
Bath Time = Scream Time. Every. Single. Night.
It starts the moment you turn on the faucet. She backs into the corner, hands shielding her face, screaming before a single drop touches her skin. You stand there holding the washcloth, exhausted, wondering what you're doing wrong. The neighbors can hear her. Your mother-in-law says she's "just being dramatic." But you see her face. That terror is real.
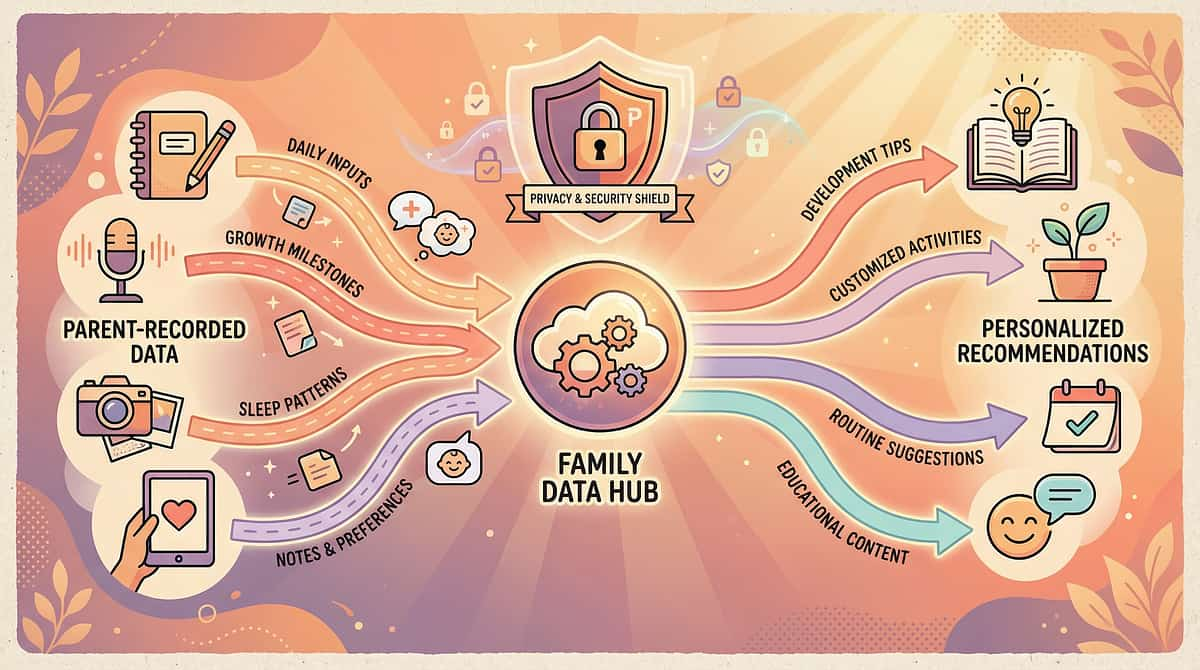
9 clinically validated materials exist that transform face washing from a nightly war zone into a manageable, even independent, self-care skill.
You are not failing. Your child's nervous system is speaking. The face contains one of the highest densities of sensory receptors in the human body — and your child's brain is amplifying every signal. This is neurology, not defiance.
Pinnacle Blooms Consortium
Sensory Solutions Series, Episode 15
Tactile-Facial Processing | Water & Touch Sensitivity | Domain Code: SEN-TAC-FAC | Age Band: 18 months – 10 years

You Are Among Millions.
You Are Not Alone: The Numbers
80%
Sensory Difficulties
Of children diagnosed with autism spectrum disorder display sensory processing difficulties, per PRISMA systematic review of 16 studies (2013–2023).
60-70%
Facial Sensitivity
Of children with sensory processing challenges experience specific facial tactile hypersensitivity, impacting daily hygiene, medical care, and social participation.
1 in 4
Families in India
Navigating autism in India report bath time and hygiene routines as a top-3 daily stressor, per Pinnacle clinical intake data across 70+ centers.
"You are among millions of families worldwide navigating this exact challenge. This is not rare. This is not unusual. And it is absolutely addressable."
Research Evidence: PRISMA systematic review (2024): 80% sensory processing prevalence in ASD. Meta-analysis: Sensory integration therapy effectively promotes social skills, adaptive behavior, sensory processing, and motor skills (World J Clin Cases, 2024). References: PMC11506176 | PMC10955541 | DOI: 10.12998/wjcc.v12.i7.1260

The Science Behind the Struggle
Why Water Feels Like an Attack
Your child's face contains among the highest density of sensory nerve endings in the entire human body. In the brain's sensory map — called the somatosensory homunculus — the face and lips are represented as enormous, because the brain dedicates massive processing power to facial sensations.
In children with facial tactile hypersensitivity, these receptors have lower activation thresholds. Sensations that feel neutral or even pleasant to you — water droplets, washcloth texture, rubbing motions — register as intense, unpredictable, or genuinely threatening in your child's brain.
This triggers the fight-flight-freeze response. Your child is not choosing to scream. Their autonomic nervous system is activating a survival response to what it perceives as an assault.
Key Insight: "This is a wiring difference, not a behavior choice. Your child's brain processes facial touch differently — and that difference has a name, a mechanism, and a solution pathway."
Research Evidence: Frontiers in Integrative Neuroscience (2020): Comprehensive framework for evaluating sensory integration/sensory processing treatment in ASD. References: DOI: 10.3389/fnint.2020.556660
Developmental Context
Your Child Is Here. Here Is Where We're Heading.
0–6 Months
Facial touch tolerance emerges through caregiver bonding and skin-to-skin contact.
6–12 Months
Water play exploration begins; some aversion is typical and developmentally appropriate.
12–24 Months
Face washing introduced in hygiene routines; sensitivity may first appear during this period.
18 Months – 5 Years ⭐
INTERVENTION WINDOW — Facial tactile desensitization is most responsive to structured intervention during this critical period.
5–10 Years
Self-care independence target — child should be progressing toward independent face washing.
10+ Years
Social implications increase — hygiene independence becomes critical for peer acceptance and self-esteem.
What commonly co-occurs: Toothbrushing meltdowns (A-016), haircut terror (A-017), nail cutting resistance (A-018), hair brushing aversion (A-019). These share the same neurological root — facial and cranial tactile hypersensitivity.
Research Evidence: WHO Care for Child Development (CCD) Package: Age-specific evidence-based recommendations for caregivers. Implemented in 54 low- and middle-income countries. UNICEF MICS indicators for developmental monitoring across 197 countries. References: PMC9978394 | WHO/UNICEF CCD Package (2023)
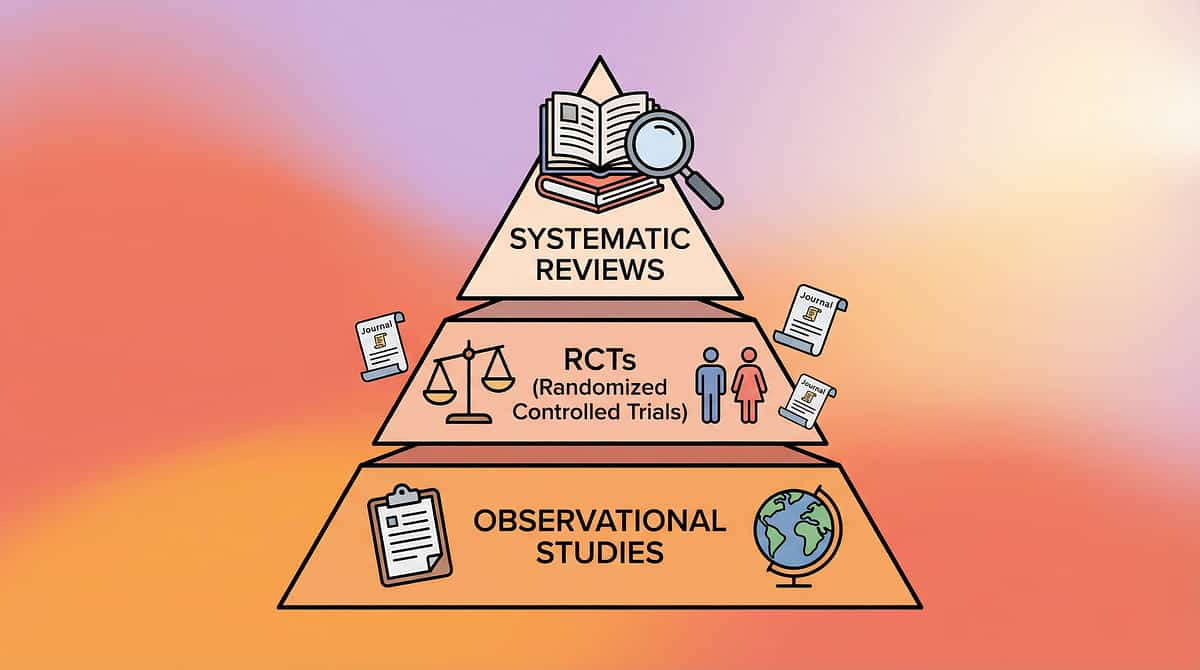
Evidence Grade: Level I–II
Clinically Validated. Home-Applicable. Parent-Proven.
1
PRISMA 2024
16 articles from 2013–2023 confirm sensory integration intervention meets criteria as evidence-based practice for children with ASD.
2
Meta-Analysis (24 Studies)
Sensory integration therapy effectively promotes adaptive behavior, sensory processing, and daily living skills (World J Clin Cases, 2024).
3
Indian RCT
Padmanabha et al. (2019): Home-based sensory interventions demonstrated significant outcomes in an Indian pediatric population — validating home execution feasibility.
4
SPD Foundation
Facial tactile desensitization using graded exposure, deep pressure, and environmental modification has established clinical consensus across OT practice.
5
NCAEP 2020
Visual supports (social stories, visual schedules) classified as evidence-based practice for autism.
References: PMC11506176 | PMC10955541 | DOI: 10.1007/s12098-018-2747-4 (Padmanabha et al., Indian J Pediatr, 2019) | NCAEP Evidence-Based Practices Report (2020) | SPD Foundation Clinical Guidelines
Confidence Meter
8.5 / 10 — Strong evidence base with multiple systematic reviews, meta-analyses, and home-based RCTs supporting the component interventions.

Act II: Knowledge Transfer
The Technique
Facial Tactile Desensitization Through Graded Material Exposure
Parent-Friendly Alias:"9 Materials That Help When Your Child Hates Face Washing"
A structured, two-track intervention combining: (1) playful facial touch desensitization outside hygiene contexts using massage tools, water play, and child-controlled spray bottles, and (2) modified hygiene routines using texture-graded washcloths, bath visors, temperature control, visual timers, mirrors for self-washing, and visual schedules — all designed to reduce facial tactile threat response and build toward independent face washing over 8–16+ weeks.
Domain
Sensory Processing — Tactile-Facial (Domain A)
Age Range
18 months – 10 years
Session Duration
5–10 min desensitization + hygiene routine
Frequency
Daily desensitization play + every hygiene occasion
Tactile Sensory Kit
Visual Supports
Self-Care Adaptation Tools
Setting: Home — bathroom, living room, outdoor play area

Who Uses This Technique
This technique crosses therapy boundaries — because the brain doesn't organize by therapy type.
Primary: Occupational Therapy (SI)
The OT designs the sensory desensitization hierarchy, selects tactile gradient materials, establishes the deep pressure protocol, and monitors sensory processing changes through standardized tools like the Sensory Profile 2.
Secondary: Applied Behavior Analysis
The BCBA structures the reinforcement schedule, designs the visual schedule for routine predictability, establishes data collection protocols (tracking tolerance duration, distress level), and implements systematic desensitization through operant principles.
Supporting: Speech-Language Pathology
The SLP addresses the oral motor component — many children with facial tactile sensitivity also have oral defensiveness affecting toothbrushing, dental visits, and food textures around the mouth area.
Supporting: Special Education
The Special Educator integrates self-care skill development into the child's educational plan, ensuring face washing independence is tracked as an Adaptive Living Skills goal with generalization across settings.
Supporting: NeuroDev Pediatrician
Rules out differential diagnoses (skin conditions, prior trauma, oral motor dysfunction, vision concerns), adjusts medication if anxiety component is significant, and monitors overall sensory processing trajectory.
Research Evidence: Adapted UNICEF/WHO Nurturing Care Framework for SLPs (2022). References: DOI: 10.1080/17549507.2022.2141327

Precision Targeting
This Isn't a Random Activity. It's a Precision Tool.
Observable Behavior Indicators
Tolerates wet washcloth on forehead for 10+ seconds without distress
Allows water from spray bottle on cheeks, self-directed
Completes face washing routine within visual timer duration
Initiates self-washing with mirror and preferred washcloth
Research Evidence: Meta-analysis (World J Clin Cases, 2024): Sensory integration therapy effectively promoted social skills, adaptive behavior, sensory processing, and motor skills across 24 studies. References: PMC10955541

Material 1 of 9
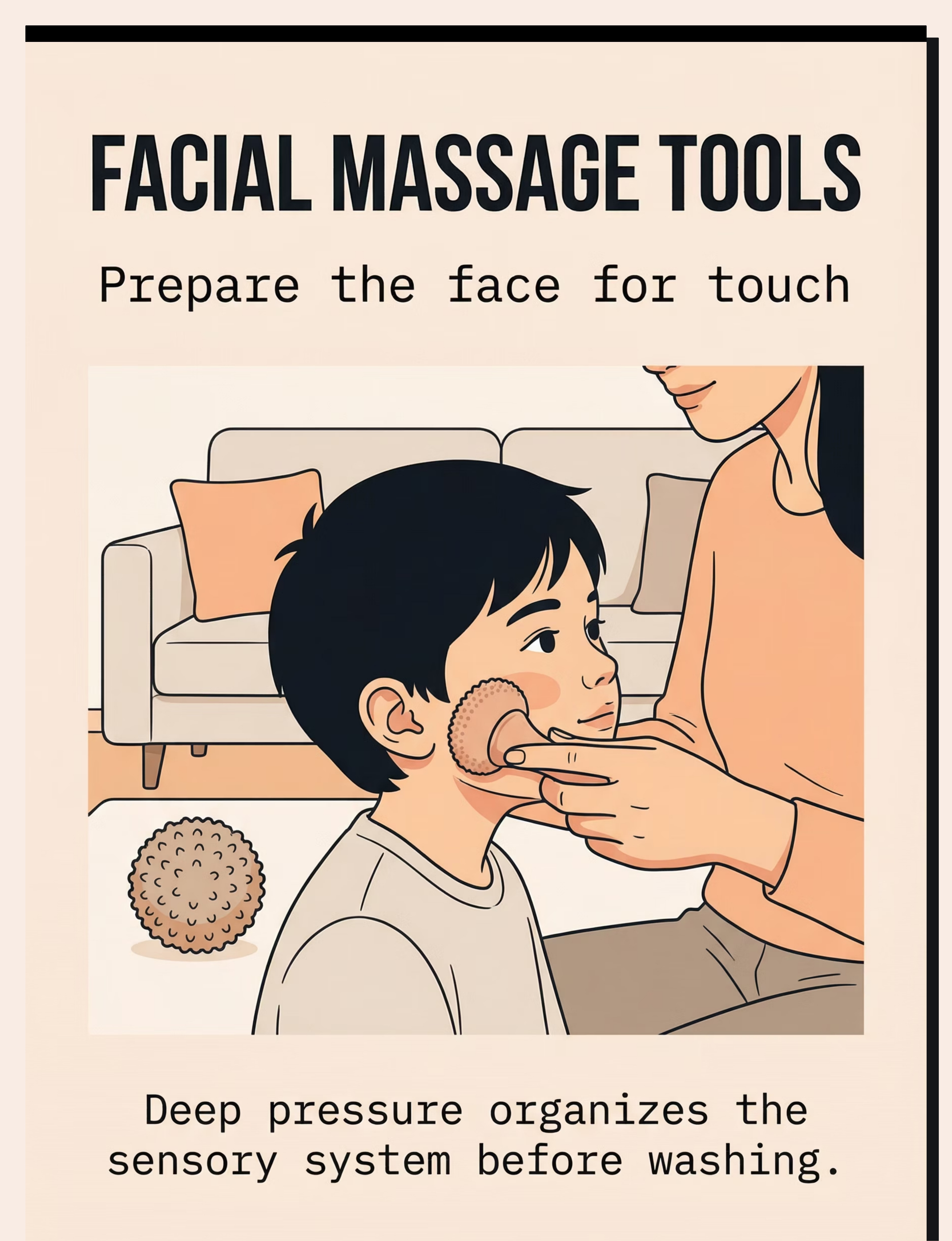
Facial Massage Tools (Soft Rollers / Textured Balls)
Canon Category: Tactile Sensory Kit
Price: ₹200–600
Facial massage tools are the cornerstone of the desensitization play track. These tools provide controlled, deep pressure input to the face — the type of sensory input that organizes the nervous system rather than triggering a defensive response.
Items included:
- Soft silicone facial roller — smooth, firm, predictable input
- Textured sensory balls (soft) — varied tactile patterns for gradual exposure
- Facial massage wand — allows parent to control pressure precisely
Start by modeling on your own face, then offer the child's arm before progressing toward facial zones. The child should always see the tool approaching — never surprise contact.
Pinnacle Recommends

Material 2 of 9
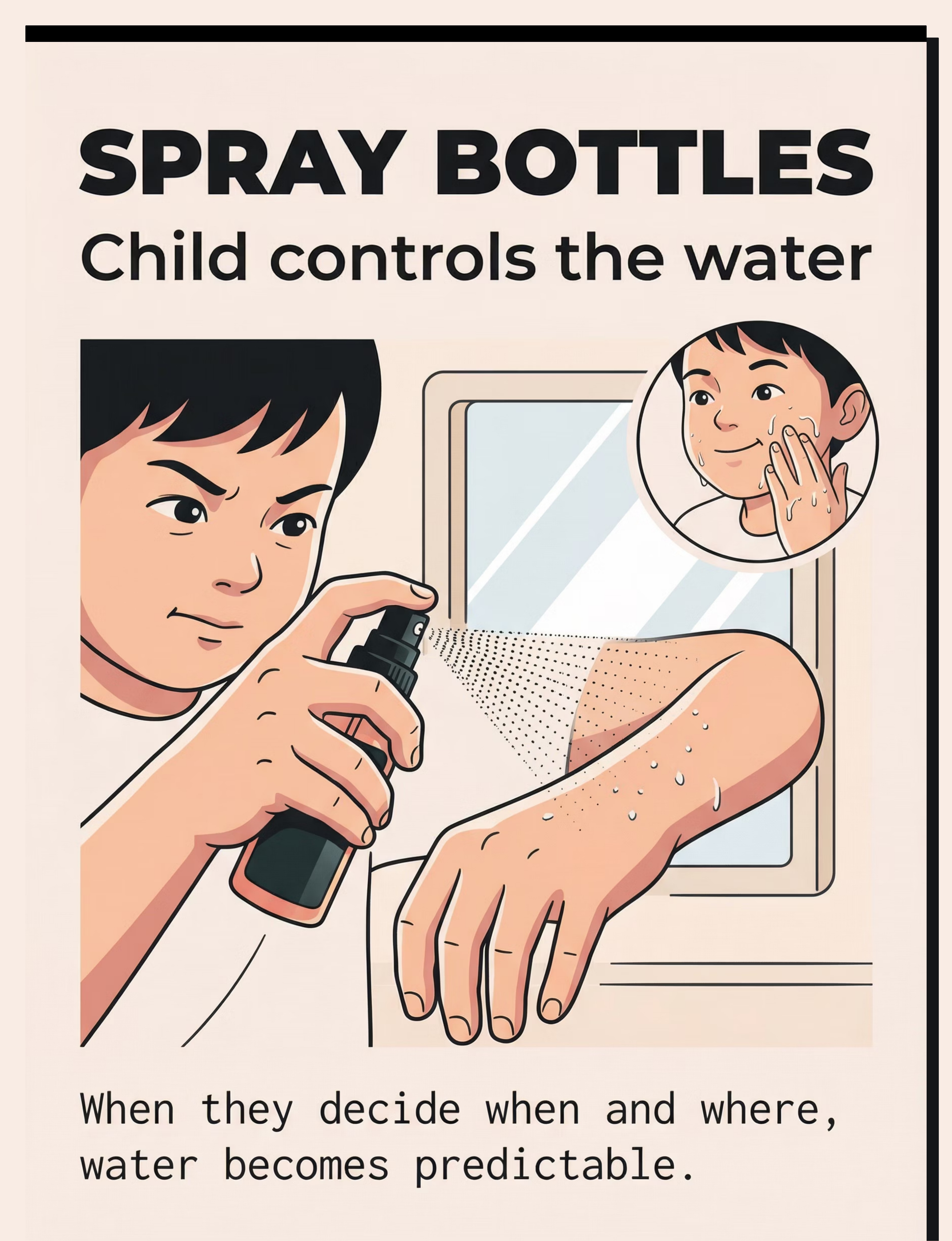
Spray Bottles (Child-Controlled Misting)

Canon Category: Self-Care Adaptation Tools
Price: ₹50–200
The spray bottle is arguably the most transformative single material in this toolkit. Its power lies in one principle: child control. When the child holds the spray bottle, they decide when, where, and how much water touches their face. This converts an unpredictable threat into a manageable, self-directed experience.
Items included:
- Small spray bottle with fine mist setting
- Adjustable nozzle for controlling spray intensity
- Child-sized grip for independent use
Let the child decorate the bottle — making it "thirs" increases willingness to engage. Begin with spraying hands and arms before ever approaching the face.

Material 3 of 9
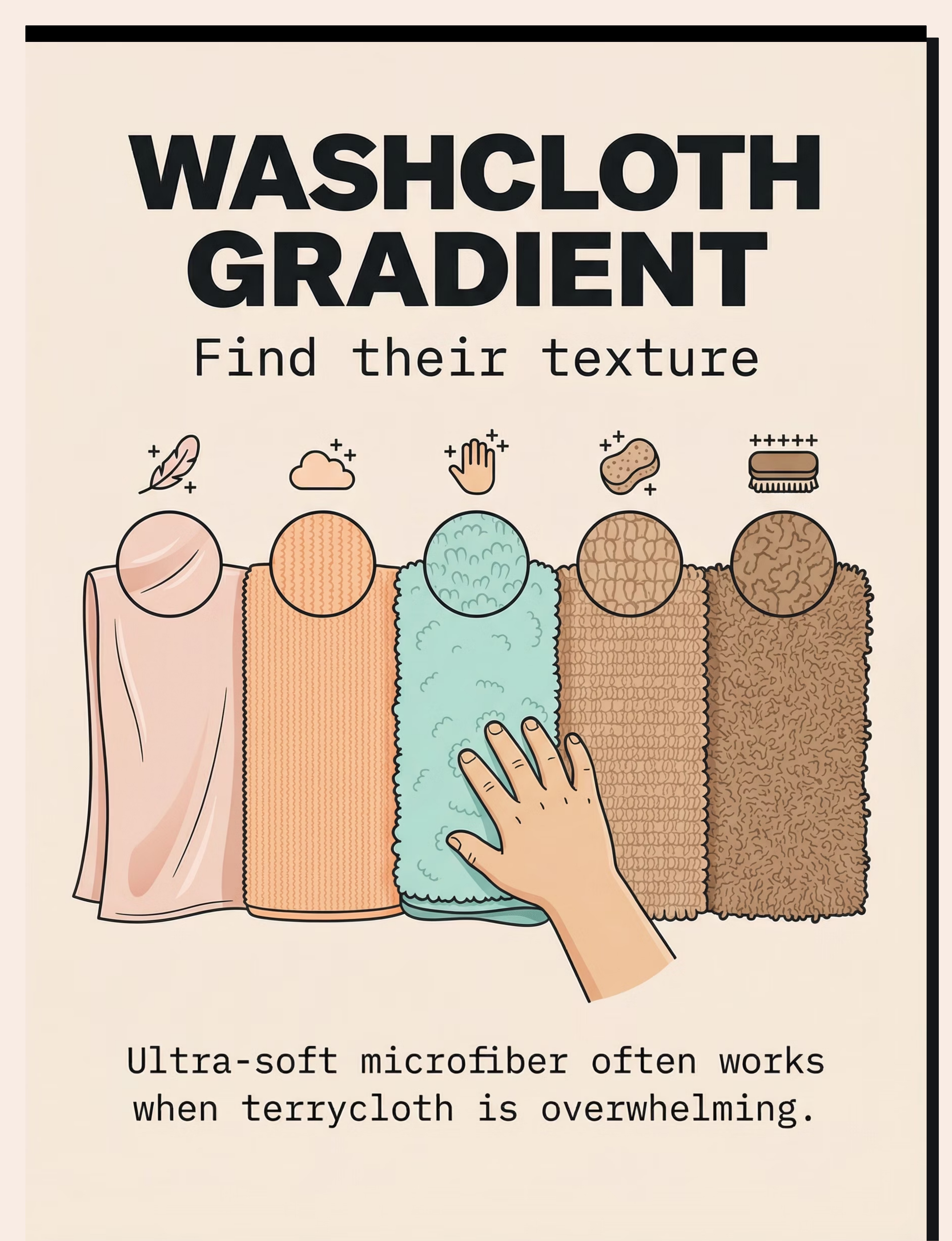
Washcloth Texture Gradient Kit
Canon Category: Tactile Sensory Kit
Price: ₹300–800 for variety pack
Not all washcloths are created equal — and for a child with facial tactile sensitivity, the texture difference between silk and terrycloth is the difference between tolerable and terrifying. This kit provides a gradient from the smoothest possible fabric to standard bath-time textures, allowing you to start where your child can succeed and progress gradually.
Texture gradient (smoothest to roughest):
- Silk/satin cloth — ultra-smooth, minimal tactile input
- Microfiber facial cloths — soft with slight texture
- Bamboo washcloths — gentle, naturally antibacterial
- Soft cotton — standard gentle option
- Regular terrycloth — the long-term goal texture
Let your child touch all options and choose their starting texture. Even if they pick silk — that's the starting point, not a failure. Progress happens one texture at a time.

Material 4 of 9
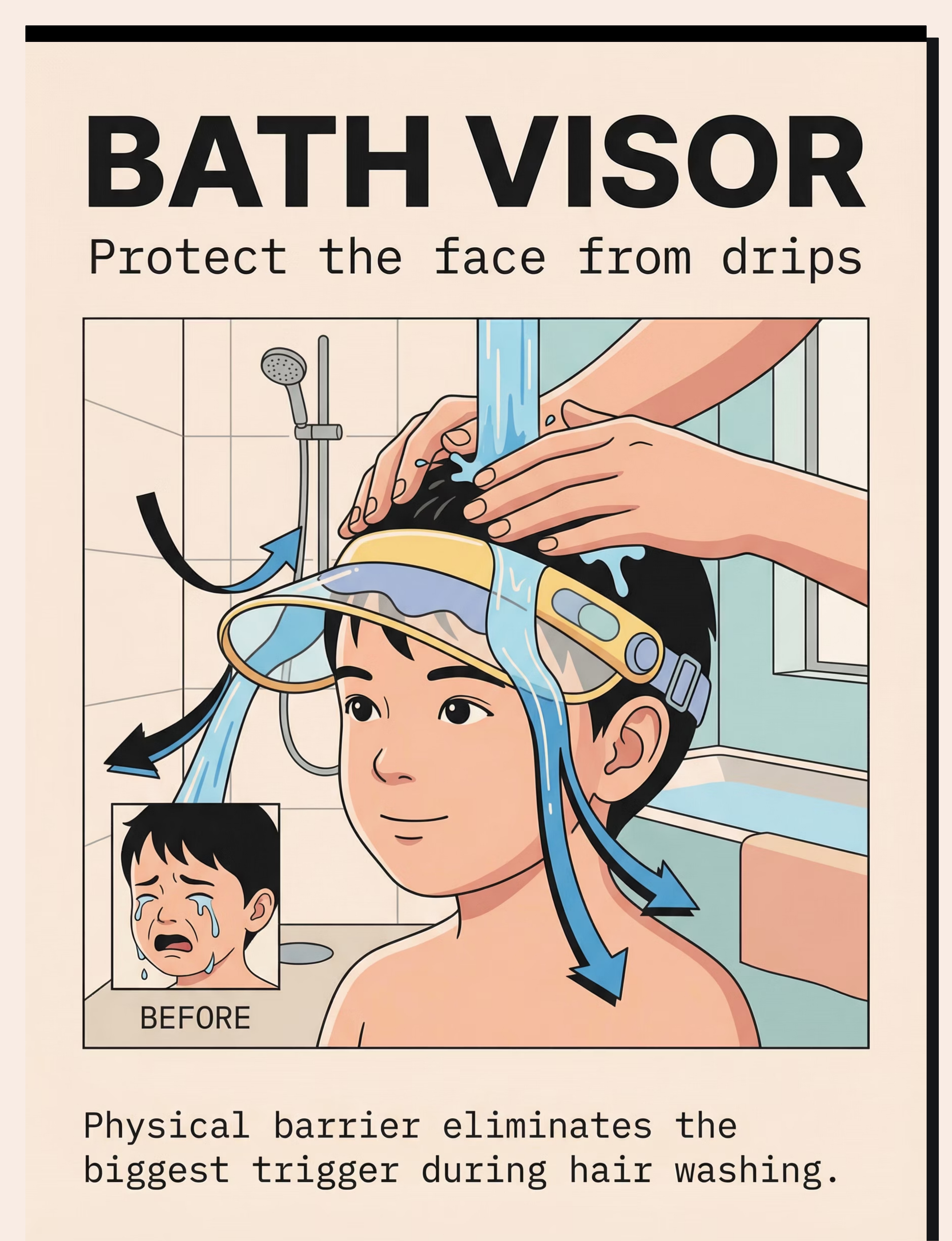
Bath Visor / Shampoo Shield

Canon Category: Self-Care Adaptation Tools
Price: ₹150–400
The bath visor serves as a physical boundary that protects the face during hair washing — one of the most common triggers for face-water meltdowns. For many children, the fear of face washing is actually the fear of water running down from their hair into their eyes, nose, and mouth during rinse time.
Items included:
- Adjustable bath visor — fits snugly around forehead
- Shampoo shield (halo style) — wider brim coverage
- Soft silicone brim visor — flexible, comfortable, non-threatening
The visor is a bridge tool, not a permanent solution. Most children use it for 6–10 weeks before their facial tolerance has developed enough to wash without it. Let the child handle and wear the visor before bath time so it becomes familiar and safe.

Material 5 of 9
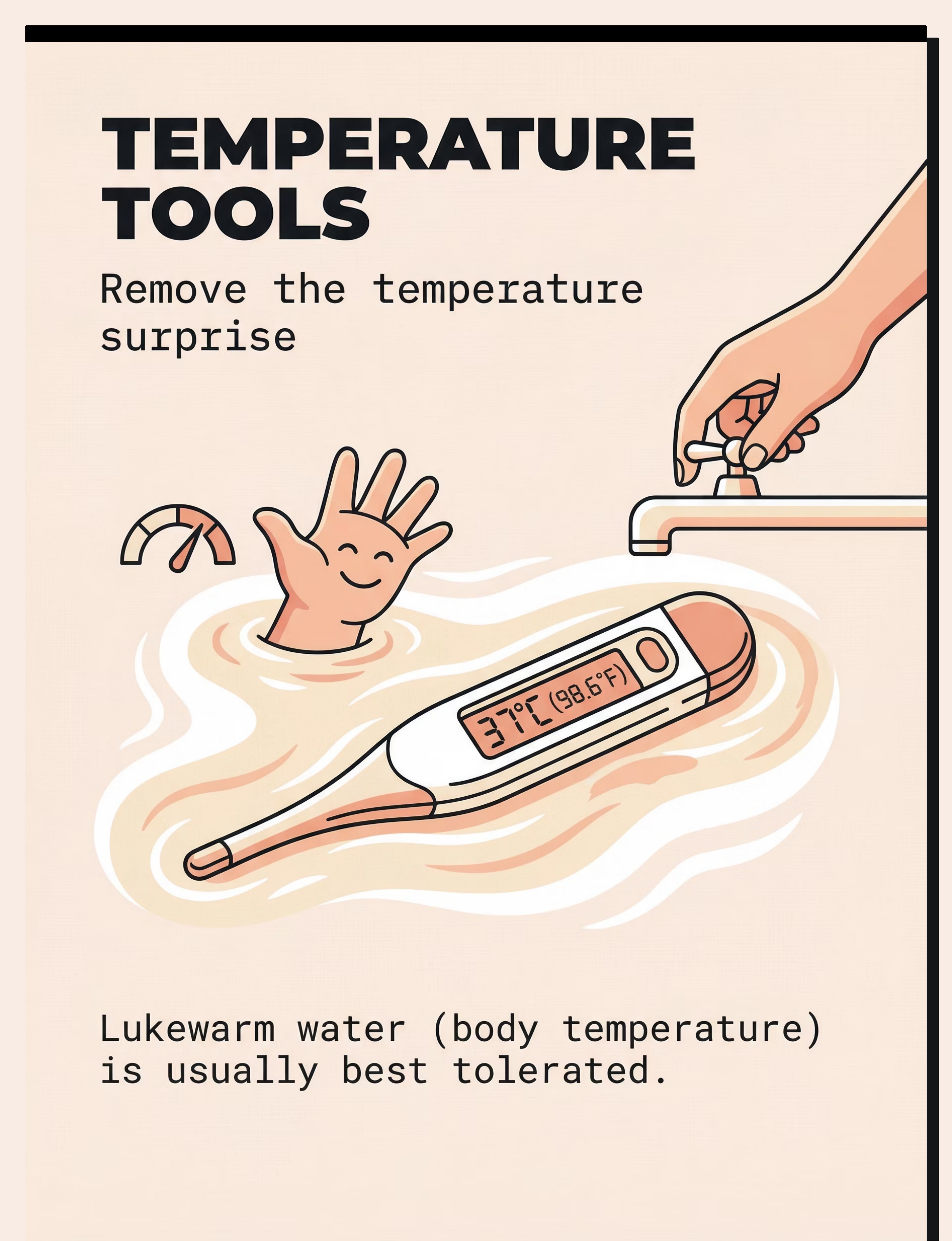
Water Temperature Control Tools
Canon Category: Self-Care Adaptation Tools
Price: ₹300–900
Temperature unpredictability is a hidden amplifier of facial tactile distress. When your child doesn't know whether the water will be hot, cold, or lukewarm, their nervous system stays on high alert — adding thermal uncertainty to an already overwhelming tactile experience.
The target temperature is 37°C (body temperature) — warm enough to be comfortable, not hot enough to startle, and never cold. Consistency is key: the same temperature every single time reduces one variable your child's brain must process.
Items included:
- Digital bath thermometer — precise, easy-to-read display
- Floating temperature indicator — visual color change for child understanding
Announce the temperature verbally each time: "Water is warm-warm today" — using the same words creates predictability that calms the threat response.

Material 6 of 9
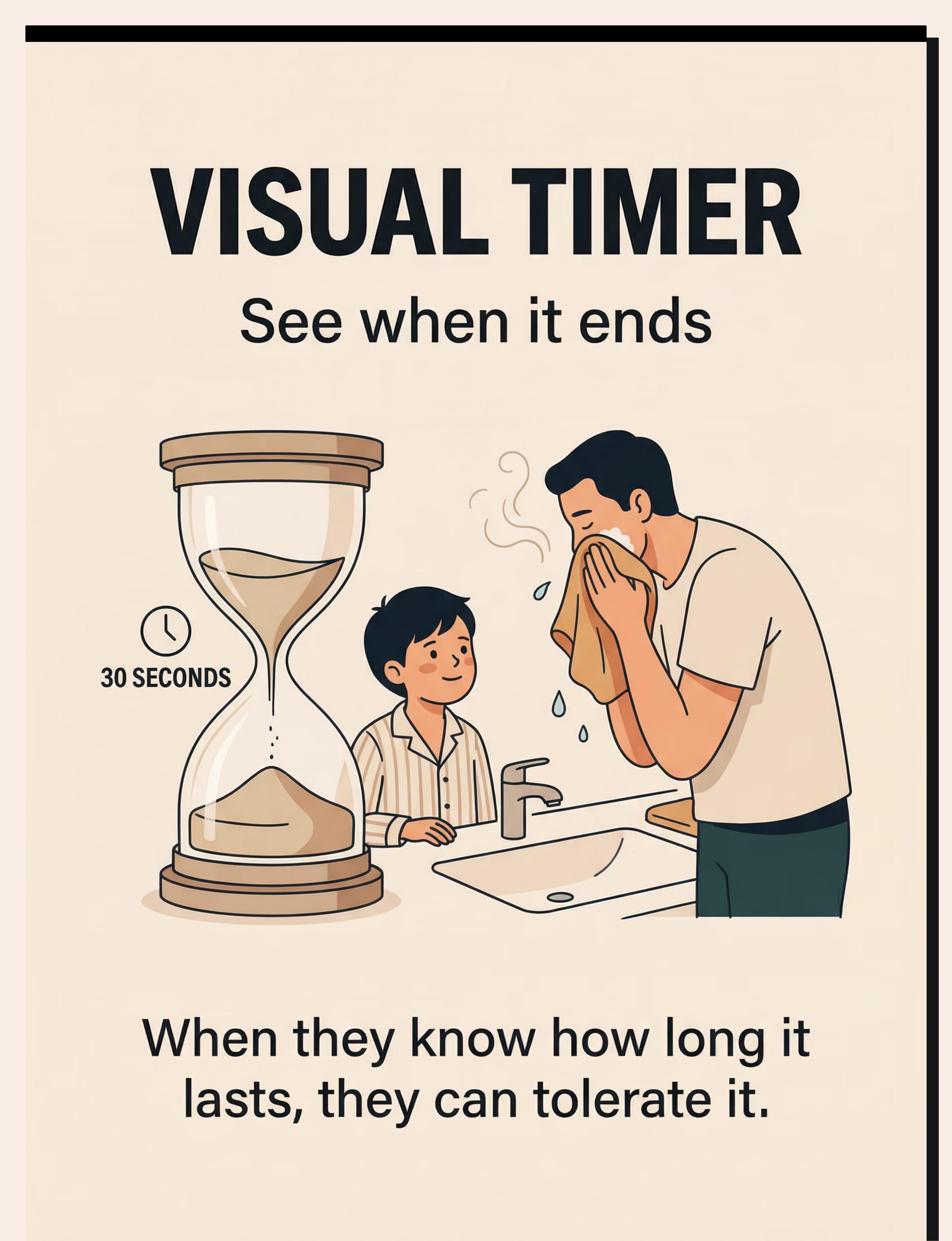
Visual Timer
Canon Category: Visual Supports
Price: ₹200–600
The visual timer answers the most anxiety-producing question in your child's mind: "When will this end?" Without a visible endpoint, the face washing experience feels infinite — and infinite discomfort triggers panic. The timer transforms an open-ended threat into a bounded, survivable event.
Items included:
- Sand timer (30 seconds or 1 minute) — visually concrete, no numbers needed
- Visual countdown timer — shrinking colored disk shows time remaining
- Time Timer (brand) — the gold standard in therapeutic visual timing
Critical rule: When the timer ends, you STOP. Even if the face isn't fully clean. Honoring the timer builds trust. Breaking the timer's promise destroys it. Your child needs to learn: "The timer protects me. When it's done, I'm done."

Material 7 of 9
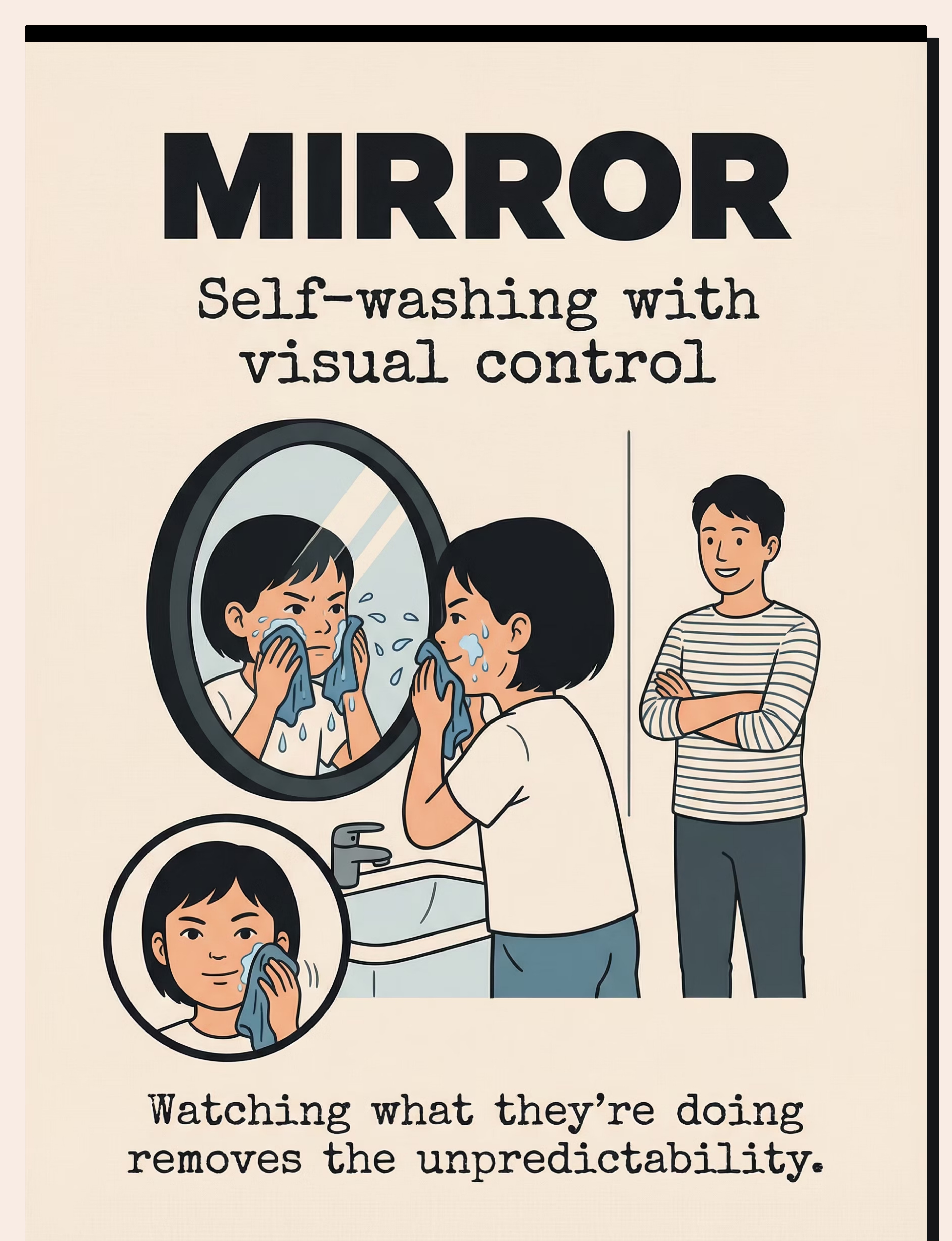
Child-Height Unbreakable Mirror
Canon Category: Self-Care Adaptation Tools
Price: ₹300–800
The mirror is your child's pathway to independence. Self-washing requires visual feedback — the child needs to see what they're doing, where the cloth is, and what's happening to their face. A mirror positioned at their eye level transforms face washing from something done to them into something they do themselves.
Items included:
- Child-height unbreakable mirror with secure wall mounting
- Good lighting positioned to illuminate face clearly
The mirror also serves a desensitization function: when children can see the washcloth approaching in the mirror, the contact becomes predictable rather than surprising. Many children who resist parent-led face washing will independently wipe their own face when watching in a mirror — because they control the movement and can see what's coming.
Pro tip: Use the mirror during desensitization play too — let the child watch themselves use the facial roller or spray bottle. Self-observation builds body awareness and reduces facial touch as a "foreign" experience.


Material 8 of 9
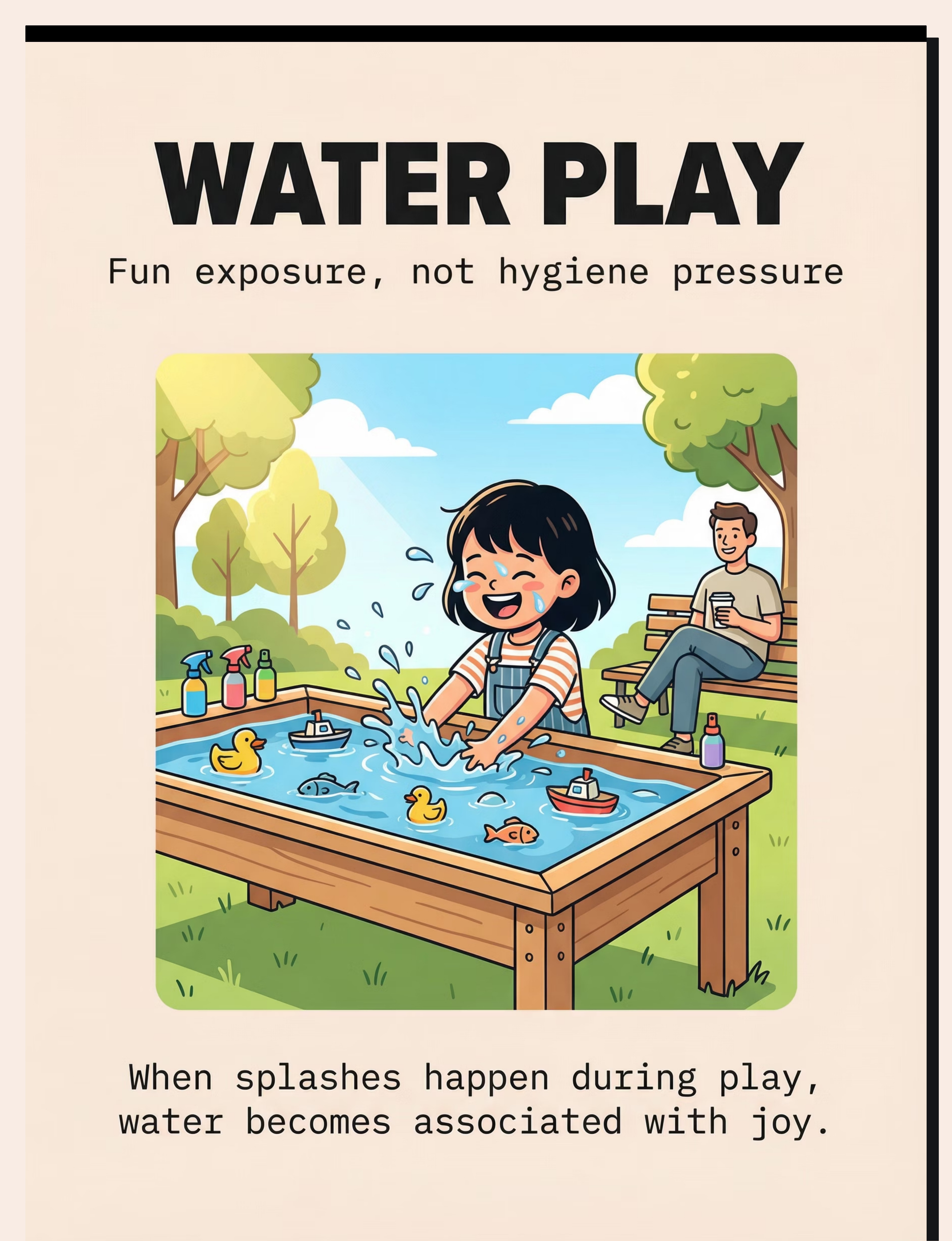
Water Play Materials

Canon Category: Sensory Play
Price: ₹500–1,500
Water play is where desensitization happens without the child even knowing it's therapy. By separating water exposure from the stressful hygiene context, you give your child's nervous system a chance to recalibrate its relationship with water on skin — including, eventually, the face.
Items included:
- Water table — child-height standing play with cups, funnels, toys
- Spray bottles for games — spraying targets, plants, each other
- Gentle sprinkler — walk-through water play outdoors
- Splash toys — rubber ducks, pouring cups, water wheels
The progression: hands in water → splashing arms → water on neck → mist near face → voluntary face splash. Never rush the face step. Some children spend weeks happily playing at the water table before a single drop touches their face — and that's exactly the right pace.

Material 9 of 9
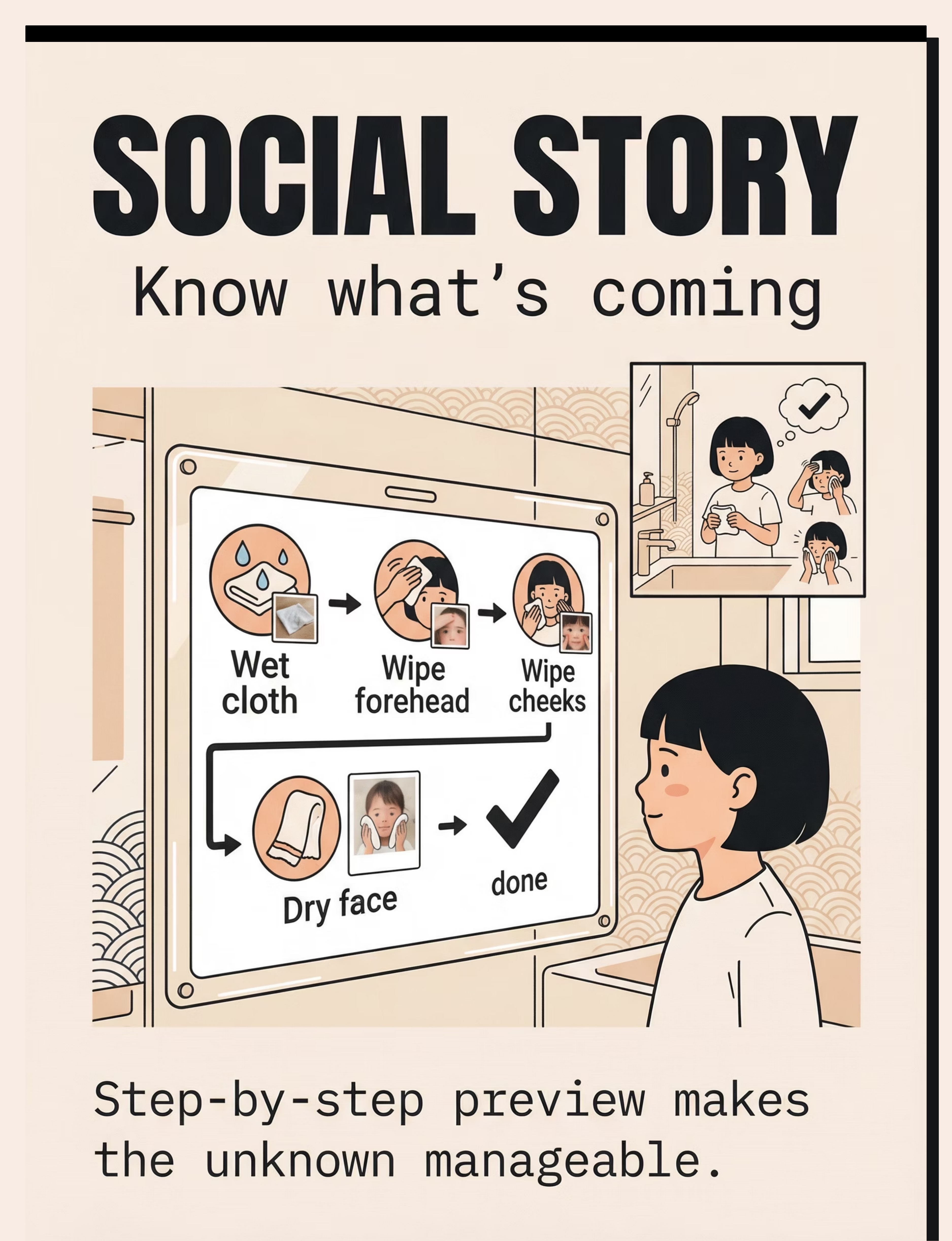
Face Washing Social Story + Visual Schedule
Canon Category: Visual Supports
Price: ₹100–400 (printable/DIY)
The social story and visual schedule are the cognitive scaffolding that make everything else work. While the other 8 materials address the sensory system, these address the predictability system — your child's need to know what's coming, in what order, and when it ends.
Items included:
- Laminated visual schedule — step-by-step picture sequence for the bathroom
- Child's own photos — pictures of YOUR child doing each step (most powerful)
- Display hook at child height — posted next to the sink
- Social story booklet — narrative format explaining why we wash faces and what happens
The visual schedule should show: wet cloth → forehead → cheeks → chin → dry → done! Read the social story at a calm time (not bath time), and review the visual schedule right before each hygiene session. NCAEP 2020 classifies visual supports as evidence-based practice for autism.


Your Complete Toolkit
Everything You Need — Priced and Ready
# | Material | Canon Category | Price Range | Priority | |
1 | Facial Massage Tools | Tactile Sensory Kit | ₹200–600 | ⭐ Core | |
2 | Spray Bottles | Self-Care Adaptation | ₹50–200 | ⭐ Core | |
3 | Washcloth Gradient Kit | Tactile Sensory Kit | ₹300–800 | ⭐ Core | |
4 | Bath Visor / Shampoo Shield | Self-Care Adaptation | ₹150–400 | Helpful | |
5 | Water Temperature Tools | Self-Care Adaptation | ₹300–900 | Helpful | |
6 | Visual Timer | Visual Supports | ₹200–600 | ⭐ Core | |
7 | Child-Height Mirror | Self-Care Adaptation | ₹300–800 | Helpful | |
8 | Water Play Materials | Sensory Play | ₹500–1,500 | Helpful | |
9 | Social Story + Visual Schedule | Visual Supports | ₹100–400 | ⭐ Core |
Total Investment
₹2,000–5,500 for comprehensive toolkit
Essential Starters
₹450–1,000: Spray bottle + Visual timer + Soft washcloth

Zero-Budget Alternatives
No Budget? No Delivery? Start Today With What You Have.
Buy This | Make This (Zero-Cost) | Why It Works | |
Facial massage roller | Parent's fingers with firm circular pressure; soft makeup sponge; smooth rubber ball from toy box | Same deep pressure input principle | |
Spray bottle with mist | Any clean spray bottle — decorate together. Adjust nozzle to finest mist | Child control is the mechanism, not the bottle | |
Washcloth gradient kit | Silk dupatta/scarf, microfiber cleaning cloth, old cotton T-shirt squares, regular towel | Same texture progression principle | |
Bath visor | Cut brim from old sun hat + elastic band. Or fold dry washcloth over forehead and eyes | Physical barrier = face protection | |
Bath thermometer | Test water on inner wrist. Verbal: "Water is warm-warm today" — same words every time | Predictability reduces threat response | |
Visual timer | Sand timer from board game, phone timer, or count down aloud: "10, 9, 8..." | Visible endpoint = bounded experience | |
Child-height mirror | Reposition existing mirror or use step stool for bathroom mirror | Visual feedback enables independence | |
Water play set | Basin/bucket outdoors, cups for pouring, homemade sprinkler from perforated bottle | Playful water exposure in non-hygiene context | |
Visual schedule | Photos of your child at each step, printed from phone, stuck on bathroom wall with tape | YOUR child's photos are most powerful |
Why the substitutes work: Same sensory and behavioral principles — deep pressure input, child control, predictability, graded texture exposure, visual structure. The clinical-grade material is preferred for precision; the DIY version gets you started today.
WHO/UNICEF Principle: "Context-specific, equity-focused interventions ensure every family, regardless of economic status, can execute evidence-based techniques." References: PMC9978394 | WHO NCF Handbook (2022)

🔴 Safety First: Before You Begin
🔴 RED LINE — STOP IMMEDIATELY IF:
- Child shows signs of skin pain, redness, or swelling on face (may indicate dermatitis, eczema — consult dermatologist before proceeding)
- Child displays extreme panic beyond typical sensory distress — hyperventilation, dissociation, freezing with dilated pupils (may indicate trauma response)
- Any sign of injury to face or eyes from materials
- Child is ill, feverish, or post-meltdown (heightened sensitivity)
🟡 CAUTION — MODIFY IF:
- Child is tired, hungry, or already dysregulated — postpone desensitization play; use minimal hygiene routine only
- Child tolerates body washing but panics specifically at face — this is typical; proceed with face-specific protocol
- Child has had a difficult day at school/therapy — reduce demands, shorter timer, preferred washcloth only
🟢 GREEN — PROCEED WHEN:
- Child is fed, rested, and in a generally calm/alert state
- Materials are prepared and within reach
- Environment is calm (no competing noise, siblings occupied)
- You are calm and patient (your dysregulation transfers)
- Timer is set and visible to child
ABSOLUTE CONTRAINDICATIONS: Never force water on face or restrain child for washing. Never surprise with water or cloth contact. Never use face washing as punishment. Never compare to siblings. Never shame for dirty face or distress. Avoid light, tickling touch — this triggers MORE aversion than firm pressure. Never skip drying — residual wetness prolongs distress.
Research Evidence: Indian Journal of Pediatrics RCT (2019): Home-based sensory interventions safety protocols. References: DOI: 10.1007/s12098-018-2747-4

Environment Setup
Spatial Precision Prevents 80% of Session Failures
🎮 Desensitization Play Setup
(Living Room / Outdoors — NOT the bathroom)
- Calm, comfortable area — separate from hygiene context
- Child seated comfortably, facing you
- Massage tools / spray bottles within child's reach (they control access)
- Mirror at child's eye level (optional)
- Timer visible to child
- Towel for immediate drying nearby
- Remove distractions: TV off, siblings in another room, phone on silent
🚿 Hygiene Routine Setup
(Bathroom)
- Visual schedule posted at child's eye level next to sink
- Preferred washcloth selected and in view (child's choice)
- Water pre-tested to 37°C / body temperature
- Timer set and positioned where child can see
- Bath visor within reach if used for hair washing
- Mirror at child height (step stool if needed)
- Dry towel within arm's reach for immediate drying
- Preferred post-routine activity ready (transition object or reward)
Lighting: Bright enough to see clearly (important for mirror work). Avoid harsh overhead fluorescent — warm lighting is calming.
Research Evidence: Sensory Integration Theory (Ayres): Environmental setup is a core principle. Meta-analysis confirms structured environment maximizes effectiveness. References: PMC10955541
Act III: The Execution
Readiness Check
Is Your Child Ready? The Pre-Session Checklist
The best session is one that starts right.
01
Fed recently
Child has eaten within the last 2 hours (not hungry)
02
Well-rested
Child has had adequate sleep (not overtired)
03
Regulated state
No meltdown in the last 30 minutes
04
Healthy skin
No illness, fever, or visible skin irritation on face
05
Calm mood
Child is in a generally calm or neutral mood
06
Recovery time
At least 30 minutes since last demanding therapy session
07
Parent readiness
You (the parent) feel calm and patient
1
🟢 All 7 Checked → GO
Proceed with full protocol
2
🟡 5–6 Checked → MODIFY
One material only, shorter duration, extra reinforcement
3
🔴 Fewer Than 5 → POSTPONE
Alternative calming activity. Try again tomorrow. Postponement is not failure — it's clinical judgment.

Step 1 of 6
30–60 seconds
The Invitation: Every Protocol Begins Here
Every protocol begins with an invitation, not a command.
"Hey [child's name], want to play the face game? Look what I have today!" (Show the material — facial roller, spray bottle, or washcloth. Hold it where they can see it, not aimed at their face.)
Body Language
- Sit at child's level, not looming above
- Relaxed posture, warm smile
- Hold material casually, not pointed at child
- No sudden movements
✅ Acceptance Looks Like
- Child looks at material with curiosity
- Child reaches for material
- Child maintains position (doesn't back away)
- Child makes eye contact or smiles
⚠️ Resistance Looks Like
- Child turns away → "That's okay. I'll just play with it myself." Model on your own face.
- Child pushes material away → "You can hold it. Want to try on my hand first?"
- Child becomes distressed → Stop. Switch to preferred calming activity. Try again tomorrow.

Step 2 of 6
1–3 minutes
The Engagement: Material Introduction
Facial Massage Tools
"Watch, I'll do mine first!" Roll the tool firmly across your own cheek. "Ooh, that feels nice!" Offer to child: "Want to try on your arm?" Start with arm → hand → neck → outer cheek (only if child allows each progression).
Spray Bottle
"You be the boss of this spray bottle. Spray my hand!" Let child spray your hand, then their own hand, then arm. Only progress to face area when child volunteers. "Want to try spraying your arm? You decide where."
Washcloth Exploration
Lay out 3–5 texture options. "Which one feels nice? Touch them all." Let child rank. Use preferred texture for hygiene — even if it's silk. That's the starting point, not the failure.
Reinforcement Cue: The moment the child touches the material or allows any facial contact: "You did it! You're so brave!" — immediate, specific, enthusiastic. Within 3 seconds of the desired behavior.
Research Evidence: Sensory integration intervention with structured material introduction meets evidence-based practice criteria (Children, 2024). References: PMC11506176

Step 3 of 6
2–5 minutes
The Therapeutic Action: Track 1 — Desensitization Play
This happens OUTSIDE bath time, in a calm, playful context.
Facial Massage Protocol
Using the facial roller or your fingers with FIRM (not light) pressure:
1
Forehead
Roll or press firmly, slowly, 5 times
2
Outer Cheeks
Firm circles, 5 times each side
3
Jawline
Firm downward strokes, 5 times
4
Nose Area
ONLY if comfortable: single gentle press
5
Chin Area
ONLY if comfortable: firm circles
Key principle: FIRM pressure is better tolerated than light touch. Light touch activates the protective response. Deep pressure organizes the sensory system.
Spray Bottle Desensitization
- Child sprays own arms (both sides)
- Child sprays own hands (both sides)
- Child sprays own neck
- Child sprays air near face (not on face yet)
- Child sprays own cheek (one mist, child decides)
- Build gradually — never push past child's voluntary comfort
Step 3 Continued
During Bath/Wash Time
The Therapeutic Action: Track 2 — Modified Hygiene Routine
1
Review Schedule
"First wet cloth, then forehead, then cheeks, then dry, then done!"
2
Prepare
Use preferred-texture washcloth, dampened with 37°C water
3
Wash (Firm Strokes)
Start at forehead, announce each action, FIRM steady strokes
4
Timer = Stop
When time is up, STOP. Even if not "done."
5
Dry Completely
Firm pressure with dry towel. Celebrate!
Child Response Spectrum
✅ Ideal
Tolerates with mild discomfort, engages with material
⚠️ Acceptable
Tolerates briefly, needs breaks, requests stopping before timer
🔴 Concerning
Escalating distress, fight-flight activation, screaming. STOP. Return to previous phase.
Research Evidence: Meta-analysis (2024): 40-minute therapy sessions showed maximum effectiveness. Home-based sessions typically 10–20 minutes. References: PMC10955541

Step 4 of 6
3–5 minutes
Repeat & Vary: 3 Good Reps > 10 Forced Reps
Target Repetitions
- Facial massage: 3–5 full face sequences per session
- Spray bottle: 5–10 self-directed sprays per session
- Washcloth: 2–3 complete face wipe sequences per session
Variations to Maintain Engagement
- Change materials between reps (roller → ball → fingers)
- Add playful element: "Can you spray the rubber duck?" then "Can you spray your hand?"
- Sing a face-washing song during routine (same song every time = predictability)
- Take turns: "My turn, now your turn" (modeling)
Satiation Indicators — Stop When:
- Child begins looking away consistently
- Quality of tolerance decreases (more fidgeting, resistance)
- Child explicitly says or gestures "all done"
- Timer expires
Principle: Short, successful experiences beat long, traumatic ones. End on a positive. Leave child wanting slightly more rather than pushing past capacity.
Step 5 of 6
30 seconds
🎉 Reinforce & Celebrate
Celebrate the attempt, not just the success.
"You let me touch your cheek! That was SO brave!"
"You sprayed your own face! Look at you!"
"You did the whole timer! High five!"
"You washed your own face! You're a superstar!"
Reinforcement Menu
Verbal Praise
Specific, enthusiastic — not generic "good job." Name the exact behavior you're celebrating.
Physical
High five, fist bump, squeeze hug (if child likes deep pressure).
Tangible
Sticker on visual schedule, token toward preferred activity.
Natural Consequence
"Face is clean! Now let's go play [preferred activity]."
Timing Rule: Within 3 seconds. Delayed reinforcement loses effectiveness. Immediate + specific + enthusiastic = behavior increase. ABA Principle: Reinforce approximations. If the goal was 30 seconds and child tolerated 15 — celebrate 15. Progress is progress.

Step 6 of 6
1–2 minutes
The Cool-Down: No Session Ends Abruptly
Transition Warning (30 seconds before end)
"Two more, then all done!" or "When the sand runs out, we're all done!"
Cool-Down Activities
- Firm pressure hand squeeze or arm squeeze (proprioceptive calming input)
- Deep breath together: "Big breath in... big breath out"
- Child helps put materials away in their special box
- Immediate transition to preferred activity: "Face game is all done! Now let's go [preferred activity]!"
If Child Resists Ending
"I know you want more! We can play again tomorrow. Right now it's time for [preferred activity]." Use transition object if child has one. Maintain firmness with warmth — consistency builds trust.
Post-Session Checklist (Critical)
Dry face completely if any water was involved
Check face for any redness or irritation
Note child's state: calmer than start? Agitated? Same?
Data Tracking
60 Seconds of Data Now Saves Hours of Guessing Later
Within 60 seconds of session end, record these 3 data points:
1. Tolerance Duration
How many seconds did the child tolerate the facial touch/water/washcloth today? (Use timer reading)
2. Distress Level (1–5)
1 = No distress (comfortable)
2 = Mild discomfort
3 = Moderate distress
4 = Significant distress (crying)
5 = Severe distress (meltdown — that's data, not failure)
2 = Mild discomfort
3 = Moderate distress
4 = Significant distress (crying)
5 = Severe distress (meltdown — that's data, not failure)
3. Independence Level
A = Fully assisted
B = Partially assisted
C = Supervised self
D = Independent
B = Partially assisted
C = Supervised self
D = Independent
Track this daily. After 2 weeks, the pattern tells you everything. Session abandonment with distress level 5 is data — it tells you what triggered escalation and prevents repeating it tomorrow.
What If It Didn't Go as Planned?
Most sessions don't go perfectly. The technique needs adjustment, not the parent.
Problem 1: "Child screamed the moment they saw the washcloth."
Why: Conditioned anxiety — the washcloth is associated with distressing face washing. The object itself triggers the fear.
Fix: Use a completely different material first (spray bottle or massage tool). Once tolerance builds, reintroduce washcloth as the LAST texture in the gradient.
Fix: Use a completely different material first (spray bottle or massage tool). Once tolerance builds, reintroduce washcloth as the LAST texture in the gradient.
Problem 2: "Worked fine on arms but complete refusal on face."
Why: This is expected. Arms → face is a significant jump. The face has 10x the sensory receptor density.
Fix: Add intermediate steps: hand → wrist → forearm → upper arm → neck → ear → outer cheek edge. Progress may take days per zone.
Fix: Add intermediate steps: hand → wrist → forearm → upper arm → neck → ear → outer cheek edge. Progress may take days per zone.
Problem 3: "Child was fine yesterday but melted down today."
Why: Sensory thresholds fluctuate with sleep, illness, stress, hunger, and overall regulation load. A bad day is a bad day — not regression.
Fix: On hard days, skip desensitization. Use minimum-demand hygiene routine with maximum accommodations. Try again tomorrow.
Fix: On hard days, skip desensitization. Use minimum-demand hygiene routine with maximum accommodations. Try again tomorrow.
Problem 4: "Visual timer made it WORSE."
Why: For some children, the visual timer creates anticipatory anxiety (watching the countdown approach the "scary moment").
Fix: Try an auditory timer (phone alarm). Or count together verbally: "5, 4, 3, 2, 1, done!" — predictable endpoint without visual countdown anxiety.
Fix: Try an auditory timer (phone alarm). Or count together verbally: "5, 4, 3, 2, 1, done!" — predictable endpoint without visual countdown anxiety.
Problem 5: "Session abandoned — child was too distressed."
This is data, not failure. Record: distress level 5, what triggered escalation, what you tried. This information prevents a repeat tomorrow. Session abandonment is clinical judgment — it protects the child and preserves trust.

Personalization
No Two Children Are Identical. Adapt & Personalize.
Adjust the protocol daily based on your child's state — moving between difficulty levels is expected and healthy.
Sensory Avoider (Most Common)
- Light mist, ultra-soft cloth
- Warm water, deep pressure
- Short duration
- Maximum predictability
Sensory Seeker (Rare for Face)
- May prefer rougher texture
- Splashier water play
- More intense input
- If unsure: default to avoider protocol
Age Modifications
1
18 months – 3 years
Maximum play emphasis, minimal routine demand, parent-led
2
3–5 years
Balance play and routine, introduce choice-making, begin self-washing
3
5–10 years
Self-care independence emphasis, mirror work, generalization to other settings

Act IV: The Progress Arc
Week 1–2
What to Expect: The First Two Weeks
15%
Progress
Early micro-improvements
✅ What You'll See
- Slightly reduced resistance to seeing the materials
- Possible curiosity about spray bottle or massage tool
- May tolerate brief facial touch during desensitization play
- Hygiene routine may not change yet (that's normal)
❌ What Is NOT Progress Yet
- Independent face washing
- No distress at all
- Eagerness for bath time
Parent Emotional Preparation: Weeks 1–2 require the most patience. You may feel like "nothing is working" — track the data; it will show micro-improvements your frustration masks. Your consistency in these early weeks determines everything that follows.
Week 3–4
Consolidation Signs: Neural Pathways Are Forming
40%
Progress
Measurable consolidation
Consolidation Indicators — Watch for These Signals
- Child begins to anticipate the "face game" without fear (may even request it)
- Tolerance duration increasing by measurable seconds
- Distress level dropping on the 1–5 scale
- Child may start touching their own face spontaneously during play
- Bath time resistance decreasing (even if meltdowns aren't eliminated)
- Child shows preference for specific washcloth texture (this is progress — they're engaging with the material)
When to Increase: If distress level has been at 1–2 for 3 consecutive sessions → introduce next facial zone or slightly less preferred washcloth texture. If spray bottle play shows voluntary face spraying → begin incorporating into hygiene transition.
Parent Milestone:"You may notice you're more confident too. You've read your child's cues 50+ times now. You know what works."
Week 5–8
Mastery Indicators: Here's How You Know
75%
Progress
Approaching mastery
Mastery Criteria
Timer Tolerance
Child tolerates full face washing with preferred washcloth and temperature for the complete visual timer duration (30+ seconds) with distress level 1–2
Self-Washing
Child demonstrates self-washing with mirror at least partially
Routine Stability
Hygiene routine completed without meltdown for 5+ consecutive days
Meal Time Transfer
Child accepts face wiping after meals with minimal protest
Generalization Indicators
- Tolerates face washing at grandparent's house
- Allows face wiping at school/daycare
- Sunscreen or lotion application accepted (partial or full)
- Swimming lessons become possible (face-in-water may still need more time)
✅ Mastery Met
Move to celebration, then progression pathway
⚠️ Partial Mastery
Continue at current level. Many children need 10–12 weeks. That's normal.
🔴 No Progress After 8 Weeks
Professional consultation indicated
🎉 Celebrate This Win
You did this. Your child grew because of your commitment.
Eight weeks ago, face washing was a nightly battle that left both of you exhausted and in tears. Today, your child washes their own face — or at least tolerates it without screaming. That transformation didn't happen by accident. It happened because you showed up every single day with patience, the right materials, and the belief that your child's nervous system could learn.
Family Celebration Ideas
Child's Choice Dinner
Let your child pick tonight's dinner to celebrate their achievement.
Achievement Certificate
Create a "I can wash my face!" certificate together — this is a real milestone.
Document the Moment
Take a photo of your child at the bathroom mirror, smiling. Six months from now, when a new challenge arrives, look at this photo and remember: your child can do hard things. And so can you.
🔴 Red Flags: When to Pause and Ask
Trust your instincts. If something feels wrong, pause and seek guidance.
1
Skin Infections or Persistent Redness
If your child's face is developing skin issues because face washing is so limited, consult a dermatologist AND an occupational therapist. Medical treatment + sensory intervention simultaneously.
2
Complete Avoidance of ALL Face Touching
If your child avoids all facial touch — not just water, but also hugs near face, wiping after food, sunscreen, doctor's touch — this may indicate a broader sensory processing disorder requiring comprehensive evaluation.
3
No Progress After 8–10 Weeks
Ask: Was the protocol actually followed daily? Was there a trust breach (forced washing, violated timer)? If yes to consistent execution with no progress → professional OT evaluation indicated.
4
Worsening Sensitivity
If tolerance is decreasing rather than staying stable — consider: new stressor at school? Medication change? Illness? Sleep disruption? Regression needs root-cause investigation.
5
Signs of Trauma Response
If child shows extreme avoidance specific to bathrooms, running water sounds, or anyone approaching their face — particularly with flashbacks or freezing — this requires a trauma-informed approach beyond standard sensory desensitization.
Escalation Pathway: Self-resolve → Teleconsultation (call 9100 181 181) → Pinnacle center visit → Comprehensive sensory evaluation

Your Journey Map
The Progression Pathway: Where You Were, Where You Are, Where You're Going
Your materials from this technique — visual timer, social story, spray bottle, sensory tools — carry forward into multiple related challenges. You're building a reusable therapeutic toolkit.
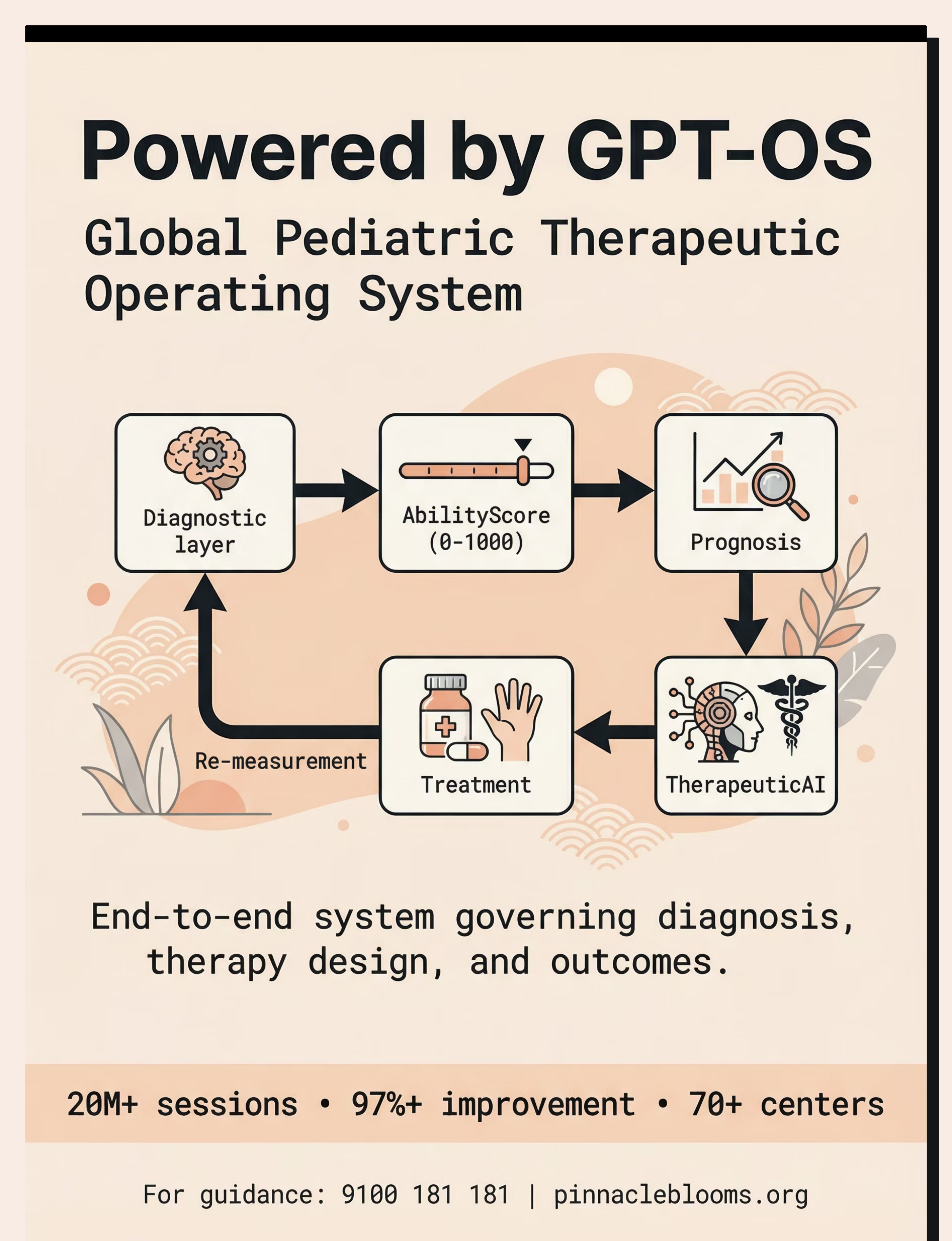
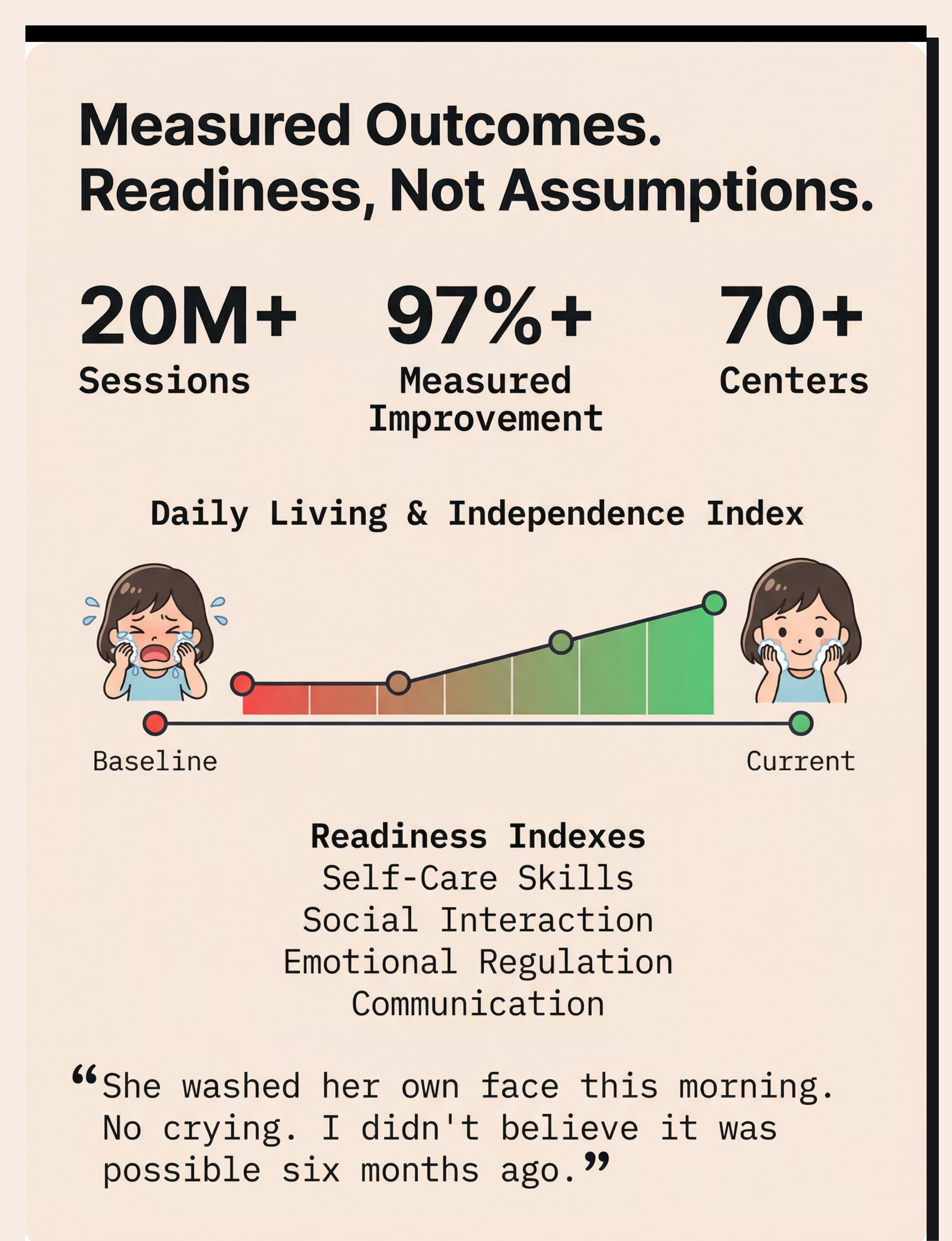
Long-Term Developmental Goal: Full self-care independence across all Activities of Daily Living — Daily Living & Independence Index progression tracked through GPT-OS® AbilityScore®.

Technique Domain
Related Techniques: You Already Own Materials for These
Technique | Difficulty | Canon Material | Your Materials Work? | |
A-001: Touch Sensitivity | Intro | Tactile Sensory Kit | ✅ Yes | |
A-009: Sand Play Avoidance | Intro | Sensory Play | ✅ Partial | |
A-016: Toothbrushing Meltdowns | Core | Oral Motor + Visual Supports | ✅ Timer, Visual Schedule | |
A-017: Haircut Terror | Core | Self-Care Adaptation | ✅ Visual Timer, Social Story | |
A-018: Nail Cutting Resistance | Core | Self-Care Adaptation | ✅ Visual Timer | |
A-019: Hair Brushing Aversion | Core | Tactile Sensory Kit | ✅ Texture Gradient |
Domain A: Sensory Processing — Tactile Series
Preview of 9 materials that help when child hates face washing Therapy Material
Below is a visual preview of 9 materials that help when child hates face washing therapy material. The pages shown help educators, therapists, and caregivers understand the structure and content of the resource before use. Materials should be used under appropriate professional guidance.






Link copied!

Your Child's Full Developmental Map
This Technique Is One Piece of a Larger Plan
A — Sensory Processing ⭐
CURRENT FOCUS — Tactile-facial desensitization
B — Gross Motor
Balance, coordination, strength
C — Fine Motor
Hand skills, writing, manipulation
E/F — Speech & Language
Receptive and expressive communication
G — Social Communication
Interaction, reciprocity, pragmatics
K — Daily Living ⭐
SECONDARY — Face washing is an ADL goal
Your Current Focus: Domain A (Sensory) feeding directly into Domain K (Daily Living). When tactile tolerance improves, self-care independence follows — the domains aren't siloed; they cascade.