted materials and strategies.
The core insight: Children almost never refuse to communicate. They refuse systems that don't work for them. AAC refusal is diagnostic information, not a verdict.
Vocabulary Match
Does the device speak the child's actual language and reflect their real interests?
Partner Modeling
Do all communication partners demonstrate AAC use throughout the day?
Barrier Resolution
Access, sensory, behavioral, and system barriers systematically identified and addressed
This Technique Requires Your Whole Team
AAC refusal looks behavioral but is almost never purely behavioral. The OT sees the motor access barrier. The SLP sees the vocabulary mismatch. The ABA therapist sees the negative conditioning history. Only a coordinated team sees all three simultaneously — and addresses them together.
🗣️ Speech-Language Pathologist — PRIMARY LEAD
Identifies the specific barrier causing refusal. Programs vocabulary. Guides modeling approach. Conducts reassessment. The SLP holds the AAC implementation map.
🧠 Occupational Therapist — ACCESS & SENSORY
Evaluates motor access barriers. Recommends keyguards, styluses, positioning. Addresses sensory aversions to device features. Essential when refusal has a physical or sensory component.
📊 BCBA / ABA Therapist — BEHAVIORAL LAYER
Analyzes the refusal behavior function. Removes pressure systematically. Engineers guaranteed-success opportunities. Builds positive conditioning through precise reinforcement.
📚 Special Educator — SCHOOL CONSISTENCY
Ensures AAC implementation at school matches home approach. Trains school staff. Creates inclusive AAC opportunities in classroom routines.
👨⚕️ NeuroDevelopmental Pediatrician — MEDICAL
Rules out medical factors affecting AAC tolerance (pain, medication effects, comorbidities). Coordinates with the full clinical team.
Six Barrier Targets. Address the Right One and Everything Changes.
Each target maps to a specific set of materials. Identifying the correct barrier is the single most important step in resolving AAC refusal. A team approach ensures no barrier goes undetected.
Target 1: Vocabulary Match
Child encounters words they genuinely care about. Measured by: AAC Engagement Index during interest-based activities.
Target 2: Partner Modeling Volume
All communication partners model with AAC 20+ times/day. Measured by: daily modeling tracking sheets.
Target 3: Access Success Rate
Greater than 80% successful symbol hits with adapted access tools. Measured by: session data tracking.
Target 4: Positive Association
Neutral to positive response when device is present. Measured by: behavioral observation (approach vs. avoidance).
Target 5: Sensory Tolerance
No covering ears, no visual avoidance, no tactile rejection. Measured by: sensory response log.
Target 6: System Match
Child engages more when system is adjusted. Measured by: comparative engagement tracking across systems.
Nine Materials. Each One Addresses a Specific Barrier.
Drawn from Pinnacle's 128 Canon Material System and verified by 20M+ session outcomes, these nine materials form a complete toolkit for overcoming AAC refusal — from ₹0 DIY approaches to specialized clinical tools.
1
Interest-Based Vocabulary Overlays
Vocabulary mismatch barrier
2
Partner Modeling Materials
Modeling deficit barrier
3
Low-Tech Starter Options
Device-specific resistance
4
Access Tools
Motor access barrier
5
Motivating Activities
Negative association barrier
6
Visual Supports
Anxiety and novelty barrier
7
Sensory-Friendly Options
Sensory barrier
8
Success-Guaranteed Opportunities
Learned helplessness barrier
9
Reassessment Materials
System mismatch barrier
💰 Price range: ₹0 → ₹20,000+ | Most effective interventions cost ₹0 (approach changes) | DIY available for all 9 materials | Need guidance? Call FREE Helpline: 9100 181 181

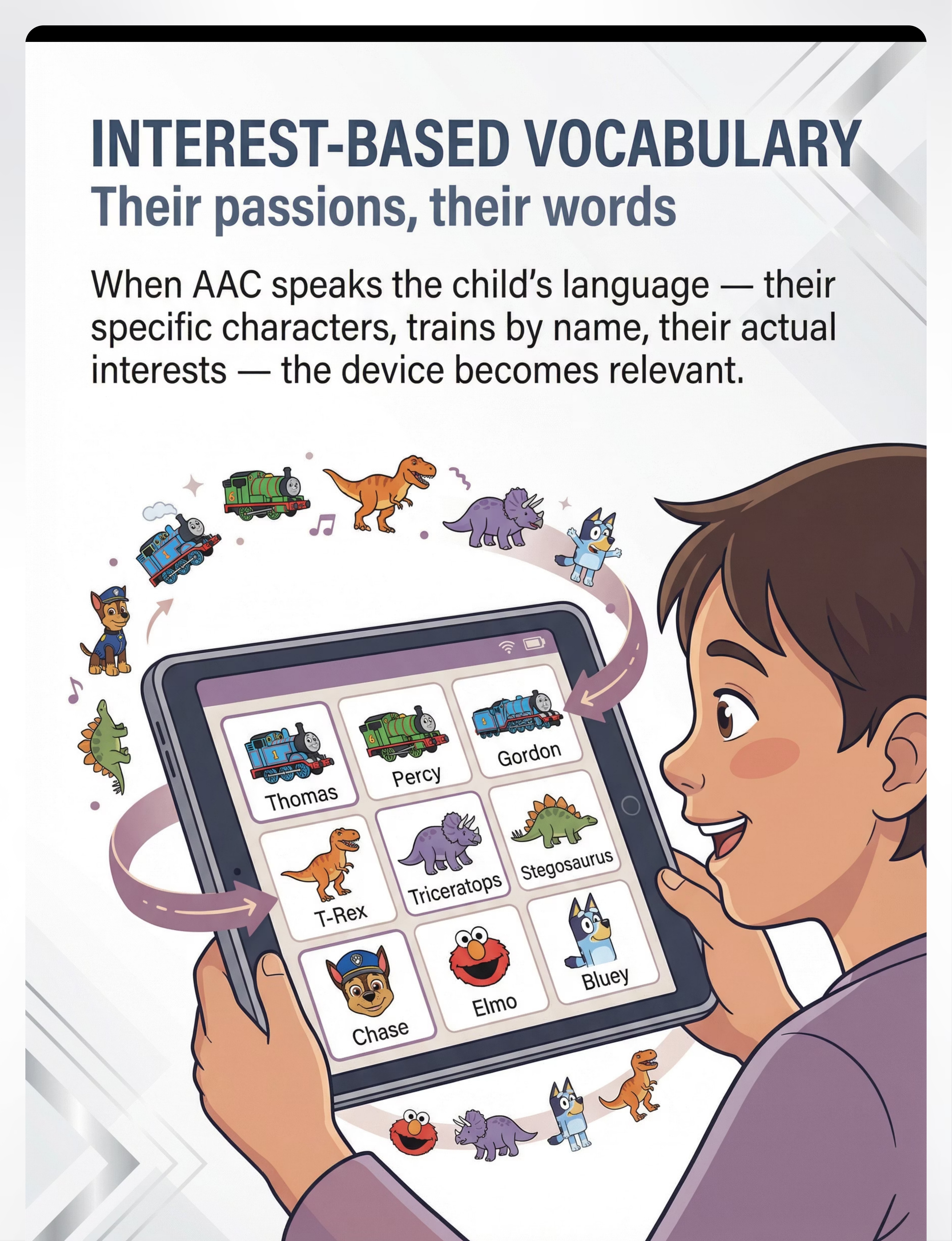
Material 1: Interest-Based Vocabulary Overlays
Their passions, their words.
Addresses: Vocabulary Mismatch
The most common cause of AAC refusal is vocabulary mismatch. Generic starter vocabularies contain words adults believe children should say — colors, numbers, "please," "thank you." But a child obsessed with specific dinosaurs finds no dinosaur vocabulary. When AAC suddenly speaks the child's actual language — not generic words but their specific passions — engagement transforms. The device becomes relevant. Worth touching. Worth the effort.
What, Why & When
What: Custom vocabulary pages programmed around the child's genuine, specific interests — actual names, specific characters, real details of their special interest.
Why: Intrinsic motivation. A device that names the exact trains a child knows by heart creates powerful motivation that generic vocabulary never can.
When: Immediately — this is the fastest change to make and often the most transformative.
How To Do It
- Observe what the child actually cares about (not what you think they should care about)
- List the specific names, characters, objects — not categories
- Add these as vocabulary pages in the existing AAC app
- Model with this new vocabulary during play with those specific interests
- Update regularly as interests evolve
📦 Brainy Bug Resources Flashcards with App-Enabled Audio: ₹305 | Amazon.in | DIY Zero-Cost: Print photos of the child's actual favorite things. Make a paper board. Cost: ₹0.
Safety Note: Interest vocabulary supplements core vocabulary — it does not replace it. The child needs both passion-words AND core language words ("want," "more," "stop," "help"). | "Would you want to use a language that couldn't express what you care about most? Neither does your child." | 📄 NCAEP 2020 — interest-based instruction classified as evidence-based practice for autism

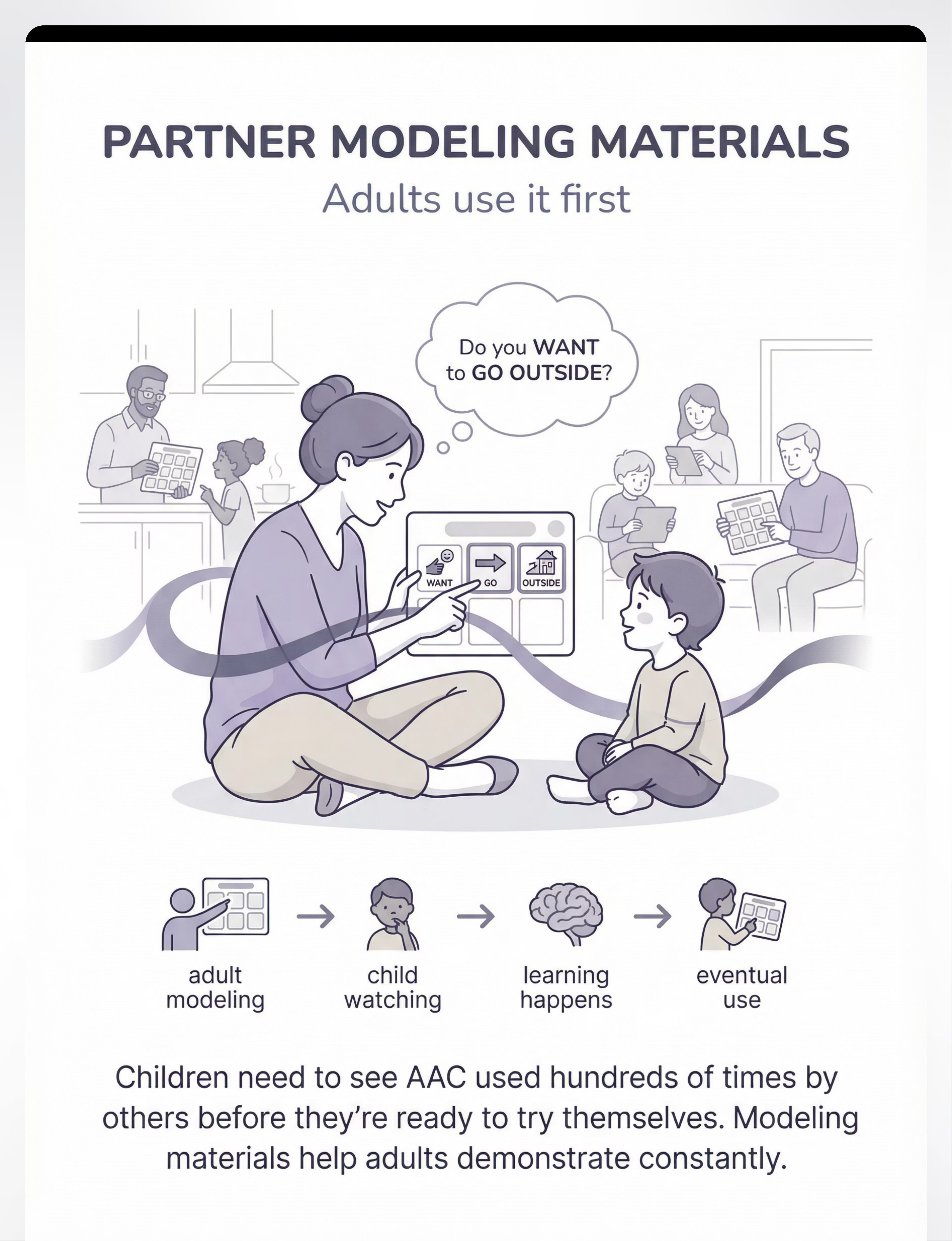
Material 2: Partner-Focused Modeling Materials
Adults use it first.
Addresses: Modeling Deficit
Many children refuse AAC because they have never seen anyone else use it. Imagine being handed a tool no one around you uses — with no demonstration of how it becomes real communication. Research consistently shows children need to observe hundreds to thousands of AAC model productions before spontaneous use emerges. This is normal. This is how language acquisition works.
The Modeling Formula: Adult points to symbol + says the word simultaneously. Not: "Can you say ___?" — just: models naturally during real conversation.
How To Model Effectively
- Print/display a communication board in every room
- Point to symbols while speaking: "Do you WANT [point] to GO [point] OUTSIDE [point]?"
- Use AAC to comment, not just request: "I SEE [point] a dog!"
- Model wrong selections occasionally — shows AAC is safe even when imperfect
- Track modeling instances with a simple daily tally
📦 Duplicate laminated communication boards: ₹200–500 | 1800+ Reward Stickers for tracking motivation: ₹364 | Amazon.in
DIY: Print core word boards from ARASAAC (free). Laminate at any local print shop (₹10–20/sheet). Post everywhere.
Where & When
Where: Everywhere the child is. Kitchen, bedroom, playground, car, classroom. AAC modeling has no "therapy room only" rule.
When: Now, and continuously for weeks to months. There is no such thing as modeling too much.
Safety Note: Modeling must be genuine communication, not drill. The child must see AAC as real language, not a therapy task.
"You wouldn't expect a child to speak English if no one around them spoke English. You cannot expect a child to use AAC if no one around them uses AAC."
📄 PMC11506176 — aided language stimulation classified Level I evidence for AAC acquisition
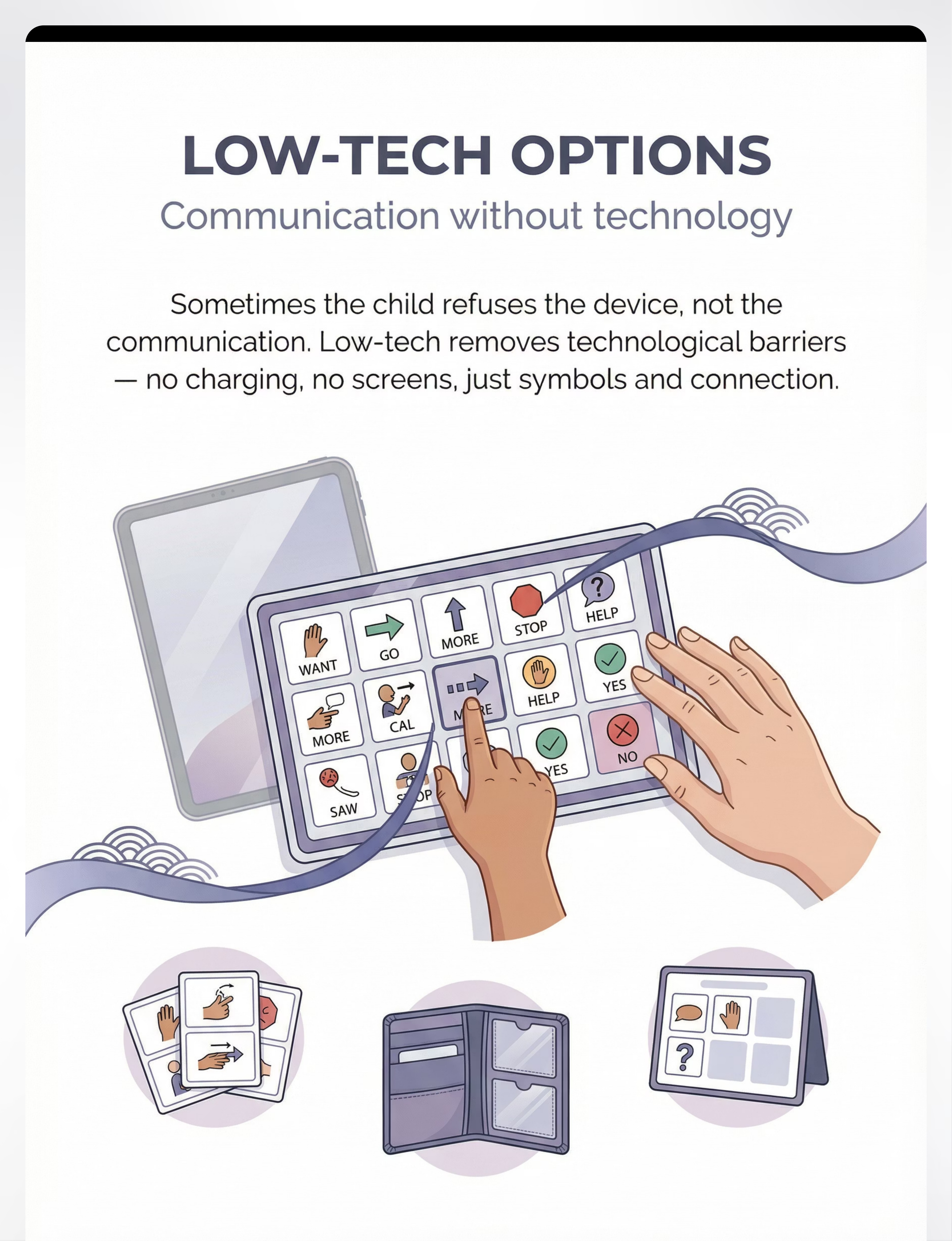
Material 3: Low-Tech Starter Options
Communication without technology.
Addresses: Device-Specific Resistance
Sometimes AAC refusal is specifically about the device — not the communication. The tablet's weight. The screen's brightness. The touchscreen's required pressure. Low-tech AAC removes every technological barrier: no charging, no loading, no navigation, no screens. Just symbols and communication. For some children, low-tech serves as a bridge. For others, it remains the permanent preference. Both are valid. The goal is communication, not device adoption.
What It Includes
- Laminated communication boards
- Paper-based PODD books
- Symbol cards with Velcro backing
- Communication wallets
- Choice boards for mealtimes and transitions
Why it works: Reveals whether the barrier is AAC itself or specifically the technology. If engagement appears with paper that didn't appear with the device, the problem is identified.
How To Implement
- Print a 12-symbol core word board (free from ARASAAC or Boardmaker)
- Laminate (₹10–20 per sheet at any print shop)
- Post at child's eye level in key locations
- Model with the paper board just as you would with the device
- Observe: does engagement increase when the tablet is out of the equation?
📦 Monkey Minds Clip The Card (visual symbol-matching readiness): ₹296 | Amazon.in
DIY Zero-Cost: Hand-draw or print symbols on regular paper. Tape to cardstock. Even a 4-symbol choice board communicates. Cost: ₹0.
Safety Note: Low-tech requires communication partners to voice the child's selections consistently. Agree on this across all adults before introducing. | "The goal is communication, not a specific device. Meet the child where they are." | 📄 NCAEP 2020 — visual supports including low-tech AAC classified as evidence-based practice for autism

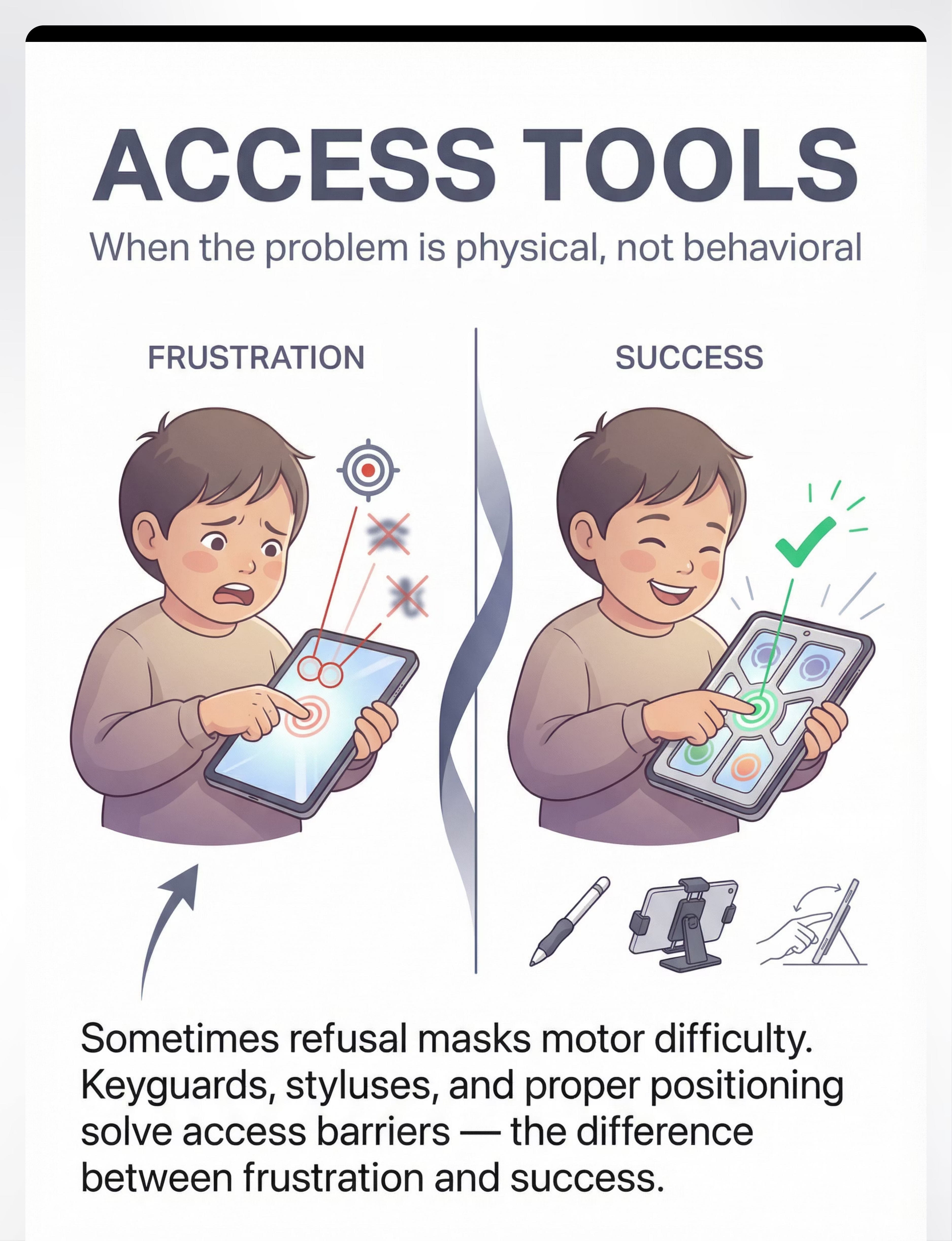
Material 4: Access Assessment and Adaptation Tools
When the problem is physical, not behavioral.
Addresses: Motor Access Barrier
A significantly underrecognized cause of AAC refusal is motor access difficulty. The child wants to communicate — but every attempt results in the wrong symbol being activated. When every touch fails, AAC becomes associated with frustration rather than successful communication. The child stops — and this reads as behavioral refusal when it is actually a motor planning and access barrier.

The Problem: Access Failure
Targets too small. Icons too close. Touchscreen pressure requirements unreliable. Device positioned poorly. Every failed touch teaches the child "AAC doesn't work."

The Solution: Access Tools
Keyguards physically separate touchscreen targets. Styluses extend reach and improve targeting accuracy. Device mounts ensure optimal positioning. Success rate jumps from under 40% to over 80%.
What to Use
- Keyguards: ₹500–5,000 (device-specific)
- Styluses (universal): ₹200–800
- Device mounts and stands: ₹1,000–5,000
- Alternative access: switch scanning, eye gaze technology
📦 Problem-Solving / Cause-Effect Toys for motor planning readiness: ₹519 | Amazon.in
How to Assess Now
- Watch 5 minutes of AAC use. Count successful vs. unsuccessful hits.
- If less than 80% accuracy: access assessment needed
- Try reducing the number of visible symbols
- Try a keyguard if available
- Consult OT for formal assessment if concern persists
DIY: Position device on non-slip mat at table height. Reduce grid to 4 symbols. Observe whether accuracy improves. Cost: ₹0. | 📞 Helpline: 9100 181 181
Safety Note: Motor access assessment should involve an OT for children with significant motor challenges. Incorrect setup can increase frustration. | 📄 ASHA AAC Practice Portal (2024) — access assessment is a core clinical practice component
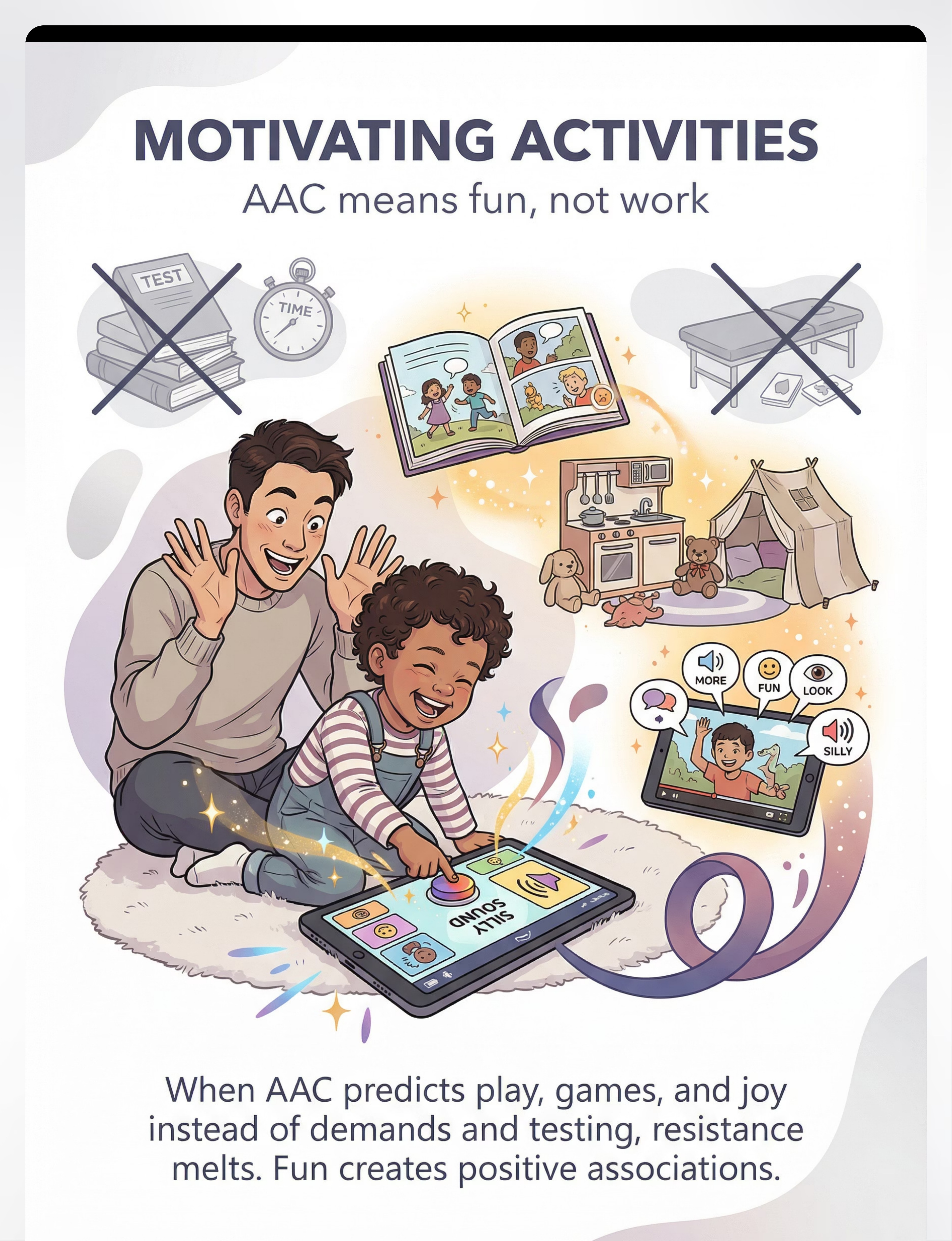
Material 5: Motivating Communication Activities
AAC means fun, not work.
Addresses: Negative Association
AAC refusal frequently traces back to AAC being consistently associated with demands, drills, testing, and pressure. When every device appearance precedes "touch the apple" — the device becomes a signal for work. The child avoids work. Motivating activities reverse this conditioning entirely. AAC appears during what the child loves most. The child's nervous system learns a new prediction: AAC = fun.
Interactive Books
Device produces story sounds, character voices. AAC becomes part of the storytelling magic.
AAC-Controlled Games
AAC delivers commands, controls outcomes, makes silly things happen. Every touch produces delight.
Pretend Play Scripts
AAC voices the characters the child loves. Their special interest meets their communication tool.
Cause-Effect Pairing
AAC symbol touches paired with delightful, immediate outcomes the child craves.
How To Implement
- List the top 5 things that make your child laugh or light up
- Embed AAC into those activities — not as a requirement but as a tool that makes the fun better
- Never require AAC use; always model and celebrate any touch attempt
- Use AAC to comment, exclaim, predict fun: "MORE [point] bubbles!"
- If the child approaches the device voluntarily: that is the beginning of acceptance
The Golden Rule
Never make fun contingent on AAC use ("You can play AFTER you use your talker"). This creates negative associations. AAC should be the fun, not the barrier to fun.
📦 Dyomnizy Educational Memory Game with Lights & Sound: ₹519 | Amazon.in | DIY: Use your paper board during favorite play. Build "symbols = getting what you want" through low-tech fun first. Cost: ₹0.
📄 NCAEP 2020 — reinforcement-based instruction classified as evidence-based practice | PMC10955541

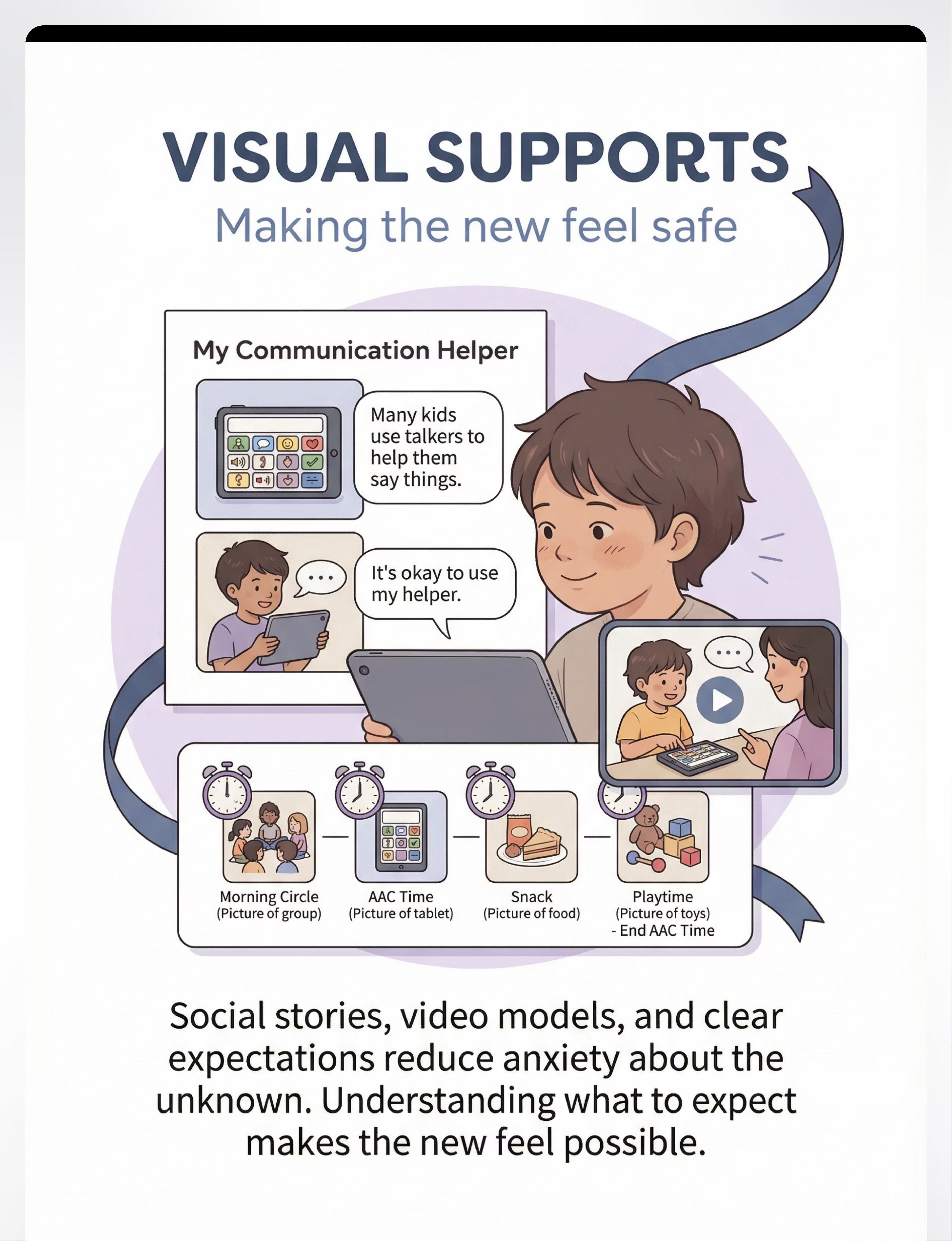
Material 6: Visual Supports for AAC Introduction
Making the new feel safe.
Addresses: Anxiety & Novelty
For children with autism, anxiety about the unknown is a major driver of refusal. A new device, new expectations, new skills to learn — all are change, and change triggers the nervous system's threat response. Visual supports prepare the child cognitively and emotionally for AAC. They don't teach AAC skills. They prepare the ground so learning can occur.
Social Stories
Simple illustrated narratives: "Many children use communication helpers. My helper is called [name]. It helps me say things. It is okay to use my helper."
Visual Schedules
Where AAC time sits in the daily routine — and when it ends. Anxiety reduces when children know what comes next and how long something lasts.
First-Then Boards
"First: we look at my talker together. Then: we play with trains." Clear, predictable, time-limited. Transforms the unknown into something manageable.
Video Models & Photo Books
Other children using AAC successfully. Photos of the child's own device in their own environments — making it familiar before use begins.
How To Implement
- Create a simple social story using photos of the child's actual device
- Read together once daily — casually, not as "AAC time"
- Show YouTube videos of children using AAC (many available publicly)
- Place AAC in the visual schedule but keep time short and follow with something desired
- Never surprise the child with AAC — always give 5-minute advance notice
Resources
Social story printing: ₹100–300 at local print shop | First-then boards: ₹200–500 | 📦 Reward Stickers for schedule completion: ₹364 | Amazon.in
DIY: Write a 5-sentence social story using Google Docs + photos from your phone. Print on regular paper. Cost: ₹0.
Safety Note: Visual supports should never promise outcomes ("You will love your talker!"). They should explain factually and validate that learning something new can feel hard.
📞 Helpline: 9100 181 181 | 📄 NCAEP 2020 — visual supports classified as evidence-based practice

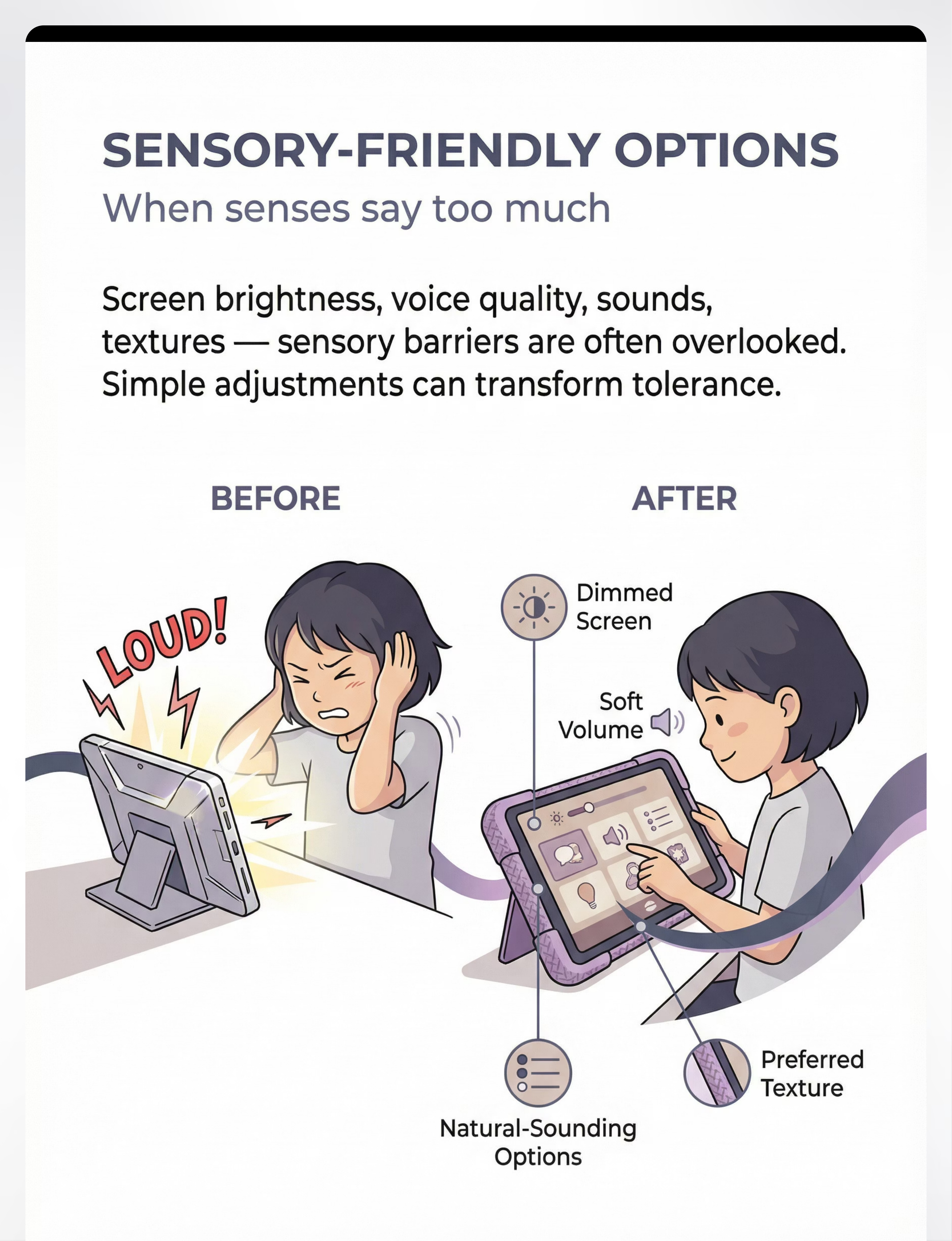
Material 7: Sensory-Friendly AAC Options
When senses say "too much."
Addresses: Sensory Barrier
Sensory factors in AAC refusal are consistently underrecognized. The device may be too heavy for children with low muscle tone. The screen brightness may be visually overwhelming. The synthesized voice may be auditorily aversive. For sensory-sensitive children, any of these factors makes the device intolerable — not because of communication resistance but because of sensory overwhelm. The child is not refusing communication. They are refusing pain.

Sensory Overload Signals
Covers ears (auditory barrier). Pulls hand back from device (tactile barrier). Looks away from screen (visual barrier). Resists device weight (proprioceptive barrier).

After Sensory Modification
Dimmed screen, natural voice, silent notifications, soft fabric case, device mounted on stand. Same child, same device — transformed experience.
Screen Settings
Reduce brightness to 30–40%, enable Night Shift/warm tone filters
Voice Settings
Select natural-sounding voices, reduce volume, slow speech rate
Sound Settings
Disable all notification sounds, click feedback, and keyboard sounds
Case & Weight
Try fabric-covered or silicone cases; use a device mount so the child never holds the device
Safety Note: If sensory issues appear significant, consult an OT. Sensory AAC modifications may need to be part of a broader sensory support plan. Most modifications cost ₹0 — start with device settings today. | 📄 Frontiers in Integrative Neuroscience (2020) — DOI: 10.3389/fnint.2020.556660
Material 8: Success-Guaranteed Communication Opportunities
Breaking the failure cycle.
Addresses: Learned Helplessness
Learned helplessness is one of the most powerful forces in AAC refusal. When a child has repeatedly experienced AAC failing, they develop a neural prediction: "This device leads to failure." Avoidance is adaptive. Why attempt something that always fails? The solution is engineering guaranteed success — communication opportunities so easy, so supported, so certain to succeed that the child experiences AAC working — perhaps for the first time.
The first experience of "I touched it, it worked, I got what I wanted" is transformative — and it must be engineered, not hoped for.
What To Use
- Errorless learning protocols — only one symbol visible, every touch is correct
- Hand-over-hand guidance fading gradually as confidence builds
- Single-symbol communication boards for initial success
- Most-to-least prompting hierarchy
- Immediate, enthusiastic response to every attempt
Step-by-Step Protocol
- Identify one thing your child wants more than anything
- Create a single-symbol board with ONLY that symbol
- Wait for the right moment and gently guide hand to touch it
- Respond IMMEDIATELY with desired item + enthusiastic praise
- Repeat 5–10 times per day
- Gradually remove physical guidance as child touches independently
- Gradually add more symbols as confidence grows
📦 Reward Jar for success celebration: ₹589 | Amazon.in | Cost for strategy: ₹0 | 📞 Helpline: 9100 181 181
Safety Note: Guaranteed success requires instant responsiveness. A successful touch that receives no response is worse than no attempt — it teaches that AAC doesn't reliably work. | "No one persists at something that only fails. Create success, and the child will want more."

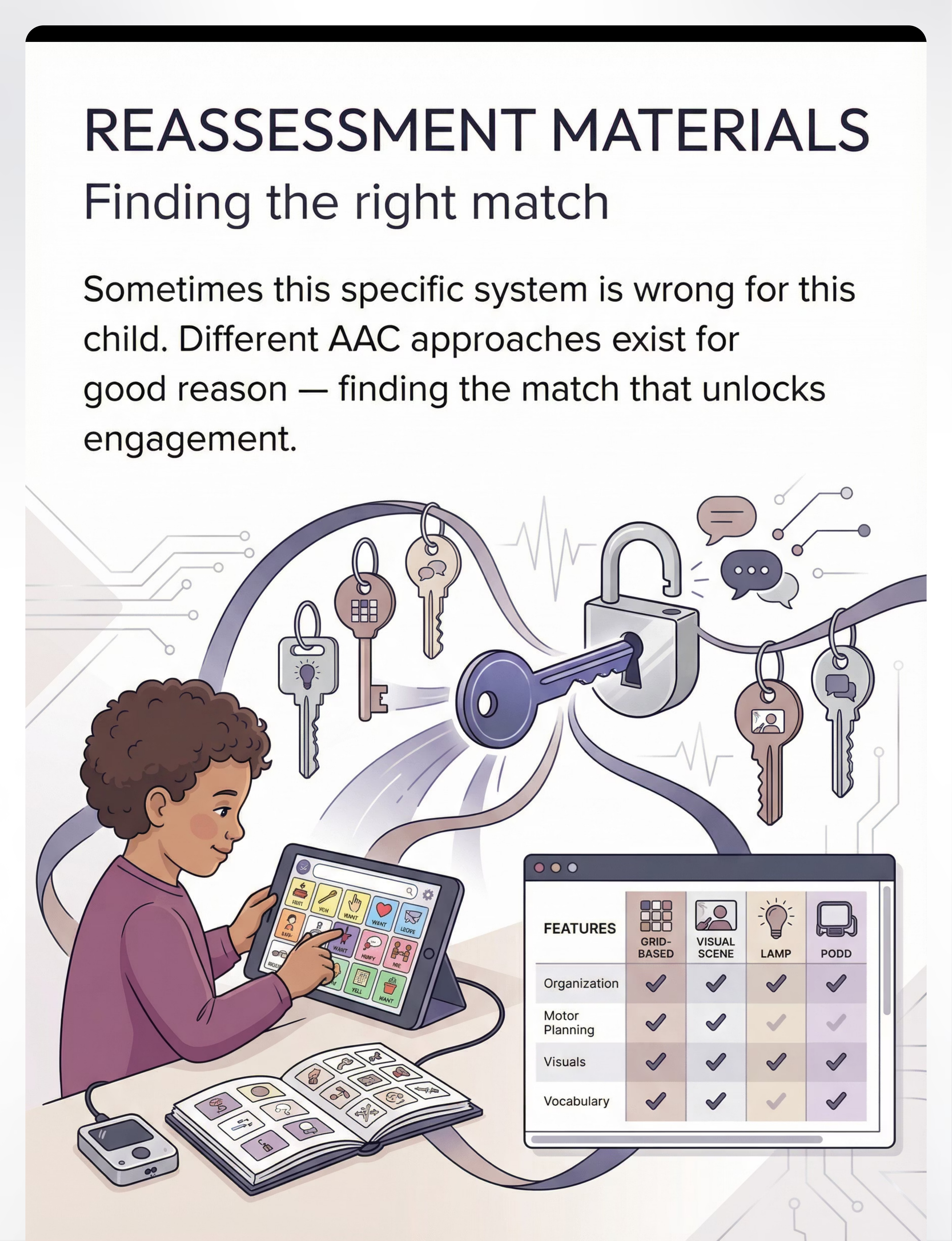
Material 9: AAC Reassessment and Alternative System Materials
Finding the right match.
Addresses: System Mismatch
Sometimes, despite addressing all other barriers, persistent refusal signals a deeper mismatch between the child and the specific system. Different AAC approaches exist for good reason. Grid-based systems work brilliantly for some children and are impossible for others. Reassessment materials help systematically evaluate whether a different system might work better — because there is no single best AAC system. There is only the best system for THIS child.
System Type | Best For | Potential Barrier | |
Grid-Based (Proloquo2Go, TouchChat) | Most learners; strong SLP support | Navigation complexity for some | |
LAMP (Motor Planning) | Consistent motor planning learners | Requires intensive motor training | |
Visual Scene Displays | Strong visual-contextual processors | Limited generalization | |
PODD | Children needing extensive vocabulary with partner support | Partner training intensive | |
Low-tech boards | Children with device-specific resistance | Partner voicing required |
Reassessment Protocol
- Document all barriers already addressed and their outcomes
- Consult SLP for formal reassessment referral
- Download trial versions of 2–3 alternative systems
- Trial each for 2–4 weeks with consistent modeling
- Track engagement data across systems
- Choose based on child's data, not adult preference
What You'll Need
- AAC app trial versions (most offer free trials)
- Comparative feature and access charts
- SLP reassessment consultation
- Systematic trial protocols (2–4 weeks per system)
- Alternative access trials (eye gaze, switches)
Safety Note: Changing systems requires professional guidance. Don't abandon a system too quickly — modeling takes months. But don't persist indefinitely with a poor match. | 📄 ASHA AAC Practice Portal (2024) | Light & McNaughton (2015)

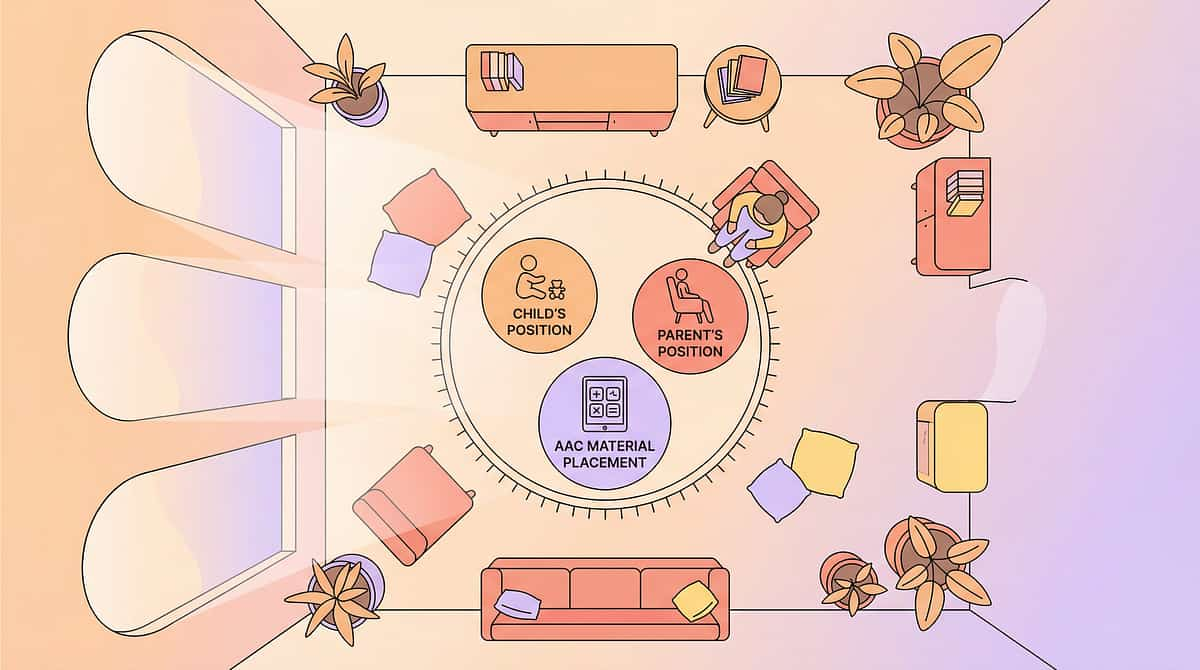
Session Readiness Gate
The best session is one that starts right. Before every AAC engagement, check these seven gates. One great session builds more positive association than ten forced sessions. Forcing AAC engagement when the child is dysregulated actively builds negative associations — precisely the opposite of what you're working to create.
🟢 GO — Proceed
- Child is calm and regulated (not in sensory overload)
- Child has been fed and is not tired
- Environment is low-stimulation (noise reduced, no competing screen)
- You have removed all demand/pressure from your own body language
- Fun materials are prepared and visible
- Duration is short (5–10 minutes maximum)
- Success is guaranteed (single-symbol or interest-first setup ready)
🟡 MODIFY — Adjust First
- Child is mildly unsettled → co-regulate first (5 min calm-down)
- Favorite activity isn't available → substitute with second-best option
- Only 3 minutes available → proceed with 1 goal only
🔴 POSTPONE — Not Today
- Child is in meltdown or post-meltdown recovery
- Child is sick, in pain, or medically unwell
- Child has just experienced significant stress/transition
- Parent/caregiver is dysregulated (calm regulation is contagious)
📄 ABA setting events and antecedent manipulation — core principles of effective behavioral intervention. Calm regulation is contagious in both directions — your regulated presence is itself a therapeutic tool.

The 6-Step AAC Acceptance Protocol
Six steps. Every AAC session, in order. This sequence is not arbitrary — each step builds the neurological and behavioral conditions that make the next step possible. Follow the order consistently for best results.
01
The Invitation (30–60 seconds)
Approach with materials the child loves — not the device. Begin play. After 1–2 minutes, introduce AAC casually: "Oh look, your talker is here too." Body language: relaxed, curious, not expectant.
02
Adult Models First (1–3 minutes)
You use the AAC. Point to the symbol + say the word. Comment on what's happening in play. Don't ask the child to do anything. Just model naturally.
03
Create the Opportunity (1–2 minutes)
Set up a moment where AAC would naturally solve a communication need. Pause expectantly. Wait 5 seconds. If no response, model the symbol yourself and deliver the item. Never withhold fun to force communication.
04
Respond Within 3 Seconds
If the child touches ANY symbol — respond IMMEDIATELY. Say the word. Deliver the associated item. Celebrate: "Yes! You said MORE! MORE bubbles coming!" Timing within 3 seconds is the mechanism of learning.
05
Repeat 3–5 Times
3 successful communication exchanges is a complete session. Quality over quantity. Stop while the child is still engaged and wanting more.
06
Cool Down Transition (1–2 minutes)
"Two more, then all done." Use a visual timer. Child puts the device in its home spot. Transition with a preferred activity. Never end abruptly.
📄 PMC11506176 | ABA aided language stimulation protocols | NCAEP 2020 | 📞 Helpline: 9100 181 181

Capture the Data — Right Now
Within 60 seconds of every session. Every time. No data means no ability to see whether the approach is working. Four sessions of data is enough to identify a pattern. Eight sessions is enough to make an informed decision about strategy adjustment.
THE 4-FIELD AAC SESSION LOG
Date: ___________ | AAC Strategy Used (circle): Vocabulary / Modeling / Low-Tech / Access Tools / Fun Activity / Visual Support / Sensory Mod / Success Guarantee / Reassessment
Symbols Touched (total): ___ | Successful Communication Exchanges: ___
Child's Response (circle): Active Refusal / Passive / Tolerating / Beginning Engagement / Engaged
Parent Note (1 sentence): ___________________________
Date: ___________ | AAC Strategy Used (circle): Vocabulary / Modeling / Low-Tech / Access Tools / Fun Activity / Visual Support / Sensory Mod / Success Guarantee / Reassessment
Symbols Touched (total): ___ | Successful Communication Exchanges: ___
Child's Response (circle): Active Refusal / Passive / Tolerating / Beginning Engagement / Engaged
Parent Note (1 sentence): ___________________________
4 Sessions
Enough data to identify a pattern and spot what's working or not working
8 Sessions
Enough to make an informed decision about whether to adjust strategy
16 Sessions
Enough for your professional team to review and recalibrate the full approach
Your session log feeds directly into GPT-OS® AbilityScore® tracking for professional team review. Every data point makes the next session smarter.
📄 BACB measurement standards — data-based decision making as core ABA practice

Troubleshooting & Personalization
When it doesn't go as planned — here's what to do. Every child's AAC journey is unique. Use this guide to identify what you're seeing, trace it to the most likely barrier, and make an immediate, evidence-based adjustment.
What You Observe | Most Likely Barrier | Immediate Adjustment | |
Child cries when device appears | Severe negative association | Remove device 2 weeks; rebuild with paper boards only | |
Touches device but wrong symbols | Motor access barrier | Reduce to 2-symbol board; try keyguard | |
Engages with play, ignores device | Vocabulary mismatch | Are the child's specific interests on the device? | |
Engaged last week, refusing today | Environmental/physiological | Check for illness, sleep changes, schedule disruption | |
Uses AAC at home, not at school | Generalization barrier | Ensure school uses identical vocabulary + modeling approach | |
Uses AAC with one parent, not other | Partner training gap | Co-train all caregivers on the same protocol | |
No progress after 8 consistent weeks | System mismatch or unidentified barrier | Request SLP reassessment |
Easier Version (Setback Days)
1 symbol only. Interest-based. Zero demand. Maximum support. This is not going backward — this is strategic consolidation.
Harder Version (Breakthrough Days)
Increase vocabulary range. Reduce prompting level. Introduce 2-symbol combinations. Expand to new settings and communication partners.
Week 1–2: Calibrate Your Expectations Here
Act IV — The Progress Arc
The first two weeks are about building the neurological foundation — not yet about visible AAC use. Progress here is real and clinically significant, even when it's invisible from the outside. Neural pathways are forming. The foundation is being built.
15%
Week 1–2 Progress
Foundation phase — tolerance and neural recalibration
✓ What You WILL See
- Child tolerates device presence in the room without distress (this is progress)
- Child watches you model with AAC (this is learning)
- Child may touch the device accidentally or exploratorily (this is the beginning)
- Reduced crying or protest when device appears (this is neurological recalibration)
✗ What You Will NOT See Yet
- Spontaneous independent symbol selections
- Consistent AAC use
- Generalization across settings
And that's okay. If your child tolerates the device for 3 seconds longer than last week — that is real, measurable, clinically significant progress.
📄 PMC11506176 — sensory integration and communication outcomes develop across 8–12 week timelines; early phase indicators focus on tolerance and participation, not production
Week 3–4: Neural Pathways Are Forming
40%
Week 3–4 Progress
Consolidation phase — approach behavior emerging
Consolidation is happening. The child's nervous system is beginning to predict something different when AAC appears. Watch for these specific indicators — they are the clinical signs that the approach is working.
Anticipation Signs
Child anticipates AAC during favorite activities — moves toward the device area before you bring it out.
Interest in Modeling
Child watches your modeling with visible interest — leaning in, tracking your finger movements.
Voluntary Touch
Child touches device voluntarily without prompting — even without communicative intent. This is exploratory engagement.
Vocabulary Response
Interest-based vocabulary produces visible engagement — child lights up seeing their words represented.
What to Increase Now
- Vocabulary range (add 5–10 new interest-based words)
- Modeling frequency (from 20/day to 30+/day)
- Variety of communication contexts where AAC appears
Parent Milestone
You may notice you're less anxious when you bring out the device. That relaxed energy reaches your child. Your growing confidence is itself therapeutic.
📄 PMC10955541 — neuroplasticity: synaptic strengthening through repeated structured input follows predictable timelines in pediatric populations
Week 5–8: The Breakthrough Zone
75%
Week 5–8 Progress
Mastery phase — functional AAC engagement emerging
This is where the transformation becomes visible. Document everything you observe in this phase — these moments are precious and they are the direct result of consistent, patient, barrier-focused work.
✓ Independent Use
Child independently touches AAC symbols to communicate — without prompting — in at least 2 different contexts
✓ Device Seeking
Child seeks out the device or communication board when wanting something. The device is now a tool, not a threat.
✓ Multiple Partners
Child uses AAC with more than one communication partner — generalization is beginning
✓ Functional Dependence
Child shows frustration when AAC is unavailable. This is good — it means they rely on it to communicate.
Generalization Check: Does AAC use happen in the kitchen? ✓ At school? ✓ During transitions? ✓ With grandparent? ✓ When mastery criteria met in 3+ contexts, introduce the next vocabulary tier or complexity level. | 🏆MASTERY UNLOCKED: Child has moved from AAC refusal to functional AAC engagement | 📄 PMC10955541 | BACB mastery criteria standards

You Did This. Your Child Found Their Voice Because You Refused to Give Up.
Your child went from refusing a communication device — from crying when it appeared, from pushing it off the table — to using it to tell you what they need and want. Think about what that means. Think about what they can now say that they could not say before.
🎉 Create a Memory
Create a "First Word on AAC" photo album. This moment deserves to be documented and remembered.
📸 Journal This
Document this milestone in your child's developmental journal — future you will want to read it.
🤝 Share With Team
Tell your Pinnacle therapy team — this goes in the progress record and informs the next phase.
💌 Share With Family
Send a message to the grandparents, the teacher, the SLP who helped you get here. They need to know.
"The first time my child used AAC to tell me something I understood was ___________. They said: ___________. My reaction was: ___________."
📄 Parental self-efficacy research — parent confidence is the strongest predictor of continued home-based intervention implementation. Your success is the intervention.

Red Flags — When to Pause
Trust your instincts — if something feels wrong, pause and ask. These are the signs that require you to stop the current approach and contact your clinical team. Early escalation is always the right call.
🔴 Motor Regression
Child was using AAC and suddenly cannot hit targets reliably → may indicate neurological concern. Stop and contact your clinician.
🔴 Complete Communication Shutdown
Child stops ALL communication attempts (AAC + other methods) → urgent clinical review. Do not wait.
🔴 Significant Behavioral Escalation
AAC sessions consistently end in severe distress → current approach creating harm; full reassessment needed immediately.
🔴 Self-Injurious Behavior
Child harms themselves during or after AAC sessions → behavioral assessment required. This is urgent.
🔴 Medical Changes
AAC regression coinciding with medication changes, illness, or sleep disruption → medical review required.
🔴 No Progress After 12 Weeks
Consistent implementation with no measurable movement → SLP + OT + ABA full reassessment needed.
Escalation Pathway: Self-resolve (1–2 days) → Call 9100 181 181 for teleconsult guidance → Schedule clinic visit → In-person assessment | Pinnacle Center Locator: pinnacleblooms.org/centers | 📄 WHO NCF Progress Report 2018–2023

The Progression Pathway
You're not done — you're on a journey. Here's where it leads. B-221 sits within a carefully sequenced curriculum of communication access techniques. Each episode builds on the last and prepares the ground for the next.
B-219: Receptive But Not Expressive
Child Has Receptive But Not Expressive Language — foundational understanding
B-220: Getting Started with AAC
Prerequisite: First introduction to AAC systems and approaches
B-221: Child Refuses AAC ← YOU ARE HERE ✓
The 9 materials that find the way back in — this episode
B-222: Building Vocabulary on AAC
Next logical step — expanding communication range
B-223 → B-225: Advanced Applications
AAC in the Classroom | AAC and Motor Access | AAC and Speech Together
Lateral Options: → B-230: PECS Implementation for Communication Beginners → B-245: Sign Language as a Communication Bridge → B-260: Speech-Generating Devices: High-Tech Options | Long-term goal: Functional communication → social participation → educational access → community independence → self-advocacy
Related Techniques in Domain B: Communication Access
The communication access domain contains a rich sequence of techniques that work together. If you've built your AAC vocabulary boards and modeling approach for B-221, you already have the materials for the next steps.
B-219: Receptive/Expressive Gap
Understanding children who understand language but cannot yet express it — the prerequisite foundation
B-220: AAC Getting Started
First introduction to AAC systems. Uses same communication boards you've already made ✓
B-222: Building AAC Vocabulary
Next step — expanding vocabulary range using same AAC system you're now engaging with ✓
B-223: AAC in School
Ensuring school consistency and generalization. Builds on home approach established in B-221.
B-224: AAC Motor Access
Advanced access assessment — for children with significant physical access challenges
B-225: AAC + Speech Together
Integrating AAC with emerging speech development — the advanced integration phase

This Technique Is One Piece of a Much Larger Plan
Domain B: Social Communication & AAC — Active
Your work on AAC acceptance doesn't exist in isolation. Every gain in communication competence ripples outward — reducing behavioral challenges, building learning readiness, opening social connection. This is how communication access becomes life access.
1
Communication Competence
AAC acceptance builds functional communication across all daily contexts
2
Social Connection
Communication enables relationships, reducing isolation and behavioral challenges
3
Learning Readiness
Reduced frustration opens the door to academic and cognitive engagement
4
Life Outcomes
Independence, self-advocacy, community participation, and quality of life
GPT-OS® Integration: Your session data from this technique feeds the AbilityScore® Communication Domain tracker. As AAC engagement increases, the score updates and TherapeuticAI® adjusts adjacent therapy goals. | 📄 WHO/UNICEF NCF (2018) — five components of nurturing care require holistic monitoring | 📞 Helpline: 9100 181 181

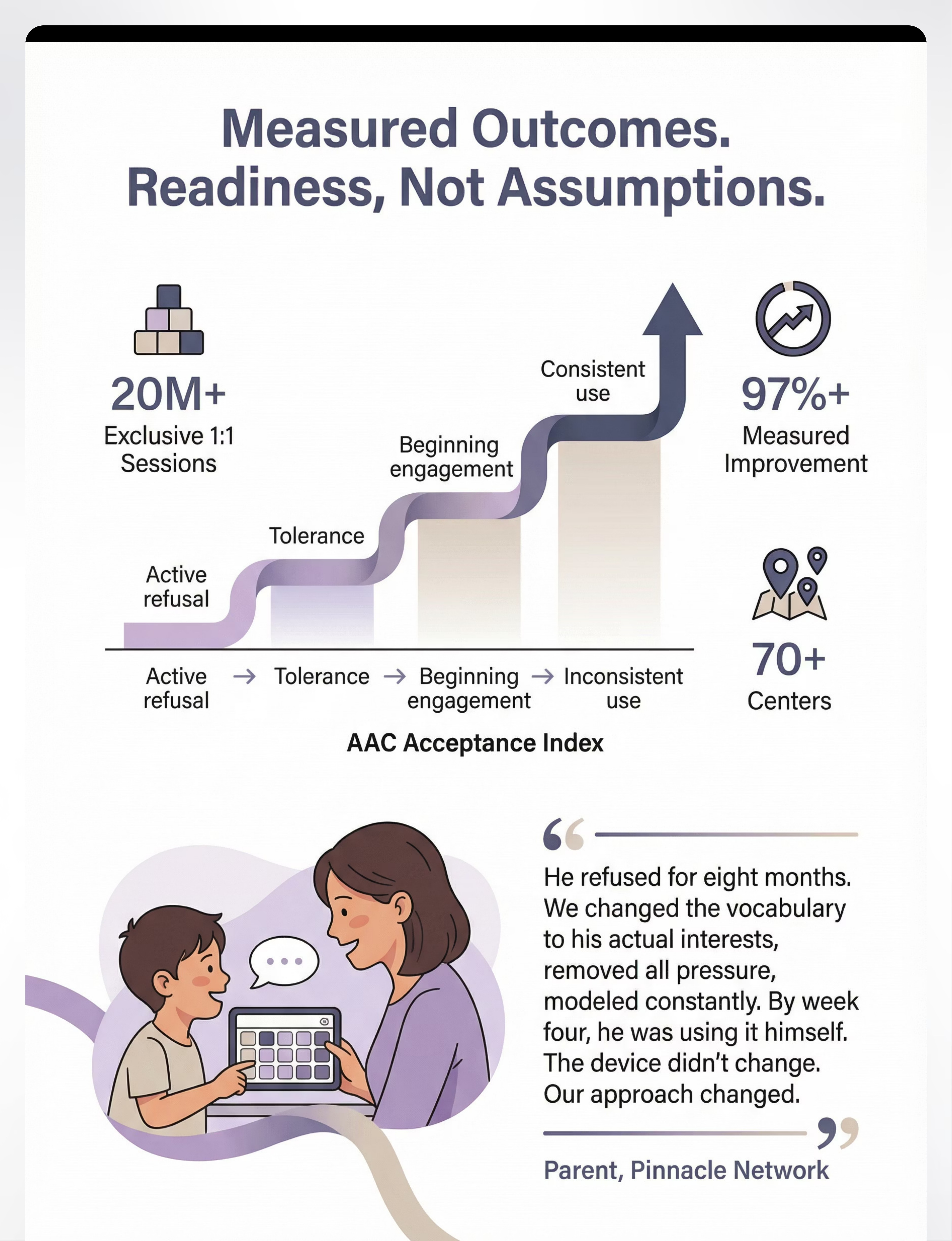
From the Pinnacle Network — Real Families, Real Outcomes
"Our daughter refused for eight months. Eight months of the device sitting there while we felt like failures. Her SLP finally asked us to step back and figure out WHY. The vocabulary was wrong — generic starter words when she was obsessed with specific things. We added her actual interests — her characters, her songs, her specific toys by name. We stopped all demands and just modeled while we played. Week two: she watched closely. Week three: she touched one symbol. Week four: she was using it independently. The device didn't change. The vocabulary changed. The approach changed. She was telling us it wasn't working. We finally listened." — Parent, Pinnacle Network Hyderabad (anonymized, consented)
"Six-year-old, non-speaking, with significant AAC resistance. OT assessment revealed motor access barriers — he was hitting adjacent symbols 60% of the time. Keyguard introduced. Within three sessions, successful hits rose to 85%. Within four weeks: spontaneous AAC requests. The refusal was never behavioral. It was physical." — Pinnacle OT + SLP team, Chennai center (anonymized)
"We stopped all pressure. We made the device appear only during his trains obsession. We added every single Thomas character by name. On day 19 he held the device himself and pressed 'Gordon' — a character we'd just added the week before. He pressed it looking directly at the train. That was his first spontaneous communication in 2 years." — Pinnacle BCBA, Bengaluru center (anonymized)
97%+
Measurable Progress
Of enrolled children show measurable AAC Acceptance Index movement within 16 weeks of systematic intervention
20M+
Sessions Validated
Therapy sessions informing these aggregate outcomes across 70+ centers

Connect With Other Parents
You are not navigating this alone. The Pinnacle parent community connects families who are 6 months ahead of you in this journey — ready to share what worked, what the timeline actually looked like, and how they held on during the hardest weeks. Your experience also has value: if your child has moved from AAC refusal to engagement, consider sharing your story. You may be the voice that helps another family not give up.
WhatsApp Group — AAC Families India
Connect directly with families navigating AAC acceptance right now. Request link via helpline: 9100 181 181
Pinnacle Parents Forum
AAC Acceptance Thread — specific vocabulary tips, school communication templates, honest timelines. pinnacleblooms.org/community
Local Parent Meetups
Organized at Pinnacle centers monthly. Meet experienced AAC parents face to face. Find your center to register.
Peer Mentoring
Connect with an experienced AAC parent who has been exactly where you are and found the way through.
📄 WHO NCF Community Engagement Principles — peer support networks improve intervention adherence and reduce parental burnout | 📞9100 181 181 to join the community
Home + Clinic = Maximum Impact
🗺️ 70+ Centers Across India
16+ Languages
Teleconsultation Available
The techniques in this guide are designed for home implementation — but they are most powerful when paired with professional assessment and monitoring. Your Pinnacle team identifies the specific barrier, customizes the approach, and tracks progress alongside you.
🗣️ SLP with AAC Specialization
Barrier assessment, vocabulary programming, modeling training. The primary lead for AAC refusal intervention.
🦾 OT for Access Assessment
Motor access evaluation, keyguard fitting, positioning. Essential when physical barriers are suspected.
📊 BCBA for Positive Conditioning
Pressure removal, success engineering, data systems. Addresses the behavioral layer of AAC refusal.
📚 SpEd for School Consistency
Staff training, classroom implementation, IEP support. Ensures generalization from home to school.
Service Options: In-center comprehensive AAC assessment (all 70+ centers) | Teleconsultation: 9100 181 181 (16+ languages, Mon–Sat) | Home visit program (selected locations) | School consultation (by arrangement) | Ask our team about insurance coverage and state disability welfare funding schemes.
The Research Library
The evidence behind this technique — for curious parents and clinicians who want to go deeper. Every recommendation in this guide traces to peer-reviewed evidence graded by the Oxford Centre for Evidence-Based Medicine framework.

Your Child's Data Makes Their Therapy Smarter. Every Session.
GPT-OS® Integration
Every data point you collect in Card 21's session log feeds a system that learns from your child's specific pattern — not from averages, but from their individual responses. Over time, the system identifies which barriers respond fastest, what optimal session parameters look like for this child, and when the next technique in the sequence is ready to be introduced.
The population-level insight is equally powerful: your child's de-identified data contributes to patterns that help children with similar profiles across India and beyond.
Privacy Commitment: All child data is encrypted, de-identified for population analytics, and governed under India's PDPB data protection framework. Your data helps every child like yours. | 📄 Digital health + ASD systematic reviews (2024) — personalized data-driven intervention shows measurable advantage over standardized protocols

Watch the Reel
The reel that started this journey — B-221. A Pinnacle SLP demonstrates all 9 materials in 75 seconds: vocabulary customization, partner modeling position, low-tech boards, keyguard, fun activity setup, visual supports, sensory adjustments, success engineering, and the reassessment framework. Watch it, share it, send it to your child's school.
Reel B-221
Title: 9 Materials That Help When Child Refuses AAC
Series: Communication Access & AAC Solutions — Episode 221
Duration: 75 seconds
Platform: @pinnacleblooms (Instagram / YouTube Shorts)
Link: pinnacleblooms.org/reels/B-221
Series: Communication Access & AAC Solutions — Episode 221
Duration: 75 seconds
Platform: @pinnacleblooms (Instagram / YouTube Shorts)
Link: pinnacleblooms.org/reels/B-221
Related Reels
- → B-220: Getting Started with AAC
- → B-222: Building Vocabulary on AAC
- → Browse all 999 Communication Reels
📄 Video modeling — NCAEP 2020 evidence-based practice for autism | Multi-modal learning improves parent skill acquisition
📞 Helpline: 9100 181 181 — Call to ask your Pinnacle SLP any questions that the reel or this guide raised for your specific child's situation
Share This With Your Family
Consistency across caregivers multiplies impact — and inconsistency across caregivers can undo weeks of progress. If only one parent uses AAC modeling, the child receives half the input. If the school is unaware of vocabulary changes, generalization doesn't happen. Every adult in the child's world must understand the same approach.
"Explain to Grandparents" Card
"We're helping [child's name] learn to use their communication device. Here's what helps:
1) Point to the symbols when you talk.
2) Never require them to use it — just model yourself.
3) Respond immediately when they touch any symbol.
4) Make it fun — use it during play.
That's it."
1) Point to the symbols when you talk.
2) Never require them to use it — just model yourself.
3) Respond immediately when they touch any symbol.
4) Make it fun — use it during play.
That's it."
Share Tools
- 📤 Share This Page — WhatsApp
- 📧 Email This Page
- 🔗 Copy Link
- 📄 Download Family Guide — 1-page PDF
- 📋 Teacher Communication Template — one-page school AAC consistency guide
The teacher template explains vocabulary used, modeling approach, response protocol, and what NOT to do.
📄 PMC9978394 — WHO CCD Package: multi-caregiver training critical for intervention generalization | 📞9100 181 181 — Call to request the school AAC consistency guide for your child's classroom
Frequently Asked Questions
Your questions, answered. These are the questions Pinnacle's clinical teams hear most often from families navigating AAC refusal — answered with the same clinical accuracy that governs our 20M+ therapy sessions.
How long does it take for AAC refusal to resolve?
With systematic barrier identification and consistent intervention, most children show measurable engagement within 4–8 weeks. Full functional AAC use typically emerges at 8–16 weeks. Some cases with significant negative conditioning history take longer. There is no standard timeline — only the child's pace.
Should I take the device away completely and start over?
Sometimes a 1–2 week "holiday" from the device (while continuing with paper boards and modeling) allows negative associations to fade. But complete abandonment is rarely necessary. A pressure-free reintroduction is usually more effective than removal.
My child uses AAC at therapy but not at home. Why?
Generalization to new environments is a specific skill that must be taught. Ensure home vocabulary matches therapy vocabulary exactly. Ensure the home modeling approach matches the therapist's approach. Practice in the environment where generalization is desired.
Is AAC refusal my fault?
No. AAC refusal happens in families who are doing everything right — it indicates a mismatch between the system/approach and the child's profile that needs adjustment. It is information, not failure.
Will AAC stop my child from developing speech?
No. Research consistently shows AAC does not inhibit speech development. It typically supports it by reducing communication frustration and building language foundations. ASHA, WHO, and all major speech therapy bodies confirm this.
My child is 12 years old. Is it too late?
AAC success is documented across all ages. There is no developmental cut-off for AAC learning. Adults with complex communication needs successfully learn AAC. Begin now.
Which AAC app is best?
There is no universal answer. The best app is the one that matches this child's learning style, vocabulary needs, motor access profile, and sensory tolerance. Request an AAC assessment from an SLP for individualized recommendation.
My child's school refuses to support AAC. What do I do?
Contact Pinnacle's advocacy support at 9100 181 181. Every child with a diagnosed communication need has the right to AAC support in educational settings under Indian disability legislation (RPWD Act 2016).

Your Child Has Something to Say. These Materials Help You Hear It.
Every week of AAC refusal is a week of communication that doesn't happen. The barriers identified in this guide are addressable — most of them starting today, at zero cost. The vocabulary customization costs ₹0. The modeling costs ₹0. The pressure removal costs ₹0. Begin now.
Start Today — Free
Customize vocabulary with the child's specific interests. Begin modeling yourself. Remove all pressure. These three changes alone transform the trajectory.
Get Expert Guidance
Speak with a Pinnacle SLP about your child's specific AAC barrier. FREE teleconsultation available in 16+ languages, Monday through Saturday.
Visit a Center
In-person AAC assessment available at all 70+ Pinnacle centers across India. Comprehensive barrier evaluation and personalized implementation plan.
CIN: U74999TG2016PTC113063 | DPIIT: DIPP8651 | MSME | GSTIN: 36AAGCB9722P1Z2
Preview of 9 materials that help when child refuses aac Therapy Material
Below is a visual preview of 9 materials that help when child refuses aac therapy material. The pages shown help educators, therapists, and caregivers understand the structure and content of the resource before use. Materials should be used under appropriate professional guidance.






Link copied!

The Pinnacle Promise
"Built by Mothers. Engineered as a System."
Every technique on this platform represents the integrated knowledge of Pinnacle's Consortium: CRO scientists, pediatric Speech-Language Pathologists, Occupational Therapists, BCBA/ABA specialists, Special Educators, NeuroDevelopmental Pediatricians — and the tens of thousands of mothers and families whose children taught us what works. This page was built to the same clinical standards that govern 20M+ therapy sessions across 70+ centers. It is not an article. It is an intervention delivery system — designed to give your home the same clinical precision as a Pinnacle therapy room.
70+
Centers
Validated across India
20M+
Sessions
Therapy sessions delivered
97%+
Improvement
Measured improvement rate
70+
Countries
Reached globally
🏛️ Pinnacle Blooms Network® — India's Largest Autism Therapy Chain
📞 FREE National Autism Helpline: 9100 181 181 (16+ languages, 24×7) | 📧 care@pinnacleblooms.org | 🌐 pinnacleblooms.org
This content is educational. It does not replace assessment by a licensed speech-language pathologist specializing in AAC. AAC refusal requires professional evaluation to identify underlying causes. Individual results vary. Statistics represent aggregate outcomes across the Pinnacle Blooms Network. © 2025 Pinnacle Blooms Network®, unit of Bharath Healthcare Laboratories Pvt. Ltd. All rights reserved.
CIN: U74999TG2016PTC113063 • DPIIT: DIPP8651 (Govt. of India) • MSME: TS20F0009606 • GSTIN: 36AAGCB9722P1Z2
CIN: U74999TG2016PTC113063 • DPIIT: DIPP8651 (Govt. of India) • MSME: TS20F0009606 • GSTIN: 36AAGCB9722P1Z2