

"This is a wiring difference, not a behaviour choice. You cannot discipline your child out of light sensitivity any more than you can discipline someone out of needing prescription glasses."

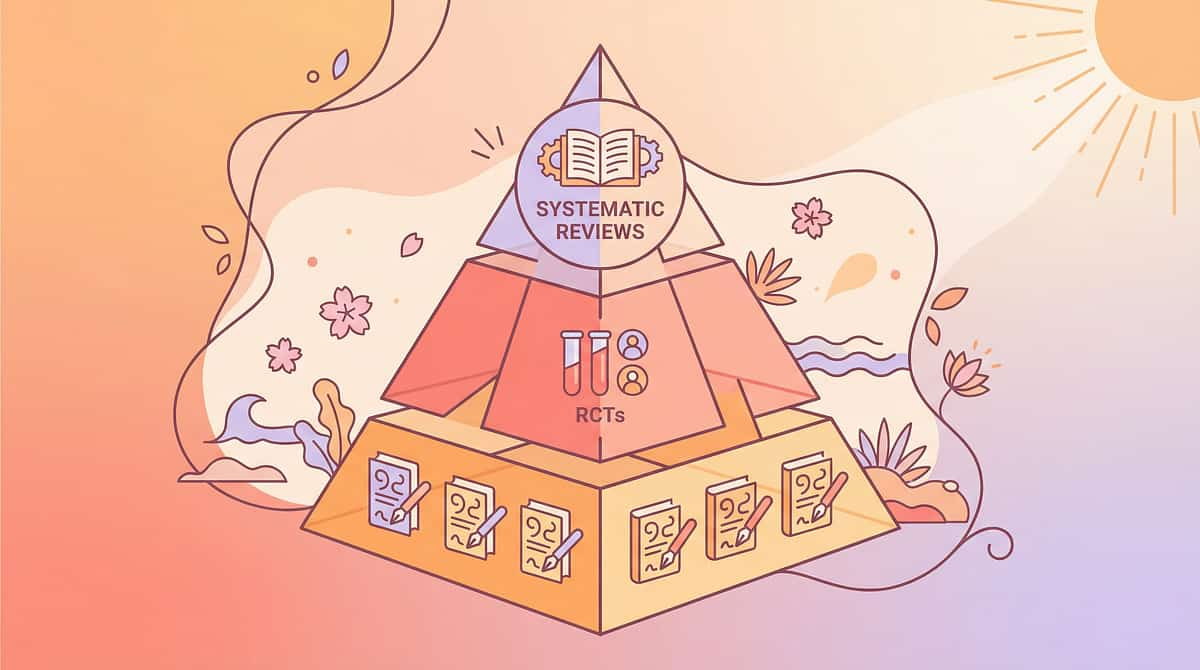
"Clinically validated. Home-applicable. Parent-proven. This protocol is backed by the highest available level of evidence in paediatric sensory intervention."










- Therapeutic Glasses: FL-41 tinted lenses with wrap-around frame — ₹1,500–8,000
- Smart Dimmer + Bulbs: App-controlled warm LED — ₹500–5,000
- Blackout Curtains: Dual-layer blackout + filtering shade — ₹1,000–10,000
- Low-Flicker LED: High-quality driver LED — ₹300–3,000
- Sensory Tent: Pop-up light-blocking fabric tent — ₹1,000–5,000
- Wide-Brim Hat: CoolShef Baby Sun Hat — ₹452
- Screen Filter: Physical blue-light filter panel — ₹200–2,000
- UPF Clothing: UPF-rated long sleeves — ₹800–4,000
- Visual Comfort Kit: Pre-assembled portable kit — ₹1,000–5,000
- Glasses: Any sunglasses from local market (₹50–200). Clip-on tinted sheets over regular frames.
- Dimmer: Lower-wattage bulbs. Dupatta draped over lamp shade. Desk lamp pointed at wall for bounce lighting.
- Window Treatment: Two dark bedsheets over windows on clips. Dark chart paper taped to glass — ₹10–20.
- Low-Flicker: Switch off all fluorescent tubes. Use incandescent bulbs or supervised candles/diyas. Cost: ₹0.
- Sensory Tent: Bedsheet draped over a table. Large cardboard box. Closet with pillow and blanket. Cost: ₹0.
- Hat: Any dupatta, towel, or handkerchief draped over the head. Newspaper folded into wide brim. Cost: ₹0.
- Screen Filter: Enable Night Mode / Eye Comfort on any device (free built-in setting). Cost: ₹0.
- Protective Clothing: Any long-sleeved cotton shirt + wide-brim hat for outdoor activities. Cost: ₹0.
- Comfort Kit: Sunglasses + handkerchief for eye covering in a ziplock bag in the school bag. Cost: ₹0–50.
- Sudden onset photophobia (not previously present) — may indicate migraine, meningitis, raised intracranial pressure, or retinal pathology. Seek immediate medical evaluation.
- Photophobia accompanied by eye pain, redness, tearing, or discharge — possible ophthalmological emergency.
- Photophobia following head injury or concussion — requires neurological assessment first.
- Child under 2 years — requires developmental paediatric ophthalmology evaluation before home accommodation.
- Do NOT create complete darkness — always maintain 10–50 lux minimum.
- Supervise candle/diya use at all times.
- Screen time limits still apply — screen filters do not override AAP/IAP guidelines.
- Tinted glasses should not be worn during sleep.
- Child has no acute eye condition or recent sudden onset photophobia.
- At least one professional consulted (OT, paediatrician, or ophthalmologist).
- Materials age-appropriate (no small parts for under-3s, no breakable glass lenses).
- Environment checked for tripping hazards in dim lighting.
- Install blackout curtains on ALL windows (dual-layer if east/west facing)
- Replace overhead light with dimmer switch OR desk lamp (2700K, 15–25W equivalent)
- Create a "dim corner" — sensory tent with indirect lighting only
- Remove or cover any standby LED lights on devices
- Night light: amber/red only — no blue/white (disrupts melatonin)
- Replace fluorescent tube lights with warm LED bulbs (2700K) on dimmer circuit
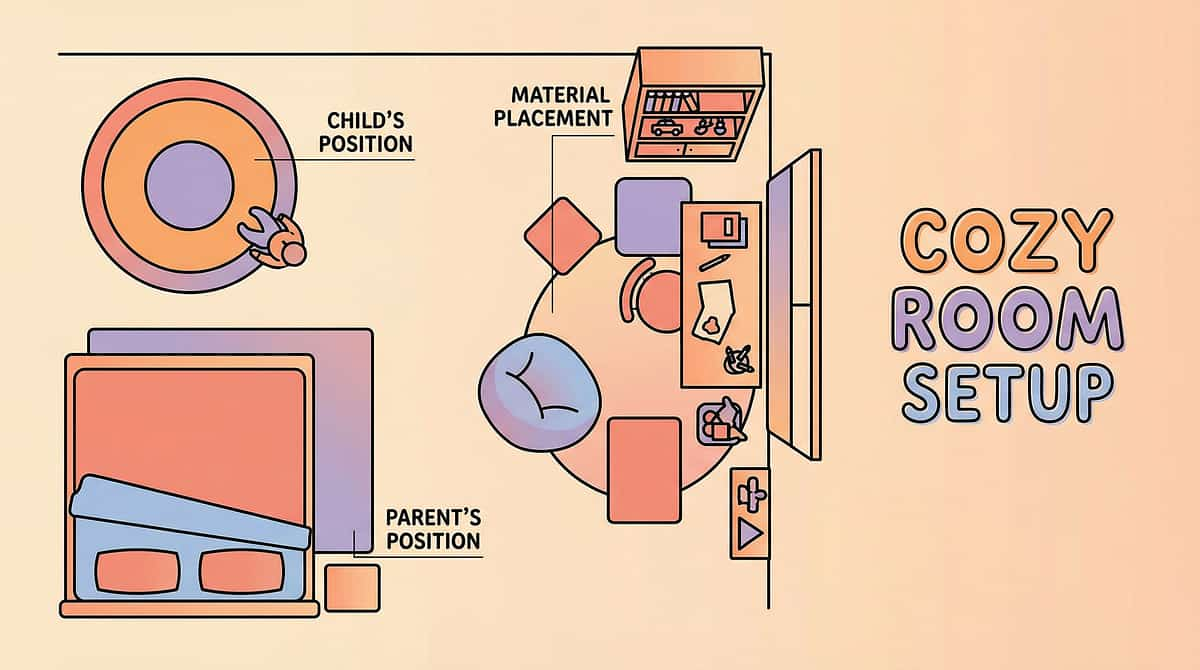
- Designate one corner as a "retreat zone" — floor cushion + overhead fabric drape
- Position TV/tablet viewing area away from direct window glare
- Install window film or sheer curtain on brightest window
- Use under-cabinet warm-tone LED strips instead of overhead fluorescent
- If overhead light is only option: reduce wattage and add a dimmer
- Position child's dining chair with back to the brightest light source
- Replace overhead fluorescent with warm-tone vanity light or battery-operated LED strip (2700K)
- Keep light-filtering glasses hanging by the bathroom door for morning routine
- Visual comfort kit in school bag (glasses + hat + cloth for eye cover)
- Teacher communication card: "I need to sit away from the window" / "I may wear tinted glasses"
- Car: window shade on child's side, sunglasses accessible in seat-back pocket


- Ideal: Child engages and moves toward activity
- Acceptable: Child watches but doesn't participate yet (observation IS participation)
- Concerning: Child becomes distressed → return to their current comfort zone, try again tomorrow


- ❌ Introducing multiple materials simultaneously
- ❌ Moving to a bright space immediately after child accepts glasses
- ❌ Forcing glasses onto the child's face
- ❌ Expressing disappointment if child rejects the material
- Ideal: Child tries glasses, keeps them on 30+ seconds, continues playing
- Acceptable: Child picks up glasses, examines them, puts them down — exploration, not rejection
- Concerning: Child throws glasses, becomes distressed → remove, return to engagement activity, try a hat next session


- Use only ONE material per week
- Stay exclusively in the child's preferred dim space — no brightness challenges
- Session duration: 5 minutes maximum
- Use only DIY materials (less novelty stress)
- Focus entirely on engagement bridge activities with accommodation materials passively present
- Combine materials: glasses + hat for outdoor excursion
- Introduce graduated brightness challenges: dim room → partially lit → briefly in bright room with tools
- Extend sessions to 20–30 minutes
- Add community exposure: wearing glasses in a market, temple, or school corridor
- Begin self-advocacy language: "The light is too bright for me. Can we dim it?"
- Child allows accommodation materials to be present in their space (even if unused)
- Reduced meltdown intensity (not frequency yet) during lighting transitions
- Child begins to associate dim space with comfort — voluntarily goes there when overwhelmed
- Parent identifies 2–3 specific light triggers (e.g., "the bathroom fluorescent" or "sunlight through the kitchen window at 4 PM")
"If your child's eyes are 3 seconds more comfortable today than last week — that's real neural change happening."
"You may notice you're more confident too. The morning bathroom routine isn't a battle anymore. The car rides have fewer tears. That's your progress — not just your child's."
"MASTERY UNLOCKED: Your child is not cured of light sensitivity. Your child is equipped to manage it. That distinction is the entire intervention." Source: PMC10955541 | BACB mastery criteria standards

"From screaming in the bathroom to choosing her own glasses before school. That's not a small thing. That's everything."
Related Techniques in Domain A — Visual Sensory Processing
Related Techniques These techniques sit within the Visual Sensory Processing subcategory of Domain A — Sensory Processing, encompassing 70+ techniques across the visual system alone. Where a technique is marked ✓, you already have the materials from this protocol. A-057: Child Squints at Lights Introductory | Canon: Sunglasses / Light Filtering Glasses You already own materials for this technique ✓ A-069: Child Covers Eyes in Bright Rooms Introductory | Canon: Blackout / Light Control You already own materials for this technique ✓ A-071: Graduated Light Exposure Protocol Core | Canon: Sunglasses + Adjustable Lighting Next step after A-070 mastery A-072: Community Light Navigation Skills Advanced | Canon: Visual Comfort Kit Next step after A-070 mastery A-075: Blue Light Management Protocol Introductory | Canon: Screen Filters You already own materials for this technique ✓ A-068: Sensory Diet for Visual System Core | Canon: Multiple Visual Tools Broader visual regulation — complements A-070 Browse Full Visual Sensory Domain
"She's not cured. She's equipped. That's the difference."
"Light sensitivity accommodation is not about reducing demands. It is about removing a neurological barrier so the child can ACCESS the demands. When we removed the visual overload, this child's true cognitive and social potential became visible for the first time." — Pinnacle OT, Hyderabad Centre

- Primary: Paediatric Occupational Therapist (Sensory Integration Certified)
- Secondary: BCBA / ABA Therapist (for behavioural patterns around light avoidance)
24x7 | 16+ Languages | No appointment needed
"Your data helps every child like yours. When 10,000 families report that warm-tone 2700K bulbs work better than cool-tone 4000K — that evidence becomes a recommendation for the next family."
- How to select the right tinted glasses for your child's face shape and sensitivity level
- How to set up a dimmer switch (60-second installation)
- How to create a sensory tent retreat from household items
- How to pack a visual comfort kit for school


© 2025 Pinnacle Blooms Network®, unit of Bharath Healthcare Laboratories Pvt. Ltd. All rights reserved. CIN: U74999TG2016PTC113063