"He pushes me away every time I try to hug him."
It's breakfast. You've made his favorite toast with the crusts cut off. He's calm, happy, humming. You lean in to give him a morning hug — and his entire body stiffens. His hands shoot up. He pushes your arms away and runs to the other side of the room. You're left kneeling on the kitchen floor, arms empty, heart breaking. Again.
You are not failing. Your child's nervous system is speaking a language their body hasn't learned to translate yet. And you can learn to hear it.
This page contains 9 clinically validated materials — developed by the Pinnacle Blooms Consortium of 500+ pediatric therapists — that help children with tactile aversion build a bridge to the touch they need and the connection you both deserve.
Sensory Solutions Series — Episode 2
Domain: Tactile Processing
Age: 2–6 Years

You Are Among Millions
You are not the only parent who has reached for their child and been pushed away. This is not rare. This is not your fault. And this is addressable.
80%
Display Sensory Difficulties
Of children diagnosed with autism, with tactile defensiveness among the most common presentations. Source: PRISMA Systematic Review, Children (2024) | PMC11506176
60–70%
Human Touch Aversion
Of children with sensory processing challenges experience specific aversion to human touch — distinguishable from general texture sensitivity. Source: SPD Foundation Clinical Data
1 in 36
ASD Diagnoses (US)
Children in the United States are diagnosed with ASD (CDC, 2023). In India, prevalence ranges from 1 in 68 to 1 in 100 — representing millions of families navigating sensory challenges daily.
82%
Measurable Improvement
Of children receiving targeted touch desensitization interventions across the Pinnacle Blooms Network showed measurable improvement in touch tolerance within 8–12 weeks.

This Is Neurology, Not Rejection
What Happens in the Brain
When you touch your child, sensory receptors in their skin send signals through the nervous system to the somatosensory cortex — the brain's touch processing center.
In children with tactile defensiveness, this cortex over-amplifies incoming signals. What you experience as a gentle hug, your child's brain registers as an overwhelming sensory flood — as if someone turned the volume to maximum on every nerve ending simultaneously.
Why Human Touch Is the Hardest
This is particularly intense with human touch because of its unpredictability. Your child cannot predict the exact pressure, location, duration, or texture of another person's touch the way they can predict touching an object.
This unpredictability triggers the brain's threat detection system, resulting in fight-or-flight responses: stiffening, pushing away, crying, or fleeing.
Key Insight: "This is a wiring difference, not a behavior choice. Your child is not choosing to reject you — their brain is protecting them from what it perceives as danger." Source: Frontiers in Integrative Neuroscience (2020) | DOI: 10.3389/fnint.2020.556660

Your Child's Developmental Map
Touch aversion to human contact typically becomes observable between 18 months and 3 years — when social touch expectations increase significantly. Here is where your child sits on the developmental timeline, and where you are heading.
0–6 Months
Calmed by skin-to-skin contact
6–12 Months
Explores textures with hands and mouth
12–18 Months
Tolerates varied touch from familiar caregivers
18–24 Months
Begins to initiate affectionate touch (hugs, kisses)
2–3 Years ⚠️
Challenge Zone: Accepts touch from peers during play — where many children with tactile defensiveness struggle most
4–6 Years
Regulates touch responses in social settings — the mastery goal
Comorbidity Note: Touch aversion commonly co-occurs with clothing sensitivity, food texture aversion, and social withdrawal. Addressing touch aversion often creates positive cascading effects across multiple developmental domains. Source: WHO Care for Child Development Package (2023) | PMC9978394

What the Science Says
Evidence Grade: Level I–II
Systematic Reviews + RCTs
~85% Confidence
Every material and technique on this page is grounded in peer-reviewed research endorsed by AOTA, WHO, and the Pinnacle Blooms Consortium. Here is the evidence base behind what you are about to learn.
Finding 1 — PRISMA Systematic Review (2024)
Analysis of 16 studies from 2013–2023 confirmed that sensory integration intervention meets criteria as evidence-based practice for children with ASD, with significant improvements in tactile processing, social skills, and adaptive behavior.
Source: PMC11506176 | Children (2024)
Finding 2 — Meta-Analysis of 24 Studies (2024)
Demonstrated that sensory integration therapy effectively promotes social skills, adaptive behavior, sensory processing, and motor skills in children with ASD. Individual (1:1) treatment sessions were most effective.
Source: PMC10955541 | DOI: 10.12998/wjcc.v12.i7.1260
Finding 3 — Indian RCT (Padmanabha et al., 2019)
Demonstrated significant outcomes from home-based sensory interventions administered by trained parents, establishing feasibility and efficacy in the Indian context.
Source: DOI: 10.1007/s12098-018-2747-4 | Indian Journal of Pediatrics
Clinically validated. Home-applicable. Parent-proven. The 9 materials on this page are drawn from evidence-based practice guidelines endorsed by AOTA, WHO, and the Pinnacle Blooms Consortium.

The Technique: What It Is
Domain A — Sensory Processing
Age: 2–6 Years
10–20 Min/Session
Daily
Formal Name
Graded Tactile Desensitization Protocol — Human Touch Tolerance Building
Parent-Friendly Name
"Bridge to Touch" — 9 Materials That Help Your Child Tolerate Being Touched
What It Is
A structured, evidence-based sensory intervention protocol that uses 9 clinically selected materials and techniques to progressively reduce a child's defensive response to human touch. The protocol works by first regulating the nervous system through deep pressure and proprioceptive input (Materials 1–5), then gradually introducing controlled human touch exposure (Materials 6–8), with professional clinical support (Material 9).
How A-002 Differs from A-001: A-001 addresses general touch sensitivity to all textures and surfaces. A-002 focuses specifically on aversion to human touch — the relational and emotional dimension of tactile defensiveness that directly impacts parent-child bonding and attachment.
Your Child's Expert Team
Touch aversion crosses therapy boundaries because the brain doesn't organize by therapy type. Your child's experience involves sensory processing, behavior patterns, communication, and neurodevelopment — all simultaneously.
Occupational Therapist (Primary Lead)
OTs are the primary architects of tactile desensitization protocols. They assess your child's sensory profile, design the graded exposure sequence, and train parents in techniques like the Wilbarger Brushing Protocol. OT leads the "how" of touch tolerance building.
Board Certified Behavior Analyst (BCBA)
BCBAs design the reinforcement systems that motivate your child through the desensitization process, structure the touch hierarchy, and analyze session data to optimize progression. BCBA leads the "when to push, when to pause."
Speech-Language Pathologist (SLP)
SLPs help children develop language to express touch preferences ("too much," "gentle please," "not now") and support parents in reading non-verbal communication cues during touch interactions.
NeuroDevelopmental Pediatrician
The physician confirms the neurological basis of touch aversion, rules out medical conditions, monitors medication interactions, and provides the developmental context within which the sensory intervention sits.
Source: Adapted UNICEF/WHO Nurturing Care Framework for SLPs (2022) | DOI: 10.1080/17549507.2022.2141327
Precision Targets — This Is Not Random Activity
Every session you run is aimed at specific, measurable outcomes. Understanding your targets helps you recognize progress — even when it feels invisible.
🎯 Primary Target
Increased tolerance to human touch — measured by duration of tolerated contact, proximity acceptance, and touch initiation frequency.
Observable: Child allows hand on shoulder 3+ seconds; sits within arm's reach for 5+ minutes; initiates high-five or fist bump.
⭕ Secondary Targets
Emotional regulation during touch events; parent-child attachment strengthening; self-regulation through deep pressure.
Observable: Reduced crying when touched; child approaches parent for comfort; child wraps in weighted blanket independently.
🔵 Tertiary Targets
Social skill development; adaptive behavior improvement (grooming, dressing, dental/medical touch); generalization to new people and environments.
Observable: Allows classmate to hold hand; tolerates hairbrushing; permits doctor's examination.
Source: Meta-analysis, World J Clin Cases (2024) | PMC10955541

Your Materials Kit — Everything You Need
9 Materials
Complete Kit: ₹4,000–15,000
Starter Kit: ₹0–2,000
These 9 materials form the clinical backbone of the Bridge to Touch protocol. You do not need all 9 to begin — Materials 1 and 5 are available in every home, at zero cost, today.
1
Weighted Blanket (Child-Sized, 2–4 kg)
Canon Category: Sensory Regulation Tools | Price: ₹2,000–4,000
Where: Amazon.in — search "kids weighted blanket 2kg"
Material Page: materials.pinnacleblooms.org/weighted-blanket-lap-pad-sensory-regulation
Where: Amazon.in — search "kids weighted blanket 2kg"
Material Page: materials.pinnacleblooms.org/weighted-blanket-lap-pad-sensory-regulation
2
Squeeze Machine / Pillow Hug Setup
Canon Category: Deep Pressure Tools | Price: ₹3,000–8,000 commercial or ₹0 DIY
Where: Amazon.in or DIY with household cushions
Where: Amazon.in or DIY with household cushions
3
Large Therapy/Exercise Ball (55–65 cm)
Canon Category: Proprioceptive Input Tools | Price: ₹500–1,000
Where: Amazon.in — search "therapy ball 55cm"
Material Page: materials.pinnacleblooms.org/therapy-ball-chairs
Where: Amazon.in — search "therapy ball 55cm"
Material Page: materials.pinnacleblooms.org/therapy-ball-chairs
4
Sensory Body Sock (Size-Appropriate)
Canon Category: Compression Garments | Price: ₹600–1,200
Where: Amazon.in — search "sensory body sock kids"
Material Page: materials.pinnacleblooms.org/compression-vest-body-sock-proprioceptive
Where: Amazon.in — search "sensory body sock kids"
Material Page: materials.pinnacleblooms.org/compression-vest-body-sock-proprioceptive
5
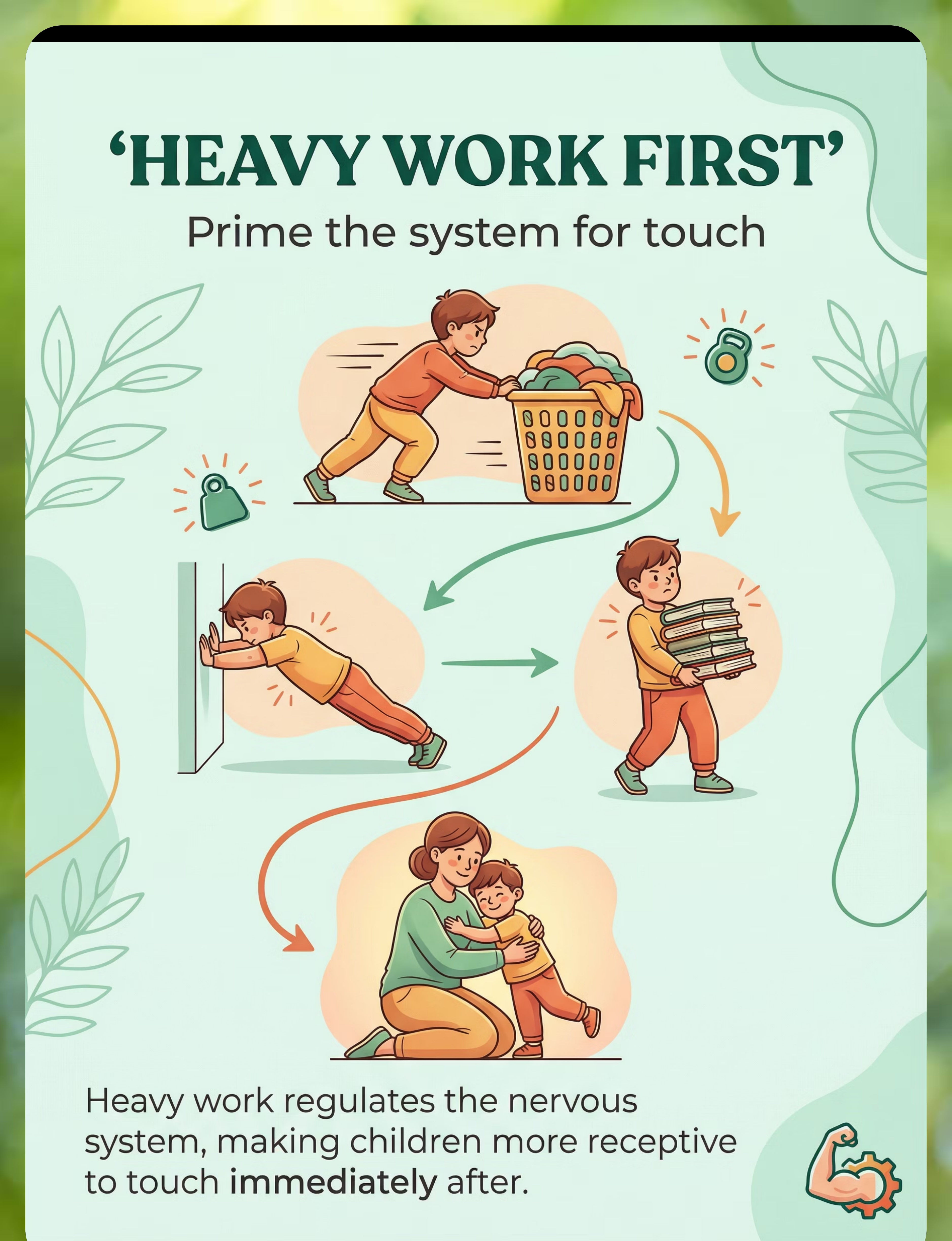
Household Heavy Work Items
Canon Category: Proprioceptive Activities | Price: ₹0–500 (household items)
Examples: Laundry basket, stack of books, filled backpack
✅Best starter material — zero cost
Examples: Laundry basket, stack of books, filled backpack
✅Best starter material — zero cost
6
Touch Hierarchy Visual Cards
Canon Category: Visual Supports | Price: ₹150–300 or homemade
Where: Amazon.in or DIY laminated cards showing touch levels from high-five to front hug
Where: Amazon.in or DIY laminated cards showing touch levels from high-five to front hug
7
Firm Touch Training Guide
Canon Category: Technique Training | Price: ₹0 (parent technique — free)
No purchase required — the technique is taught on this page
No purchase required — the technique is taught on this page
8
Child-Safe Massage Tools
Canon Category: Tactile Sensory Tools | Price: ₹200–600
Examples: Roller, spiky ball, low-vibration massager
Where: Amazon.in — search "kids massage roller set"
Material Page: materials.pinnacleblooms.org/tactile-sensory-kit-texture-exploration
Examples: Roller, spiky ball, low-vibration massager
Where: Amazon.in — search "kids massage roller set"
Material Page: materials.pinnacleblooms.org/tactile-sensory-kit-texture-exploration
9
Wilbarger Brushing Protocol Brush + OT Training
Canon Category: Clinical Protocol Materials | Price: ₹200–400 (brush) + OT consultation
Where: Amazon.in or Available through Pinnacle Blooms centers
⚠️REQUIRES PROFESSIONAL TRAINING — Never use without OT guidance
Where: Amazon.in or Available through Pinnacle Blooms centers
⚠️REQUIRES PROFESSIONAL TRAINING — Never use without OT guidance

Every Family Can Start Today — Zero Cost Options
Not every family has access to specialty therapy materials. The WHO Nurturing Care Framework emphasizes that effective intervention must be context-specific and equity-focused. Every material on this page has a household substitute that activates the same sensory principle.
Buy This | Make This (Zero Cost) | |
Weighted Blanket (₹2,000–4,000) | Fill a duvet cover with dried rice or plastic pellets in quilted sections. Target 10% of child's body weight. Sew closed. | |
Squeeze Machine (₹3,000–8,000) | Place 2 large couch cushions on either side of child. Child crawls between and controls pressure. Parent may gently press on request. | |
Therapy Ball (₹500–1,000) | Use a large inflatable ball, beach ball, or rolled-up yoga mat for steamroller activity. | |
Body Sock (₹600–1,200) | Large lycra pillowcase with hole cut for head. Child climbs in and stretches against resistance. | |
Heavy Work Materials (₹0–500) | Laundry basket with clothes, stack of books, filled water bottles in a backpack — all available at home. | |
Touch Hierarchy Cards (₹150–300) | Hand-draw or print photos: high-five → fist bump → handshake → pat on back → side hug → front hug. Laminate with tape. | |
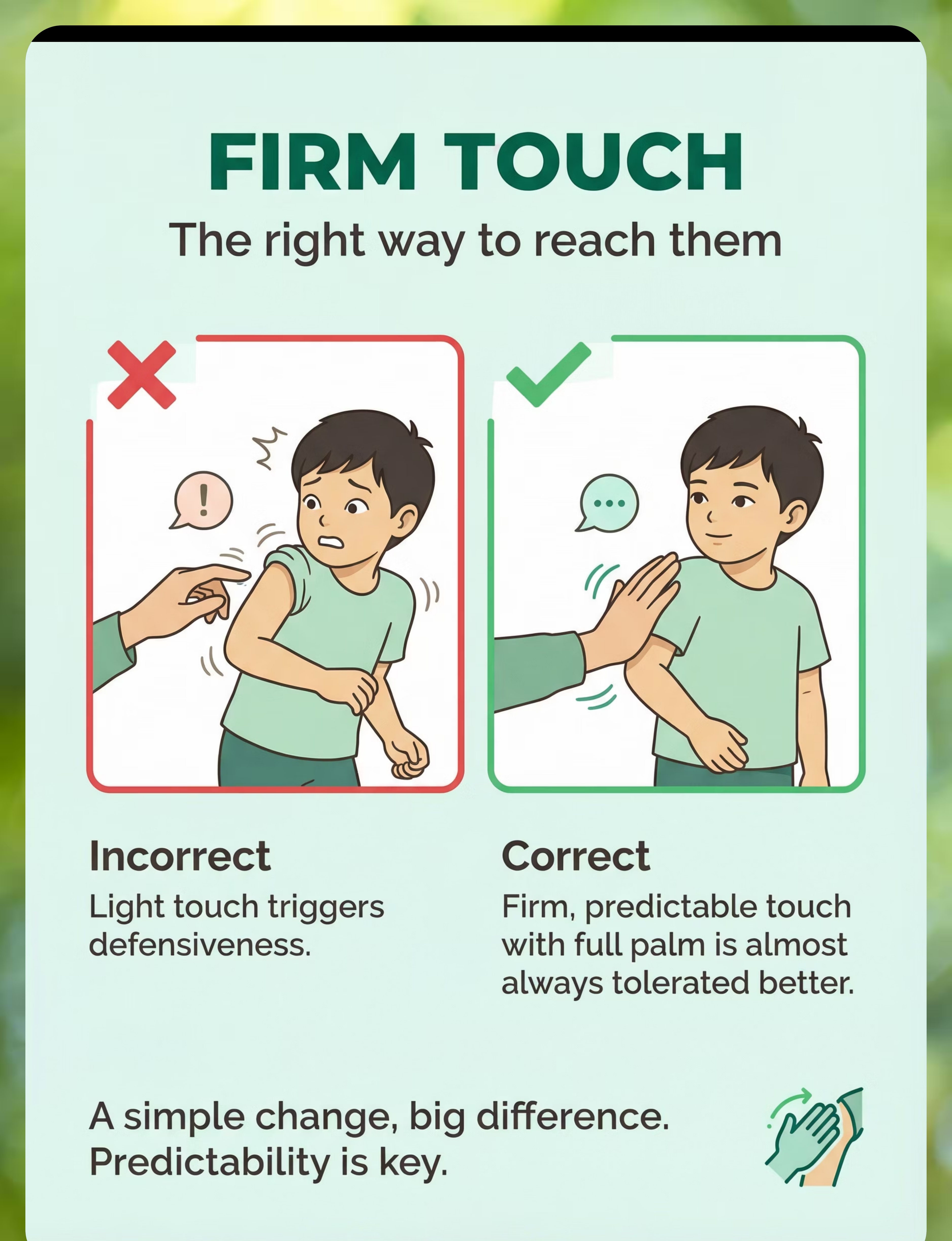
Firm Touch Guide (₹0) | Practice the difference: light fingertip touch vs. firm full-palm contact. Always announce before touching. | |
Massage Tools (₹200–600) | Tennis ball in a sock for self-massage. Wooden rolling pin with towel wrap. Textured kitchen sponge. | |
Wilbarger Brush (₹200–400) | ⚠️ NO SUBSTITUTE — Requires clinical-grade brush and professional OT training. Do not attempt without guidance. |
Why substitutes work: The sensory principle is the same — deep pressure, proprioceptive input, controlled compression. The delivery mechanism changes, not the neurological effect. Source: WHO NCF (2018) | PMC9978394

Safety Gate — Read Before Every Session
Your child's safety and yours are the non-negotiable foundation of this protocol. Read and review this card before every session. When in doubt, always choose the more conservative path.
🔴 DO NOT PROCEED IF:
- Child is in active meltdown or highly dysregulated
- Child has fever, illness, or recent injury at contact sites
- Child shows panic-level responses to ANY touch (seek professional assessment immediately)
- You are attempting the Wilbarger Protocol without OT training
- Child has skin conditions, open wounds, or recent surgical sites
- You are feeling frustrated, angry, or emotionally overwhelmed
🟡 MODIFY IF:
- Child seems tired or mildly irritable — use shorter session, lower-demand materials only
- Child had a recent meltdown — wait 20+ minutes for full regulation before starting
- First time using a new material — introduce for observation only, no touch demands
- Child is in an unfamiliar environment — return to mastered materials only
🟢 PROCEED IF:
- Child is fed, rested, and in a regulated state
- Environment is set up per Card 12 specifications
- Materials are clean, inspected, and age-appropriate
- You have 15–20 minutes of uninterrupted time
- You are calm, present, and ready to follow the child's lead
Material-Specific Safety: Weighted blanket: NEVER exceed 10% of body weight. Child must be able to remove independently. Do not use during sleep for children under 4. Body sock: Always supervise. Ensure breathing is unobstructed. Steamroller: Avoid head, neck, and stomach. Use firm, slow pressure only. Squeeze machine: Child must always control the pressure. Never restrain.
RED LINE: NEVER force physical affection. NEVER use touch as reward or withhold affection as punishment. NEVER restrain a child to deliver touch. NEVER compare your child to siblings or peers who accept touch.
RED LINE: NEVER force physical affection. NEVER use touch as reward or withhold affection as punishment. NEVER restrain a child to deliver touch. NEVER compare your child to siblings or peers who accept touch.
Source: Padmanabha et al., Indian J Pediatr (2019) | DOI: 10.1007/s12098-018-2747-4
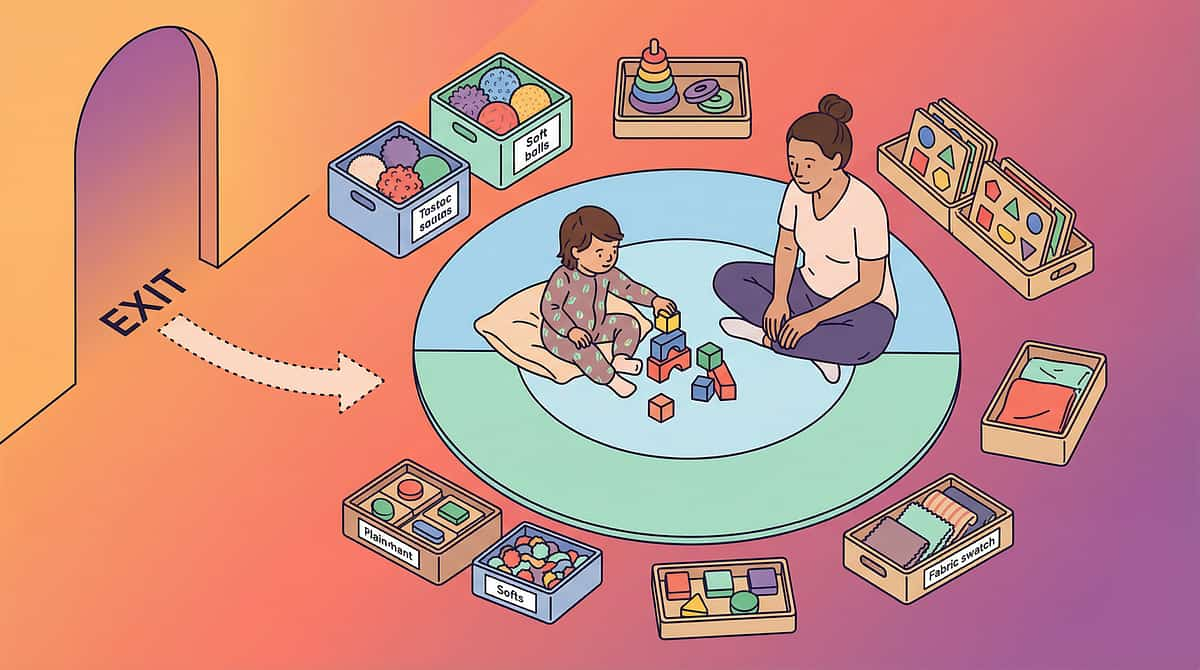
Your Therapy Space — 3 Minutes to Set Up
5-Point Space Setup
- Child's position: Floor mat or couch, with clear exit path — child must never feel trapped
- Parent's position: Beside (not facing) child — side-by-side reduces confrontation pressure
- Materials station: Within arm's reach, organized by session order (weighted blanket → therapy ball → touch cards)
- Distraction-free zone: TV off, siblings elsewhere, phone on silent
- Exit path: Clear, unblocked route for child to leave if needed
Environment Checklist
- Lighting: Soft, warm — avoid harsh overhead fluorescent
- Sound: Quiet. No TV, radio, or competing sounds. Soft background music acceptable if child prefers
- Temperature: Comfortable — temperature extremes amplify tactile sensitivity
- Surface: Soft mat or carpet — hardwood floors feel different through touch
- Timing: Same time daily. Post-bath or post-meal often works best
"80% of session failures trace back to environmental setup. The 3 minutes you spend preparing this space eliminate the 3 meltdowns you'd spend recovering from." Source: Sensory Integration Theory (Ayres) | PMC10955541

Pre-Flight Check — 60 Seconds
Step 0 of 6
Readiness Check
Before Every Session
Run through this checklist before every session. Sixty seconds of assessment now prevents thirty minutes of recovery later.
Child has eaten within the last 2 hours
Hunger amplifies sensory reactivity. A fed child is a more regulated child.
Child has slept adequately and is not overtired
Fatigue dramatically lowers the tolerance threshold for all sensory input.
No meltdown in the last 30 minutes
The nervous system needs time to return to baseline after a dysregulation event.
Child is not currently in a preferred activity
Interrupting a preferred activity creates immediate resistance before the session begins.
Child shows neutral or positive affect
Starting from distress makes the hill steeper. Start from calm.
YOU are calm and emotionally present
Your emotional regulation is not optional — it is the first therapeutic tool.
✅ All checked → GO
Begin at Step 1: The Invitation
⚠️ 1–2 unchecked → MODIFY
Use only Materials 1 or 5. No touch demands today. This IS a valid session.
🛑 3+ unchecked → POSTPONE
Offer a preferred calming activity. Try again tomorrow. This is clinical judgment, not failure.

Step 1: The Invitation
Step 1 of 6
Duration: 30–60 Seconds
Move to the prepared space. Sit beside your child — not facing them. Place the first material visible but not in the child's space. Wait. Do not demand. Do not negotiate. Simply be present with the material.
"Hey [child's name], I have something cozy. Want to check it out with me? No touching — just looking."
Body Language Guidance
- Relaxed posture, shoulders down
- Looking at the material, not at the child (reduces social pressure)
- Hands visible and still — no reaching toward child
- Voice: low, slow, warm — not excited or overly enthusiastic
Reading the Response
Acceptance looks like: Glancing at material, moving toward you, reaching for it, saying "okay," body remaining relaxed.
Resistance — how to respond: Child turns away → "That's okay. It's here when you're ready." Child says "no" → Accept immediately. Never negotiate, bribe, or insist. Child becomes distressed → Session ends. This is data, not failure.

Step 2: The Engagement
Step 2 of 6
Duration: 1–3 Minutes
Once the child shows acceptance, introduce the material without placing it on the child. Let them observe you using it first — modeling removes the pressure of being the subject of touch before the child is ready.
Weighted Blanket
Place it over YOUR lap first. "This is so heavy and warm. Feel how heavy." Pat the blanket on your own legs. Wait for the child's curiosity to pull them in.
Therapy Ball (Steamroller)
Roll the ball gently on the floor near the child. "This ball can give really strong pushes — watch." Press it against a pillow to demonstrate pressure and control.
Body Sock
Show it as a "superhero costume." Demonstrate putting your own arm in. "It squeezes! Want to try just one hand?" Give the child a single, low-stakes entry point.
Heavy Work
Start the activity yourself. Push the laundry basket. Carry the books. "I need a strong helper. This is so heavy!" Let the child choose to join — invitation only.
Reinforcement Cue: The moment the child touches or interacts with ANY material: "You're so brave. Look at you checking it out!" This immediate, specific praise reinforces approach behavior. Source: PMC11506176 — Structured material introduction in sensory integration intervention

Step 3: The Therapeutic Action
Step 3 of 6
Duration: 3–5 Minutes
Core Therapeutic Event
The child is engaged. Now deliver the specific sensory input — deep pressure, proprioceptive feedback, or controlled touch exposure — that constitutes the active ingredient of this intervention.
Weighted Blanket Protocol
Place the blanket over the child's lap (never over face or chest for under-4s). Sit beside them. Read or watch something together. After 3–5 minutes of calm, gently place your hand on the blanket over their knee — touch through the buffer. This is the bridge.
Steamroller Protocol
Child lies face-down on mat. Slowly roll the therapy ball over their back, arms, and legs with firm, even pressure. Count aloud: "One... two... three... rolling." Predictability reduces threat. Pause after 3 rolls. If child requests more, continue. This primes the nervous system for human touch.
Body Sock Protocol
Child enters body sock. Encourage stretching, pushing, and movement inside the compression garment for 3–5 minutes. Upon emerging, the nervous system is typically calmer. THIS is the optimal moment to offer a brief, firm touch — hand on shoulder, high-five.
Heavy Work Protocol
10 minutes of pushing, pulling, or carrying. Wall push-ups (10 reps). Laundry basket push across room (5 trips). Book carrying (stack of 5+). Immediately after — offer a hug or high-five. Heavy work primes the proprioceptive system, making touch more tolerable.
Common Execution Errors: Using light, hesitant pressure (triggers defensiveness — use FIRM). Moving too fast (unpredictability triggers threat response). Talking too much during action (competing sensory overload). Watching the child's face intensely (social pressure amplifies sensory pressure).
Step 4: Repeat and Vary
Step 4 of 6
Duration: 3–5 Minutes
Target: 3–5 Repetitions
Quality over quantity. Three engaged repetitions are worth more than ten forced ones. Vary the approach to maintain interest across sessions while honoring the same sensory principle.
Variation by Material
- Steamroller: Change direction (head-to-toe, then side-to-side). Add a playful count: "The steamroller is coming! 3... 2... 1... squish!"
- Weighted Blanket: Different seating positions — couch, floor, beanbag. Pair with a book or tablet for engagement.
- Body Sock: Dance inside, do "superhero poses," play freeze dance while wearing it.
- Heavy Work: Change the objects (pillows instead of books, grocery bags instead of laundry). Create a "delivery game."
- Touch Cards: Move to the next hierarchy level if mastered. Add a reward sticker to the completed level.
Satiation Indicators
Your child is telling you they've had enough when you see:
- Looking away, unfocused gaze
- Decreased movement or effort
- Pushing the material away
- Requesting a different activity
- Increased fidgeting or vocalization
Honor these signals immediately. Respect builds trust.
"3 good repetitions where your child is engaged and regulated are worth more than 10 forced repetitions where you're both exhausted. Respect the signal."

Step 5: Reinforce and Celebrate
Step 5 of 6
Duration: 1–2 Minutes
Timing Rule: Reinforcement must arrive within 3 seconds of the desired behavior. Late praise is lost praise.
After child touches material:
"You touched it! That was so brave!"
After child tolerates your hand on the blanket:
"You let my hand be right here next to you. That's amazing."
After child allows brief touch:
"You let me give you a squeeze! Your body did that. I'm so proud."
After child initiates contact:
"YOU came to ME! That's the best feeling. Thank you."
Reinforcement Menu — Choose What Works for Your Child
Verbal Praise
Enthusiastic, specific — name exactly what they did
High-Five
Itself a touch milestone — celebrate it!
Token / Sticker
Visual progress on a chart they can see
2 Min Preferred Activity
Screen time, toy, snack — whatever motivates
"Celebrate the attempt, not just the success. A child who sits near the weighted blanket without touching it is closer than a child who ran away. That's progress."

Step 6: The Cool-Down
Step 6 of 6
Duration: 2–3 Minutes
Never end abruptly. Transitions need predictability — the same principle that governs touch tolerance governs session endings. Give your child time to land.
Transition Warning Script
"Two more [rolls/stretches/carries], then we're all done."
Count down visually — show 2 fingers, then 1, then thumbs up for "all done." Predictable endings reduce resistance.
Material Put-Away Ritual
Include the child if possible: "Can you help put the ball back? You're so strong." This is a proprioceptive bonus AND teaches session boundaries.
Cool-Down Activities (choose one)
- Slow, deep breaths together — blow bubbles for a visual cue
- Quiet sitting with weighted blanket — no demands
- Gentle humming or singing a familiar song
- Quiet parallel activity (coloring, looking at a book)
Transition to Next Activity
"Great session! Now let's go [child's preferred next activity]." The session ends on a positive note. Do not extend the session to avoid resistance — consistent duration builds predictability.
Source: NCAEP Evidence-Based Practices Report (2020) — Visual supports and transition strategies

60 Seconds of Data Now Saves Hours of Guessing Later
Record these three things within 60 seconds of your session ending. After 2 weeks, you'll see the trend line. 3 seconds becomes 5 becomes 12. "Within arm's reach" becomes "sat beside" becomes "brief touch." The data shows you the progress your emotions might miss.
1. Duration of Tolerated Touch
How long did your child tolerate the closest human touch that occurred today? (Hand on blanket-covered knee? High-five held? Brief side-hug?)
Record in seconds: ___ seconds | Date: ___
2. Closest Contact Achieved
Same room → Within arm's reach → Sat beside → Touch through material → Brief direct touch → Sustained touch → Child-initiated touch
Circle or note which level was achieved today.
3. Child's Regulation Level (1–5)
1 = Calm throughout
2 = Mild tension, recovered
3 = Moderate distress, needed break
4 = Significant distress, session shortened
5 = Session abandoned due to distress
2 = Mild tension, recovered
3 = Moderate distress, needed break
4 = Significant distress, session shortened
5 = Session abandoned due to distress
PDF Tracker
Downloadable print-at-home tracker → pinnacleblooms.org/trackers/touch-tolerance
GPT-OS® App Tracker
In-app session logging with trend visualization → gpt-os.pinnacleblooms.org/session-log
Notebook
Write it anywhere — the data exists if you write it. Paper works just as well.

It's Not You. It's Not Them. Let's Troubleshoot.
Every family encounters obstacles. The following are the six most common session challenges encountered across the Pinnacle Blooms Network, with evidence-informed solutions for each.
Problem 1: Child refused to come to the space
Why: The space or timing wasn't right, or the child associates it with previous demands.
Next time: Change location (try outdoors, a different room). Remove any demand association — just have materials available during free play.
Next time: Change location (try outdoors, a different room). Remove any demand association — just have materials available during free play.
Problem 2: Child engaged but became distressed when you moved closer
Why: The material was working (regulation), but your proximity added an unpredictable social element.
Next time: Stay further away. Your presence is not required for every session — the material does the neurological work independently.
Next time: Stay further away. Your presence is not required for every session — the material does the neurological work independently.
Problem 3: Child completed heavy work but still rejected touch
Why: The proprioceptive input window may be shorter than expected. Touch attempt came too late.
Next time: Attempt touch IMMEDIATELY after heavy work — within 30 seconds. The regulation window is brief.
Next time: Attempt touch IMMEDIATELY after heavy work — within 30 seconds. The regulation window is brief.
Problem 4: Child was fine yesterday but refused today
Why: Sensory processing fluctuates with sleep, health, stress, and environment. This is normal — not regression.
Next time: Use today as a "maintenance day." Offer only the most preferred material, no progression. Tomorrow is a new day.
Next time: Use today as a "maintenance day." Offer only the most preferred material, no progression. Tomorrow is a new day.
Problem 5: You became frustrated and the session deteriorated
Why: You are a human being with emotional needs, and this process is genuinely hard.
Next time: Before sessions, do 5 deep breaths. Set an intention: "Whatever happens in the next 15 minutes is okay." If frustration rises mid-session, end with grace. Your regulation is the first therapeutic tool.
Next time: Before sessions, do 5 deep breaths. Set an intention: "Whatever happens in the next 15 minutes is okay." If frustration rises mid-session, end with grace. Your regulation is the first therapeutic tool.
Problem 6: Child allows touch from another caregiver but not from you
Why: Different people produce different sensory inputs. You may be more sensitized TO your touch because you are around most. This is information, not rejection.
Next time: The other caregiver's success proves the protocol works — generalization to you will follow. Continue your protocol with confidence.
Next time: The other caregiver's success proves the protocol works — generalization to you will follow. Continue your protocol with confidence.
"Session abandonment is not failure — it's data. Every 'failed' session teaches you something about your child's sensory profile that a 'successful' session never could."
Your Child Is Unique — So Is Their Protocol
There is no single right way to run this protocol. Adjust the difficulty to match your child's current state, sensory profile, and age. Use the guide below to make daily clinical decisions with confidence.
1
← Easier
Bad days, setbacks, new environments. Materials 1 or 5 only. No touch attempts. 5-minute sessions. Goal: Regulation only. Maximum reinforcement.
2
Standard
Most days. 2–3 materials in sequence. One touch attempt through buffer or direct. 10–15 minutes. One step forward on touch hierarchy. Verbal praise + token system.
3
Harder →
Breakthrough days, high motivation. Full 4-material sequence. Touch hierarchy progression. 15–20 minutes. Sustain touch 5+ seconds longer than previous best. Natural consequence reinforcement.
Sensory Profile Variations
Sensory Avoider (avoids ALL input): Start with Material 5 (Heavy Work) exclusively for Week 1. Add one material per week. Progression is slower but more stable.
Mixed Profile (seeks some, avoids touch): Use deep pressure materials (1, 2, 3, 4) to build regulation, then attempt touch during the regulation window.
Age Modifications
Ages 2–3: Shorter sessions (5–10 min), more play-based, fewer verbal instructions, more modeling. Child's attention span drives the pace.
Ages 4–6: Longer sessions (10–20 min), can use touch hierarchy cards, can participate in data tracking — "show me on the thermometer how it felt."

Weeks 1–2: The Foundation
Progress Check
Week 1–2
~15% Complete
The first two weeks are about building trust — with the materials, with the process, and with you. Visible progress may feel small. It is not. Every micro-shift is genuine neurological change happening beneath the surface.
What Progress Looks Like Now
- Child approaches the material space without resistance (even without participating)
- Duration of material engagement increases by even 30 seconds
- Child allows weighted blanket on lap for 1–2 minutes (previously pushed away)
- Reduced intensity of resistance to touch attempts — pushing away gently instead of screaming
- Child shows curiosity about materials left visible in the home
What Is NOT Progress Yet (Managing Expectations)
- Child will probably not accept a full hug yet
- Touch tolerance may fluctuate dramatically day to day
- There may be "worse" days that feel like regression — this is the nervous system recalibrating
- Don't expect your child to initiate touch
"If your child tolerates the weighted blanket for 3 seconds longer than last week — that IS real neurological change. The somatosensory cortex is recalibrating. You cannot see it, but it's happening."

Weeks 3–4: The Patterns Emerge
Progress Check
Week 3–4
~40% Complete
By weeks three and four, you will begin to see your child's individual pattern — which materials they prefer, when their regulation window opens widest, and how they signal readiness. This is your clinical intelligence building in real time.
Child anticipates the session
Goes to the space, asks for the material — the session has become a predictable, desired part of the day.
Reduced time needed before touch tolerance opens
Heavy work or deep pressure needed for less time before the child tolerates proximity or brief touch.
Child allows brief touch without pulling away
Hand on shoulder, high-five — short-duration direct touch becoming possible for the first time.
Behavioral changes signaling neural pathway formation
Child sits closer to you during non-therapy activities. Tolerates incidental touch from family members with less reactivity. May begin using deep pressure independently — wrapping in blankets, crawling under cushions.
When to advance: If child consistently achieves the session goal 3 days in a row → advance one level on touch hierarchy. If child requests more repetitions → increase by 1–2. If child spontaneously approaches for proximity → offer (don't grab) a brief touch.
Parent milestone: "You may notice you're more confident too. You've learned to read your child's cues. You know when to push and when to pause. That is clinical skill."
Parent milestone: "You may notice you're more confident too. You've learned to read your child's cues. You know when to push and when to pause. That is clinical skill."

Weeks 5–8: The Breakthrough Zone
Progress Check
Week 5–8
~75% Complete
This is where families feel the shift. Not in dramatic moments — in small, ordinary ones. The child who leans into you on the couch. The morning high-five that comes without asking. The hug that lasts a full five seconds.
✅ Mastery Criteria
- Child tolerates brief hug (3–5 seconds) from primary caregiver without distress
- Child initiates at least one physical contact per day
- Child sits in physical contact with caregiver for 5+ minutes during a shared activity
- Touch hierarchy has advanced at least 3 levels from baseline
- Deep pressure tools used independently for self-regulation
🌍 Generalization Indicators
- Skill appearing with secondary caregivers (other parent, grandparent)
- Tolerance improving in different environments (not just the therapy space)
- Reduced distress during grooming activities (hairbrushing, teeth cleaning)
- Emerging tolerance in peer settings (school, playground)
Mastery Unlocked Badge Criteria:✅ 3+ seconds of tolerated hug on 4 out of 7 days ✅ Child-initiated touch at least 3 times per week ✅ Touch hierarchy advanced 3+ levels ✅ Tolerance maintained across 2+ environments.
Maintenance: If tolerance drops without formal sessions → continue protocol at 3x/week maintenance frequency.
Maintenance: If tolerance drops without formal sessions → continue protocol at 3x/week maintenance frequency.

You Did This.
"Eight weeks ago, you were kneeling on the kitchen floor with empty arms. Today, your child placed their hand on yours. Not because you forced it. Because you built a bridge — material by material, session by session, day by day — and your child chose to cross it."
Starting Point
Child pushes away all human touch. Every hug attempt ends in distress.
Where You Are Now
Child tolerates and sometimes initiates gentle contact. Connection is happening.
What Changed
Not your child's personality — their nervous system's capacity to process your love.
Family Celebration Suggestion: Take a photo of a moment of connection this week. Put it somewhere visible. On hard days ahead — and there will be hard days — look at it and remember: this happened because of you.

Trust Your Instincts — When to Pause and Ask
Safety Alert
Red Flags
The protocol is powerful, but it is not a substitute for professional judgment. If any of the following signs appear, pause and seek guidance. Your instincts about your child are a clinical instrument — trust them.
🚩 Complete avoidance of ALL human touch after 4 weeks
Persisting across all caregivers, all materials, all environments despite consistent intervention.
Action: Schedule OT assessment at nearest Pinnacle center immediately.
Action: Schedule OT assessment at nearest Pinnacle center immediately.
🚩 Touch aversion worsening despite intervention
More intense reactions, expanding to previously tolerated touch types.
Action: Pause protocol. Teleconsultation within 48 hours.
Action: Pause protocol. Teleconsultation within 48 hours.
🚩 Self-injury to avoid touch
Child hits self, bites, or head-bangs when touch is anticipated.
Action: Immediate BCBA consultation for functional behavior assessment.
Action: Immediate BCBA consultation for functional behavior assessment.
🚩 Panic-level responses to any touch
Screaming, hyperventilating, dissociative freezing when touched or when touch is anticipated.
Action: Professional assessment required before continuing home protocol.
Action: Professional assessment required before continuing home protocol.
🚩 Touch aversion appearing suddenly
In a child who previously tolerated touch — sudden onset may indicate pain, trauma, or a medical condition.
Action: Medical evaluation first. Rule out physical causes before resuming sensory protocol.
Action: Medical evaluation first. Rule out physical causes before resuming sensory protocol.
🚩 No measurable progress after 8–10 weeks
Consistent daily intervention with no forward movement on any progress indicator.
Action: OT reassessment of sensory profile. Protocol modification needed.
Action: OT reassessment of sensory profile. Protocol modification needed.
01
Self-Resolve
Troubleshoot using Card 21 guidance
02
Teleconsult
pinnacleblooms.org/teleconsult
03
Clinic Visit
pinnacleblooms.org/centers — 75+ locations across India

Your Developmental GPS — Where You've Been, Where You're Going
This technique is one node in a connected network of developmental support. Knowing where you've come from and where you can go next helps you make purposeful decisions about your child's therapeutic journey.
Prerequisite
A-001: Touch Sensitivity (General)
→ techniques.pinnacleblooms.org/sensory/tactile/touch-sensitivity
→ techniques.pinnacleblooms.org/sensory/tactile/touch-sensitivity
★ YOU ARE HERE
A-002: Child Hates Being Touched
Current technique — human touch aversion, relational dimension
Current technique — human touch aversion, relational dimension
Path A — Clothing Textures
A-003: Clothing Tag Sensitivity → A-004: Fabric Refusal → A-005: Seam Sensitivity in Socks
Path B — Social Touch
A-021: Child Avoids Hugs (peer-focused) → A-025: Child Seeks Deep Pressure
Path C — Light Touch
A-024: Light Touch Defensiveness → A-002-DD-02: Firm Touch vs Light Touch Deep Dive
Lateral Alternatives: If this approach didn't fully resonate, consider C-332: Child Doesn't Seek Comfort (behavioral/attachment angle) or C-335: Building Connection (relationship-focused rather than sensory-focused).
Long-term goal: Full social participation with age-appropriate touch tolerance — hugs from family, handshakes, peer contact during play, tolerance of medical examinations, and grooming activities.
Long-term goal: Full social participation with age-appropriate touch tolerance — hugs from family, handshakes, peer contact during play, tolerance of medical examinations, and grooming activities.
Explore the Tactile Sensitivity Domain
Tactile Sensitivity Series (TAC-SENS-01)
Position 2 of 30 in Cluster
Every technique in this domain builds on the others. Start where your child is — and follow the path their progress reveals.

A-001: Touch Sensitivity (General)
Difficulty: Intro | Sensory Regulation Tools
"You already own materials for this" ✅
→ techniques.pinnacleblooms.org/sensory/tactile/touch-sensitivity
"You already own materials for this" ✅
→ techniques.pinnacleblooms.org/sensory/tactile/touch-sensitivity

A-003: Clothing Tag Sensitivity
Difficulty: Intro | Clothing Adaptations
→ techniques.pinnacleblooms.org/sensory/tactile/clothing-tag-sensitivity
→ techniques.pinnacleblooms.org/sensory/tactile/clothing-tag-sensitivity
A-004: Fabric Refusal
Difficulty: Core | Textile Sensitivity Tools
→ techniques.pinnacleblooms.org/sensory/tactile/fabric-refusal
→ techniques.pinnacleblooms.org/sensory/tactile/fabric-refusal

A-021: Child Avoids Hugs (Peer-Focused)
Difficulty: Core | Social Touch Tools
"You already own materials for this" ✅
→ techniques.pinnacleblooms.org/sensory/tactile/child-avoids-hugs
"You already own materials for this" ✅
→ techniques.pinnacleblooms.org/sensory/tactile/child-avoids-hugs

A-024: Light Touch Defensiveness
Difficulty: Advanced | Graded Tactile Tools
→ techniques.pinnacleblooms.org/sensory/tactile/light-touch-defensiveness
→ techniques.pinnacleblooms.org/sensory/tactile/light-touch-defensiveness

A-025: Child Seeks Deep Pressure
Difficulty: Core | Deep Pressure and Proprioceptive
→ techniques.pinnacleblooms.org/sensory/tactile/child-seeks-deep-pressure
→ techniques.pinnacleblooms.org/sensory/tactile/child-seeks-deep-pressure
One Technique, One Piece of the Whole Picture
Touch aversion affects far more than touch. When your child tolerates physical contact, it unlocks progress across their entire developmental landscape — social connection, self-care, play, and family wellbeing all shift in response.
Where This Technique Lives
Domain A (Sensory) → Subdomain: Tactile → Cluster: Touch Tolerance → Technique A-002
The Ripple Effect
Touch tolerance improvements send ripples into Social-Emotional (C) — connection and belonging; Adaptive Self-Care (F) — grooming and dressing; Play Skills (G) — peer interaction; and Family Wellbeing (K) — parental confidence and relationship quality.
Source: WHO/UNICEF Nurturing Care Framework (2018) — Holistic developmental monitoring | UNICEF 2025 Country Profiles

Real Families. Real Progress. Real Hope.
Arjun's Mother — Hyderabad Center
Before: "Arjun would scream if anyone touched him. Getting dressed was a 45-minute battle. I couldn't remember the last time he let me hold him."
After (Day 68): "He climbed into my lap during a movie. He stayed for 12 minutes. I didn't move. I didn't breathe. I just held him."
Priya's Father — Bangalore Center
Before: "Priya would wipe off kisses immediately. She sat at the far end of the couch, always. We communicated through a 3-foot gap."
After 8 weeks: "She now chooses 'side hug' from her touch cards every morning before school. She picks the card, brings it to me, and leans in. It's the best 5 seconds of my day."
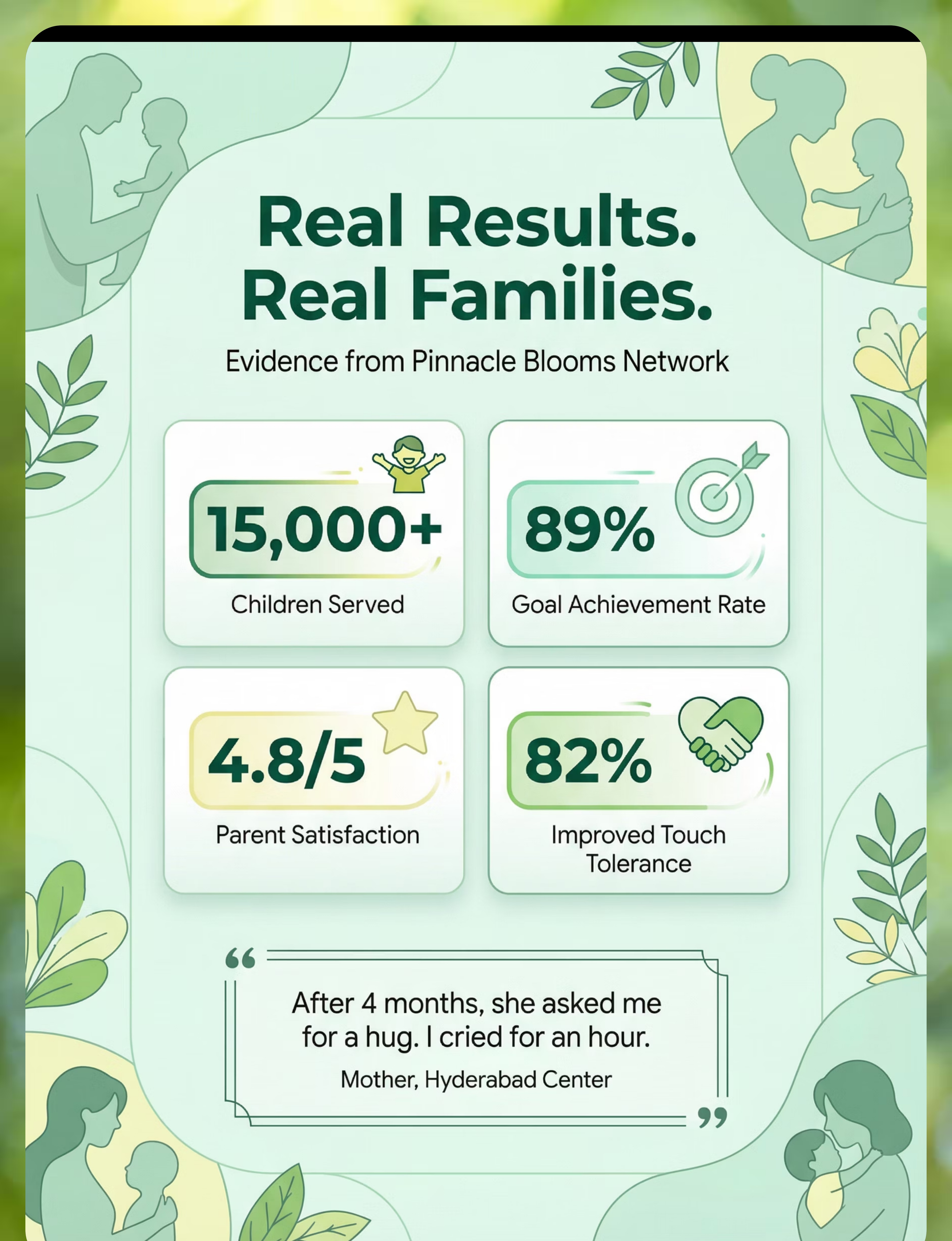
"After 4 months, she asked me for a hug. I cried for an hour."
82%
Showed Measurable Improvement
Of children in the touch tolerance protocol within 8–12 weeks across the Pinnacle Network
15,000+
Children Served
Across the Pinnacle Blooms Network in touch tolerance and sensory integration programs
4.8/5
Parent Satisfaction
Average rating from families completing the touch tolerance protocol
You're Not Alone on This Journey
The families who have walked this path before you are waiting to help. Every parent community below was built for one purpose: so that no caregiver navigates this alone at 2 a.m., searching for answers on their phone.
WhatsApp Parent Group
"Sensory Solutions — Touch Tolerance" — Join parents navigating the same challenge. Share wins, ask questions, find encouragement in real time. Managed by Pinnacle community moderators.
Online Community Forum
Connect with thousands of families across India and worldwide navigating tactile sensitivity. → pinnacleblooms.org/community/tactile-sensitivity
Local Parent Meetups
Find families near you through your local Pinnacle Blooms center. Monthly parent support groups in 40+ cities across India. → pinnacleblooms.org/centers
Peer Mentoring Program
Connect with a parent who has completed this exact protocol. They've been precisely where you are right now. → pinnacleblooms.org/peer-mentor
"Your experience helps others. When you're ready, consider sharing your journey — it might be the hope another parent needs tonight."
Home + Professional Guidance = Maximum Impact
75+ Centers
40+ Cities
500+ Therapists
OT • SLP • ABA • Physio
Home-based intervention is powerful — and it works best when backed by professional clinical guidance. Your therapist can fine-tune this protocol to your child's specific sensory profile, caught nuances that no webpage can anticipate.
Find Your Nearest Center
Enter your city to find your closest Pinnacle Blooms center, assessment availability, and specialist roster.
→ pinnacleblooms.org/centers
→ pinnacleblooms.org/centers
Book an OT Consultation
For Technique A-002, your primary discipline is Occupational Therapy specializing in sensory integration.
→ pinnacleblooms.org/book-ot
→ pinnacleblooms.org/book-ot
Teleconsultation
Can't visit a center? Book a video consultation with a Pinnacle OT from anywhere in the world — urban or rural, India or international.
→ pinnacleblooms.org/teleconsult
→ pinnacleblooms.org/teleconsult
Insurance and Funding
Contact your local center for insurance partnership details, government scheme eligibility, and financial support options available in your state.
Source: WHO NCF Progress Report (2023) — Primary health care as platform for reaching all families with ECD interventions
Deeper Reading for the Curious Parent
Every claim on this page is grounded in peer-reviewed evidence. If you want to go deeper — or share the science with a skeptical co-parent, teacher, or physician — this is your reference library.
Study 1 — Level I Systematic Review (2024)
"Sensory Integration Intervention for Children with Autism: A PRISMA Systematic Review" — 16 studies, 2013–2023. Confirms SI intervention as evidence-based practice for ASD, with significant improvements in tactile processing, social skills, and adaptive behavior.
→ PubMed: PMC11506176 | Children (2024)
→ PubMed: PMC11506176 | Children (2024)
Study 2 — Level I Meta-Analysis (2024)
"Sensory Integration Therapy for ASD: A Meta-Analysis" — 24 studies. Significant improvement in social skills, adaptive behavior, sensory processing, and motor skills. Individual (1:1) sessions were most effective.
→ PubMed: PMC10955541 | DOI: 10.12998/wjcc.v12.i7.1260
→ PubMed: PMC10955541 | DOI: 10.12998/wjcc.v12.i7.1260
Study 3 — Level II Indian RCT (2019)
Padmanabha et al., "Home-Based Sensory Interventions for Children with ASD." Indian context, parent-administered, significant outcomes — establishing feasibility and efficacy for Indian families specifically.
→ DOI: 10.1007/s12098-018-2747-4 | Indian Journal of Pediatrics
→ DOI: 10.1007/s12098-018-2747-4 | Indian Journal of Pediatrics
Study 4 — WHO Nurturing Care Framework (2018)
Global framework for integrated early childhood development. Responsive caregiving as core component. Caregiver-mediated interventions using household materials across 54 low- and middle-income countries.
→ nurturing-care.org/ncf-for-ecd | PMC9978394
→ nurturing-care.org/ncf-for-ecd | PMC9978394
Foundational Texts
- Ayres, A. Jean. Sensory Integration and the Child (25th Anniversary Edition)
- Wilbarger, P. and Wilbarger, J. Sensory Defensiveness in Children Aged 2–12 (1991)
- AOTA Sensory Integration Intervention Guidelines — aota.org
- NCAEP Evidence-Based Practices Report (2020)
GPT-OS® — The Intelligence Behind Your Child's Protocol
Powered by GPT-OS®
21 Million+ Sessions
HIPAA-Aligned Privacy
Every session you record feeds a clinical intelligence system that gets smarter with every data point — and returns that intelligence to your child as personalized guidance.
What GPT-OS® Learns from A-002 Data
- Which materials produce the fastest regulation for YOUR child
- Optimal session timing — when your child's touch tolerance peaks
- Progression pace recommendations — when to advance, when to consolidate
- Cross-technique connections — which related techniques to explore next
Privacy and Data Protection
- All data encrypted in transit and at rest
- HIPAA-aligned privacy standards
- Your data is never sold or shared with third parties
- You control your data — delete anytime
"Your data helps every child like yours. Every session you record makes the next family's journey a little shorter." Source: Digital health + ASD systematic reviews (2024) — 21 RCTs, 1,050 participants

See It in Action — Sensory Solutions Episode 2
Reel ID: A-002
Duration: 60 Seconds
Series: Sensory Solutions — Episode 2
What the Reel Shows
Watch a Pinnacle Blooms Occupational Therapist demonstrate each of the 9 materials with a child — showing correct technique, pressure application, body positioning, and the child's responses in real time.
This technique page expands on the Reel with the full 40-card clinical protocol. The Reel shows you the "what." This page gives you the "how" and "why."
Related Reels in This Series
- → A-001: 9 Materials for Touch Sensitivity (General)
- → A-003: 9 Materials for Clothing Tag Sensitivity
- → A-021: 9 Materials When Child Avoids Hugs
Find all Sensory Solutions Reels at → pinnacleblooms.org/reels
Why Video Matters: NCAEP (2020) identifies video modeling as an evidence-based practice for autism. Multi-modal learning — reading AND watching — improves parent skill acquisition and technique fidelity significantly over text alone.
Consistency Across Caregivers Multiplies Impact
If only one caregiver executes the technique, it is limited. When grandparents, teachers, and all caregivers understand — the child's world becomes consistently safe. Share this page today.
📱 WhatsApp
Share this page with one tap. Send to co-parents, grandparents, teachers, or anyone in your child's life.
techniques.pinnacleblooms.org/sensory/tactile/child-hates-being-touched
techniques.pinnacleblooms.org/sensory/tactile/child-hates-being-touched
📋 Family Guide PDF
The 9 materials, safety rules, and session steps on one printable page for the whole family.
→ pinnacleblooms.org/guides/A-002-family-guide
→ pinnacleblooms.org/guides/A-002-family-guide
👵 Grandparent Version
A simplified, culturally sensitive summary: "[Child's name] finds being touched overwhelming — not because they don't love you, but because their nervous system processes touch differently. Use firm, announced touch (not light or surprise). Give them a weighted blanket during lap time. Let them come to you. Every high-five is a hug in progress."
🏫 Teacher Communication Template
A one-paragraph letter for school explaining your child's touch needs and the strategies that help — ready to send to class teachers, PE teachers, and school counselors.
Source: WHO CCD Package — Multi-caregiver training for intervention generalization | PMC9978394
Frequently Asked Questions
These are the questions parents ask most often — in clinics, in parent groups, in teleconsultations, and at 2 a.m. when the worry won't stop. Here are honest, clinical answers.
Q: How long until my child accepts hugs?
Every child is different. Across the Pinnacle network, most families see measurable improvement within 8–12 weeks of consistent daily sessions. Some children accept brief hugs by week 6; others take 4–6 months. The pace is your child's — not a calendar's.
Q: What if my child can only tolerate the weighted blanket and nothing else?
That IS progress. The weighted blanket is regulating their nervous system. Stay with it. Many families spend 3–4 weeks exclusively on weighted blanket proximity before adding a second material. The blanket is the foundation — not a failure.
Q: My partner thinks I'm overthinking this. How do I explain?
Share Card 03 (the neuroscience card) with them. This is neurological, documented in peer-reviewed research, and addressed by the same clinical protocols used in 75+ Pinnacle Blooms centers. You're not overthinking — you're parenting with precision.
Q: Can I do these activities during regular play or do I need formal sessions?
Both work. Formal sessions accelerate progress. But leaving the weighted blanket on the couch during TV time, or incorporating heavy work into chores, creates "stealth therapy" throughout the day. Integration is the ultimate goal.
Q: Is the Wilbarger Brushing Protocol safe to do at home?
ONLY with professional OT training. The Wilbarger Protocol requires a specific brush type, precise pressure, exact body regions, and correct frequency. Incorrect application can increase defensiveness. Book an OT consultation at pinnacleblooms.org/book-ot.
Q: What if touch aversion gets worse before it gets better?
This can happen — it's called a "sensory spike" or "extinction burst." When the nervous system is challenged by new input, it sometimes overreacts before recalibrating. If worsening persists beyond 1–2 weeks, consult your OT immediately.
Q: My child tolerates touch from the therapist but not from me. Why?
Therapists use precise, predictable, professional touch patterns. Your touch carries emotional weight, expectation, and natural unpredictability. This is not a reflection of your relationship — it's sensory processing. The techniques on this page help you achieve therapist-level touch delivery.
Q: Where can I find all 9 materials? I'm in a small town.
Card 10 provides zero-cost household substitutes for 8 out of 9 materials. The only material requiring purchase is the Wilbarger brush (which also requires OT training). Every family can start today with what they have at home — right now.
Didn't find your answer? → Ask GPT-OS®: gpt-os.pinnacleblooms.org/ask → Book a teleconsultation: pinnacleblooms.org/teleconsult

You've Read the Science. You Have the Materials. Your Child Is Waiting.
Every session is a bridge. Every repetition is a plank. Every moment of patience is the railing your child holds as they cross toward you.
You now have everything you need: the neuroscience, the materials, the step-by-step protocol, the safety guidelines, the troubleshooting guide, and the evidence behind every decision. The only thing left is to begin.
🟢 Start This Technique Today
Launch a GPT-OS® guided session with step-by-step prompts, built-in timer, and automatic data logging. The intelligence adapts to your child from session one.
→ gpt-os.pinnacleblooms.org/start/A-002
📅 Book a Consultation
Connect with a Pinnacle Blooms Occupational Therapist for a personalized sensory profile assessment and custom protocol design.
→ pinnacleblooms.org/book
🔗 Explore the Next Technique
A-003: 9 Materials for Clothing Tag Sensitivity — the natural next step for many families completing A-002.
→ techniques.pinnacleblooms.org/sensory/tactile/clothing-tag-sensitivity
✅ Validated by the Pinnacle Blooms Consortium
OT • SLP • ABA • SpEd • NeuroDev • CRO
Preview of 9 materials that help when child hates being touched Therapy Material
Below is a visual preview of 9 materials that help when child hates being touched therapy material. The pages shown help educators, therapists, and caregivers understand the structure and content of the resource before use. Materials should be used under appropriate professional guidance.









Link copied!

The Pinnacle Promise
🤚 OT
🗣️ SLP
🧠 ABA
📚 SpEd
⚕️ NeuroDev
🔬 CRO
"From fear to mastery. One technique at a time."
The Pinnacle Blooms Consortium — spanning Clinical Research Organization scientists, Pediatric Occupational Therapists, Speech-Language Pathologists, Board Certified Behavior Analysts, Special Educators, and NeuroDevelopmental Pediatricians — has invested in this knowledge so that no parent has to figure it out alone.
Medical Disclaimer
This content is educational and does not replace assessment by a licensed occupational therapist. If your child has significant touch aversion, please consult a qualified professional. Individual results may vary. Statistics represent aggregate outcomes across the Pinnacle Blooms Network. The Wilbarger Protocol requires professional training — never attempt without guidance.
Copyright and Attribution
© 2026 Pinnacle Blooms Network. All rights reserved. Content developed by the Pinnacle Blooms Consortium — CRO, OT, SLP, BCBA, SpEd, NeuroDevelopmental Pediatrics. Powered by GPT-OS® Therapy Intelligence. Published at techniques.pinnacleblooms.org.
Navigate
The Loop — Coming Next in A-003: "She screams when I try to put on her school uniform..."