Squeeze Me Tighter. Every. Single. Hug.
He crashes into the couch 40 times a day — on purpose. She wraps herself in every blanket in the house. His nervous system is asking for something his words cannot express. Today, you learn how to answer.
Sensory Series A-101
Ages 2–12 Years
OT-Led · ABA-Supported · WHO-Aligned
Home-Executable

You Are Among Millions of Families Navigating This Exact Challenge
When your child asks to be squeezed tighter, crashes into furniture on purpose, or wraps themselves in every blanket they can find — they are not alone. Proprioceptive seeking is one of the most documented sensory profiles in children with autism, sensory processing differences, and neurodevelopmental variation. Across cultures, across continents, across every economic background — millions of parents are navigating this same exhaustion.
80%
Experience Sensory Difficulties
Of children with autism experience significant sensory processing difficulties. PRISMA Systematic Review, 2024.
1 in 36
Children in India
Diagnosed with developmental differences involving sensory challenges. National estimates, India.
21M+
Therapy Sessions
Delivered by Pinnacle Blooms Network® — the world's largest autism therapy data system.
"The sensory system doesn't know what zip code you live in. What your child's body needs is universal. What works, crosses every border." — Pinnacle Blooms Consortium, Occupational Therapy Division
Research basis: Meta-analysis (World J Clin Cases, 2024): SI therapy effective across 24 studies (PMC10955541). PRISMA Review 2024: SI intervention meets evidence-based practice criteria (PMC11506176). WHO/UNICEF: Sensory and developmental challenges documented in 197 countries.

What's Happening in Your Child's Brain
Proprioception is sometimes called the "sixth sense" — the sense that tells us where our body is in space, how much force we're using, and whether we feel grounded and present. Unlike sight or sound, you cannot consciously observe proprioception. You feel it.
The Proprioceptive Pathway
Muscles & Joints → send position signals. Tendons → detect force and pressure. Spinal Cord → transmits proprioceptive data. Somatosensory Cortex → processes "where am I?" Parasympathetic System → activated by deep pressure → CALM.
In deep pressure seeking children: the proprioceptive threshold is higher than typical. More intense input is needed to register sensation. The body isn't broken — it needs a louder signal.
Plain English: What This Means for Your Child
For your child, the receptors in their muscles, joints, and tendons need more intense input than typical to register sensation. This is not hyperactivity. It is not attention-seeking. It is a neurological threshold — like a thermostat set higher than usual that needs more heat to register.
When your child crashes, squeezes, or wraps themselves tight — they are self-regulating their nervous system through the only tool that works: intense proprioceptive input. The crashing calms them. The bear hug grounds them. The weighted blanket settles them.
Wiring difference. Not a behavior choice. Not a parenting failure. A nervous system asking for the right kind of input. When deep pressure activates proprioceptors → the parasympathetic nervous system fires → the child feels calm, present, and organized. This is the science behind those hugs.
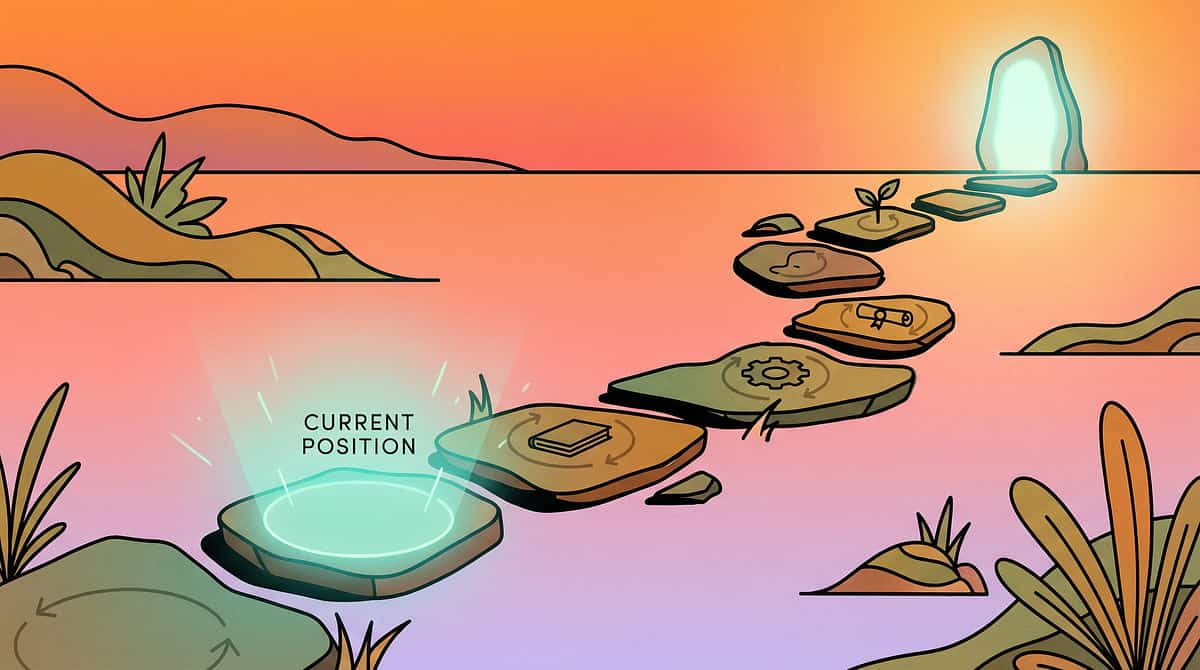
Your Child's Proprioceptive Journey — Where They Are, Where This Leads
Deep pressure seeking typically intensifies between ages 2–5 as the child becomes mobile enough to seek input through crashing and physical contact, but before they have the language and self-awareness to communicate what they need. This is why the behaviour feels relentless — the nervous system is calling urgently and getting no structured answer.
1
Ages 0–12 months
Proprioceptive system develops through rolling, crawling, tummy time, grasping.
2
Ages 1–2 years
Body awareness through normal climbing, grasping, and physical exploration.
3
Ages 2–5 years ◄ YOU ARE HERE
Peak Seeking Zone: Crashing, intense hugging, body slamming, constant squeezing. Nervous system calling urgently.
4
Ages 5–8 years
Learning to identify the need and communicate it. Tool preference forming.
5
Ages 8–12 years
Self-regulation mastery — choosing tools independently. Goal: self-initiated use.
Often co-occurs with: Vestibular seeking (spinning, swinging) — proprioceptive and vestibular systems are closely linked. Oral motor seeking (chewing) — covered separately in A-100. Attention/focus challenges — proprioceptive input regulates the arousal system. Sleep difficulties — under-regulated proprioceptive system affects transition to rest.
With the right materials and protocol — used consistently — the trajectory points toward self-regulation. This has been documented across 70+ centers and 21 million sessions. It is not a hope. It is a documented pathway. WHO Care for Child Development Package (2023) | PMC9978394

The Evidence Behind This Technique
Evidence Grade: Level I — Systematic Review + RCT
This technique has been reviewed and validated by the Pinnacle Blooms Consortium — OT, SLP, ABA, SpEd, NeuroDev, CRO — and is part of the GPT-OS® evidence-based intervention library. Clinically Validated. Home-Applicable. Parent-Proven.
📄 PRISMA Systematic Review (Children, 2024)
16 articles, 2013–2023 confirm sensory integration intervention meets evidence-based practice criteria for ASD. PMC11506176
📄 Meta-Analysis (World J Clin Cases, 2024)
24 studies. SI therapy effectively promotes social skills, adaptive behavior, sensory processing, and motor skills. PMC10955541
📄 Indian RCT (Indian Journal of Pediatrics, 2019)
Home-based sensory interventions demonstrated significant outcomes in Indian pediatric population. Parent-administered protocol validated. DOI: 10.1007/s12098-018-2747-4
✓ 24+ Studies Reviewed
Meta-analytic base confirms efficacy
✓ India-Specific RCT
Validated for Indian pediatric populations
✓ WHO/UNICEF Endorsed
Aligned with Nurturing Care Framework
✓ NCAEP 2020 Validated
Evidence-based practice classification
Foundational texts: Ayres, A.J. — Sensory Integration and the Child (1979, 2005). Grandin, T. — Thinking in Pictures (1995). Kranowitz, C.S. — The Out-of-Sync Child (1998). SPD Foundation — Proprioceptive input clinical guidelines.

The Technique: Deep Pressure / Proprioceptive Input Protocol
Also known as: "Bear Hug Technique" | "Heavy Work Program" | "Sensory Diet for Proprioceptive Seekers"
What It Is
A structured approach to meeting a child's proprioceptive seeking needs through 9 clinically-selected materials and home-based protocols that deliver deep pressure input to the muscles, joints, and tendons — calming the nervous system, reducing unsafe seeking behaviours (crashing, too-hard hugging), and building toward independent self-regulation.
What It Does
Activates the parasympathetic nervous system through intense proprioceptive input; reduces arousal level; grounds the child's body awareness; decreases crashing, slamming, and excessive hugging as the need is safely met.
Who It's For
Children aged 2–12 who are under-responsive to proprioceptive input — the child who seeks bear hugs that are never tight enough, crashes into furniture and people, throws themselves onto surfaces, and calms primarily through intense physical pressure.
Domain | Age Band | Frequency | |
Sensory — Proprioceptive | 2–12 years | 3–5× daily | |
Technique Code | Session | Setting | |
A-101 | 10–20 mins | Home / School |
"The goal is not to stop the crashing. The goal is to answer the crash. When the body gets what it's asking for — the asking quiets down."
Who Uses This Technique: The Pinnacle Consortium Approach
5 disciplines. 1 converged protocol. This technique crosses therapy boundaries because the brain doesn't organize itself by therapy type. Proprioception affects attention, learning, communication, behavior, and development — simultaneously.
Occupational Therapy (Primary Lead)
OTs design the sensory diet — the schedule of proprioceptive input built into daily life. They assess the child's sensory profile (Dunn Sensory Profile, SPM), determine input intensity, select materials, and train parents in safe technique execution.
ABA / BCBA
BCBAs address the behavioral dimension: reinforcing the use of appropriate tools (crash pad, compression vest) over unsafe seeking. Functional behavior assessment guides substitution — replacing crashing with weighted blanket use.
Speech-Language Pathology
SLPs address the link between proprioceptive dysregulation and communication breakdown. A child who cannot regulate their body cannot attend to language. Deep pressure strategies precede speech sessions. SLPs also help the child verbalize: "I need a squeeze."
Special Education
SpEd teachers integrate proprioceptive accommodations into the classroom: weighted lap pads, compression vests under uniforms, heavy work "helper jobs," movement breaks. IEP/504 sensory accommodation documentation guided jointly by SpEd and OT.
NeuroDevelopmental Pediatrics
NeuroDev Pediatricians rule out differential diagnoses, confirm safety for proprioceptive protocols, and integrate the sensory diet with any medication management. They provide the medical clearance that authorizes home-based deep pressure programs.
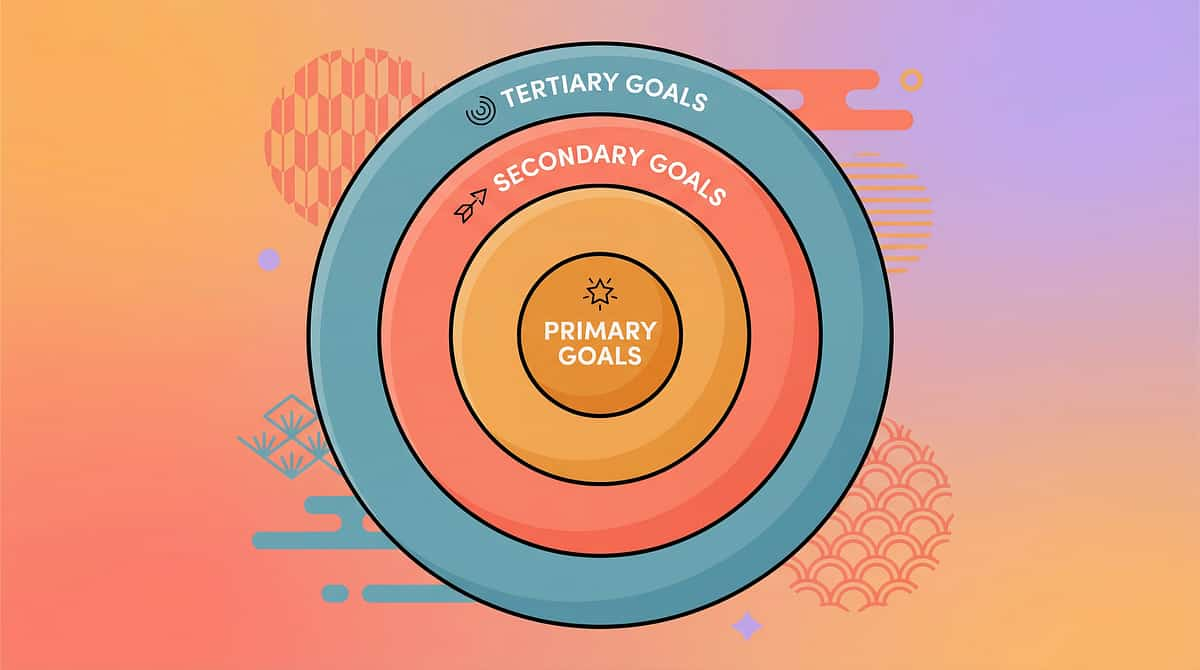
What This Technique Targets
A-101 addresses a layered cascade of outcomes — from the primary neurological goal of proprioceptive self-regulation, through to social participation and academic readiness. Research (PMC10955541) confirms SI therapy promoted social skills, adaptive behavior, sensory processing, and motor skills across 24 studies.
🎯 Primary: Proprioceptive Self-Regulation
Reduce crashing into furniture, walls, and people. Replace too-hard hugging with appropriate tools. Build from unconscious seeking toward conscious tool selection. Observable indicator: Child moves toward crash pad rather than the couch when seeking.
🔵 Secondary: Attention, Emotion & Transition
Proprioceptive input organizes the arousal system → child can sit, attend, and learn. Deep pressure activates parasympathetic system → reduced meltdown frequency. Scheduled input before transitions reduces resistance and refusals.
⚪ Tertiary: Social, Academic & Sleep
A child who regulates proprioceptive needs engages more safely with peers. An organized nervous system enables learning engagement. Weighted blanket as nighttime proprioceptive input improves sleep onset.
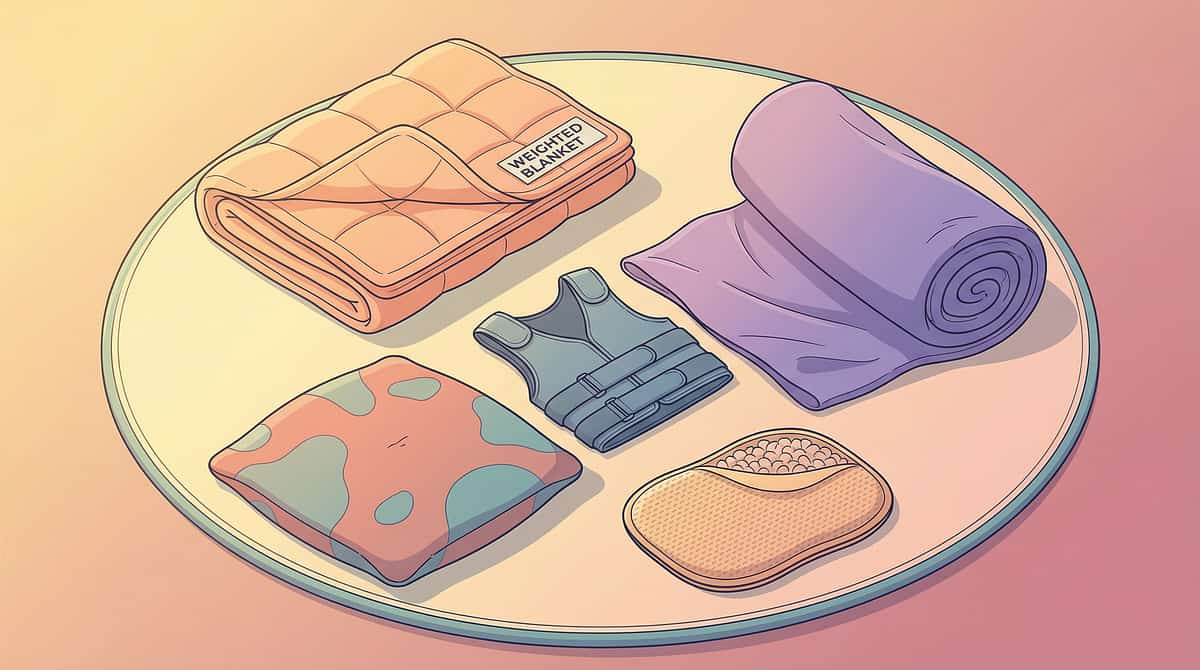
9 Clinically-Validated Materials for Deep Pressure Seeking
Each material below targets proprioceptive input from a different angle — passive, active, wearable, environmental. Together, they form a complete sensory diet for your proprioceptive seeker. You don't need all 9 at once — start with the essentials and build gradually.
Essential Starters — Begin Here
- Burrito Roll — ₹0 — TODAY
- Crash Pad — DIY with cushions — THIS WEEK
- Weighted Blanket — ₹2,000–6,000 — ORDER NOW
Complete Kit Cost Range
₹0–20,000+ for full approach. Most impactful combo: Crash Pad + Weighted Blanket + Heavy Work routine. DIY-friendly options: Burrito Roll, Crash Pad, Heavy Work, Squeeze Adaptation, Lap Pad.
All 9 Materials
- Weighted Blanket
- Compression Vest or Shirt
- Body Sock / Sensory Sock
- Crash Pad / Crash Mat
- Weighted Lap Pad
- Lycra Swing / Cuddle Swing
- Heavy Work Activities Kit
- Squeeze Machine Adaptation
- Burrito Roll

Material 1: Weighted Blanket
Canon Category: Sensory Regulation Materials
₹2,000–6,000
"A hug that doesn't end." Provides sustained, distributed deep pressure across the entire body. The weight (approximately 10% of child's body weight) stimulates proprioceptors, activating the parasympathetic nervous system for lasting calm. Unlike a human hug, it requires nothing from the child — it simply delivers continuous, passive input.
Child Weight | Blanket Weight | |
15–20 kg | 1.5–2 kg | |
20–30 kg | 2–3 kg | |
30–40 kg | 3–4 kg | |
40–50 kg | 4–5 kg |
Use when: Homework, screen time, post-school transition, sleep, calm-down space. Search: "Weighted Blanket" on Amazon.in. Child must be able to independently remove the blanket at all times.

Material 2: Compression Vest or Shirt
Canon Category: Sensory Regulation — Compression
₹1,500–4,000
"Wearing a hug all day." Provides constant wearable deep pressure to the torso throughout the day. The child receives proprioceptive input continuously without needing to seek it through crashing. Invisible under school uniforms. Evidence-based for improving attention and reducing sensory-seeking behaviours.
Best Use Times
- School hours
- Homework time
- During transitions
- High-demand activities
Key Benefits
Continuous proprioceptive input without any active effort from parent or child. Once it becomes a morning routine habit, no special protocol is needed — the vest does the work all day. Particularly powerful for school settings where other tools aren't available.
Search: "Compression Vest for Kids" on Amazon.in. Can also be used as a compression shirt underneath regular clothing.

Material 3: Body Sock / Sensory Sock
Canon Category: Sensory Regulation — Proprioceptive
₹800–2,500
"Full-body pressure through movement." A full-body stretchy lycra enclosure. The child climbs inside and pushes, stretches, and moves against the resistance — proprioceptive input from all directions simultaneously. Combines deep pressure with body awareness and motor planning. A staple in OT sensory gyms, now for the home.
How It Works
Every push into the fabric fires proprioceptors. Suggest activities inside: make a star shape, do yoga poses, try to touch the edges with hands and feet. The resistance provides the input — every push fires more proprioceptors.
⚠️ Safety Note
Always supervise. Child must be able to exit independently. Never leave unattended. Do not use with children who have a co-occurring tactile sensitivity profile without OT guidance first.
Search: "Body Sock Sensory" on Amazon.in. What correct use looks like: Child experiments with the resistance playfully. Calming visible after 5–10 minutes of active use.

Material 4: Crash Pad / Crash Mat
Canon Category: Sensory Regulation — Proprioceptive / Impact
₹3,000–8,000 | ₹0 DIY
"A safe place to crash." Provides a sanctioned, safe surface for the crashing behavior the child is already seeking. This is the MEET THE NEED approach — instead of trying to stop crashing (which cannot work neurologically), the crash pad redirects it. Place it where the child already naturally crashes.
The Core Principle
The crash pad works because the child chooses how to use it. Do not direct or limit. The crashing IS the therapy — meeting the need directly. Parent's role: proximity and safety monitoring, not direction.
What correct use looks like: Child crashes repeatedly, then begins to slow down. Frequency of crashes decreases organically as the need is met.
DIY Alternative
Stack couch cushions + large floor pillows + old duvets. Cover with a durable sheet. Minimum 20 cm deep pile. Same impact absorption; crash landing is equally sanctioned by the nervous system.
Minimum Requirements
Minimum thickness: 15–20 cm. Clear surrounding area of all hard objects. Position in corner where child naturally crashes — placement matters.

Material 5: Weighted Lap Pad
Canon Category: Sensory Regulation — Weighted
₹500–1,500
"Deep pressure while sitting." Localized weight across the lap and thighs during seated activities. Portable, discreet, works at home, school, and in the car. Grounds the child without restricting movement — enabling longer seated engagement for homework, school, and meals.
At Home
Use at the homework table, during meals, or screen time. Drape across lap. No special setup required. Can be combined with compression vest for layered input.
At School
A common IEP/504 accommodation. Invisible under desk. Send one to school with a note from your OT. Ask the teacher to allow use during all seated work.
DIY Option
Long sock filled with 1–1.5 kg dried rice. Tie closed. Drape across lap. Made in 10 minutes. Same localized pressure as commercial versions.
Search: "Weighted Lap Pad" on Amazon.in.

Material 6: Lycra Swing / Cuddle Swing
Canon Category: Vestibular/Proprioceptive Combined
₹2,000–5,000 + mounting hardware
"Wrapped and swinging." The most powerful combined input available for home use. The stretchy fabric wraps around the body (deep pressure/proprioception) while the swinging provides vestibular input simultaneously. 5–15 minutes organizes the child for 30–60 minutes of focused engagement.
⚠️CRITICAL SAFETY REQUIREMENT: Must be mounted in a weight-rated ceiling beam. Professional installation is non-negotiable. Supervise ALL use. Inspect hardware before every session. Do NOT use a doorframe bar without proper load rating confirmation from a hardware professional.
Why It's So Powerful
The lycra fabric provides proprioceptive input (deep pressure from cocoon). The swinging motion provides vestibular input simultaneously. Two sensory systems addressed in one tool — which is why 5–15 minutes creates 30–60 minutes of organized engagement afterward.
Usage Protocol
First 3 sessions: limit to 5 minutes of gentle linear swinging only. Gradually increase duration as child demonstrates positive regulation response. Use before high-demand activities — homework, meals, transitions, school departure.
Search: "Lycra Cuddle Swing Sensory" on Amazon.in.

Material 7: Heavy Work Activities Kit
Canon Category: Heavy Work / Proprioceptive Active
₹500–2,000 | ₹0 with household items
"Pushing, pulling, lifting, carrying." The lowest-cost, highest-impact proprioceptive input category. Heavy work — any activity requiring significant muscle engagement — delivers intense proprioceptive input through natural, functional actions. Schedule heavy work breaks every 1–2 hours throughout the child's day.
Carrying
Carry laundry basket, grocery bags, water bottles, stacks of books. The heavier and more sustained, the more effective.
Pushing & Pulling
Push shopping cart, pull wagon, push chairs across the floor, drag a heavy bag from room to room. Make it a game.
Resistance
Wall push-ups, wheelbarrow walks, garden work, moving furniture. Any activity that makes muscles work hard delivers the input.
Heavy work activities using household items have an IDENTICAL therapeutic effect to commercial kits. Heavy work is the activity, not the tool. Zero cost, maximum impact.
Material 8: Squeeze Machine Adaptation
Canon Category: Controlled Deep Pressure
₹5,000–15,000 adapted | ₹0 DIY
"Controlled deep pressure from both sides." Inspired by Temple Grandin's squeeze machine — designed by an autistic person who sought deep pressure herself — home adaptations provide bilateral, controlled deep pressure the child can regulate. The key distinction: the child controls the intensity.
"I craved the feeling of being held, but I was overwhelmed by the feeling of being held by someone." — Temple Grandin. The squeeze machine resolved this tension between the need for deep pressure and the social overwhelm of human touch.
DIY Squeeze Machine
Child positioned between two large bean bag chairs. Parent applies slow, firm pressure from both sides simultaneously. Child controls pressure by saying "more," "less," or "stop." Never use chest compression — lateral pressure only. Child's voice controls every moment.
Why Child Control Matters
The therapeutic principle of the squeeze machine is the child's ability to control the intensity of input. This meets the proprioceptive need without the unpredictability of human touch — critically important for children who seek deep pressure but are overwhelmed by social physical contact.

Material 9: Burrito Roll (Blanket Compression Technique)
Canon Category: Sensory Techniques — Zero-Cost / Immediate
₹0
"Full-body compression, zero cost." The single most accessible deep pressure tool that exists. Child is rolled firmly in any household blanket like a burrito — full-body compression, no equipment, no purchase, no setup. Taught in OT and parent training programs globally. Often becomes the child's favourite calming strategy.
01
Position
Child lies at edge of blanket on back or stomach. Arms at sides, relaxed.
02
Roll
Parent rolls child firmly across blanket from one edge to the other — snug, like a burrito. Tuck edges underneath.
03
Apply Pressure
Optional: apply gentle palm pressure on top through the blanket. Check in verbally.
04
Duration & Exit
2–10 minutes. Unroll immediately on child's request. Child always controls when it ends.
The word "burrito" is often magic. Most children laugh — and laughter is the perfect entry to a calming protocol. Full execution protocol detailed in Steps 1–6 (Cards 27–32).

DIY & Substitute Options: Every Child Deserves Access
Following the WHO/UNICEF principle of context-specific, equity-focused intervention — every material in A-101 has a functional household substitute. The proprioceptive principle works regardless of the wrapper. Deep pressure works because of the neurological mechanism — not because of the brand name on the blanket.
Buy This | Make This Today | Why It Works | |
Weighted Blanket ₹2,000–6,000 | Duvet cover filled with evenly distributed dried beans/rice sewn into pockets (~10% child body weight) | Same weight distribution; same proprioceptive input activation | |
Compression Vest ₹1,500–4,000 | Layer snug-fitting athletic wear or swimwear — multiple tight layers add compression | Same continuous torso pressure; slightly less precise but functional | |
Body Sock ₹800–2,500 | Large stretchy pillowcase or lycra fabric sewn into a sack (must have stretch and resistance) | Same resistance-against-movement proprioceptive principle | |
Crash Pad ₹3,000–8,000 | Stack couch cushions + large floor pillows + old duvets. Cover with durable sheet. Minimum 20 cm deep pile. | Same impact absorption; crash landing is equally sanctioned | |
Weighted Lap Pad ₹500–1,500 | Long sock filled with 1–1.5 kg dried rice. Tie closed. Drape across lap. | Same localized pressure; easy to make in 10 minutes | |
Lycra Swing ₹2,000–5,000 | Fabric hammock from durable lycra. NOTE: Do NOT DIY mount hardware — use hardware-store doorway frame mount with verified load rating only. | Proprioceptive cocoon effect; professional mounting non-negotiable | |
Heavy Work Kit ₹500–2,000 | Household chores: laundry basket, grocery bags, garden work, moving furniture. Zero cost. | IDENTICAL therapeutic effect — heavy work is the activity, not the tool | |
Squeeze Machine ₹5,000–15,000 | Child between two large bean bag chairs. Parent applies slow, firm pressure from both sides. Child controls with "more/less/stop." | Same bilateral deep pressure; child-controlled intensity | |
Burrito Roll ₹0 | This IS the DIY. Household blanket. No purchase needed. | Zero-cost, immediate, full-body compression. Works every time. |
"Context-specific, equity-focused intervention is not a compromise. It is the WHO/UNICEF mandate. In 54 low- and middle-income countries, the WHO Care for Child Development package demonstrates that household-material-based intervention achieves equivalent outcomes." — WHO NCF (2018) | PMC9978394

Safety First: Before You Begin
This is a non-negotiable read-before-execution card. Read all three levels before your first session. Most families will proceed on green. The amber and red sections exist to protect your child and give you clear thresholds for when to pause, modify, or stop.
🔴 RED LIGHT — Do Not Proceed If:
- Child has respiratory difficulties, cardiac conditions, or hypotonia without medical clearance
- Child has recently sustained a physical injury to muscles or joints
- Child shows signs of fever, illness, or acute distress
- Lycra swing/ceiling mount is not professionally installed and weight-rated
- Weighted blanket is being used on a child who cannot independently remove it
- Weighted blanket weight exceeds 10% of child's body weight
- Child cannot communicate or signal discomfort (modify protocol)
🟡 AMBER LIGHT — Proceed With Modification:
- Child is hyperaroused or post-meltdown → begin with passive deep pressure (burrito roll) rather than active (body sock)
- First-time use of any material → start with 5-minute exposure, observe response, increase gradually
- Weighted blanket new users → begin with legs/torso coverage only, not full-body
- Lycra swing: first 3 sessions → limit to 5 minutes of gentle linear swinging only
- Squeeze machine: never use chest compression — lateral/lateral only
- Child has hypersensitivity profile alongside seeking profile → consult OT before beginning
🟢 GREEN LIGHT — Safe to Proceed When:
- Child is calm or mildly regulated (not in acute meltdown)
- Child has eaten within the last 90 minutes
- Space is prepared and materials are ready
- All materials are at correct weight/intensity for child's size
- Parent has read full protocol before first session
- At least one adult is present and focused
⛔STOP IMMEDIATELY IF: Child reports pain · Skin appears red, mottled, or shows circulation marks · Child becomes severely distressed or panicked · Child's breathing sounds labored or restricted · Child loses consciousness or appears confused. After any STOP situation: consult your OT or NeuroDev Pediatrician before resuming. Call Pinnacle Helpline: 9100 181 181

Set Up Your Home Therapy Space — In 5 Minutes
Your space doesn't need to be a dedicated therapy room. It needs to be safe, prepared, and consistently available. Children respond to predictable environments — when the crash pad is always in the same corner, the nervous system begins to associate that space with regulated input.
Room Setup Checklist
- Crash pad positioned in corner where child naturally crashes
- Weighted blanket folded nearby, ready to drape
- Body sock accessible (not in a drawer)
- Compression vest on child already (if using for the day)
- Weighted lap pad at desk/table ready
- Lycra swing checked — hardware tested, floor below cushioned
- Heavy work items staged near door
- Blanket accessible for burrito roll
- All hard furniture edges away from crash zones
- Screens off or reduced
- Visual timer available for transitions
Environment Settings
Lighting | Moderate, natural or warm. Avoid harsh fluorescent. | |
Sound | Low background music or quiet. Avoid sudden loud sounds. | |
Temperature | Slightly cool — compression and heavy work generate body heat. | |
Space | Minimum 2m × 2m clear area for crash pad and movement. | |
Other children | Preferably separate session — prevent crashing into siblings. |
Remove from the Space
- Hard furniture edges near crash zones
- Fragile objects within crashing radius
- Distracting screens/devices

Is Your Child Ready? The 60-Second Pre-Session Readiness Check
Every session begins with this gate. A postponed session is not a failed session — it is a data point that tells you your child's needs that day. Starting at the right moment multiplies the impact of every technique. Starting at the wrong moment can escalate rather than regulate.
🟢 GO — All Clear to Start
- Child is neither starving nor just finished eating (90-min window ideal)
- No fever, illness, or physical injury observed
- Child's arousal level: seeking (crashing) but not meltdown-level
- Materials are set up and ready
- At least one focused adult is present
- No major transitions immediately ahead in the next 15 minutes
🟡 MODIFY — Start With Passive Only
- Child is post-meltdown but calming → start with weighted blanket or burrito roll only
- Child slept poorly → shorten session to 5 minutes of passive input
- Child is hypervigilant or extra-sensitive today → reduce intensity
- You are tired or depleted → use passive-only materials (blanket, lap pad)
🔴 POSTPONE — Try Again in 30 Minutes
- Child is in active meltdown
- Child is running fever or showing illness signs
- Child just had a physical injury
- Child is immediately pre-transition (leaving in 5 minutes)
- Child is refusing all physical contact today
Step 1 of 6: The Invitation
⏱️ 30–60 seconds
The invitation sets the tone for the entire session. Calm, warm, low-demand. You are offering — not directing. Be at the child's physical level. Face relaxed, open body posture. No hovering or pressure.
💬 "Hey [child's name], do you want to do your heavy work time? I have [crash pad / blanket / burrito roll] ready for you."
By Communication Level
- Verbal child: "Want your squeeze time? Your blanket is right here."
- AAC user: Hold up the symbol/image for the chosen material
- Pre-verbal: Walk to the material with child, gesture towards it, model getting in/on
- Resistant child: "We can start with just the blanket — just 2 minutes"
✅ Acceptance Cues
- Child moves toward the material
- Child lies down, gets in, or positions themselves
- Child makes eye contact or approaches you
- Reduction in crashing behavior (orienting to the offered input)
🟡 Resistance Cues & Responses
- Child moves away or ignores → try a different material from the 9
- Child continues crashing → say "Let's put that crash energy HERE" and redirect to crash pad
- Child is fixated on another activity → pair the material with that activity (blanket while watching preferred video)

Step 2 of 6: The Engagement
⏱️ 1–3 minutes
Introducing the material and reading the child's response. Your job here is to follow the child's lead, observe their response spectrum, and reinforce even 10 seconds of engagement. When the child engages — even briefly — say immediately: "YES. That's exactly right. Your body knows what it needs."
💬 Weighted Blanket Script
"Let's put your heavy blanket on. Can you feel the weight? It's going to help your body feel calm." Drape across lap/legs/full body based on child's preference. Let them guide coverage.
💬 Crash Pad Script
"Here's your crash spot — this is the safe place to crash as much as you need." Stand back. Child leads. First crash is always the biggest — this is the release of seeking tension.
💬 Body Sock Script
"Want to get inside your squeeze sock? See if you can make a star shape inside." Hold opening. Let child climb in at their pace.
💬 Burrito Roll Script
"Should I roll you up? Can I make you into a burrito?" The word "burrito" is often magic. Most children laugh — perfect entry to calming protocol.
Full Engagement ✅ | Tolerance 🟡 | Avoidance 🔴 | |
Child actively seeks more, asks for harder/heavier | Child stays with material passively | Child moves away from material | |
Continue, follow child's lead | Maintain, add gentle descriptive language | Switch to a different material from the 9 |

Step 3 of 6: The Therapeutic Action
⏱️ 5–15 minutes
The core protocol — what to do, precisely. For each material, the execution is different but the principle is the same: deliver deep proprioceptive input, let the child lead, maintain quality of engagement over clock time.
🔵 Weighted Blanket
Child lies under blanket, arms inside or out per preference. Parent drapes blanket from feet to shoulders with even weight distribution (no bunching). Child remains under blanket during a calm activity. Duration: 15–30 minutes for maximum effect. Correct: child's body visibly relaxes within 2–5 minutes, breathing slows.
🔵 Crash Pad
Child runs, jumps, falls, rolls onto crash pad freely. No limitation on number of crashes during the session. Parent's role: proximity and safety monitoring only — not direction. The crashing IS the therapy. Correct: child crashes repeatedly, then begins to slow down organically as the need is met.
🔵 Burrito Roll
Child lies at edge of blanket on back or stomach, arms at sides. Parent rolls child firmly — snug, like a burrito. Tuck edges underneath. Optional: apply gentle palm pressure on top through the blanket. Duration: 2–10 minutes. Correct: face relaxes, may request "tighter" or "more."
🔵 Body Sock
Child inside body sock, pushing and stretching the fabric. Suggest activities: star shape, yoga poses, trying to touch the edges with hands and feet. The resistance provides proprioceptive input — every push fires proprioceptors. Correct: child experiments playfully; calming visible after 5–10 minutes.
🔵 Heavy Work
Child carries weighted backpack, pushes laundry basket, does wall push-ups, carries grocery bags. Make it a game: "See how many times you can carry this from here to there." Correct: child engages with visible effort; proprioceptive input from muscle exertion self-regulates.
Common Execution Errors: Moving through activity too fast (this is input, not a task — let child lead duration). Talking too much during the session (quiet presence is more therapeutic than narration). Stopping when child "seems calm" (maintain input for 5 more minutes after calming is achieved). Using too-light weighted blanket (check weight against 10% guideline).

Step 4 of 6: Repeat & Vary
⏱️ 3–5 minutes additional
Therapeutic Dosage Principle: "3 good repetitions are worth more than 10 forced ones. Proprioceptive input works on dosage, not duration alone. Quality of engagement matters more than clock time." SI therapy: 2–3 sessions/week, 8–12 weeks typical. Home-based: multiple mini-sessions throughout the day more effective than one long session.
Calm Seeker Session
Child is regulated but seeking. → Weighted blanket 15–20 min + lap pad during homework. Single material, sustained, passive.
Active Seeker Session
Child is crashing, dysregulated. → Crash pad 5 min → body sock 5 min → burrito roll 10 min. Multiple materials, highest-intensity first, wind down to passive.
School/Homework Session
→ Heavy work (carry bags) → compression vest on → weighted lap pad at desk. Input before demand, passive input during demand.
01
Weeks 1–2: Single Material
One material per session. Observe full response. Establish tolerance and preference.
02
Weeks 3–4: Pair Two Materials
Combine crash pad + burrito roll or similar. Build the routine.
03
Week 5+: Child Chooses
Let child select from the 9 materials. Develops self-awareness and meta-cognition.
04
Advanced: Self-Initiation
Child initiates use of materials without prompting. This is the self-regulation goal.
Satiation indicators (when to stop): Child is clearly calming (body relaxes, movement slows). Child signals "done" or attempts to leave the material. Child has achieved calm baseline for 5+ continuous minutes. Child falls asleep — success, deep pressure supported sleep onset.
Step 5 of 6: Reinforce & Celebrate
⏱️ Within 3 seconds of target behavior
The ABA Reinforcement Core Rule: Deliver reinforcement WITHIN 3 SECONDS of the desired behavior. Immediate, specific, enthusiastic. Timing matters more than magnitude. Celebrate the attempt, not just the success — the child who walks toward the crash pad instead of crashing into the couch made progress, even if they then crashed.
Behavior Observed | Say Exactly This | |
Child uses crash pad instead of crashing into couch | "YES! You went to your crash pad! That was so smart. Your body knew exactly what it needed." | |
Child asks for burrito roll (verbally or by gesture) | "I love that you asked for your squeeze. Let's do it right now." | |
Child stays under weighted blanket for 5+ minutes | "Look how calm your body is. The blanket is really helping, isn't it?" | |
Child uses compression vest independently in morning | "You remembered your vest! You're taking such good care of your body." | |
Child uses body sock then sits calmly for homework | "I saw that — you did your body sock and now you're ready. You're figuring this out." |
⭐ Verbal Praise
Immediate, specific — use the scripts above
⭐ Physical Affirmation
High-five, fist bump — brief and warm
⭐ Token Economy
1 star → 5 stars → preferred activity
⭐ Natural Consequence
"You did your heavy work — now let's do the thing you wanted to do." The regulation itself is reinforcing.
Step 6 of 6: The Cool-Down
⏱️ 2–3 minutes
Why the cool-down matters: Abruptly ending a sensory session can cause dysregulation — the child goes from deep input to nothing, and the nervous system spikes. The cool-down transitions the child gradually from maximum input to baseline. Never skip this step. (NCAEP 2020: Visual supports are evidence-based practice for transitions.)
01
Transition Warning (30 seconds before ending)
💬 "Two more minutes, then we're all done with this for now. You can do this again after [next activity]." Set a visual countdown timer — Time Timer, sand timer, or phone timer with a visible display.
02
Reduce Intensity
Shift from active to passive: crash pad → weighted blanket for 2 minutes. Lower your own voice and movement simultaneously.
03
Materials Away
Child participates in putting materials away. Builds routine and ownership. "Blanket goes here. Body sock goes there. Good job taking care of your things."
04
Bridge to Next Activity
"We're done with squeeze time. Now we're going to [next activity]." Concrete, predictable, immediate.
If child resists ending:💬 "I know you want more. Your body is working hard. We'll do this again [at homework time / before bed]. For now, let's [transition activity]." Do NOT abruptly remove the material while child is using it, force completion, or shame the child for wanting to continue.
Capture the Data: Right Now
Track immediately after every session. Data captured now is data that drives your child's next GPT-OS® recommendation. 60 seconds of data now saves hours of guessing later. Every data point you capture joins 21 million+ real-world therapy sessions in GPT-OS® — your child's data makes every child's recommendation smarter.
Field 1: Seeking Frequency Today
🔢 How many times did child seek input unsafely today? (crashing into people/furniture): ____
Field 2: Tool Use
✅ Did child use an appropriate material today? Yes — which one?
Crash Pad / Weighted Blanket / Compression Vest / Body Sock / Lap Pad / Lycra Swing / Heavy Work / Squeeze / Burrito Roll
Crash Pad / Weighted Blanket / Compression Vest / Body Sock / Lap Pad / Lycra Swing / Heavy Work / Squeeze / Burrito Roll
Field 3: Regulation Outcome
🟢 Fully regulated (calm baseline achieved)
🟡 Partially regulated (calmer but still seeking)
🔴 Dysregulated (session abandoned — document what happened)
🟡 Partially regulated (calmer but still seeking)
🔴 Dysregulated (session abandoned — document what happened)
Research basis: ABA Data Collection Standards: BACB Guidelines + Cooper, Heron & Heward (Applied Behavior Analysis, 8th ed.) — continuous measurement (frequency, duration) as standard practice.
What If It Didn't Go as Planned? That's Data — Not Failure.
"Session abandonment is not failure — it is the most valuable data you can collect. It tells you exactly what to adjust." No parent should feel they failed because a session was difficult. The troubleshooting below addresses the most common challenges in the A-101 protocol.
❓ Child refused to engage with any material
Why: Child was not in a seeking state, or readiness assessment was missed. Next time: Wait for a natural seeking moment (child begins crashing) and then introduce the material as an alternative. Don't pre-schedule if child isn't actively seeking.
❓ Child used crash pad but continued crashing into furniture anyway
Why: Redirection to the crash pad is a learning process — it takes 2–4 weeks of consistent use before the child's seeking behavior fully redirects. Next time: Every time child crashes into furniture: immediately, calmly redirect to crash pad. "Crashes go HERE." No scolding. Repeat for weeks. Consistency — not intensity of correction — is what makes this work.
❓ Weighted blanket — child kicked it off immediately
Why: Weight may be wrong (too heavy), temperature (too warm), or full-body coverage was overwhelming for first use. Next time: Start with legs-only coverage. Try a lighter blanket. Try during screen time when child is distracted by preferred content.
❓ Burrito roll — child panicked or screamed
Why: Possibly claustrophobic response or tactile sensitivity co-occurs with proprioceptive seeking. Next time: Do NOT re-attempt roll immediately. Try a looser fold instead of a tight roll. Consult OT — this child may need a modified approach.
❓ Child used heavy work but sought crashing again 10 minutes later
Why: Heavy work provides input for approximately 1–2 hours. The child's threshold may require more frequent breaks. Next time: Increase heavy work frequency to every 60 minutes. Add a second material (compression vest) for continuous passive input between active sessions.
❓ Session escalated — child became MORE dysregulated
Why: Child was already at meltdown threshold before session began. Active materials (body sock, crash pad) can increase arousal briefly before calming. Next time: Passive-first rule for dysregulated children: weighted blanket or burrito roll ONLY until baseline is reached. Never introduce active materials during active meltdown.
❓ Child loved it and refuses to end the session
Why: This is success. The child has found something that works for their nervous system. Next time: Pre-set visual timer. Build transition warning into every session. Schedule the next session immediately: "We can do this again at [specific time]." Predictability reduces ending resistance.
🆘 If your child became severely distressed, injured, or you are concerned about a session outcome: Call 9100 181 181 (FREE Pinnacle National Autism Helpline, 18+ languages) or book an immediate teleconsultation at pinnacleblooms.org.
Adapt & Personalize: No Two Proprioceptive Seekers Are Identical
The A-101 protocol is a framework, not a rigid script. Every child's proprioceptive threshold is different. Every family's daily routine is different. Use this card to customize the protocol to your child's specific profile and intensity level.
1
⬅️ EASIER
Burrito roll only. Shorter sessions (5 min). Passive only (blanket, lap pad). Child's preferred single material. For bad sensory days.
2
STANDARD
Full 9-material rotation available. 10–20 min sessions. Passive + active mix. OT-recommended material rotation. Standard daily protocol.
3
HARDER ➡️
Extended heavy work + lycra swing combo. 20–40 min sessions. High-intensity active (crash pad + body sock + squeeze). Child-designed sensory diet. For high seeking periods.
Intense Seeker Profile
Maximum weight blanket (upper range of 10% guideline). Multiple crash pad sessions per day. Heavy work built into every daily task. Compression vest worn throughout school and home. Lycra swing before all demanding activities.
Seeker With Social Overwhelm (Temple Grandin Profile)
Controllable deep pressure preferred (squeeze machine, burrito roll child controls). Avoid materials that require parental physical contact. Body sock excellent — full-body input without social interaction. Weighted blanket during social situations.
Seeker With Co-occurring Tactile Sensitivity
Consult OT before beginning — rare but important profile. Avoid body sock. Start with weighted blanket only under child's own clothes. Burrito roll: let child control blanket texture and tightness.
Ages 2–4 | Shorter sessions (5–10 min). Burrito roll and crash pad most natural at this age. Heavy work: pushing stroller, carrying small bags. | |
Ages 5–8 | Full protocol. Introduce self-selection: "Which one do you want today?" Begins building meta-awareness. | |
Ages 8–12 | Teach the child WHY they need input. Name proprioception. Help them identify their own seeking signals. Goal: self-initiated tool use without parent prompting. |

Weeks 1–2: What Progress Actually Looks Like at This Stage
Progress: 15% — Building the Foundation
✅ You MAY See
- Child shows initial interest in at least one material from the 9
- First signs of calming within a session (body softens, movement slows)
- Child tolerates the crash pad or weighted blanket 2–3 minutes longer than day 1
- Occasional spontaneous approach to a material (most powerful early signal)
❌ You Will NOT See Yet
- Significant reduction in unsafe crashing (too early — tool-seeking is still forming)
- Child independently using materials (this comes in weeks 5–8)
- Meltdown frequency decrease (nervous system adaptation takes time)
- School reports of improved behavior (wait for week 4–6)
"Weeks 1–2 will feel slow. You may feel uncertain whether this is working. The nervous system doesn't announce its adaptation. But under the surface, new neural pathways are forming every time you offer safe proprioceptive input. Your consistency now is building the architecture for week 8 mastery. Keep going."
IF YOUR CHILD TOLERATES THE MATERIAL FOR 3 SECONDS LONGER THAN LAST WEEK — THAT IS REAL PROGRESS. Research: PMC11506176 — SI intervention outcomes emerge across 8–12 week timelines. Early-phase indicators focus on tolerance and participation, not skill mastery.

Weeks 3–4: The Nervous System Is Learning to Prefer the Tool
Progress: 40% — Neural Pathways Forming
This is the consolidation phase. The nervous system has had enough repetition to begin forming preferences. You may notice your child orienting toward the tools before being offered them — this is the earliest sign of self-regulation emerging.
Anticipation
Child approaches crash pad or asks for blanket before becoming dysregulated — a profound early self-regulation sign. The nervous system is learning to anticipate the input.
Preference Formation
Child shows clear preference for one or two materials from the 9. This preference is clinical data — it tells you which input modality is most regulating for your specific child.
First Spontaneous Requests
"Can I do my burrito?" — even once — is a consolidation milestone. The child is beginning to connect the input to the feeling of regulation.
Shorter Post-Session Recovery
Child returns to focused activity more quickly after session ends. Duration of calm after input is increasing — a measurable indicator of protocol effectiveness.
Parent milestone: "By week 3–4, you may notice you feel more confident. You're starting to read your child's seeking signals before the crash. You can see the wave before it breaks. That situational awareness — that is your expertise growing." If seeking has not reduced at all by week 4, consult OT. The material weight/intensity may need adjustment.
Weeks 5–8: Mastery Indicators — Self-Regulation Emerging
Progress: 75% — Mastery Within Reach
These are specific, observable, measurable mastery criteria — not vague improvements. Each one has a defined threshold. Use these to know when your child has truly mastered A-101 and is ready to progress.
Mastery Indicator | What It Looks Like | Measurement | |
Tool selection | Child independently chooses appropriate tool when seeking urge arises | ≥3 spontaneous tool uses per week without prompting | |
Unsafe seeking reduction | Crashing into furniture/people significantly decreased | ≤25% of week-1 baseline frequency | |
Generalization | Child uses tools in new settings (grandparents' house, school, travel) | Reports from other caregivers | |
Communication | Child can verbalize or signal their proprioceptive need | "I need my blanket" / "Can I crash?" / AAC symbol use | |
Session independence | Child initiates session start without parent prompt | ≥2 times per week child goes to material without being offered |
🏆 A-101 Mastery Badge Unlocked
"PROPRIOCEPTIVE SELF-REGULATION"
✅ Consistent tool use without prompting
✅ Unsafe seeking reduced ≥75%
✅ Generalization to 2+ settings
✅ Consistent tool use without prompting
✅ Unsafe seeking reduced ≥75%
✅ Generalization to 2+ settings
When to Move Forward
→ Child meets mastery criteria → proceed to A-102 (Vestibular Seeking).
→ Meets criteria in some but not all settings → maintain and generalize before advancing.
→ Not met by week 8 → consult OT via 9100 181 181.
→ Meets criteria in some but not all settings → maintain and generalize before advancing.
→ Not met by week 8 → consult OT via 9100 181 181.

Celebrate This Win — You Did This.
Eight weeks ago, you were exhausted and confused by a child who crashed into everything and asked for hugs that were never tight enough. You may have been told to "set firmer limits." You may have been made to feel the crashing was a discipline problem. You kept going anyway.
You learned the science. You gathered the materials. You built the protocol. You tracked the data. You adapted. You stayed consistent. The child who now reaches for their crash pad instead of their sibling. The child who asks for their burrito roll at bedtime. The child who wears their compression vest to school and comes home more regulated. That is your work. That is 8 weeks of your commitment made visible.
✅ What You've Achieved
- Proprioceptive seeking is now meeting a safe, appropriate outlet
- Your home has been transformed into a regulated sensory environment
- Your child's nervous system has learned it can trust that the input will come
- You have acquired a clinical skill — you can read proprioceptive seeking and respond
📸 Family Milestone
Document this milestone. Take a photo of your child with their favourite material. Write the date. In 6 months, when they're independently choosing their crash pad or asking for their squeeze vest — look back at this moment. Then share with the Pinnacle Parent Community.

Red Flags: Even in the Celebration Zone — Know These Warning Signs
This card exists not to frighten you, but to empower you with specific thresholds. Most families will never need this card. Read it once and keep it as your clinical guardrail. Trust your instincts — you have 8 weeks of data and daily observation of your child.
Red Flag | What It Looks Like | Why It Matters | Action | |
Increasing pain insensitivity | Child appears not to feel injuries, doesn't react to knocks | May indicate broader sensory underresponsivity requiring NeuroDev evaluation | Teleconsult or clinic visit | |
Seeking intensity escalating | At week 6–8, crashing is MORE frequent, not less | Protocol may need OT adjustment; sensory threshold may be shifting | OT consultation urgently | |
Skin/circulation changes | Red marks, mottled skin from compression materials | Compression fit is wrong or duration is too long | Stop compression; adjust fit | |
Regression after improvement | Child reverts to week-1 seeking intensity after progress | May signal environmental stressor, health change, or new sensory challenge | Note triggers, consult OT | |
Sleep disruption | Weighted blanket use is disrupting sleep | Weight, temperature, or fabric may need adjustment | Modify weighted blanket protocol | |
Injuries to self or others | Child seeks input through self-harm or injuring others | Behavioral overlay requiring ABA consultation alongside OT | Immediate consultation |
Escalation Pathway: Issue arises → Self-resolve with card guidance (try 3 days) → If not resolved: GPT-OS® Helpline 9100 181 181 (FREE, 18+ languages) → Teleconsultation with Pinnacle OT → In-person clinic visit → NeuroDev Pediatrician assessment (if flagged by OT). 📧 care@pinnacleblooms.org | 🌐 pinnacleblooms.org

The Progression Pathway — Your Developmental GPS
You are here. A-101 is mastered. Here is where we go next. The progression pathway is determined by your child's primary remaining sensory challenge — not by a fixed sequence. Choose the next technique based on what you observe most.
Code | Technique | Description | Materials Overlap | |
A-100 | Oral Seeking (prev.) | Chewing, mouthing | Different materials | |
A-101 | Bear Hugs ← YOU ARE HERE | Deep pressure seeking | All 9 materials | |
A-102 | Vestibular Seeking | Spinning, swinging | Lycra swing shared ✓ | |
A-103 | Crashing Into Things | Impact seeking | Crash pad, heavy work ✓ | |
A-107 | Seeking Tight Spaces | Enclosure seeking | Body sock, burrito roll ✓ |
Unsure of your next step? Call GPT-OS® Helpline: 9100 181 181 for a personalized progression pathway recommendation based on your child's current profile.

Related Techniques in This Domain: Your Technique Neighbourhood
All 8 techniques in the Proprioceptive/Deep Pressure cluster of the Sensory Domain. The good news: materials you already own from A-101 overlap significantly with the next techniques — your investment compounds across the entire cluster.
A-101 — Seeks Bear Hugs ← You Are Here
All 9 materials from this page. Core technique. ✅ Complete
A-102 — Vestibular Seeking (Spinning, Swinging)
Core difficulty. Lycra swing ✓ from A-101. Next recommended technique for most seekers.
A-103 — Crashes Into Things/People
Core-Advanced. Crash pad ✓ Heavy work kit ✓ from A-101. Builds directly on this protocol.
A-105 — Uses Too Much Force
Core difficulty. Heavy work kit ✓ from A-101. Closely related seeking profile.
A-107 — Seeks Tight Spaces
Core difficulty. Body sock ✓ Burrito roll ✓ from A-101. Strong materials overlap.
A-108 — Prefers Heavy Blankets/Objects
Introductory. Weighted blanket ✓ from A-101. Often the first technique for younger seekers.
Your Child's Full Developmental Map — A-101 Is One Piece of a Larger Plan
One technique inside a complete developmental plan. GPT-OS® maps your child's entire developmental profile across all 12 domains — identifying which techniques to prioritize, in which sequence, at which intensity. This is not one parent navigating alone. This is a system designed for your child.
Why All 12 Domains Matter
A — Sensory: Tactile, proprioceptive, vestibular, visual, auditory processing
B — Social Communication: Eye contact, joint attention, social reciprocity
C — Emotional Regulation: Meltdown management, frustration tolerance
D — Behavior/Flexibility: Transitions, rigidity, repetitive behaviors
E — Feeding/Oral: Food acceptance, oral motor, mealtime behavior
F — Play/Learning: Imitation, pretend play, academic readiness
B — Social Communication: Eye contact, joint attention, social reciprocity
C — Emotional Regulation: Meltdown management, frustration tolerance
D — Behavior/Flexibility: Transitions, rigidity, repetitive behaviors
E — Feeding/Oral: Food acceptance, oral motor, mealtime behavior
F — Play/Learning: Imitation, pretend play, academic readiness
GPT-OS® Full Profile
G — Communication: Verbal language, AAC, comprehension
H — Sleep: Sleep onset, maintenance, regulation
I — Self-Care: Dressing, hygiene, toileting
J — Motor Skills: Gross/fine motor, coordination
K — Adaptive: Daily living skills, independence
L — Executive Function: Attention, planning, working memory
H — Sleep: Sleep onset, maintenance, regulation
I — Self-Care: Dressing, hygiene, toileting
J — Motor Skills: Gross/fine motor, coordination
K — Adaptive: Daily living skills, independence
L — Executive Function: Attention, planning, working memory
WHO/UNICEF Nurturing Care Framework: 5 components of nurturing care require holistic developmental monitoring. WHO NCF (2018) | UNICEF 2025 Country Profiles.
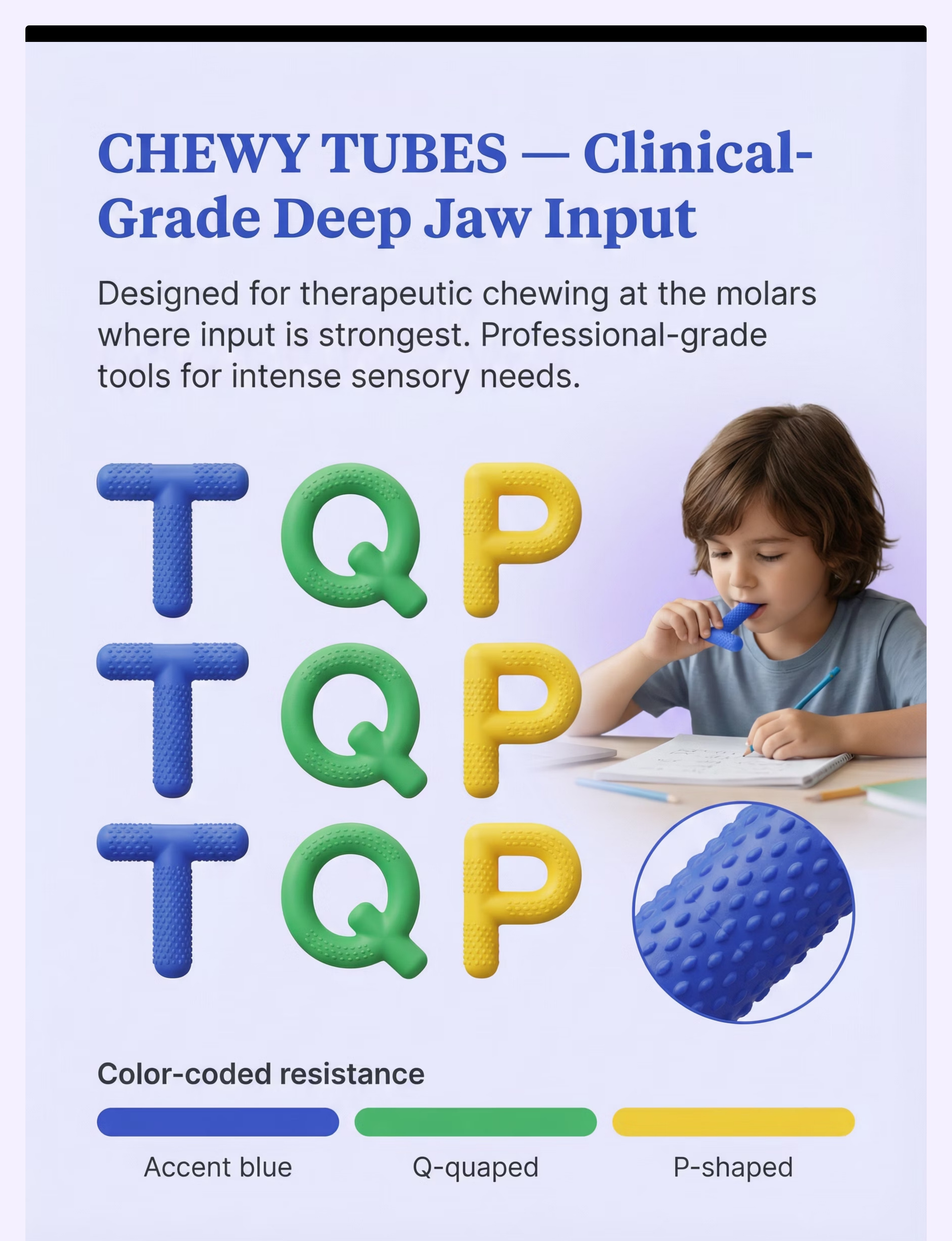
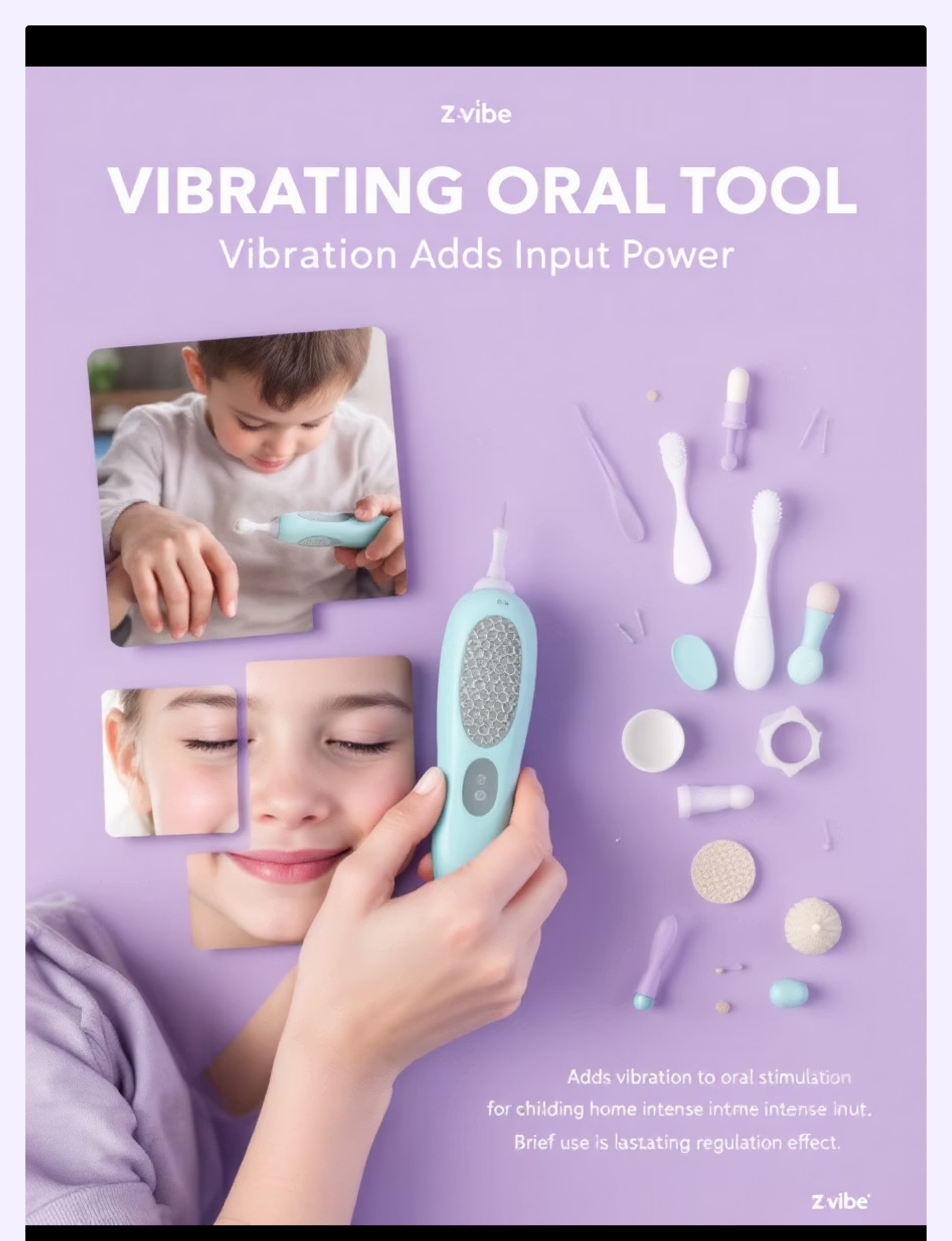
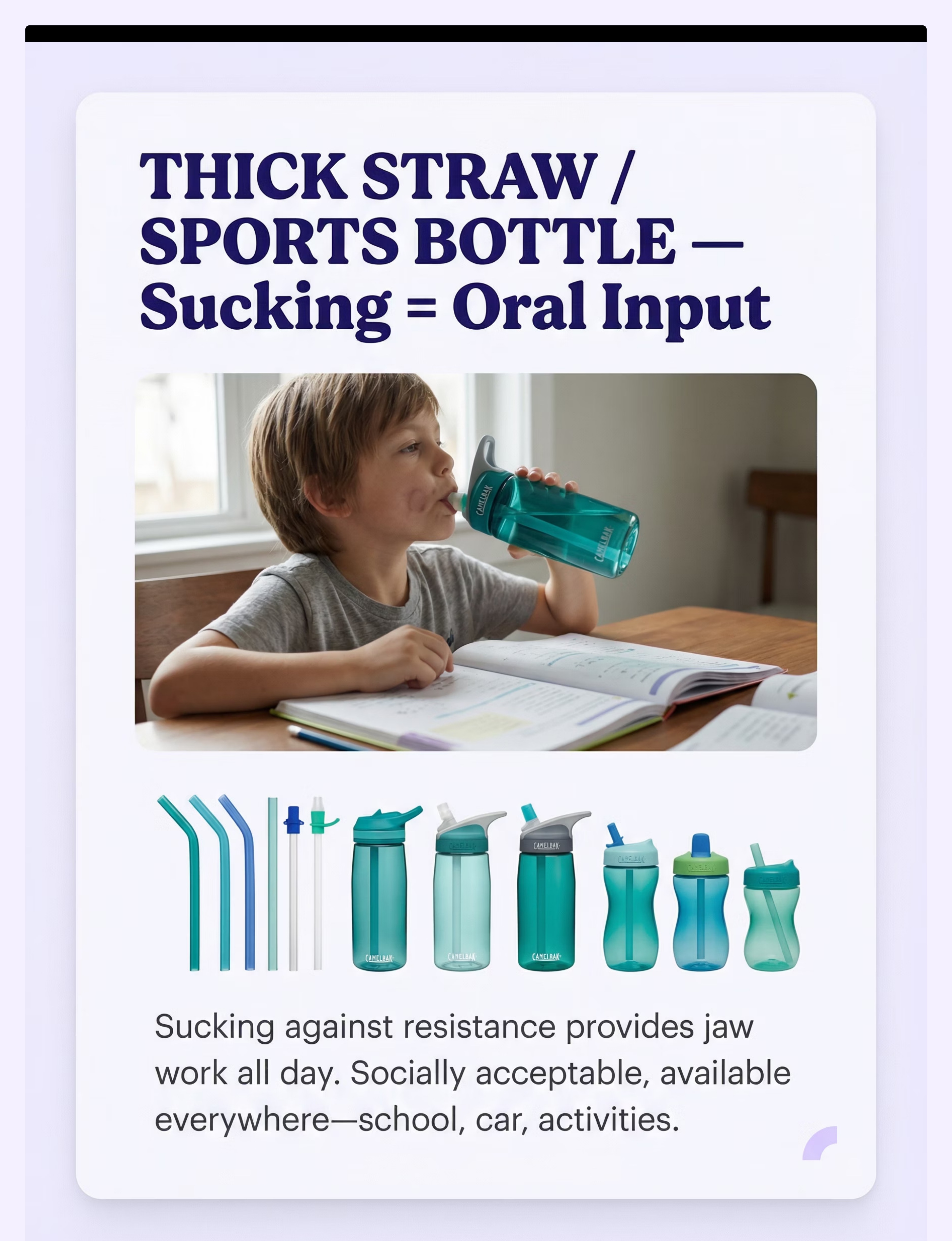
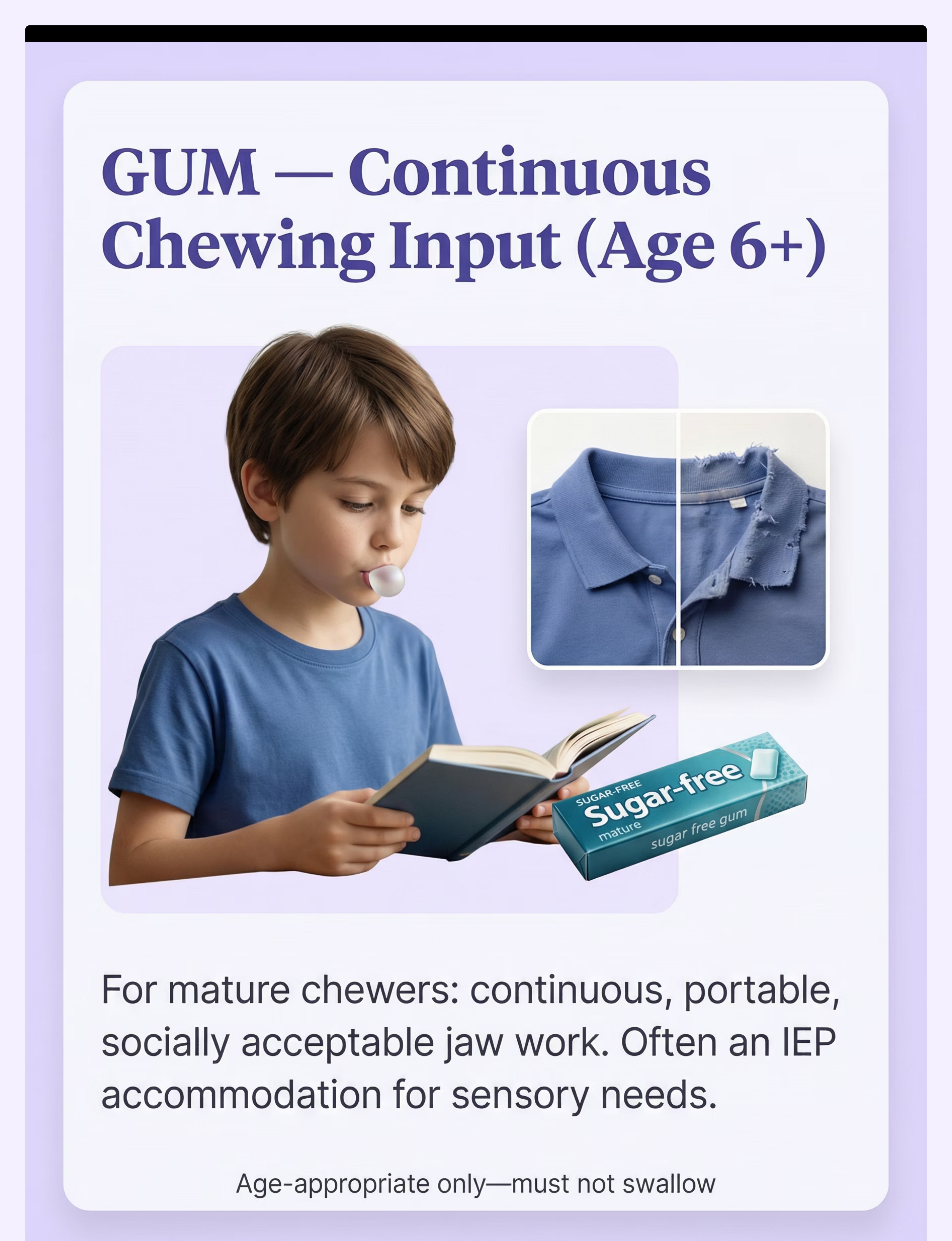
Preview of 9 materials that help when child chews everything Therapy Material
Below is a visual preview of 9 materials that help when child chews everything therapy material. The pages shown help educators, therapists, and caregivers understand the structure and content of the resource before use. Materials should be used under appropriate professional guidance.




Link copied!
Families Who've Been Here: Three Journeys, One Pattern — It Gets Better
These are clinical narratives — honest, specific, and grounded in what actually happens across Pinnacle centers. Not promotional copy. Real patterns from real families navigating exactly what you are navigating.
Arjun, 4 years — Hyderabad
Challenge: Arjun crashed into furniture and walls 40–60 times daily, hugged his younger sister with enough force to knock her down, and could not sit for any activity longer than 90 seconds. His family had tried "firm boundaries" for 18 months. Nothing changed.
What changed: Crash pad in the corner near the couch. Weighted blanket at his homework chair. Burrito roll became his "bedtime game."
By week 6: Crashing frequency reduced to approximately 8–12 times daily. He began walking to the crash pad before his sister came home from school — independent regulation timing.
What changed: Crash pad in the corner near the couch. Weighted blanket at his homework chair. Burrito roll became his "bedtime game."
By week 6: Crashing frequency reduced to approximately 8–12 times daily. He began walking to the crash pad before his sister came home from school — independent regulation timing.
"We were told he was 'out of control.' He was never out of control. He was asking for something. When we gave it to him, he settled. Just like that." — Arjun's mother
🩺From the Therapist: Arjun's profile is textbook proprioceptive under-responsivity. The seeking behavior was not behavioral — it was neurological. Once the environment was equipped, the nervous system found what it needed. — OT, Pinnacle Hyderabad Center
Diya, 7 years — Bengaluru
Challenge: Diya's teacher called weekly about her "rough play" — hugging classmates too hard, bumping into peers, unable to sit at her desk. Her parents were embarrassed and frightened. School had suggested possible suspension.
What changed: Compression vest under her school uniform. Weighted lap pad at her desk. A "heavy work helper" role at school — daily book-carrying responsibility.
By week 5: Teacher reported Diya was sitting for full class periods for the first time. Peer complaints stopped.
What changed: Compression vest under her school uniform. Weighted lap pad at her desk. A "heavy work helper" role at school — daily book-carrying responsibility.
By week 5: Teacher reported Diya was sitting for full class periods for the first time. Peer complaints stopped.
"She hasn't changed. Her environment changed. And everything changed." — Diya's father
🩺From the Therapist: School-based proprioceptive accommodations are among the most impactful interventions we provide. Invisible tools delivering continuous therapeutic input throughout the school day. — SpEd Coordinator + OT, Pinnacle Bengaluru
Rahul, 9 years — Mumbai
Challenge: By age 9, Rahul's seeking behaviors had become socially isolating. He had no friends because he hugged "too hard" and couldn't stop crashing games. His self-awareness was causing him visible distress.
What changed: OT taught Rahul the word "proprioception" and explained what his body was doing. He was involved in choosing his materials. He learned to recognize his seeking urge before it expressed as a crash.
By week 8: Rahul had shared his "squeeze vest" with one friend and explained why he wore it. He now asks for a "heavy work break" at school using his own language.
What changed: OT taught Rahul the word "proprioception" and explained what his body was doing. He was involved in choosing his materials. He learned to recognize his seeking urge before it expressed as a crash.
By week 8: Rahul had shared his "squeeze vest" with one friend and explained why he wore it. He now asks for a "heavy work break" at school using his own language.
"Teaching him the science of his own body was the most powerful thing anyone had done for him. He stopped feeling like something was wrong with him." — Rahul's mother
🩺From the Therapist: For older children, metacognitive awareness of their sensory profile is a transformational intervention. When a child can name their need, they can communicate it rather than act it out. — OT + NeuroDev, Pinnacle Mumbai
All vignettes are illustrative composites based on clinical patterns at Pinnacle centers. Names changed. Individual outcomes vary.