When every other child runs toward the swings — and yours runs the other way.
You tried placing him gently on the baby swing, thinking he'd relax once he experienced it. He screamed like you were hurting him. His knuckles went white gripping the chains. Twenty minutes to stop shaking. You haven't been near the swing area since. This is not defiance. This is your child's vestibular system sending genuine danger signals.
🌿Pinnacle Blooms Network® | Occupational Therapy • ABA/BCBA • SLP • SpEd • NeuroDev Pediatrics | FREE Helpline: 9100 181 181
You are among millions of families navigating this exact challenge.
80%
Sensory Difficulties
of children diagnosed with autism experience sensory processing difficulties including vestibular hypersensitivity. PRISMA Systematic Review, 2024 | PMC11506176
1 in 6
General Population
children show some degree of sensory processing difficulty affecting daily participation. Sensory Processing Research Consortium | CDC
Top 5
Swing Fear Ranking
Swing fear is among the top 5 reported sensory avoidance behaviors by parents across Pinnacle centers in India. Pinnacle GPT-OS® Clinical Data | 20M+ sessions
Vestibular hypersensitivity and gravitational insecurity are not rare. They are not overreactions. They are a documented neurological processing pattern affecting millions of children across India and 70+ countries. Your child is not the only one who runs from what others race toward.
📚Citations: PMC11506176 | PMC10955541 | DOI: 10.12998/wjcc.v12.i7.1260 | Pinnacle Clinical Data 2024

The vestibular system is not misbehaving. It is over-responding.
The Science
The vestibular system lives in your child's inner ear. Its job: detect head position and movement, keep the body oriented in space, and signal "safe" or "danger" based on what it feels.
For children with vestibular hypersensitivity, swinging triggers a genuine DANGER response — identical to the signal the brain sends when you're about to fall off a cliff.
Plain English
This is not a behavioral choice. This is not a tantrum. This is not "being difficult." This is a wiring difference in how sensory input is processed — the same movement registers as completely different threats in different nervous systems.
The technical terms: Vestibular Hypersensitivity and Gravitational Insecurity — the profound unease when feet leave the ground and the body must trust something other than solid earth.
🧠"Wiring difference, not behavior choice." The child cannot will themselves out of this response any more than they can will away a fever. The nervous system needs to be gently re-taught that movement is safe. DOI: 10.3389/fnint.2020.556660 | Frontiers in Integrative Neuroscience (2020)
Your child is not behind. They are at a waypoint — with a clear path forward.
Birth – 6 Months
Vestibular reflexes and head righting emerge
12 Months
Walking and balance begin
2 Years
Playground exploration begins
★ Ages 3–7
The Vestibular Integration Window — swing tolerance builds through graduated exposure
8+ Years
Full vestibular integration matures
Ages 2–10: The Vestibular Integration Window. This is when the brain is most plastic and most responsive to graduated vestibular input. Intervention NOW — even gentle home-based intervention — produces the most durable outcomes.
Children with swing fear often also show: motion sickness in cars/boats/elevators, preference for feet-firmly-on-ground activities, avoidance of being picked up or "swung" by adults, and possible sensitivity to other sensory input. These co-occurring patterns are expressions of the same underlying vestibular processing difference — not separate problems.
📚 PMC9978394 | WHO/UNICEF Care for Child Development Package (2023) | WHO Milestones Framework

This approach is not intuitive guesswork. It is evidence-graded clinical science.
LEVEL I–II EVIDENCE
Systematic Review + RCT Support
Sensory Integration Interventions for Vestibular Hypersensitivity
Clinically validated. Home-applicable. Parent-proven.
Key Evidence Summary
Study | Finding | |
PRISMA Review 2024 (PMC11506176) | 16 studies confirm sensory integration is evidence-based practice for ASD | |
Meta-Analysis WJCC 2024 (PMC10955541) | 24 studies confirm SI therapy effectiveness across behavior, motor, sensory | |
Indian RCT Padmanabha 2019 | Home-based sensory interventions show significant outcomes in Indian pediatric populations | |
NCAEP Evidence Report 2020 | Visual supports and graduated exposure classified as evidence-based practices |
📞FREE National Autism Helpline: 9100 181 181 — Available in 16+ languages. Our specialists explain this evidence in your language.

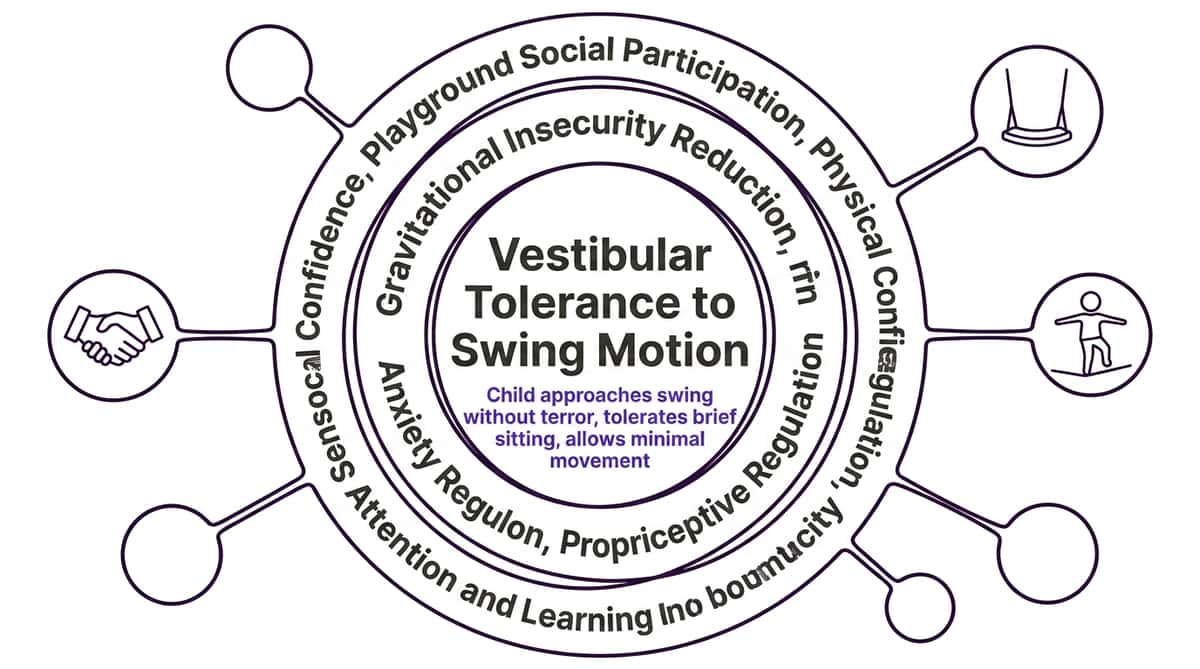
Graduated Vestibular Desensitization via Therapeutic Swing Materials
Parent alias: "Building Swing Safety Step by Step"
A structured, multi-material approach to treating vestibular hypersensitivity and gravitational insecurity in children aged 2–10 years. The technique uses 9 categories of therapeutic materials — each carefully selected to provide vestibular input at progressively increasing challenge levels — to systematically recalibrate the child's nervous system response to movement. Unlike forced exposure (which traumatizes), this approach starts well below the child's fear threshold and advances only when the child signals readiness.
🧠 Domain A
Sensory Processing
🌀 Vestibular
System
⚠️ Gravitational
Insecurity
🏃 Motor
Development
💚 Anxiety
Reduction
Age Range: 2–10 years | Session Duration: 10–20 minutes | Frequency: Daily or 3×/week minimum
Setting: Home + Playground + Therapy Room | Lead Discipline: Occupational Therapy (OT)

Five therapy disciplines converge on this one challenge. Here is how each contributes.
Occupational Therapy — PRIMARY LEAD
OT therapists design and deliver the core vestibular integration protocol. They assess the child's sensory profile, identify the exact threshold of tolerance, and prescribe the graduated exposure hierarchy. They select which swing types to use in which order.
Applied Behavior Analysis (ABA/BCBA)
Designs the reinforcement strategy for each step. Tracks behavioral data — approach distance, tolerance duration, distress indicators — to objectively measure progress. Develops the token economy for celebrating each tiny step forward.
Neurodevelopmental Pediatrics
Rules out medical causes of vestibular dysfunction. Coordinates with ENT if indicated. Prescribes clinical intensity and frequency of intervention. Monitors developmental trajectory within the GPT-OS® diagnostic framework.
Special Education
Adapts school environment to accommodate swing fear — recess planning, playground support. Prepares teachers with appropriate language and approach protocols. Ensures the child's playground participation is not further impaired by peer pressure or adult-initiated forcing.
"The brain doesn't organize by therapy type. Swing fear involves sensory processing (OT), behavioral response (ABA), neurological function (NeuroDev), and social participation (SpEd). We treat the whole child." — Pinnacle Blooms Consortium, Clinical Leadership
This is a precision approach. Here is exactly what it rebuilds.
Stage | Observable Milestone | |
Week 1–2 | Child doesn't immediately bolt when entering swing area | |
Week 3–4 | Child touches swing chain without pulling away | |
Week 5–6 | Child sits on still swing for 5–10 seconds | |
Week 7–8 | Child tolerates 1–2 seconds of gentle movement | |
Week 10–12 | Child chooses supported swinging as an activity |
📚 PMC10955541 | World J Clin Cases Meta-Analysis (2024)

9 Materials. Each addresses a different layer of the fear. Used in graduated sequence.
Material Overview
Lap Sitting Swings
Safety of a trusted body while moving — platform, nest, saucer, tire swings
Enclosed Cocoon Swings
Contained movement in a safe, bounded, womb-like space
Ground-Level Movement Equipment
Vestibular input with feet near the floor — the essential foundation
Bolster Swings
Stable body position, entirely different movement experience — prone position
Infant/Toddler Bucket Swings
Complete containment — impossible to fall
Visual Supports and Social Stories
Preparing the mind before the body
Gradual Approach Hierarchy Materials
Tiny visible steps — the architecture of courage
Proprioceptive Preparation Materials
Grounding the body before movement challenge
Adaptive and Platform Swings
Wide, stable, flexible positioning — beyond the belt swing
✅Clinically validated material selection per GPT-OS® Vestibular Processing Protocol
Material 1: Lap Sitting Swings
Safety of a trusted body while moving
The standard swing position — seated alone, feet dangling — represents maximum vulnerability. Lap sitting swings allow the child to experience swinging while completely held by a trusted adult. The adult's body is the stable reference point. The nervous system processes movement in a zero-threat context. This is often the very first elevated swing exposure a fearful child can tolerate.
Clinical Grade
Types: Platform swings • Nest/saucer swings • Tire swings • Therapy platform swings
Price: ₹2,000–8,000
🛠 DIY Version (₹0)
Use existing tire swings or saucer swings at your local playground that are wide enough for two. Start with child facing you, chest-to-chest, for maximum security. Standard belt swings do NOT work for lap sitting.

Material 2: Enclosed Cocoon Swings
Contained movement in a safe, bounded space
Open space can be as terrifying as the movement itself. Cocoon swings provide a contained, womb-like space that moves. The fabric sides offer visual and physical boundaries, deep pressure through enclosure, and a sense of "inside" rather than "floating in space." Many children who refuse standard swings will tolerate cocoon swings immediately — the enclosure removes a major layer of the threat signal.
Clinical Grade
Types: Therapy cocoon swings • Pod swings • Lycra sensory swings • Cuddle swings
Price: ₹3,000–12,000
🛠 DIY Version (₹200–500)
Place a large piece of soft Lycra fabric (from any fabric store) inside a standard swing, bunching it up around the child's body. Not identical to purpose-built versions but provides the containment principle. The therapeutic goal is genuine deep pressure — not just visual enclosure.
Material 3: Ground-Level Movement Equipment
Vestibular input with feet near the floor — the essential foundation
Before any elevated swing attempt, the nervous system needs to learn that movement is safe at ground level. Balance boards, wobble cushions, sit-and-spin toys, and rocking toys provide genuine vestibular input while keeping the child's feet near the floor. This builds the vestibular tolerance foundation that eventually supports swing tolerance. This is where most children begin — and where they spend the first several weeks.
Clinical Grade
Types: Balance boards • Wobble cushions • Sit-and-spin toys • Rocking chairs • Balance pods
Price: ₹500–3,000
🛠 DIY Version (₹0)
A firm couch cushion on the floor as a wobble surface. A spinning office chair for controlled rotational input. A wooden board placed on a rounded object for a balance board effect. Rocking in a rocking chair. All zero cost.

Material 4: Bolster Swings
Stable body position, entirely different movement experience
The traditional upright swing position may be uniquely threatening. Bolster swings allow the child to lie across or straddle a padded cylinder — providing more body surface contact, more proprioceptive input through the torso, and a fundamentally less threatening visual field. Many children who cannot tolerate upright swinging manage bolster swings immediately because the prone position changes the entire sensory experience.
Clinical Grade
Types: Therapy bolster swings • Padded cylinder swings • Barrel-style swings
Price: ₹2,500–8,000
🛠 DIY Version (₹300–800)
A large, firm, tightly-stuffed cylindrical pillow (yoga bolster or DIY fabric roll) suspended at very low height from a door frame or patio beam using strong rope. Keep very low — 15–20cm off ground initially. Ensure weight capacity is tested thoroughly.

Material 5: Infant/Toddler Bucket Swings
Complete containment — impossible to fall
Even for older children, returning to the full containment of a bucket swing can provide the maximum safety signal a nervous system on high alert needs. Surrounded on all sides, unable to fall, the child receives constant physical evidence of being completely held. For children whose fear includes the possibility of falling, this addresses that fear at the most fundamental neurological level.
Clinical Grade
Types: High-back bucket swings • Full-support adaptive swing seats • Toddler bucket swings with extended weight capacity
Price: ₹1,000–4,000
🛠 DIY Note
Bucket swings are not easily DIY'd safely. If purchasing is not possible, a basket/hammock chair with deep sides suspended very low from a beam can approximate the containment principle. Safety first — always supervise. This is the one material where clinical-grade is strongly preferred.

Material 6: Visual Supports and Social Stories
Preparing the mind before the body
Swing fear includes anticipatory anxiety — the child becomes afraid before approaching swings. Visual supports prepare the child cognitively and emotionally. Social stories explain what will happen ("We will look at swings. You can hold my hand. You can say stop."). Visual schedules show the gradual approach steps. Photos of the specific playground reduce uncertainty. The prefrontal cortex stays online; fight-or-flight is less likely to hijack the approach.
Clinical Grade
Types: Social story templates • Custom photo books • Visual sequence cards • Stop/Go signals
Price: ₹100–2,000
Search "social story autism swing" → Teachers Pay Teachers / Pinterest
🛠 DIY Version (₹0)
Take 4–5 photos of your actual local playground swings. Create a simple booklet: "The Swings at [Park Name]. Sometimes we look at them. Sometimes we touch them. We always decide together. I am safe. Mummy/Daddy is here." Laminate or put in a clear sleeve. Read before every playground visit.
Material 7: Gradual Approach Hierarchy Materials
Tiny visible steps — the architecture of courage
Terror does not respond to flooding or logic. It responds to hundreds of tiny positive experiences that teach the nervous system that movement is not danger. Hierarchy materials make this invisible internal process visible and manageable — a step ladder from distant observation to eventual swinging, with each step practiced until comfortable before advancing. Progress becomes visible. The child controls the pace.
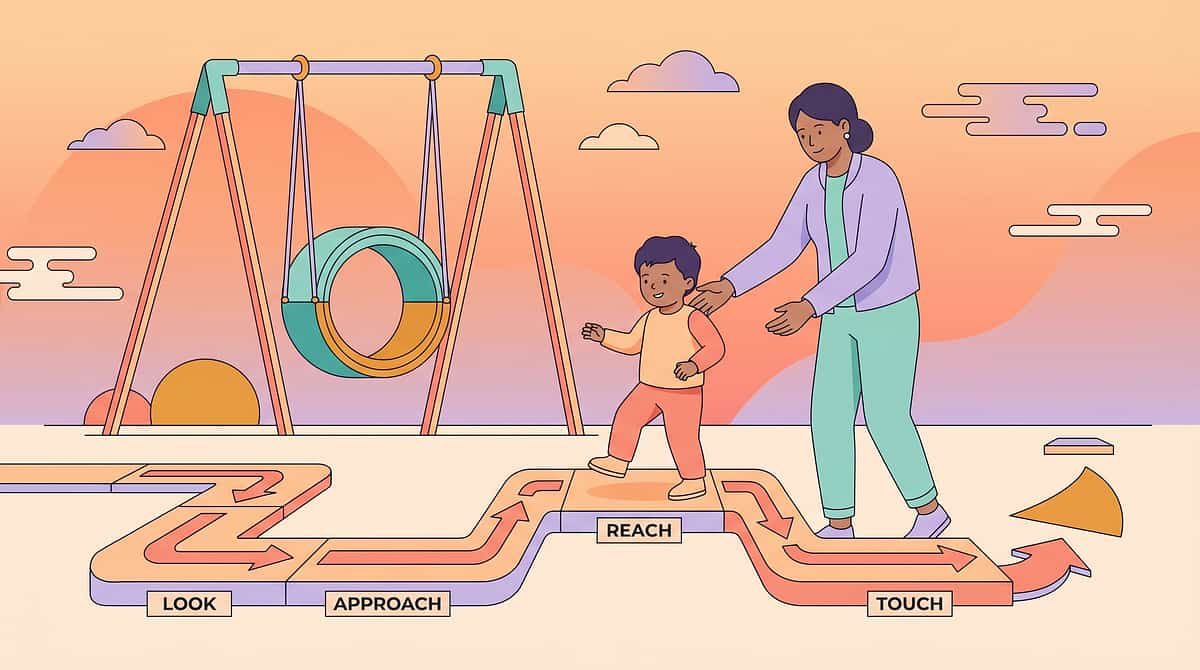
Steps 1–3: Observe
Look at swings from the gate → Walk to within 5m → Walk to swing and touch chain
Steps 4–6: Sit
Sit on still swing 3 seconds → Sit 10 seconds → One barely-perceptible push
Steps 7–10: Move
Three gentle pushes → 30 seconds swinging → 1 minute → Child chooses to swing ⭐
⚠️NEVER skip steps. NEVER rush. Each step may take days or weeks. That is correct. Put a gold star sticker on each completed step. Canon products: Reward Stickers ₹399 | Reward Jar
Material 8: Proprioceptive Preparation Materials
Grounding the body before movement challenge
Proprioceptive input — deep pressure, heavy work, joint compression — calms and organizes the nervous system before vestibular challenge. When the body's proprioceptive system is well-fed, the vestibular system becomes less reactive. Think of proprioception as the anchor that allows the child to tolerate movement without alarm. Do 10 minutes of proprioceptive prep BEFORE every swing approach session.
Clinical Grade
Types: Weighted lap pads • Compression vests or shirts • Resistance bands • Body socks • Crash pads
Price: ₹500–4,000
🛠 DIY Version (₹0)
- 10 wall push-ups (press flat palms against wall, push hard)
- Carry a small backpack with 1–2 books inside
- 5 tight bear hugs from a parent
- Jump on a pillow or mattress 20 times
- "Sandwich" game: child lies on floor, parent presses firm pillow on top gently

Material 9: Adaptive and Platform Swings
Wide, stable, flexible positioning — because the belt swing is one design, not the only way to swing
Standard belt swings require a very specific, challenging body position: narrow seat, legs dangling, balance maintained independently. Platform swings offer alternatives: wide flat surfaces for sitting, lying, or kneeling; multiple holding points; space for an adult alongside. Many children reach platform swing tolerance months before they can manage traditional belt swings — and some may always prefer platform swings. That is completely valid.
Clinical Grade
Types: Therapy platform swings • Disc/saucer swings • Nest swings • Rectangular platform swings • Multi-person platform swings
Price: ₹3,000–15,000
🛠 DIY Version (₹500–1,500)
A large wooden board (60×60cm, sanded smooth) with four strong rope attachment points, suspended level from a sturdy overhead beam or outdoor structure. Test weight capacity thoroughly before use. Keep low — 15–20cm off ground — for initial introduction.
Material | Clinical Grade | DIY Cost | |
Lap Sitting Swings | ₹2,000–8,000 | ₹0 (use existing) | |
Cocoon Swings | ₹3,000–12,000 | ₹200–500 | |
Ground-Level Equipment | ₹500–3,000 | ₹0 | |
Bolster Swings | ₹2,500–8,000 | ₹300–800 | |
Bucket Swings | ₹1,000–4,000 | Not recommended | |
Visual Supports | ₹100–2,000 | ₹0 | |
Hierarchy Materials | ₹100–500 | ₹0 | |
Proprioceptive Materials | ₹500–4,000 | ₹0 | |
Platform Swings | ₹3,000–15,000 | ₹500–1,500 |

Every family can start today. Regardless of budget. Regardless of location.
🌍WHO/UNICEF equity principle: No child should be denied evidence-based intervention because of material cost. Every material in this protocol has a zero-cost equivalent. The therapeutic principle is what matters — not the brand. A child's nervous system cannot tell the difference between a ₹8,000 platform swing and a ₹800 DIY equivalent built with the same principle.
1. Visual Story
Phone photos of your local playground swings + 5 handwritten sentences
2. Approach Ladder
Hand-drawn staircase on a piece of paper — 10 steps, one star per step
3. Proprioceptive Prep
Wall push-ups, heavy carrying, tight hugs — zero cost, infinite value
4. Lap Sitting
Your own lap + any wide outdoor swing that fits two people
This is sufficient to begin. The clinical materials enhance the protocol but are not required to start.
When clinical-grade is non-negotiable: If the child has severe vestibular dysfunction, consult a sensory integration OT before using DIY vestibular equipment. Ensure DIY cocoon versions provide genuine deep pressure, not just visual enclosure. Suspension hardware for bolster swings must be professionally rated for weight. PMC9978394 | WHO NCF Handbook (2022)

Read this before every session. This is the safety gate.
🔴 RED — ABSOLUTE STOP
Child in heightened distress or post-meltdown recovery • Child is sick, feverish, or has active ear infection • Equipment has not been inspected today • Child is not giving consent (verbal or behavioral)
🟡 AMBER — MODIFY
Difficult morning but now regulated (reduce intensity 50%) • Child tired or hungry (shorten session, offer snack) • New/unfamiliar playground (add prep, start 2 steps back) • Another child previously pressured your child
🟢 GREEN — PROCEED
Child is fed, rested, regulated • Proprioceptive preparation complete • Visual story reviewed in past 24 hours • You have time and patience • Emergency exit plan is ready
⚠️STOP IMMEDIATELY IF: Skin color change (pallor or flushing) • Vomiting or nausea • Inconsolable crying 3–4+ minutes • Child reports dizziness • Child is begging to stop. NEVER FORCE A CHILD WITH SWING FEAR ONTO A SWING. Not even for one second. Forced exposure confirms to the nervous system that swings ARE dangerous, sensitizes the system, and destroys trust. It can set progress back by months. Always. Child-led. Always.

The right environment prevents 80% of session failures before they start.
Starting Position
Child starts 10+ meters from swing. Parent immediately beside, not blocking. Comfort object within reach.
Visual Tools Ready
Hierarchy card in parent's hand or pocket. Visual story reviewed in past 24 hours.
Reinforcement Prepared
Reward in parent's pocket, accessible within 3 seconds of target behavior.
Exit Direction Clear
Child knows where "all done" leads — removes uncertainty from ending the session.
Environment Checklist
- Session: 10–20 minutes maximum (not negotiable)
- Timing: when child is typically most regulated
- Off-peak playground for initial sessions
- Low sound level — avoid unpredictable noise
- Phone on silent — your full attention is required
Parent Body Language
Position at child's level (crouch or kneel). Open, sideways body position — NOT facing the swing. Relaxed shoulders. Slow breathing.
Your nervous system is contagious — a calm parent calms a dysregulated child.
60 seconds before every session. The best session starts right.
Readiness Check
✅ Child has eaten in last 2 hours
✅ Child is not showing signs of illness (fever, ear discomfort, unusual crying)
✅ Child has had proprioceptive preparation (wall pushes, heavy carrying, tight hugs)
✅ Child is in a regulated state — not currently mid-meltdown or in recovery
✅ Visual story/schedule has been reviewed
✅ No major stressors in the last 30 minutes
✅ Child is aware this is a "swing practice day" — NO surprises, EVER
Checkmarks | Decision | Action | |
All 7 ✅ | GO | Proceed to full protocol | |
5–6 ✅ | MODIFY | First 3 hierarchy steps only, 5 minutes max | |
4 or fewer ✅ | POSTPONE | Do proprioceptive play instead. Tomorrow. |
"The best session is one that starts right. A postponed session is a gift to tomorrow's progress."

Step 1
The Invitation
Every session begins with an invitation. Never a command. Never a surprise.
"Hey, do you want to come see the swings with me? We don't have to do anything — just look. I'll be right here."
Body Language Guidance
- Crouch to child's eye level
- Open, relaxed body — do NOT point toward swings
- Offer hand (don't grab)
- Smile with your eyes, not performatively
- Speak at 60% of your normal volume
If Resistance
Do NOT push through. Today's goal may simply be "We walked to the playground gate." Celebrate it specifically:
"You came to the playground today. That was brave. Well done."
Acceptance indicators: child takes your hand, takes a step toward playground, makes eye contact, or even just a body turn toward the swings. Any of these is "yes." | Timing: 30–60 seconds

Step 2
The Engagement
The child is moving toward the challenge. Meet them where they are. Check your approach ladder — what step are you on TODAY? Do ONLY that step. Not the next one. Not "just a little more."
Match Their Pace
Do not walk ahead toward the swings. Let the child lead the approach speed entirely.
Narrate Calmly
Don't over-explain or over-encourage: "We're walking closer to the swings. You're doing it."
Notice and Name
What the child IS doing — not what you want them to do: "You touched the chain! You touched it!"
Stay Regulated
If you feel excitement or anxiety about whether they'll do more, they can feel it. Breathe.
"This is the [swing name]. See how it [describe one feature: wide/soft/enclosed/still]. You can touch it if you want. You can just look. You are in charge."
The moment the child does ANY part of the current hierarchy step — even partially — deliver praise within 3 seconds. Specific, calm, genuine: "You walked all the way to the swing. That's brave." | Timing: 1–3 minutes

Step 3
The Therapeutic Action
The main therapeutic event. This is where the nervous system does its learning. The child receives vestibular input that is just tolerable — not comfortable, not terrifying — and the nervous system registers: "I survived that movement. It was okay." This micro-registration, repeated hundreds of times, is how vestibular tolerance is built.
Lap Sitting Swing
Child on lap on platform swing. NO movement initially. If tolerates 30 seconds, one barely-perceptible push (2–3cm). STOP. "Was that okay?"
Cocoon Swing
Child climbs in. Hold still. No movement until child signals readiness. First movement: gentle rocking of 5cm amplitude.
Ground Equipment
Child on balance board. You do NOT control movement — child initiates all movement. Be present, narrate positively, ensure safety.
Bolster Swing
Child drapes over bolster prone. Hold still initially. First movement: side-to-side weight shift 5–10cm. Duration: 30 seconds before checking in.
❌ Moving swing without checking first ❌ Letting movement increase because "they seem fine" ❌ Talking constantly ❌ Looking at your phone ❌ Letting other children approach during this session | Timing: 2–5 minutes
Step 4
Repeat and Vary
Three good repetitions are worth more than ten forced ones. For vestibular work with fearful children: 2–4 repetitions per session at the current hierarchy step, with a clear stop between each. More than 4 repetitions often overwhelms before you see it — the nervous system needs processing time between exposures.
Change the Social Element
Same swing, parent position changes (facing/beside)
Change the Object
Comfort toy vs. nothing during the swing experience
Change the Communication
Silent swinging vs. "I'm going to count to 3, then stop"
Change the Reward
Sticker chart vs. verbal praise vs. preferred activity after
These variations maintain interest WITHOUT increasing the vestibular challenge itself. Vestibular intensity increases ONLY when the child explicitly signals readiness.
"Three repetitions where the child felt SAFE are worth infinitely more than eight repetitions where the child felt overwhelmed but complied. The quality of each vestibular experience determines what the nervous system learns." — Pinnacle OT Clinical Guidelines
Satiation indicators: Increased distraction • Looking away • Reduced engagement • Slight increase in body tension • Requests for "all done" (ALWAYS honor immediately) • Yawning or drooping. | Timing: 3–5 minutes
Step 5
Reinforce and Celebrate
Timing matters more than magnitude. Celebrate the attempt, not just the outcome. The moment the child does ANY part of the current hierarchy step — not the whole step, not the next step, ANY part — deliver reinforcement within 3 seconds.
Child Behavior | Your Response Script | |
Approached the swing area | "You came to the swings today. That took courage." + sticker | |
Touched the swing chain | "You TOUCHED it! Your hand touched the swing!" + enthusiastic but calm | |
Sat on still swing 3 seconds | "You sat on the swing! You did it! How did that feel?" + big sticker on chart | |
Tolerated one gentle push | "You stayed on. One whole push. I'm so proud of your brave body." + preferred reward | |
Asked to stop and you stopped | "I heard you say stop and I stopped. You can always say stop." + praise for self-advocacy |
✅ Celebrate the ATTEMPT
"You tried. That matters."
✅ Celebrate the STEP
"You got to Step 4 today."
❌ Do NOT Say
"You'll try MORE next time!" — adds pressure
"That wasn't so bad, was it?" — minimizes the real effort the child expended
Canon products: Sticker reward chart | Reward jar with tokens | Verbal praise (always free, always powerful when specific)

Step 6
The Cool-Down
No session ends abruptly. The transition is part of the therapy. A predictable ending reduces resistance and helps the nervous system process what it just learned.
"Two more swings, then we're all done for today."
If Child Resists Ending (Wants More)
"I know you want more! That makes me so happy that you want to swing more. We're done for today so your brave brain can rest. Tomorrow we can do it again."
Do not extend the session beyond plan — the brain needs recovery time to consolidate what it learned.
If Child Is Upset at Ending
Normalize: "It's okay to feel sad it's done. It means you liked it. Let's get a sticker for the chart."
Visual timer used throughout session — child can see remaining time. Predictability reduces resistance.
📚 NCAEP Evidence-Based Practices Report (2020) | Visual timer evidence | Transition support for autism
60 seconds. Right now. While it's fresh. This data drives next session's plan.
Data Point 1
Hierarchy Step Achieved Today (1–10)
Which numbered step did the child reach? Circle: 1 — 2 — 3 — 4 — 5 — 6 — 7 — 8 — 9 — 10
Which numbered step did the child reach? Circle: 1 — 2 — 3 — 4 — 5 — 6 — 7 — 8 — 9 — 10
Data Point 2
Maximum Swing Tolerance Duration
Longest time the child tolerated the current swing type without distress: _____ seconds
Longest time the child tolerated the current swing type without distress: _____ seconds
Data Point 3
Distress Level at Peak Moment (1–5)
1 = Completely calm | 3 = Visibly tense but regulated | 5 = Full distress response
1 = Completely calm | 3 = Visibly tense but regulated | 5 = Full distress response
Data captured today tells you: Is tolerance increasing week over week? Is distress decreasing? Is hierarchy advancement happening? Without data, progress is invisible — even when it's happening. Parents who track data demonstrate 3× higher intervention adherence (Pinnacle outcome data, 2024).
📥Download: A-077 Vestibular Progress Tracking Sheet (8-week log) at pinnacleblooms.org/resources/A077-tracker | 📞Share your tracking data with a Pinnacle OT: 9100 181 181 — FREE. Specialists review home tracking data and adjust your protocol accordingly.
Most sessions don't go perfectly. That is expected data, not failure.
❓ Child refused to even approach the playground today
Why: High baseline anxiety, unexpected change, insufficient preparation.
What to do: Today's goal was "come to the playground." You achieved it. The swing was visible. That is enough. Review visual story tonight. Tomorrow: same thing.
What to do: Today's goal was "come to the playground." You achieved it. The swing was visible. That is enough. Review visual story tonight. Tomorrow: same thing.
❓ Child had immediate panic response when near swing
Why: You may have advanced one hierarchy step too fast, or a previous negative experience was triggered.
What to do: Back up two steps on the hierarchy. Spend one week at "walk to within 5 meters." No shame — recalibration is data.
What to do: Back up two steps on the hierarchy. Spend one week at "walk to within 5 meters." No shame — recalibration is data.
❓ Child was fine on first session, then much worse on second
Why: The nervous system needs 24–48 hours to consolidate vestibular learning. Second-session regression is NORMAL and temporary.
What to do: Match exactly what worked in session 1. Repeat for 3–4 sessions before advancing.
What to do: Match exactly what worked in session 1. Repeat for 3–4 sessions before advancing.
❓ Child did well at home but refuses at public playground
Why: Generalization takes longer than acquisition. Public playgrounds have different sensory loads and social dynamics.
What to do: Home mastery → familiar outdoor space → quiet public playground → normal playground. Each step requires its own graduated exposure.
What to do: Home mastery → familiar outdoor space → quiet public playground → normal playground. Each step requires its own graduated exposure.
Emergency response if child became severely distressed: 1) Remove from swing area immediately — no explanations. 2) Deep pressure: firm hug, weighted lap pad. 3) Do NOT return to swings today. 4) Do NOT discuss incident for 30+ minutes. 5) Reconnect over preferred activity. | 📞9100 181 181 if intense distress is recurring.

No two children have the same vestibular profile. Here is how to tune this for yours.
Easier Modifications (scores 1–3)
Begin at ground-level equipment ONLY — no swings yet. Increase proprioceptive prep from 10 to 20 minutes. Add comfort object to every approach. Spend 2 weeks on each hierarchy step. Add co-regulating adult presence (second trusted adult also present).
Standard Protocol (scores 4–6)
Follow the 9-material sequence as described across Cards 14–19. One hierarchy step per comfortable completion. Advance only when child achieves same step 3–4 times without distress.
Advanced Modifications (scores 7–10)
Introduce 2 different swing types in one session. Reduce adult proximity gradually. Introduce brief peer presence. Introduce unfamiliar playground settings. Extend swing duration by 30-second increments.
Sensory Profile | Modification | |
Vestibular avoider | Start even slower. Ground-level only 4+ weeks. Every step takes longer. | |
Dual-register (avoids AND seeks) | May tolerate spinning before linear swinging — use sit-and-spin as bridge | |
High proprioceptive need | More prep, more bolster swing (prone), more deep pressure throughout | |
Visual-dominant anxiety | Enclosed cocoon first — removes visual open-space component before adding movement |
Age Modifications: Ages 2–3: Lap sitting almost always the starting point. 3-minute sessions maximum. | Ages 4–6: Core protocol as described. Visual story critical. | Ages 7–10: Child can participate in designing their own hierarchy ladder. More verbal processing after sessions.
Weeks 1–2 are about tolerance, not mastery. Here is what real progress looks like.
Progress: Week 1–2 — Foundation
15%
Foundation Phase
You are here — building the neural foundation that everything else depends on
✅ Observable Progress Indicators
- Child arrives at playground without immediately melting down
- Child can see the swing area without immediately leaving
- Child touches a still swing (even once, even briefly)
- Distress duration is decreasing (was 20 min, now 10 min to recover)
- Child engages with the visual story at home
❌ Not Progress Yet (Manage Expectations)
- Child spontaneously asking to go on swings
- Child tolerating movement
- Child being "fine" at playgrounds
- Siblings and others noticing a change
"If your child can walk within 5 meters of a swing and not immediately run away — that is REAL neurological progress. The nervous system has just registered: 'Swings are survivable to be near.' That's the foundation everything else is built on."
These first two weeks are often the hardest for parents because the change is invisible. You are doing the work and not seeing the results yet. Trust the process. The neural pathways are forming beneath what you can observe. PMC11506176 | Early-phase outcome literature (8–12 week timelines)
Something is changing. Here is how to recognize the consolidation signals.
Progress: Week 3–4 — Neural Pathways Forming
40%
Consolidation Phase
Neural pathways forming — behavioral shifts becoming visible
🔵 Child approaches the playground without the same baseline dread
🔵 Visual story review takes less time — less reassurance needed
🔵 Child can sit on a still swing for 15–30 seconds without distress
🔵 Child ASKS about swings — even "are there swings?" is engagement, not avoidance
🔵 Child watches other children swinging more curiously than fearfully
Subtle micro-behaviors signaling neural reclassification: Child stops walking the long way around the swings. They push an empty swing themselves without prompting. They mention swings in a neutral context. These mean the nervous system is reclassifying swings from DANGER to UNFAMILIAR.
Consider increasing frequency/intensity when: Child has achieved the same hierarchy step 3–4 times without distress • Child self-initiates the approach • Data shows 3+ consecutive sessions with distress level ≤2
The nervous system has learned. Here are the signs that mastery has arrived.
Progress: Week 5–8 — Mastery Phase
75%
Mastery Phase
Week 5–8: Mastery indicators present — maintenance and generalization begin
✅ Independent Approach
Child approaches swing area without preparation — no visual story required
✅ Tolerates Swinging
Child tolerates 1–2 minutes of supported swinging with minimal distress
✅ Self-Initiates
Child ASKS to go on swings spontaneously — even once is mastery
✅ Quick Recovery
Child recovers within 1–2 minutes if overstimulated (was 20+ minutes at baseline)
🏆MASTERY UNLOCKED: Child swings for 3+ consecutive minutes on any adaptive swing type with distress level ≤1. Next: Introduce traditional belt swing (begin hierarchy from Step 1). Introduce novel swing environments. Explore A-080 Height/Climbing Fear, A-085 Escalator Fear, A-086 Elevator Fear.

You did this. Your child grew because of your commitment.
Somewhere between Week 1's knuckle-white terror and today, the nervous system of your child revised its entire classification of swings.
Not because you forced it. Because you were patient when it would have been easier to give up. Because you celebrated touching a chain for one second. Because you never forced. Because you showed up — even on the hard days — with proprioceptive prep and visual stories and your own regulated nervous system. That was you. Your child grew because of your commitment.
Where You Started
Complete swing avoidance with terror response — knuckles white, body rigid, 20 minutes to stop shaking
Where You Are Now
Tolerates supported swinging — and sometimes asks for it | Timeline: ~6–8 weeks of consistent, gentle, parent-led protocol
🎉Mark this milestone. A photo at the swing. A certificate of bravery. A celebration dinner. The nervous system remembers positive milestones too. | Journal prompt: "On [date], my child [did the specific thing]. I remember thinking they would never be able to. I was wrong." Keep this. Read it when future challenges feel insurmountable.
Even in the progress zone, these signs mean "pause and consult."
Red Flag | What It Looks Like | What To Do | |
Persistent vomiting/nausea during swinging | Child vomits, reports spinning sensation, extreme pallor | STOP. Do not resume until assessed by ENT/pediatrician. Possible vestibular disorder beyond sensory processing. | |
Fear spreading to new domains | Child now also terrified of cars, elevators, being picked up (wasn't before) | Possible sensitization. Reduce all vestibular work. Consult Pinnacle OT. | |
No measurable progress after 8 weeks | Distress levels unchanged, hierarchy steps not advancing | Comprehensive sensory integration evaluation needed. Call 9100 181 181. | |
Trauma-type responses | Nightmares about swings, crying at swing-related images, hypervigilance | Trauma-informed approach needed alongside sensory work. Mental health consultation. | |
Physical asymmetry in movement | Falling to one side consistently, head tilting, eye movement irregularities | Rule out neurological or vestibular disorder. Pediatric neurologist referral. | |
Sudden regression after long progress | Was tolerating swings, suddenly returns to baseline fear | Check for illness (ear infection), major life stressor, or re-traumatization event. |
Escalation Pathway: 1) Self-resolve: pause 1 week, resume 2 hierarchy steps back. 2) Teleconsult: Pinnacle OT phone/video — 9100 181 181. 3) Clinic visit: in-person sensory integration assessment. 4) Medical referral: ENT or pediatric neurology if physical signs present.
"If something feels wrong, pause and ask. A cautious pause costs one week. Missing a red flag costs months. You know your child better than any protocol."
You are not done. You are on a journey. Here is where A-077 sits.
Path A — Ready to Progress
→ A-079: Child Seeks Intense Movement — Vestibular seeking as the flip side of vestibular avoiding
Path B — Related Vestibular Fears
→ A-080: Height and Climbing Fear | → A-092: Slide Fear — address these after swing mastery
Long-term developmental goal: Vestibular Processing Index Mastery → Playground Participation → Physical Confidence → Social Inclusion → School Readiness | WHO/UNICEF Developmental Milestones Framework | Pinnacle 12-Domain Architecture

The vestibular processing domain contains 15+ techniques. Here are the ones most relevant after A-077.


🌀 A-079 — Child Seeks Intense Movement
Domain: Vestibular / Sensory Seeking | Difficulty: 🟡 Core

🌀 A-080 — Height and Climbing Fear
Domain: Vestibular / Gravitational Insecurity | Difficulty: 🟡 Core


✅ Ground-level movement equipment from A-077 is reused in A-078, A-079, A-080. ✅ Visual story and hierarchy materials are used across ALL related techniques. ✅ Proprioceptive prep materials are used in every sensory domain technique. Browse all Domain A Sensory Processing techniques →
The research library. Every claim on this page has a source.
1. PRISMA Systematic Review (2024)
16 studies (2013–2023) confirm sensory integration intervention is evidence-based practice for ASD. PMC11506176
2. Meta-Analysis: World J Clinical Cases (2024)
24 studies demonstrating SI therapy effectiveness across adaptive behavior, motor, and sensory processing domains. PMC10955541
3. Indian RCT: Padmanabha et al. (2019)
First Indian RCT establishing home-based sensory interventions show significant outcomes in Indian pediatric populations with ASD. DOI:10.1007/s12098-018-2747-4
4. WHO Care for Child Development Package (2023)
Evidence base for caregiver-delivered developmental interventions across 54 low- and middle-income countries. PMC9978394
5. NCAEP Evidence-Based Practices Report (2020)
Visual supports and graduated exposure classified as Level 1 evidence-based practices for autism. NCAEP 2020 Report
6. Frontiers in Integrative Neuroscience (2020)
Neurological framework for sensory integration treatment in ASD, establishing the basis for all materials in this protocol. DOI:10.3389/fnint.2020.556660
Full Pinnacle evidence library → pinnacleblooms.org/research/domain-a | 📞FREE National Autism Helpline: 9100 181 181
Preview of 9 materials that help when child fears swings Therapy Material
Below is a visual preview of 9 materials that help when child fears swings therapy material. The pages shown help educators, therapists, and caregivers understand the structure and content of the resource before use. Materials should be used under appropriate professional guidance.




















Link copied!
Frequently Asked Questions
❓ How long will it realistically take for my child to use swings normally?
For children with mild vestibular sensitivity, 6–10 weeks of consistent graduated approach often produces functional swing tolerance. For significant vestibular hypersensitivity, 4–6 months is realistic. Some children achieve "comfortable" swinging; others achieve "tolerable with preferred support swing" — both are complete success. The goal is participation without terror, not a specific swing type or duration.
❓ My child LOVES spinning in circles but hates swings. How is this possible?
Rotational input (spinning) uses the semicircular canals differently than linear acceleration (swinging). Many children are sensitive to one type but not the other. If your child tolerates rotational input, we can use that as a vestibular foundation while building linear tolerance gradually. Tell your OT about this pattern.
❓ Should I try to talk my child through the fear? Explain that swings are safe?
Brief, simple reassurance helps. What does NOT help: extended explanations, logical arguments, or repeating reassurances many times (this actually increases anxiety). The nervous system cannot be reasoned out of a physiological response. The body must experience safety, not just hear about it.
❓ We were told to "push through the fear" for exposure therapy. Is that right?
Graduated exposure is evidence-based. Flooding (forcing full exposure) is generally contraindicated for vestibular hypersensitivity and can cause sensitization and re-traumatization. If you are being advised to force your child onto swings "for exposure," please seek a second opinion. Call 9100 181 181.
❓ My child's swing fear suddenly appeared at age 6 — they used to love swings.
Sudden onset can indicate: a frightening incident, a medical event affecting the vestibular system (ear infection, head injury), or a developmental shift in sensory processing. Start with the protocol but also consult a pediatrician to rule out medical causes.
❓ My child has ASD and sensory challenges across multiple domains. Which first?
The GPT-OS® AbilityScore® assessment identifies which sensory domains are creating the most developmental interference and sequences intervention accordingly. Vestibular processing is a foundation sense — addressing it often produces broader benefits across domains. Call 9100 181 181 for your child's individualized sequence.
📞Still need help? Book a teleconsultation → 9100 181 181 | FREE, 24x7, 16+ Languages
🚀 You now understand the science. You have the materials. You have the protocol.
There is one thing left to do.
There is one thing left to do.
📞FREE National Autism Helpline: 9100 181 181 | 24x7 | 16+ Languages | India's Largest Pediatric Therapy Network
🌿 Validated by the Pinnacle Blooms Consortium | Occupational Therapy • ABA/BCBA • SLP • SpEd • NeuroDev Pediatrics
© 2025–2026 Pinnacle Blooms Network®, unit of Bharath Healthcare Laboratories Pvt. Ltd. All rights reserved. | CIN: U74999TG2016PTC113063 | DPIIT: DIPP8651 | MSME: TS20F0009606 | GSTIN: 36AAGCB9722P1Z2