Sensory Solutions Series — Episode A-020
Tactile Processing · Ages 2–12
"Her skin is cracking. She needs lotion. But she screams like I'm hurting her."
You hold the bottle. You see the dry, bleeding skin. You know she needs it. And yet — the moment lotion touches her arm, she fights you like you're causing her pain. You're not imagining this. You're not failing. And you are not alone.
"Her skin is cracking and bleeding from dryness. The doctor says she needs lotion twice a day. But the moment I try to put it on, she screams like I'm hurting her. I feel like I'm choosing between her skin health and her mental health."
— Parent, Pinnacle Blooms Network intake
Domain
Tactile Processing — Touch Defensiveness
Age Band
2–12 years
Setting
Home
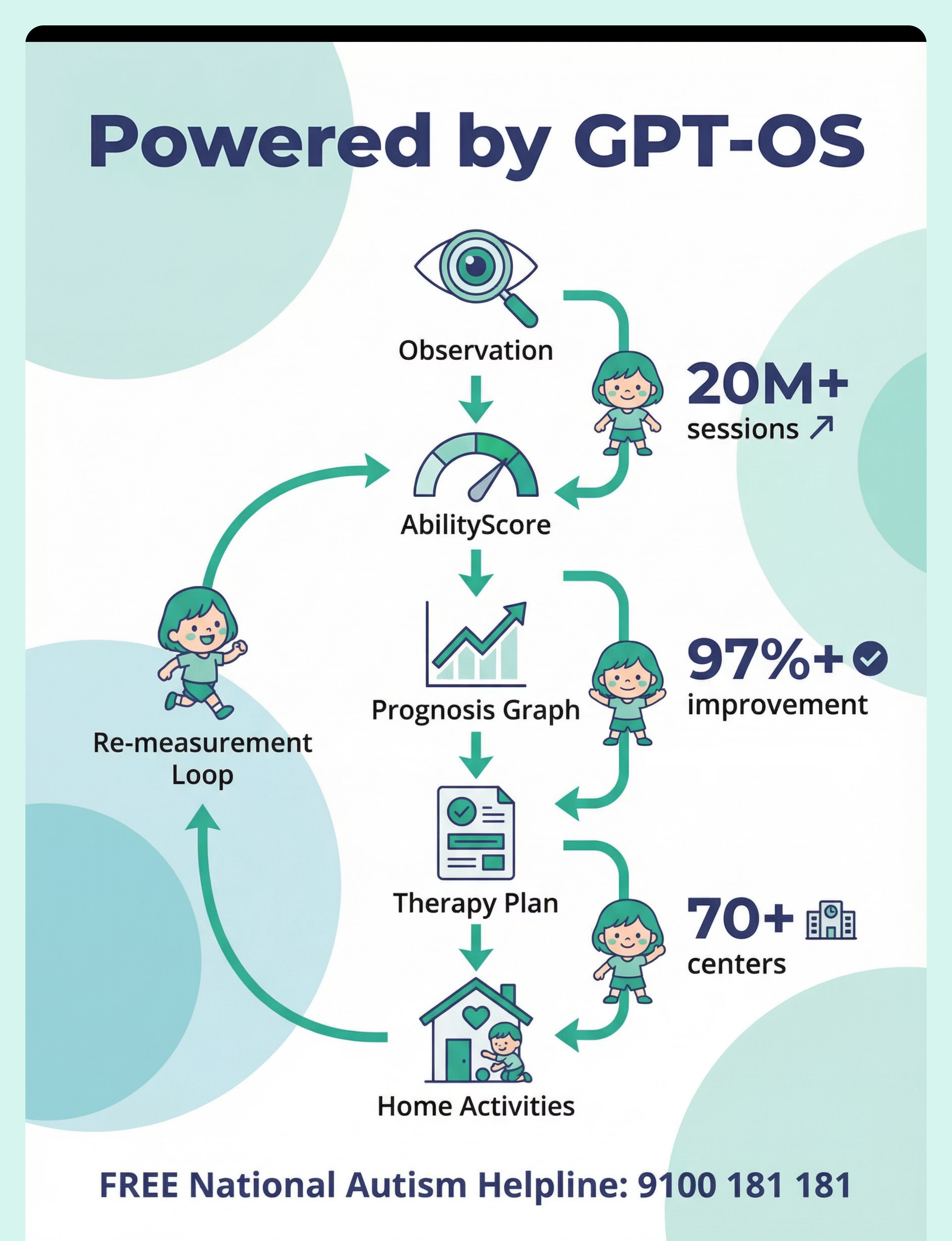
Powered by
GPT-OS® Therapy Intelligence
Pinnacle Blooms Network® — Built by Mothers. Engineered as a System.

You're Not Alone — This Is One of the Most Common Daily Battles
Tactile over-responsivity — the clinical term for what your child experiences when lotion touches skin — affects a significant proportion of children on the autism spectrum. Research published in Frontiers in Integrative Neuroscience (2020) estimates that 60–95% of children with ASD demonstrate some form of sensory processing difference, with tactile defensiveness being one of the most functionally impactful presentations.
Across the Pinnacle Blooms Network, lotion and moisturizer resistance is among the top 10 personal care challenges reported by parents during intake assessments. This is not rare. This is not strange. This is one of the most common daily battles families face — and it has solutions.
60–95%
Children with ASD
show some form of sensory processing difference
#1
Personal Care Battle
lotion/moisturizer application reported by parents at intake
20M+
Sessions
across the Pinnacle Blooms Network confirm this challenge is universal
Research: Frontiers in Integrative Neuroscience (2020) · DOI: 10.3389/fnint.2020.556660 | SPD Foundation clinical data | Pinnacle Blooms Network intake assessment database

Where This Sits in Development
Tactile defensiveness with moisturizer aversion typically emerges between ages 1–3 as personal care routines establish, and can persist into adolescence without intervention. It sits within the broader developmental domain of sensory processing — specifically tactile modulation — and intersects critically with the Activities of Daily Living (ADL) milestone trajectory.
0–6 Months
Tactile system developing; early signs of sensitivity to textures may appear
6–18 Months
Tactile preferences forming; bath/lotion resistance may begin to emerge
18 Months–3 Years ★
Peak Emergence Zone — personal care routines collide with tactile defensiveness. Most families seek help here.
3–6 Years
Patterns consolidate; compensatory behaviors develop; social awareness increases
6–12 Years
Social impact increases; self-care independence expected but blocked; intervention urgency grows
Lotion aversion commonly co-occurs with: sunscreen resistance, bath time meltdowns, hair brushing resistance, clothing texture sensitivity, food texture selectivity, and resistance to medical topical treatments. · Research: WHO Care for Child Development Package (2023) | PMC9978394 | UNICEF MICS developmental monitoring indicators

Evidence Grade: Level II
Supported by Systematic Reviews and RCTs
The Evidence Behind This Technique
Sensory integration intervention — the foundation of this technique — meets criteria to be classified as an evidence-based practice for children with ASD, based on a PRISMA Model Systematic Review (2024) analyzing 16 articles from 2013–2023. A separate meta-analysis published in World Journal of Clinical Cases (2024) across 24 studies confirmed that sensory integration therapy effectively promoted adaptive behavior, sensory processing, and motor skills.
Indian-specific evidence from Padmanabha et al. (2019) demonstrated significant outcomes from home-based sensory interventions in pediatric populations — validating that this approach works in real homes, not just clinical settings.
16 Studies
2013–2023 confirm evidence-based practice status for sensory integration
24-Study Meta-Analysis
Confirms functional improvement in adaptive behavior and sensory processing
Home-Based Validated
Indian pediatric populations — results in real homes, not just clinics
20M+ Sessions
Real-world Pinnacle Blooms data confirms operational effectiveness
"Clinically validated. Home-applicable. Parent-proven."
Research: PMC11506176 — PRISMA Systematic Review (2024) | PMC10955541 — Meta-analysis, World J Clin Cases (2024) | DOI: 10.1007/s12098-018-2747-4 — Padmanabha et al., Indian J Pediatr (2019)
The Technique
A-020 · Sensory Processing · ADL
Sensory-Adapted Moisturizer Format Selection
Parent-Friendly Name: "Finding the Right Way to Moisturize Your Sensory-Sensitive Child"
A systematic approach to resolving the conflict between a child's tactile defensiveness and their medical need for skin moisturizing. Rather than forcing the child to tolerate conventional lotion — which triggers genuine sensory distress — this technique identifies alternative moisturizer formats (solid bars, sprays, oils, bath oils) that deliver the same skin care through completely different sensory profiles, combined with application modifications (warming, self-application, deep pressure prep) that reduce the neurological defensive response.
Domain
Sensory Processing (A) · Tactile Processing (SEN-TAC) · Daily Living (ADL)
Duration & Frequency
5–15 minutes per session · Daily (aligned with skin care needs)
Setting & Age
Home — bathroom/bedroom · Ages 2–12 years
Canon Materials
Body Care Products · Sensory Preparation Tools

Who Uses This Technique
This technique crosses therapy boundaries — because the brain doesn't organize by therapy type. Four disciplines collaborate to deliver the best outcomes for lotion-avoidant children.
🟣 Occupational Therapist (OT) — Primary Lead
Designs the sensory integration protocol — selects alternative formats based on the child's specific tactile profile, implements systematic desensitization, and monitors sensory processing improvements over time.
🔵 Board Certified Behavior Analyst (BCBA) — Secondary
Structures the behavioral protocol — reinforcement schedules for tolerance building, graduated exposure hierarchies, data collection on tolerance duration, and functional behavior assessment of the avoidance response.
🟢 Speech-Language Pathologist (SLP) — Supporting
Addresses the communication component — building the child's ability to express sensory preferences, request modifications, and communicate tolerance levels using AAC if needed.
🟠 NeuroDevelopmental Pediatrician — Supporting
Coordinates the medical-sensory interface — ensuring the moisturizing approach meets dermatological needs while accommodating the sensory profile. May coordinate with pediatric dermatologist.
Research: DOI: 10.1080/17549507.2022.2141327 — Adapted UNICEF/WHO Nurturing Care Framework for SLPs (Int J Speech-Lang Pathol, 2022)
What This Technique Targets
This technique is designed with layered targets — from the immediate goal of tolerating moisturizer to the long-term goal of independent self-care. Each layer of progress builds toward the next.
Primary Target
Tolerance of topical moisturizer application — measured by duration, body area coverage, and distress level during application
Secondary Targets
Self-care independence in hygiene · Skin health maintenance · Reduction in anticipatory anxiety · Parent-child interaction quality during care routines
Tertiary Targets
Generalized tactile tolerance · Body awareness and interoception · Self-regulation during aversive sensory experiences · ADL independence
Observable Behavior Indicators — Measuring Success
Child remains calm during moisturizer application for ≥2 minutes
Child does not attempt to wipe off product within 5 minutes
Child accepts application on ≥3 body areas
Child self-applies with supervision
Research: PMC10955541 — Meta-analysis confirming SI therapy targets: social skills (primary), adaptive behavior (secondary), sensory processing and motor skills (tertiary)

The 9 Materials: Your Quick Reference Guide
These 9 materials address lotion avoidance through two strategies: Alternative Formats (completely different sensory profiles than conventional lotion) and Application Modifications (changing how any moisturizer is delivered). Together, they cover every tactile trigger profile.
# | Material | Price Range (INR) | Type | |
1 | Solid Lotion Bars | ₹300–900 | Alternative Format | |
2 | Spray Moisturizers / Oil Sprays | ₹400–1,200 | Alternative Format | |
3 | Pure Oils (Coconut, Jojoba, Sweet Almond) | ₹200–800 | Alternative Format | |
4 | Bath Oils / In-Shower Moisturizers | ₹300–1,500 | Alternative Format | |
5 | Warming Technique | ₹0 | Application Modification | |
6 | Fragrance-Free / Hypoallergenic Formulas | ₹200–1,000 | Application Modification | |
7 | Fast-Absorbing / Non-Greasy Formulas | ₹300–1,200 | Application Modification | |
8 | Self-Application Tools (pump bottles, applicators) | ₹0–600 | Application Modification | |
9 | Sensory Prep — Deep Pressure | ₹0 | Preparation Technique |
Essential Starter Kit (Pinnacle Recommends): 1× Solid lotion bar · 1× Pure jojoba or coconut oil · 1× Fragrance-free lightweight lotion · Total Starter Investment: ₹500–1,500 · Available at Amazon.in — search "solid lotion bar kids" | "fragrance free baby moisturizer" | "jojoba oil pure"

Material 1
Solid Lotion Bars — The Game-Changer for Texture Sensitivity
Solid lotion bars are the single most transformative material for texture-sensitive children. Unlike conventional lotion, they are completely dry to the touch — no wet, no creamy, no sticky. The bar melts only when it contacts warm skin, delivering moisture through body heat alone. For children whose primary trigger is the wet/creamy texture of conventional lotion, this format eliminates the trigger entirely.
Buy This
Commercial solid lotion bars — search "solid lotion bar kids" on Amazon.in · Price: ₹300–900 · Look for: shea butter base, fragrance-free, no nut allergens
Make This (DIY Version)
Melt coconut oil + shea butter + beeswax in a 2:2:1 ratio using a double boiler. Pour into silicone molds or ice cube trays. Cool until solid. Store at room temperature. Same experience — zero cost if you have ingredients.
No rubbing required — glide the bar directly on skin
Child can self-apply — holding a bar feels safe and controlled
No greasy residue — absorbs cleanly as it melts

Material 2
Spray Moisturizers — Zero Rubbing, Zero Residue
Spray moisturizers are the fastest, lowest-contact format available. A fine mist deposits moisture on skin without any rubbing, spreading, or sustained touch. For children whose primary trigger is the act of being touched by another person, spray format eliminates that trigger entirely. The application is over in seconds — before the sensory system can mount a full defensive response.
Buy This
Spray moisturizers or body oil sprays — search "body mist moisturizer fragrance free" on Amazon.in · Price: ₹400–1,200 · Look for: lightweight, fast-absorbing, no alcohol
Make This (DIY Version)
Mix 3 parts distilled water + 1 part light oil (jojoba or sweet almond) + a few drops vitamin E in any spray bottle. Shake well before each use. Use within 2 weeks (no preservatives). Cost: near zero.
Application Tip: Spray once into the air first so child sees and hears the mist — no surprises. Then spray on your own arm to demonstrate. Then offer to spray child's arm. The child feels in control throughout.
Material 3
Pure Oils — Coconut, Jojoba, Sweet Almond
Pure oils present a fundamentally different sensory experience than conventional lotion. They feel smooth and "clean" rather than thick and creamy, absorb without leaving a white residue, and have no synthetic chemicals or binding agents that can feel strange on skin. Jojoba oil in particular is chemically similar to the skin's own sebum — making it feel like "nothing" to many tactile-sensitive children.
Coconut Oil
Likely already in your kitchen. Warm slightly between palms. Solid at room temp, liquid when warm. Cost: ₹0 if you already own it.
Jojoba Oil
Most skin-similar of all oils. Technically a liquid wax — non-greasy, fast-absorbing. Ideal for face and sensitive areas.
Sweet Almond Oil
Lightweight, neutral scent, excellent for dry skin and eczema. ⚠️ Avoid if nut allergy present.
Allergy Warning: Coconut and almond oils are nut-derived. Perform a patch test on inner forearm and wait 24 hours before full application. Consult your physician if any nut allergy history is present.

Material 4
Bath Oils — Moisturizing Without a "Lotion Event"
Bath oils are the most powerful tool for children who resist all forms of direct topical application. Added to bathwater, they coat the skin during bathing — delivering full-body moisturizing without any separate lotion event, no direct application, and no rubbing. From the child's perspective, they're simply taking a bath. The moisturizing happens invisibly.
How to Use
Add 1–2 tablespoons of bath oil (or pure oil) to warm bathwater after filling. Allow child to bathe as normal. Pat dry gently — do not rub. The oil coating remains on skin post-bath, providing lasting moisture. No separate lotion step needed.
Price range: ₹300–1,500 for commercial bath oils. Pure coconut or jojoba oil from your kitchen works identically at zero additional cost.
Why It Works
Zero direct application. Child is already in water — a familiar sensory context. No "lotion time" trigger. Skin is moisturized by the time they leave the tub. Ideal as a starting point for severely avoidant children.
Safety: Oil makes bathtub surfaces extremely slippery. Always use a non-slip bath mat. Supervise at all times. Apply bath mat before adding oil to water.

Material 5
Warming Technique — Eliminate the Cold Shock Trigger
The cold shock of lotion from a bottle is one of the most powerful tactile defensiveness triggers — and one of the easiest to eliminate entirely, at zero cost. Warming any moisturizer to body temperature before application removes the temperature trigger completely, often dramatically reducing distress even with conventional lotion.
That's it. No special product needed. Rub any lotion between your palms for 15–20 seconds before applying. The warmth removes the cold shock trigger and simultaneously signals to the child that your hands are approaching — reducing the startle response from unpredictable touch.
Let child feel your warm hands first — before product contacts skin
Never microwave lotion — warm to body temperature only (test on your own wrist)
Store products in a warm location (not cold bathroom cabinet) to reduce starting temperature
Cost: ₹0 · This modification works with any moisturizer format and should be standard practice regardless of which product you choose.

Material 6
Fragrance-Free & Hypoallergenic Formulas
For children with fragrance as a primary sensory trigger, switching to a truly fragrance-free formula is not optional — it is foundational. Fragrance is processed by both the tactile and olfactory systems simultaneously, compounding the sensory load. Eliminating it removes an entire layer of the defensive response before application even begins.
"Fragrance-Free" ✅
Contains no added fragrance compounds whatsoever. This is the label you want. Safer choice. Look for: CeraVe, Vanicream, Dove Sensitive, or any pediatric-labeled fragrance-free moisturizer.
"Unscented" ⚠️
May still contain masking fragrances — added to cover the smell of other ingredients. The word "unscented" does not mean fragrance-free. Always check the ingredient list for "fragrance," "parfum," or "perfume."
Price range: ₹200–1,000. Available at medical pharmacies, baby care sections, and online. When in doubt, choose pediatric formulas — they are held to higher sensitivity standards than adult products.

Material 7
Fast-Absorbing & Non-Greasy Formulas
For children whose primary trigger is the residue — the persistent greasy or sticky feeling that doesn't go away after lotion application — fast-absorbing, non-greasy formulas address the problem at its source. These lightweight gel-based or water-based moisturizers absorb within 30–60 seconds, leaving minimal detectable residue on the skin surface.
Fast Absorption
Look for gel-based or "aqua" formulas. Water-based moisturizers absorb 2–3x faster than oil-based creams. Residue is minimal or undetectable within 60 seconds.
Non-Greasy Texture
Avoid: petroleum jelly (Vaseline), heavy ointments, thick creams. Choose: lightweight lotions, gel moisturizers, or water-cream hybrids labeled "non-greasy."
Allow Absorption Time
Even fast-absorbing formulas need 3–5 minutes before clothing contact. Build this buffer into the routine. Use a timer the child can see — it creates a clear endpoint.
Price range: ₹300–1,200. Brands to look for: Neutrogena Hydro Boost, Cetaphil Light Hydrating Lotion, or any pediatric "daily lotion" marketed as lightweight.

Material 8
Self-Application Tools — Give Your Child Control
For children whose primary trigger is touch by others — the unpredictability and loss of control inherent in being touched — self-application tools transfer control directly to the child. When the child applies the moisturizer themselves, the touch becomes predictable, controllable, and self-initiated, which dramatically reduces the neurological defensive response.
Pump Dispensers
Child controls how much product comes out. No parent hands needed on the bottle. Child squirts product onto their own palm and self-applies. Price: ₹0 (repurpose any pump bottle).
Foam Rollers / Applicators
Extend the application tool so child isn't directly touching the product or being touched. Available at beauty supply stores. Price: ₹200–600.
Mirror Setup
Place a mirror so child can watch their own application. Seeing the touch coming (proprioceptive preview) reduces startle response and increases sense of control. Price: ₹0.

Material 9
Sensory Prep — Deep Pressure Before Lotion Time
Deep pressure is one of the most well-researched sensory regulation tools available. Applied 2 minutes before lotion time, firm joint compressions and deep pressure input "prime" the tactile system — shifting it from a hypervigilant defensive state to a more regulated, receptive state. Children who receive deep pressure prep typically tolerate lotion application significantly better than those who do not.
This is Material 9 — but consider it the foundation of all other materials. Regardless of which moisturizer format you choose, beginning every session with 2 minutes of deep pressure prep sets the nervous system up for success. Cost: ₹0. Equipment needed: your hands.
How to do it: Firm palm squeezes down your child's arms and legs (like squeezing a tube of toothpaste from shoulder to hand). Joint compressions at elbows, wrists, knees, ankles. Firm, predictable pressure — not light or ticklish touch. 2 full minutes before lotion application begins. · Equity Statement: Every parent, regardless of economic status, can execute this technique TODAY with household items.

DIY & Substitute Options for Every Budget
Every one of the 9 materials has a zero-cost or near-zero-cost substitute. Evidence-based sensory intervention does not require purchasing anything new. The technique works with what you already own.
DIY Solid Lotion Bars
Melt coconut oil + shea butter + beeswax in a 2:2:1 ratio in a double boiler. Pour into ice cube trays. Cool until solid. Same experience as commercial bars — identical sensory profile. Cost: ₹50–150 for ingredients.
DIY Spray Moisturizer
3 parts distilled water + 1 part jojoba or sweet almond oil + few drops vitamin E in any spray bottle. Shake before use. Use within 2 weeks. Cost: ₹0 if you have a spare spray bottle and oil.
Coconut Oil — Already In Your Kitchen
The coconut oil in your pantry is chemically identical to "body oil" sold in beauty stores. Warm between palms before applying. Cost: ₹0 additional.
Warming Technique — Zero Cost
Rub any lotion between palms for 15–20 seconds. Removes cold shock trigger. No new product needed.
Deep Pressure Prep — Zero Cost
Firm palm squeezes and joint compressions using only your hands. 2 minutes before lotion time. Clinically validated preparation technique. No equipment needed.
"Every parent, regardless of economic status, can execute this technique TODAY with household items."
Safety First
Read Before You Begin
Safety Guidelines: Before You Start Any Session
These safety guidelines protect both your child's skin health and their sensory wellbeing. Review this card every time you introduce a new product or modify your approach.
🔴 Do NOT Proceed If
Child has known allergy to any ingredient · Skin shows signs of infection (spreading redness, warmth, pus, fever) · Child has open wounds requiring medical dressing · Child is in active meltdown — this is preparation, not crisis intervention
🟡 Modify If
Child has diagnosed eczema — coordinate with pediatric dermatologist · Child takes prescription topical medications — consult physician · Oil-based products make surfaces slippery — use bath mat, supervise · DIY products: use within 2 weeks, no preservatives
🟢 Always Do
Patch test every new product on inner forearm · Wait 24 hours before full application · "Fragrance-free" is safer than "unscented" · Warm to body temperature ONLY — never microwave · Test temperature on your own skin first
🚨 Red Line — Stop Immediately If: skin rash, hives, breathing changes, or any sign of allergic reaction appears. Seek medical attention. · Research: DOI: 10.1007/s12098-018-2747-4 — Padmanabha et al.: Home-based sensory intervention safety protocols | National Eczema Association guidelines

Set Up Your Space: The Ideal Environment
The environment where lotion application happens is not neutral — it either supports or undermines the session. A well-prepared space reduces total sensory load before the first drop of moisturizer is applied. Spend 5 minutes setting up, and the session will be easier for everyone.
Temperature
Warm room — cold environments increase skin sensitivity and tighten the defensive response
Lighting
Soft, warm lighting — avoid harsh overhead fluorescents that add to sensory load
Noise
Minimize background noise — reduce total sensory load before you begin touch
Surface
Towel laid down where child will sit/stand — catches product, prevents slipping, soft underfoot
Materials Ready
Selected moisturizer, towel for patting, timer (optional), mirror (if self-applying) — all visible before you begin
Parent Position
Beside child (not looming over). At eye level. Hands visible at all times. No surprise approach.
Comfort Items
Favorite stuffed animal or fidget nearby for post-application comfort and transition
Material Placement: Products within child's sight — no surprise introduction. Let child see and touch the closed container first if needed. · Research: PMC10955541 — Structured environment in 1:1 sessions was most effective | Ayres' Sensory Integration Theory: Environmental setup as core principle

Readiness Check
Is Your Child Ready? The 60-Second Pre-Session Check
The best session is one that starts right. This 60-second readiness assessment takes less time than a failed application attempt — and prevents the kind of traumatic experience that makes the next session harder. Check all seven indicators before you begin.
✅ Child is fed — not hungry
✅ Child is rested — not overtired
✅ Child is in a regulated state — no meltdown in the past 30 minutes
✅ Child is not ill
✅ Skin is clean and dry — post-bath is optimal
✅ Selected moisturizer is at room temperature or warmed
✅Environment is set per Card 12 (Space Setup)
All ✅ — GO
Proceed to Step 1: The Invitation
1–2 Concerns — MODIFY
Use simplified version: single body area only, preferred product, shortest duration
3+ Concerns — POSTPONE
Try again tomorrow. Use bath oil tonight as alternative moisturizing method.
Step 1 of 6
Step 1: The Invitation — 30–60 Seconds
How you begin the session sets the emotional tone for everything that follows. A calm, matter-of-fact invitation — not apologetic, not demanding — communicates to the child that this is a normal, manageable routine. You are in charge of your own nervous system first.
"It's time for skin care. Your skin needs some help today. Let's use [name of product]. You're in charge — you can choose where we start."
Body Language Guidance
- Calm, matter-of-fact tone — not apologetic, not demanding
- Show the product before opening — no surprises
- Let child touch or hold the container if they want
- Wait for acceptance cue before proceeding
Read the Cues
Acceptance: Looks at product, touches container, nods, moves closer, extends arm, says "okay"
Resistance: Turns away, stiffens, covers body, says "no," begins to cry
If Resistance: Do NOT proceed. Say: "That's okay. Would you like to try the bar instead? Or should we do hands first?" Offer format choice or body part choice. Never proceed without a consent cue. · Research: ABA Pairing Procedures | OT "Just-Right Challenge" principle

Step 2 of 6
Step 2: The Engagement — 1–3 Minutes
Material introduction is not one-size-fits-all — each format has its own introduction protocol that previews the sensory experience before it touches the child's body. The preview eliminates the element of surprise, which is a major amplifier of defensive response. Follow the protocol for your chosen format.
Solid Lotion Bar
Let child hold the bar. Let them rub it on the back of their own hand first. Say: "See? It's dry. It melts when it touches warm skin. You try."
Spray Moisturizer
Spray once into the air first — child sees the mist, hears the sound. Then spray on your own arm to demonstrate. Say: "Quick mist — no rubbing needed. Watch."
Pure Oil
Drop oil onto your palm and show child. Let them feel a drop on their fingertip first. Say: "This isn't lotion — it feels different. No sticky coating."
Bath Oil
Already in bathwater — no separate introduction needed. Child is already being moisturized as they bathe. No script required.
Warming Technique
Show child you're warming the lotion between your palms. Let them feel your warm hands before lotion contacts skin. Say: "I'm making it warm first — no cold surprise."
Reinforce engagement: "You're checking it out — that's exactly right." · Research: PMC11506176 — Structured material introduction | ABA reinforcement scheduling

Step 3 of 6
Step 3: The Therapeutic Action — 3–5 Minutes
This is the core of the session. Five specific techniques make application significantly more tolerable for tactile-defensive children. Each one has a neurological rationale — this is not intuitive, which is why so many parents unknowingly do the opposite of what helps.
Start with Most-Tolerated Area
Usually shins or upper arms. Never start with face, hands, or feet — these are the most sensitive areas.
Use FIRM Pressure
Not light, ticklish touch. Firm pressure is LESS aversive to tactile-defensive children. This is counterintuitive but neurologically critical.
Work in One Direction
Downward strokes only — not back-and-forth rubbing. Predictable, consistent movement reduces startle response.
Apply Thin Layers
Less residue = less sensory load. Thin layers absorb faster. More is not better.
Support Self-Application
If child self-applies, supervise without touching. Verbal guidance only: "You're doing the arm — great. Now try the other arm."
✅ Ideal
Child calm, tolerating or participating, minimal fussing
⚠️ Acceptable
Child whimpering but staying still, tolerating with verbal support, asking "how much longer?"
🛑 Stop
Child pulling away, crying escalating, trying to wipe product off aggressively → Move to Cool-Down
Common Errors to Avoid:❌ Light, tentative touch (MORE aversive) ❌ Cold product from bottle ❌ Thick layers "for better moisturizing" ❌ Restraining child during application

Step 4 of 6
Step 4: Repeat & Vary — Expanding Body Area Coverage
After the first body area is covered successfully, the goal is to expand coverage — gradually, at the child's pace. For severe tactile defensiveness, this may mean only 1–2 areas initially. That is correct. Expand over days and weeks, not in a single session. Partial progress is real progress.
1
Face, Hands, Feet
Most sensitive — introduce last, after other areas are well-established
2
Inner Arms, Stomach
Moderately sensitive — introduce after shins, upper arms, and back
3
Thighs, Shoulders
Moderate tolerance — typically manageable in first 2 weeks
4
Upper Arms, Back
Usually well-tolerated early — good second or third area
5
Shins, Lower Legs
Typically most tolerated — start here in first sessions
Give the child choice: "Arms or legs next?" Count together: "Five strokes on this arm, then done with this arm." Use a mirror so child can watch and feel more in control. Honor satiation signals — increasing restlessness, verbal "all done," pulling away after cooperation.
"3 good, calm body areas > 8 forced, distressed body areas."

Step 5 of 6
Step 5: Reinforce & Celebrate — Within 3 Seconds
Reinforcement is most effective when delivered within 3 seconds of the cooperative behavior. Waiting longer breaks the neurological link between the action and the reward. Celebrate the attempt, not just the completion — every moment of tolerance is progress worth acknowledging.
"Your skin is going to feel so much better. You helped it!"
"You did your skin care — that was brave."
"Look — no more dry spots on that arm. YOU did that."
Verbal Praise
Specific, not generic. Name what they did: "You kept your arm still for five whole strokes."
Activity Choice
"Skin care done! Would you like [preferred activity]?" Transition immediately to something enjoyable.
Visual Progress
Sticker on body map showing areas covered. Token economy token if in use. Visual progress is powerfully motivating.

Step 6 of 6
Step 6: The Cool-Down — Closing the Session Well
How a session ends determines how the next session begins. A deliberate, calm cool-down protocol signals to the child's nervous system that the sensory challenge is over — and that safety follows. Never leave the child dysregulated at session close.
Signal ending: "All done with skin care! Great job." — clear, definitive close
Offer clean towel — child may pat (not wipe) any residue. Pat only, never rub.
Wait for absorption — 2–3 minutes before dressing if using lotion
Transition immediately to a preferred, calming activity — maintain the positive association
Material put-away: child helps close containers and put away supplies — builds ownership and routine
If Child Is Distressed at Session End: Provide deep pressure (firm hug, wrap in blanket). Offer preferred sensory input: fidget, heavy blanket, snack. DO NOT apply more product — the session is over. Note distress level in your data tracker. · Research: NCAEP Evidence-Based Practices Report (2020) — Visual supports and transition strategies
Data Capture
Capture the Data: Right Now — Within 60 Seconds
Data captured immediately after a session is data that drives progress. Within 60 seconds of session end — before you do anything else — record these four fields. Over weeks, this data reveals patterns that no amount of memory can replicate, and it gives your therapist the information they need to refine your approach.
1
Product Used Today
Name and format of the moisturizer used (e.g., "solid lotion bar — DIY shea butter")
2
Body Areas Covered
List all areas where product was applied successfully (e.g., "left shin, right shin, upper arms")
3
Tolerance Rating (1–5)
1=Refused/meltdown · 2=High distress, minimal application · 3=Moderate distress, partial coverage · 4=Mild discomfort, full coverage · 5=Calm/independent
4
Notes (Optional)
Any observations — what worked, what triggered distress, child's verbal feedback, anything unusual
"Data captured now is data that drives progress."
📊 Product tracking identifies which formats work · 📊 Body area mapping builds your tolerance hierarchy · 📊 Ratings show longitudinal progress over weeks · 🔗 GPT-OS® in-app tracker: pinnacleblooms.org

What If It Didn't Work? Troubleshooting Guide
Not every session goes as planned. When something doesn't work, the answer is almost never "try harder" — it is "try differently." Every problem below has a specific, actionable solution.
Child refused ALL formats today
→ Try bath oil approach — add oil to bathwater. Moisturizing happens without any separate "lotion event." No direct application needed.
Child tolerated format but cried throughout
→ Reduce scope to single body area only. Add longer deep pressure prep. Reassess format: try spray (fastest, least touch).
Child wiped product off immediately
→ Use fast-absorbing formula that "disappears" within 30 seconds. Or use bath oil — nothing to wipe off.
Product caused skin irritation
→ Stop immediately. This may be contact sensitivity, not tactile defensiveness. Patch test a different product. Consult pediatric dermatologist.
Fine in practice but resists real routine
→ Generalization issue. Use identical product, same time, same script, same space every day. Predictability reduces anticipatory anxiety.
Dermatologist needs full body coverage but only 1 area is tolerated
→ Communicate with dermatologist: "We can reliably cover arms and legs. Working on expanding. Can we use bath oil for remaining areas?" Advocate for your child's sensory needs while meeting medical requirements.
Didn't find your solution? Ask GPT-OS® at pinnacleblooms.org or book a teleconsultation: 📞9100 181 181
Adapt to Your Child: The Personalization Matrix
No two tactile-defensive children have identical trigger profiles. Once you've identified your child's primary trigger, this matrix tells you exactly which materials and modifications to prioritize — and which to avoid.
Primary Trigger: TEXTURE
Wet/creamy feeling on skin · Priority: Solid lotion bars, spray moisturizer · Avoid: Thick creams, ointments, petroleum jelly
Primary Trigger: TEMPERATURE
Cold shock from product · Priority: Warming technique (15–20 sec between palms) · Store products in warm area, not cold bathroom
Primary Trigger: SMELL
Fragrance overwhelm · Priority: Fragrance-free formulas, pure unscented oils · Check label: "fragrance-free" NOT "unscented"
Primary Trigger: TOUCH BY OTHERS
Loss of control, unpredictability · Priority: Self-application tools, spray (no rubbing), bath oils (zero direct application)
Primary Trigger: RESIDUE
Greasy/sticky aftermath · Priority: Fast-absorbing formulas, gel-based moisturizers, spray · Allow 3–5 minutes absorption before dressing
❄️ Winter Adaptation
Richer products needed. Increase frequency. Skin loses moisture faster in cold air. Layer oil under lotion for extra protection.
☀️ Summer Adaptation
Lighter products may suffice. Coordinate with sunscreen needs (A-019). Spray formats are especially useful in heat.

Progress Arc
Week 1–2
Week 1–2: What to Expect — The Testing Phase
The first two weeks are a discovery phase — for you as much as for your child. You are learning which formats, which body areas, and which conditions yield the most tolerance. Inconsistency is expected and normal during this phase. Your job is to observe, record, and stay patient.
Testing phase: child may accept one format and reject others — this variability is data, not failure
Inconsistency expected: tolerance may vary day to day depending on regulation state, illness, and stress
Body area acceptance limited: 1–2 areas is a successful Week 1 outcome
Anticipatory anxiety may increase initially — child now knows what's coming. This is normal and temporary.
Target by Week 2
✅ Identified at least ONE tolerated format · ✅ Established consistent time/place for routine · ✅ Capturing daily data · ✅ Deep pressure prep integrated if helpful
Parent Milestone
"You're learning your child's specific trigger profile." This knowledge is irreplaceable — no therapist can discover it without your daily observations.
Progress Arc
Week 3–4
Week 3–4: Consolidation — Patterns Are Emerging
By weeks 3 and 4, the routine is becoming routine. The child's nervous system has encountered the stimulus enough times to begin reducing the threat response. Anticipatory anxiety — the dread before lotion time — often begins to decrease noticeably during this window.
Less Anticipatory Anxiety
Child shows less distress before the routine begins. Doesn't run when they see the product. May approach more neutrally.
Tolerance Duration Increasing
From 2 minutes to 5 minutes. From 2 body areas to 4. The neurological habituation is measurable in your data.
Preference Emerging
Child may begin requesting a specific product: "I want the bar, not the spray." This is a major milestone — expressing preference rather than blanket refusal.
Skin Condition Improving
Consistent moisturizing is delivering dermatological benefit. Dryness reducing. Eczema flares decreasing. The medical goal is being met.
"You may notice you're more confident too — the routine is becoming routine."
Research: Neuroplasticity: Synaptic strengthening through repeated structured input | PMC10955541

Progress Arc
Week 5–8
Week 5–8: Mastery — You're Almost There
Weeks 5–8 are when the transformation becomes undeniable. The routine that once required careful planning and bracing for a battle has become simply: skin care time. Mastery isn't about perfect — it's about consistent, low-distress coverage that protects your child's skin without trauma.
Mastery Criteria
✅ Preferred format tolerated with minimal or no distress · ✅ Full body coverage in single session · ✅ Self-application on at least some areas · ✅ Routine completed in under 10 minutes with cooperation · ✅ Skin health significantly improved
Generalization Indicators
✅ Tolerates unfamiliar brand (not just the one tested) · ✅ Accepts moisturizer in different settings (travel, grandparent's house) · ✅ Tolerance extends to similar topicals (sunscreen, bug spray)
Maintenance Check: Does the routine persist without extensive sensory prep? If yes — mastery achieved. You can begin gradually reducing deep pressure prep duration and testing new product varieties.
Research: PMC10955541 | BACB mastery criteria standards

Celebrate This Win 🎉
"You did this. Your child's skin is healthy because you didn't give up."
Remember Card 1? The parent holding the lotion, the child screaming, the impossible choice between skin health and sensory safety? Look where you are now. You didn't force your child through a traumatic routine — you found the format that works for their specific neurology, and you built a daily practice that protects their skin without distress.
You Identified Triggers
You now understand your child's specific sensory trigger profile — knowledge no off-the-shelf resource could give you.
You Found What Works
You found the format that works for YOUR child — not the "right" product, but the right product for your family.
You Built a Routine
A daily routine that protects their skin without traumatizing them — that's not a small thing. That's life-changing.
📸Journal Prompt: Document this milestone. Take a photo of your child's healthy, moisturized skin. Save it for the hard days.
The Progression Pathway: Where You Are & Where You're Going
This technique — A-020: Lotion Avoidance — sits within a connected network of techniques. Understanding where you are in the progression helps you plan the most effective next steps for your child's sensory development.
Prerequisites (What Came Before)
A-001: Touch Sensitivity Foundations · A-019: Sunscreen Application
⭐ CURRENT: A-020
Lotion/Moisturizer Resistance — YOU ARE HERE
Next-Level Options
A-021: Bath Time Meltdowns · A-024: Medicine Topical Application · A-019: Sunscreen · A-023: Bug Spray
If Tolerance Is Strong → Advance
A-021: Bath Time Meltdowns (complex personal care) · A-024: Hates Having Medicine Applied (medical topicals)
If Tolerance Is Specific → Expand Laterally
A-019: Sunscreen Application (similar format, outdoor) · A-023: Bug Spray Resistance (spray format, outdoor)
If technique was challenging → Strengthen foundations with A-001: Touch Sensitivity (broader tactile desensitization) and A-015: Face Washing Resistance. · Long-Term Goal: Independent self-care in daily hygiene routines → Daily Living & Independence Index
Related Techniques in the Sensory Domain
The materials and skills you've developed in A-020 transfer directly to several related techniques. You've already done more preparation than you realize — here's what you're ready for next.
Technique | Name | Level | Material Overlap | |
A-018 | Haircut Refusal | Core | Some overlap | |
A-019 | Sunscreen Application | Core | High overlap ● | |
A-020 | Lotion Avoidance — CURRENT | Core | ● Your technique | |
A-021 | Bath Time Meltdowns | Core | Moderate overlap | |
A-022 | Hates Hair Brushing | Intro | Different materials | |
A-023 | Bug Spray Resistance | Core | High overlap ● (spray) |
"You already own materials for A-019 and A-023." Your spray moisturizer, fragrance-free products, and deep pressure techniques transfer directly. · 🔗 Browse full Sensory Domain techniques → techniques.pinnacleblooms.org/sensory
Domain A: Sensory
Primary domain — this technique lives here, under Tactile Processing sub-domain
Domain I: Self-Care
Secondary impact — every successful moisturizing session builds ADL independence
Domain H: Emotional
Tertiary impact — reduced daily battle improves overall emotional regulation
Families Who've Been Here
These illustrative case summaries — representative of outcomes across the Pinnacle Blooms Network — show what becomes possible when format is matched to the child's neurological profile. Note: Illustrative cases; outcomes vary by child profile.
Family Story #1 — The Solid Lotion Bar Discovery
"Every bath ended in a 20-minute meltdown. His skin was cracking, bleeding at the knuckles. The dermatologist said 'moisturize twice daily' — she didn't understand what that cost us emotionally."
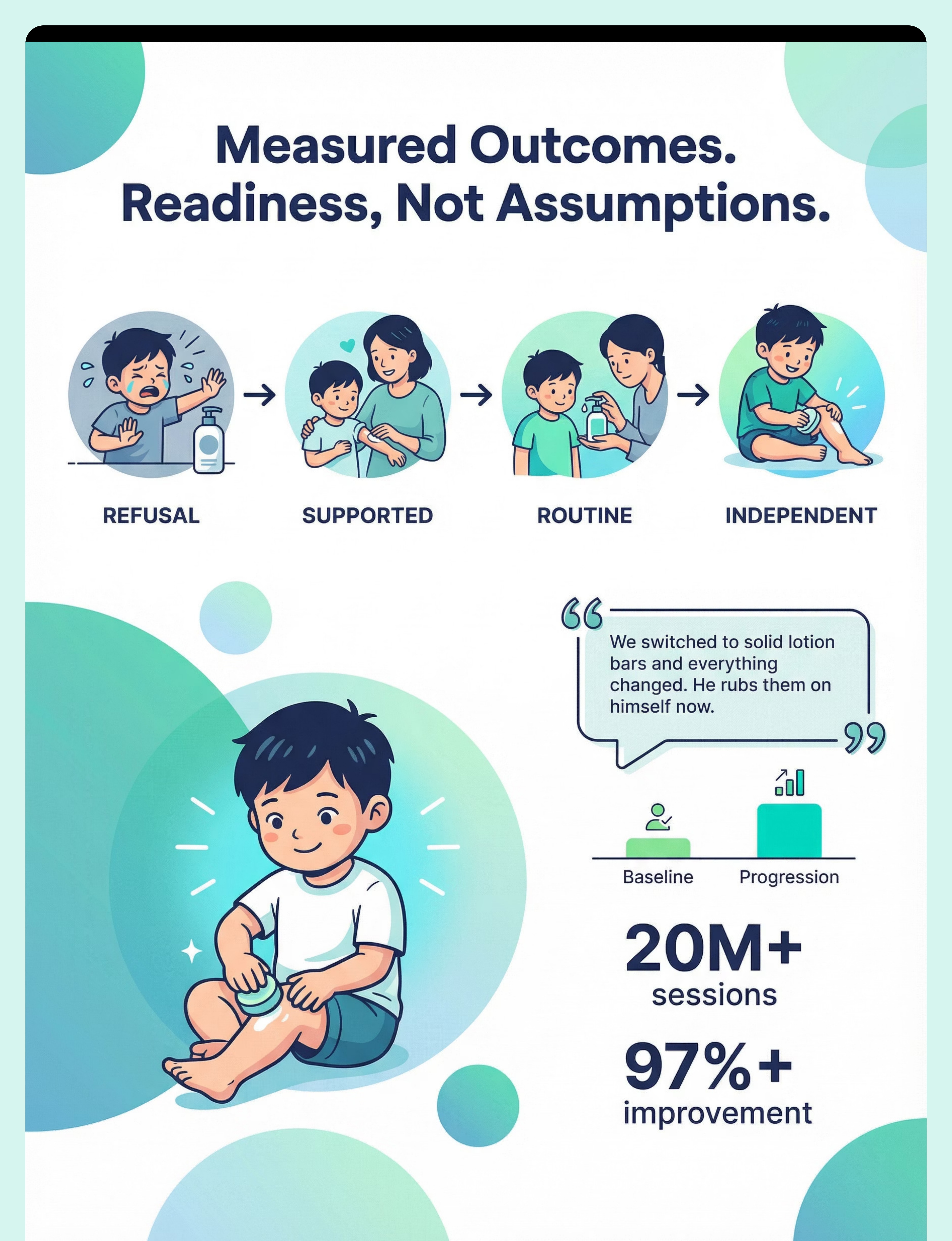
→ After (Week 3): "We switched to solid lotion bars and everything changed. He rubs them on himself now — every night after bath. His eczema is finally under control." Timeline: Complete refusal → self-application in 3 weeks.
Family Story #2 — The Bath Oil Breakthrough
"We tried every lotion, cream, and ointment. She rejected them all. Her legs looked like sandpaper."
→ After (Week 2): "Bath oil. That was the answer. We add it to her bathwater and there's no separate 'lotion time.' She doesn't even know she's being moisturized." Timeline: Total rejection → seamless routine in 2 weeks.
"Lotion avoidance is one of the most solvable personal care challenges we see. The key is format — not persistence. When we match the moisturizing format to the child's tactile profile, resistance often disappears within days." — Pinnacle Blooms OT Consortium
Preview of 9 materials that help when child avoids lotion Therapy Material
Below is a visual preview of 9 materials that help when child avoids lotion therapy material. The pages shown help educators, therapists, and caregivers understand the structure and content of the resource before use. Materials should be used under appropriate professional guidance.












Link copied!