
Pinnacle Blooms Network® | Sensory Solutions Series — Episode 21
9 Materials That Help When Your Child Avoids Hugs
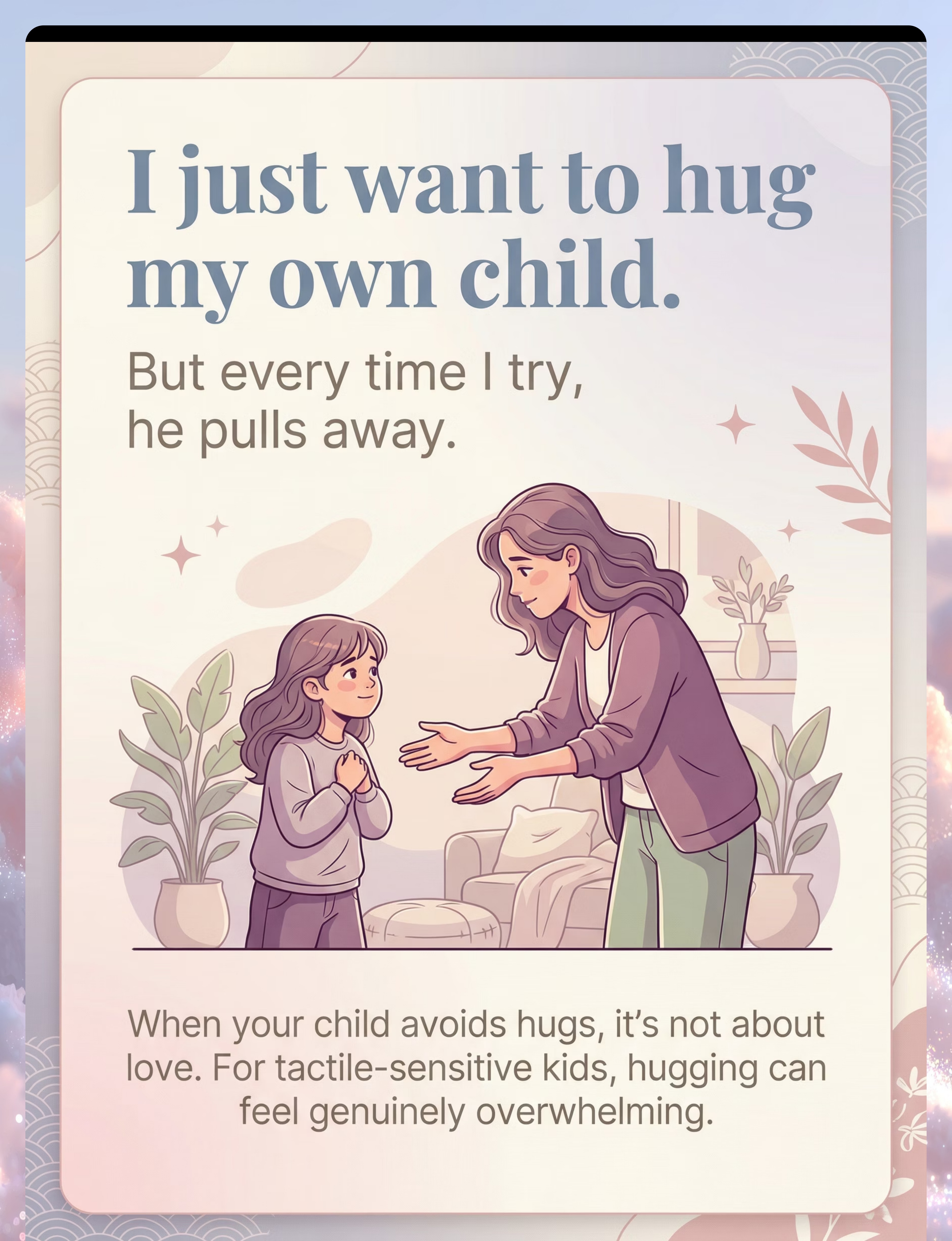
"I just want to hug my own child. But every time I try, he pulls away or goes stiff. His grandmother thinks he doesn't love us. But I see how he looks at me — he does love me. He just can't handle being held."
When your child loves you deeply — but can't tolerate your touch.
You are not failing. Your child's nervous system is speaking. And there is a proven path forward. WHO Nurturing Care Framework (2018) confirms that early identification and parental awareness directly impact outcomes.

You Are Not Alone
The Numbers Behind Hug Avoidance
Millions of families worldwide are navigating this exact challenge — a child who loves deeply but cannot tolerate the physical sensation of being hugged. The science is clear: this is a neurological difference, not a behavioral choice, and not a reflection of how much your child loves you.
80%
Sensory Difficulties
Of children diagnosed with autism display sensory processing difficulties, including tactile over-responsivity (PRISMA Systematic Review, 2024 — PMC11506176)
1 in 6
Children Affected
Children globally are affected by sensory processing challenges that impact physical affection and social connection (WHO/UNICEF developmental monitoring data)
24
Studies Confirm It
Meta-analysis across 24 studies confirms sensory integration therapy effectively promotes social skills, adaptive behavior, and sensory processing (World J Clin Cases, 2024 — PMC10955541)
Your child is not broken. Their brain simply processes touch differently — and science has mapped exactly how to bridge this gap. You are among millions of families navigating this, and a proven intervention path exists for you.
What's Happening in Your Child's Brain
Understanding the neuroscience — in plain English — is the first step toward compassion and effective action.
The Neuroscience
Your child's somatosensory cortex — the brain region that processes touch — over-amplifies the sensory signals from physical contact. When you hug your child, their brain receives the tactile input at dramatically amplified intensity.
What feels like a warm embrace to you may register as overwhelming compression, unpredictable pressure, and alarming heat to your child's nervous system. The light touch of your arms, the heat of your body, the compression of their chest, the restriction of their movement — each element triggers defensive neural responses.
Reference: Frontiers in Integrative Neuroscience (2020) — DOI: 10.3389/fnint.2020.556660
What This Means for Your Family
This is a wiring difference, NOT a behavior choice. Your child's emotional attachment system — love, bonding, connection — works perfectly. Their sensory processing system simply over-amplifies tactile input. These are independent neurological systems.
Your child can love you with their whole heart while their nervous system rejects the physical sensation of your hug. The love is real. The sensory barrier is real. Both exist simultaneously — and both deserve to be honored.
The goal of this intervention is not to eliminate your child's sensory differences, but to build new pathways for connection that their nervous system can actually receive and enjoy.

Where This Sits in Development
Age Band: 2–12 years | Domain: Sensory Processing → Tactile Over-Responsivity → Social-Emotional Connection | Domain Code: SEN-TAC-SOC
0–12 Months
Touch tolerance patterns begin to emerge. Some infants show early signs of tactile sensitivity — resisting being held or soothed through touch.
12–24 Months
Affectionate touch avoidance becomes observable. Child may resist cuddling, holding, and being carried. Caregivers begin to notice something is different.
2–5 Years ★ Primary Window
Hug avoidance becomes pronounced. Family notices. Grandparents question. Social situations create pressure. This is where intervention has maximum impact.
5–8 Years
Social expectations increase (peer hugging, teacher greetings). Without intervention, compensatory behaviors develop and avoidance becomes entrenched.
8–12 Years
Self-awareness emerges. Child may feel different, ashamed, or confused about their own touch responses. Early intervention prevents this.
Comorbidity Awareness: Tactile over-responsivity affecting affection frequently co-occurs with auditory and visual sensory differences, anxiety, clothing texture sensitivity, food texture sensitivity, and challenges with personal care routines such as hair washing and nail cutting. References: PMC9978394 | WHO/UNICEF CCD Package (2023)
The Evidence Behind This Technique
This intervention is not guesswork. Every recommendation on this page is grounded in peer-reviewed research, systematic reviews, and randomized controlled trials.
PRISMA Systematic Review (2024)
16 articles from 2013–2023 confirm sensory integration intervention meets criteria for evidence-based practice for children with ASD. Level I Evidence. → PMC11506176
Meta-Analysis (World J Clin Cases, 2024)
Across 24 studies, sensory integration therapy effectively promoted social skills, adaptive behavior, sensory processing, and motor skills. Level I Evidence. → PMC10955541
Indian RCT (Padmanabha et al., 2019)
Home-based sensory interventions demonstrated significant outcomes in Indian pediatric population. Level II Evidence. → DOI: 10.1007/s12098-018-2747-4
WHO Nurturing Care Framework
Neurological basis for sensory-based interventions established across 54 low- and middle-income countries. SPD Foundation and AOTA Clinical Practice Guidelines aligned. → nurturing-care.org | aota.org
Clinically validated. Home-applicable. Parent-proven. Backed by 20M+ exclusive 1:1 sessions at Pinnacle Blooms Network with 97%+ measured improvement.

Technique A-021
The Technique — What It Is
Formal Clinical Name
Tactile Desensitization Through Deep Pressure Alternatives and Affection Ritual Modification
A multi-material, multi-strategy intervention approach that addresses hug avoidance in tactile over-responsive children by providing alternative deep pressure input, modifying the sensory properties of physical affection, creating personalized connection rituals, and systematically building touch tolerance — all executable at home by parents and caregivers.
Parent-Friendly Name
Helping your child accept physical affection through sensory-smart materials and connection rituals.
At a Glance
- Domain: Sensory Processing — Tactile | Social-Emotional
- Age Range: 2–12 years
- Session Duration: 10–20 minutes
- Frequency: Daily, integrated into natural routines
- Setting: Home
- Difficulty: Introductory–Core
- Canon Categories: Weighted/Pressure Materials | Compression Clothing | Tactile Tools | Behavioral Techniques

Who Uses This Technique
This technique crosses therapy boundaries because the brain doesn't organize by therapy type. Sensory processing, behavior, communication, and social connection converge in a single challenge — requiring a single integrated response.

Occupational Therapist (OT)
Primary Lead. Designs the sensory diet, selects deep pressure tools, conducts sensory processing evaluation, and guides the desensitization protocol progression.

BCBA / BCaBA
Secondary Lead. Designs alternative affection ritual sequences, implements systematic desensitization using ABA principles, and tracks touch tolerance data.

Speech-Language Pathologist
Supporting Role. Helps the child express comfort/discomfort with touch verbally and supports social communication around physical greetings.

NeuroDevelopmental Pediatrician
Supporting Role. Evaluates differential diagnoses, monitors neurological progression, and provides medical oversight for complex cases.
Reference: Adapted UNICEF/WHO Nurturing Care Framework for SLPs (2022) — DOI: 10.1080/17549507.2022.2141327

DIY & Substitute Options
Every material in this protocol has a free or low-cost household substitute. The WHO Nurturing Care Framework emphasizes context-specific, equity-focused interventions — you don't need to buy anything to start. (References: PMC9978394 | WHO NCF Handbook 2022)
Buy This
- Weighted Blanket — Commercially available, precise weight distribution
- Body Sock — Reinforced seams, designed for safety and repeated use
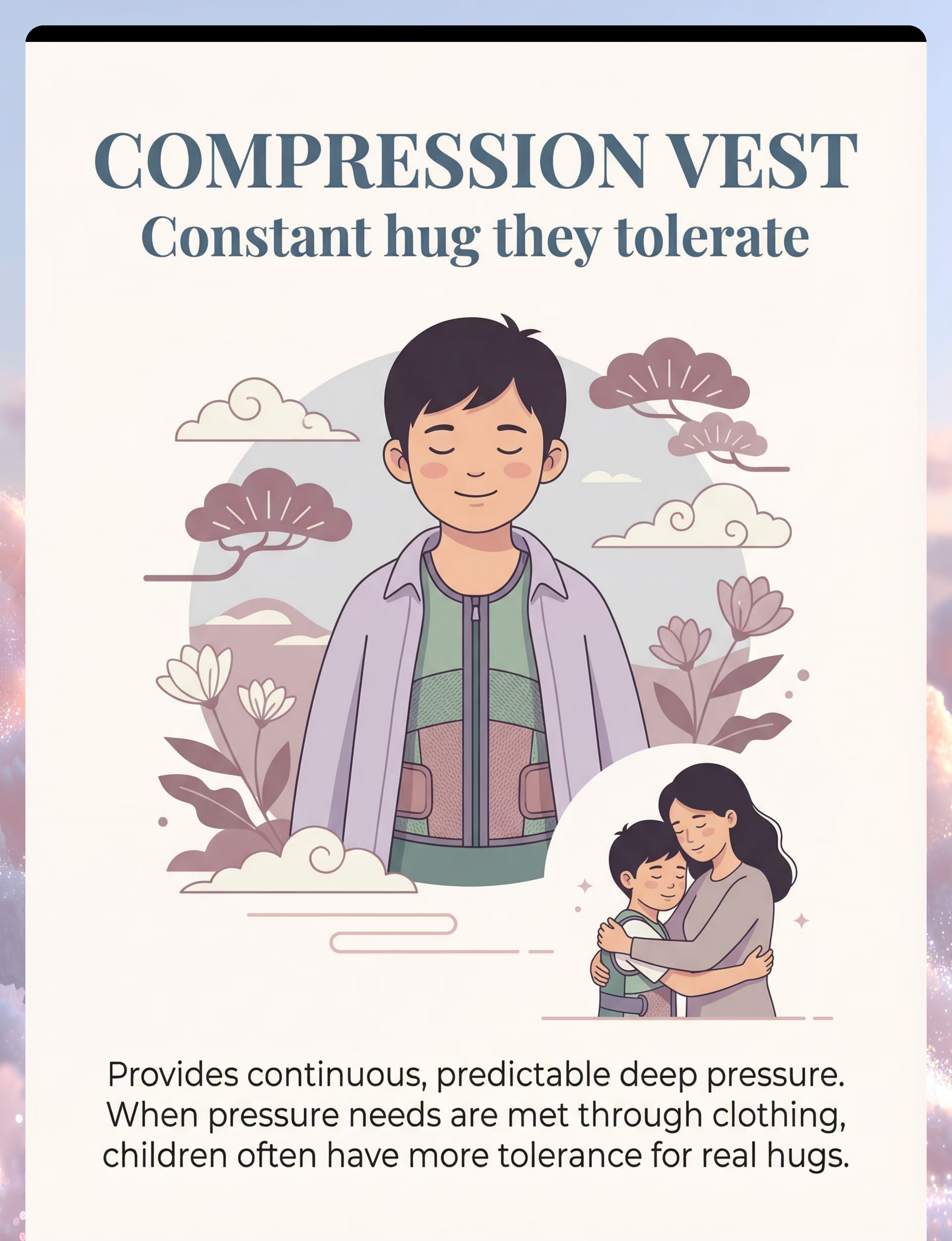
- Compression Vest — Calibrated pressure, breathable materials
- Large Stuffed Animal — Consistent texture, easy to hold
- Massage Tools — Ergonomic grip, varied textures
Make This (Free or Near-Free)
- Weighted Blanket → Pillowcase filled with rice or dried beans, sewn shut. A heavy quilt or multiple layered blankets also works.
- Body Sock → Stretchy Lycra fabric sewn into a pillowcase shape. A large stretchy pillowcase works for smaller children.
- Compression Vest → Tight-fitting athletic wear (compression shirts, rash guards). Slightly snug undershirts layered.
- Stuffed Animal → Large body pillow. Oversized pillowcase stuffed with soft materials and tied closed.
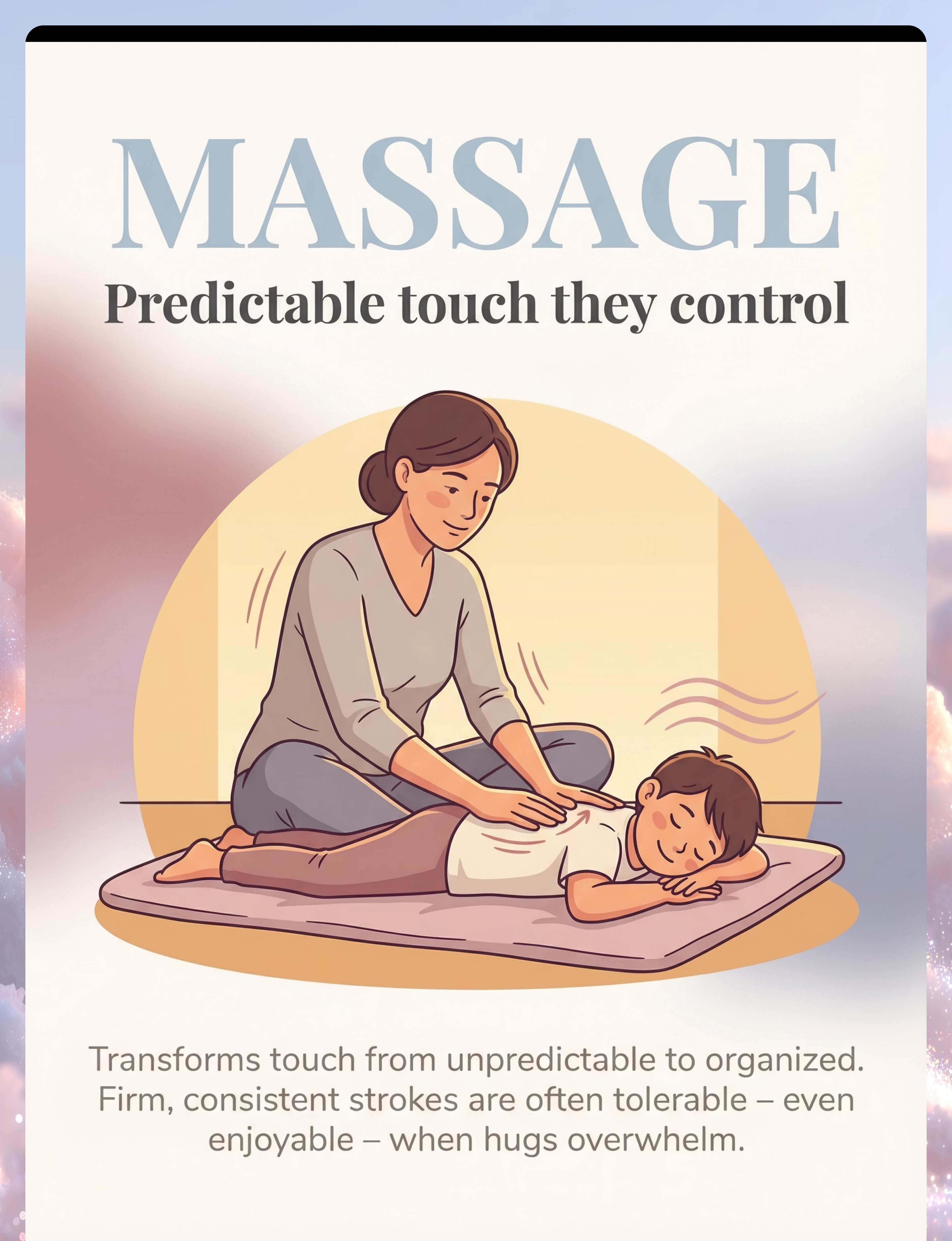
- Massage → Firm, slow hand strokes using cooking oil. Practice on yourself first.
Zero-Cost Version: You can begin this entire intervention TODAY with firm pressure hugs, side-by-side sitting, alternative affection rituals, and gradual desensitization — all free, all proven, all waiting for you right now.

Safety First — Before You Begin
Every effective intervention has clear safety boundaries. Read these carefully before your first session. Your child's safety and emotional security are the non-negotiables of this protocol.
🔴 Red Line — Stop Immediately If:
- Child shows extreme distress beyond typical sensory discomfort (screaming, panic, hyperventilating)
- Any sign of physical pain with touch — could indicate a medical issue
- Touch avoidance is sudden or new onset (not a lifelong pattern) — may indicate trauma. Seek professional evaluation immediately.
- Touch avoidance is specific to certain people but not others — may indicate trauma. Professional evaluation essential.
- Child has open wounds, skin conditions, or recent medication changes
🟡 Caution — Modify If:
- Child is already dysregulated (post-meltdown, overtired, hungry, or ill)
- Environmental stressors are high (loud, crowded, or unfamiliar setting)
- Child is in a transition period (new school, new home, family change)
- Previous session resulted in significant distress
🟢 Proceed When:
- Child is calm, fed, rested, and in a regulated state
- Environment is quiet, familiar, and low-stimulation
- Materials are prepared and within reach
- You have 15–20 uninterrupted minutes
- You feel calm and patient — your regulation matters
Material Safety Reminders: Weighted blanket must be ≤10% of child's body weight. Child must be able to remove it independently. NEVER use with infants. Body sock: always supervise; ensure adequate head opening. Compression vest: 20–30 minute intervals with breaks; watch for redness or marks. CRITICAL: Never force hugs or physical affection. Child's consent is essential at every step.

Set Up Your Space
The environment is not incidental — it is therapeutic. Sensory Integration Theory (Ayres) identifies environmental setup as a core principle of effective intervention. A well-prepared space reduces overwhelm before you even begin. (Reference: PMC10955541)
Physical Setup — Step by Step
- Location: Living room, bedroom, or any comfortable, familiar space your child associates with safety
- Seating: Couch, large beanbag, or floor cushions — choose a surface that allows side-by-side sitting with natural proximity
- Materials Station: Place selected materials within arm's reach but not in the child's direct eyeline (reduces overwhelm)
- Lighting: Warm, dim preferred. Avoid overhead fluorescent lights. A lamp or natural light works best.
- Sound: Quiet environment. Turn off TV. Soft background music acceptable if child enjoys it.
- Temperature: Comfortable — not warm. Heat adds to tactile overwhelm during physical closeness activities.
Remove From Space
- Screens and electronic distractions
- Siblings (unless part of the activity plan)
- Strong scents (perfume, air freshener, cooking smells)
- Visual clutter around the activity area
Parent Positioning
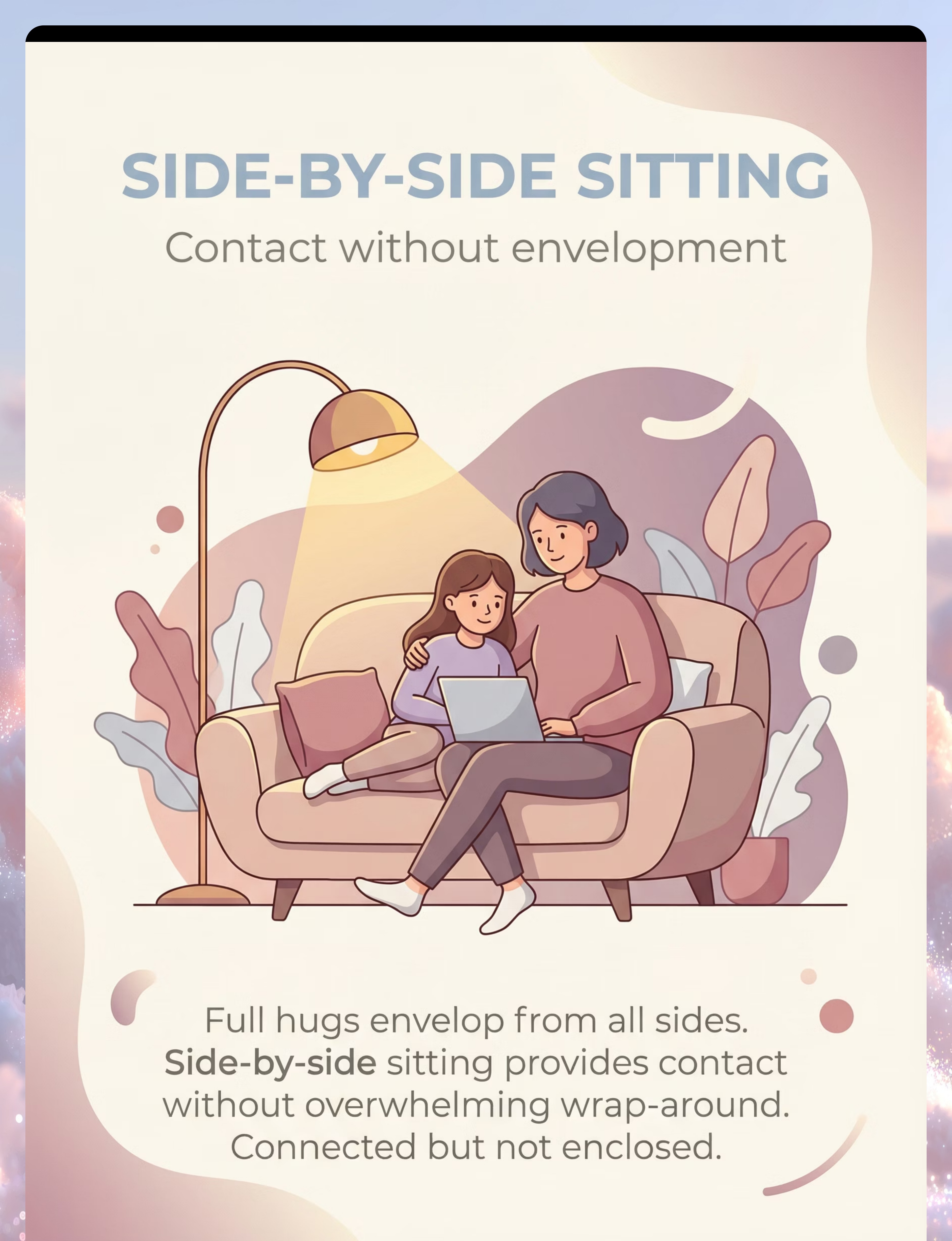
Side-by-side with child — NOT face-to-face. Face-to-face adds facial proximity overwhelm. Side-by-side allows the child to control how much they look at you and reduces the "inescapable" feeling of frontal approaches.

Before You Begin
Is Your Child Ready? — Readiness Check
Sixty seconds of honest assessment before every session saves hours of setback. The best session is one that starts right. A well-timed 5-minute session outperforms a forced 20-minute session every time.
✅ Run the 60-Second Check
Child has eaten within the last 2 hours • Child has slept adequately (not overtired) • No meltdown in the last 30 minutes • Child is not ill or in pain • Child appears calm or neutral • Child is not deeply engaged in a preferred activity • YOU are calm, patient, and emotionally regulated
All Green → GO
Begin the protocol at Step 1. Your child is ready and your window is open. Start gently and follow their lead throughout.
1–2 Amber → MODIFY
Use only the lowest-demand activities: side-by-side sitting, offering a weighted blanket, or a familiar alternative ritual. Skip active desensitization steps today.
Any Red → POSTPONE
Today is a rest day. Offer your child's preferred calming activity. Try again tomorrow. Postponing is not failure — it's data-driven decision-making.

Step 1 of 6
Step 1: The Invitation
Entering your child's space with warmth and zero pressure. Duration: 30–60 seconds. This step is about availability, not demand.
What to Say — Script Options
"Hey [child's name], I'm going to sit on the couch. Want to come sit with me? We can use the cozy blanket."
"Look, I got our special blanket out. Want to come be cozy?"
Body Language
- Sit down first. Don't approach the child.
- Keep your body language open but NOT expectant — no extended arms.
- Smile warmly. Make eye contact if child is comfortable, but don't insist.
Reading Your Child's Response
Acceptance looks like: Moving toward you (even slowly), making eye contact or verbal acknowledgment, sitting on the couch even at the far end, or touching the offered material.
Resistance and how to respond:
- Child ignores: Say once more, then engage yourself with the activity. Let curiosity bring them.
- Child says "no": "That's okay. The blanket will be here if you want it." No pressure.
- Child moves away: Respect it completely. Do the activity yourself. Model enjoyment.
ABA Pairing Procedures: Establishing motivating operations before demand placement. OT "Just-Right Challenge" principle: matching task demand to child's current capacity.

Step 2 of 6
Step 2: The Engagement
Introducing the material — duration 1–3 minutes. Choose ONE material today based on your child's current profile. Consistency and simplicity beat variety at this stage.
1
Tolerates Space, Not Touch
Start with the weighted blanket. Sit together under it. No direct contact required. Shared deep pressure creates proximity without body-to-body contact.
2
Enjoys Enclosed Spaces
Offer the body sock. Play alongside them. Gently press on the sock only if they invite it. The fabric does the therapeutic work.
3
Wears Tight Clothing Comfortably
Try the compression vest under their shirt. Once pressure needs are met through the vest, tolerance for other affection often increases naturally.
4
Hugs Objects, Not People
Introduce the large stuffed animal. Sit together, both hugging your own pillows. Parallel hugging — same activity, individual control.
5
Tolerates Some Touch
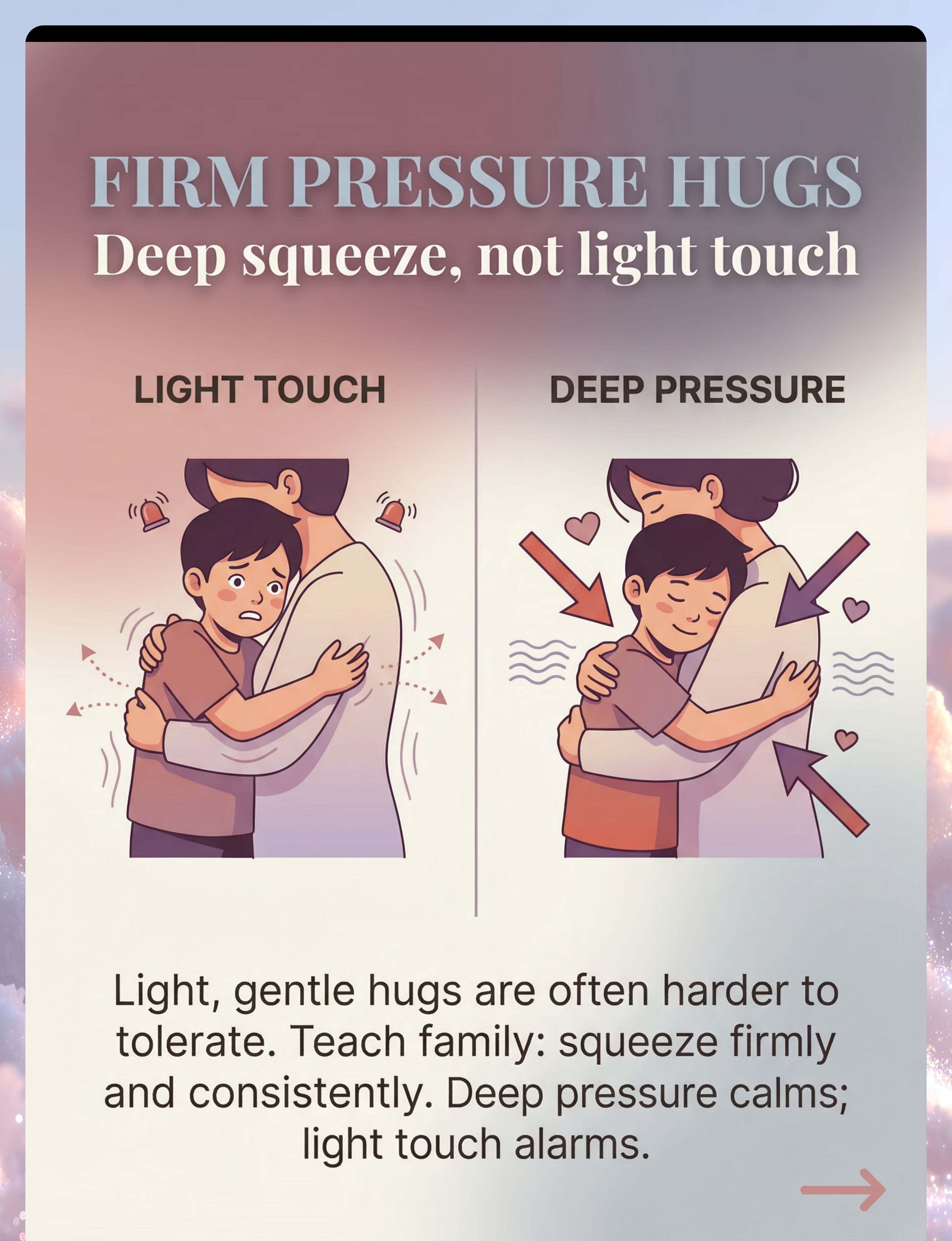
Practice firm pressure hugs. Quick, firm squeeze with immediate release. Deep pressure activates the calming system; light touch activates the alarm system.
"Here's our cozy [blanket/sock/buddy]. I'm going to use mine too. Let's be cozy together."
Reinforcement cue: The moment the child engages with the material or moves closer to you — verbal praise immediately. "I love sitting with you like this." (Reference: PMC11506176)

Step 3 of 6
Step 3: The Therapeutic Action
The Connection Moment — duration 3–5 minutes. This is the heart of the session. While your child is engaged with their chosen material, you create the conditions for connection.
The therapeutic value is in the tolerated contact, however brief. Three seconds of comfortable shoulder-to-shoulder contact is worth more than thirty seconds of endured hugging.
✅ Ideal Response
Child relaxes into proximity, initiates touch, smiles, engages with the ritual. Celebrate it fully.
✅ Acceptable Response
Child tolerates proximity without distress, participates in the ritual even briefly. This IS progress.
⚠️ Concerning Response
Child tenses, pulls away, or shows anxiety. Back up immediately to the previous comfortable level. Never push through distress.
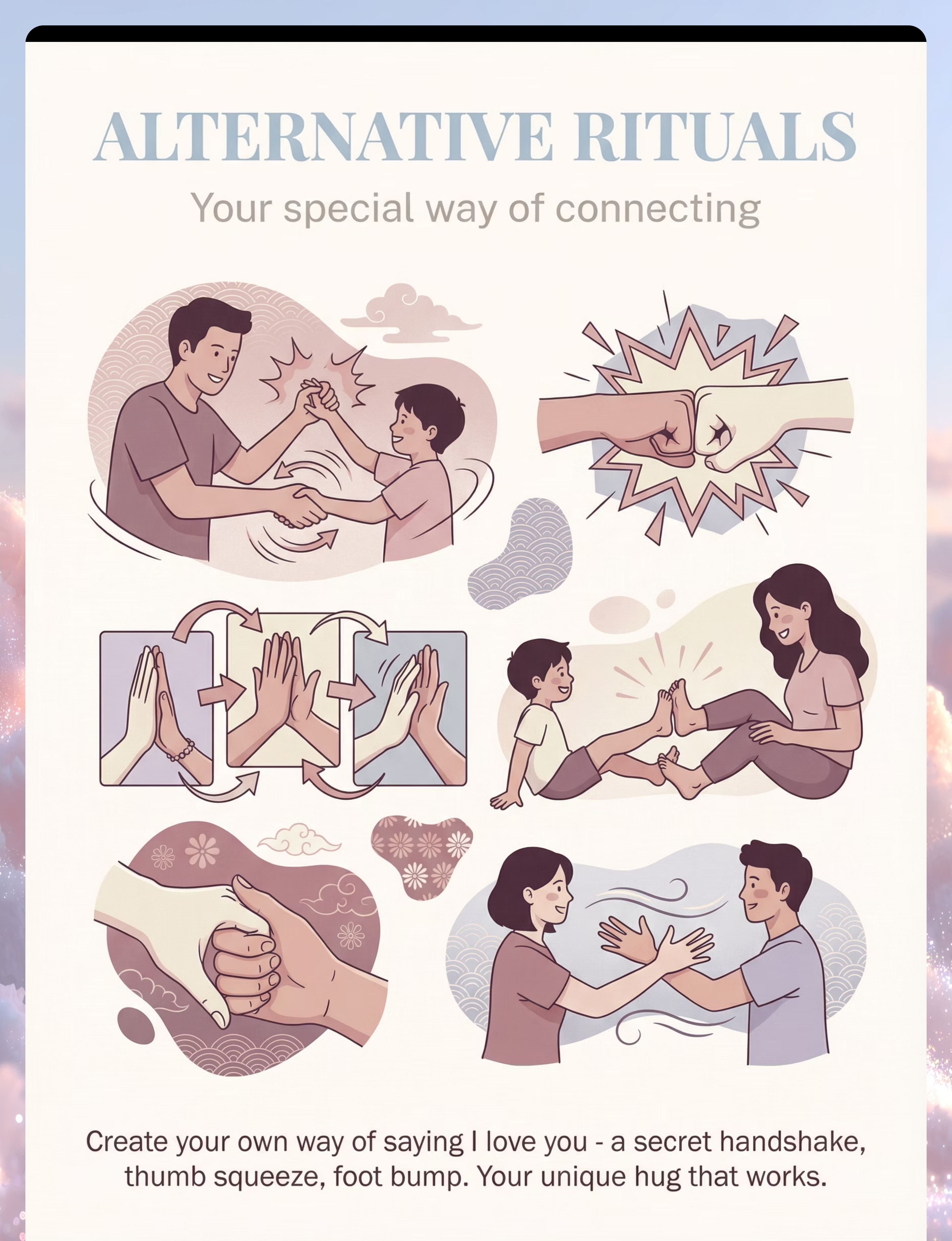
Alternative Affection Ritual Ideas: Special handshake sequence • Fist bump with personalized "explosion" • Three hand squeezes (I — Love — You) • Foot touch side-by-side • High-five sequence you created together. Reference: PMC10955541

Step 4 of 6
Step 4: Repeat and Vary
Duration: 3–5 minutes. Target 2–4 connection attempts per session — offered, never forced. Variety maintains engagement and prevents the activity from feeling clinical or repetitive.
Variation A — Blanket Fort
Build a fort together using the weighted blanket. Proximity happens naturally when you're building and then sitting inside together. Play transforms the therapeutic goal.
Variation B — Massage Trade
"I'll rub your back, then you rub mine." Turn touch into a reciprocal game. The child experiences giving and receiving on equal terms.
Variation C — Stuffed Animal Sandwich
Both of you "hug" the stuffed animal from opposite sides. Your arms are near each other without direct contact — proximity without pressure.
Variation D — Ritual Challenge
Can we do our special handshake faster? Slower? With eyes closed? Adding playful challenge to the affection ritual keeps it fresh and motivating.
3 good connection moments are worth infinitely more than 10 forced ones. Watch for satiation: child looking away, moving away, activity quality decreasing, or body language shifting from relaxed to tense. Follow their lead — always.
Step 5 of 6
Step 5: Reinforce and Celebrate
Reinforcement timing: within 3 seconds of any positive connection behavior. The key principle — celebrate the attempt, not just the success. Every move toward connection deserves recognition.
What to Reinforce — Say This
- Child sat near you → "I love it when we sit together like this."
- Child accepted the blanket → "This cozy blanket time is my favorite."
- Child did the special handshake → "Our handshake is the best one in the whole world."
- Child tolerated brief touch → "Thank you for that hug/high-five. It made my day."
- Child initiated contact → (This is gold.) "That was so nice. I love when you do that."
What NOT to Do
"See? That wasn't so bad!"— Invalidates their real sensory experience
Extend contact beyond what child offered— If they did a 2-second hug, don't grab and hold for 10
Compare to other children— "Your cousin hugs grandma — why can't you?"
Make the celebration bigger than the child is comfortable with— Match their energy level
The goal is for connection to feel safe and predictable — not like a performance evaluation. Keep your celebration warm, genuine, and proportional.

Step 6 of 6
Step 6: The Cool-Down
Duration: 1–2 minutes. A gentle, predictable ending is as therapeutic as the session itself. Transitions that feel abrupt can undo the trust built during the activity — plan the ending before you begin.
Give a Transition Warning
"We're going to finish our cozy time in a minute. One more [handshake/squeeze/moment], then all done." Predictability reduces the anxiety of transitions.
Cool-Down Activity
Continue sitting near each other without active demands. Let the child choose what they want to do next. If using the weighted blanket, let the child decide when to come out.
Material Put-Away Ritual
"Let's put the blanket back on the couch so it's ready for next time." Child participating in put-away gives them closure, control, and a sense of ownership over the activity.
Transition to Next Activity
"What would you like to do now?" Let the child lead the transition. Their choice here signals that the connection time was safe — they're still in control.
If child resists ending: This is a POSITIVE sign — they're enjoying the connection. "I know, this is so nice. We'll do it again tomorrow. I promise." Consistency with the promise is essential.

Capture the Data — Right Now
Capture these three data points within 60 seconds of session end. Sixty seconds of data now saves hours of guessing later. Over 4–8 weeks, these three numbers reveal your child's trajectory with precision no memory can match.
1
Data Point 1 — Closest Contact Achieved
Rate 1–5:
1 = Same room, no approach
2 = Side-by-side sitting (no physical contact)
3 = Shared material with proximity
4 = Brief physical contact (handshake, shoulder touch)
5 = Sustained contact (hug, cuddle, leaning together)
1 = Same room, no approach
2 = Side-by-side sitting (no physical contact)
3 = Shared material with proximity
4 = Brief physical contact (handshake, shoulder touch)
5 = Sustained contact (hug, cuddle, leaning together)
2
Data Point 2 — Child Initiation
Did the child initiate any physical contact today?
Yes / No
If yes, what form did it take? (Note it — initiation is the most powerful data point you can collect.)
Yes / No
If yes, what form did it take? (Note it — initiation is the most powerful data point you can collect.)
3
Data Point 3 — Duration
Seconds of the closest contact achieved today.
Write the three numbers: Contact Level / Initiated? / Seconds
A simple notebook works. GPT-OS® in-app tracker available at pinnacleblooms.org
Write the three numbers: Contact Level / Initiated? / Seconds
A simple notebook works. GPT-OS® in-app tracker available at pinnacleblooms.org
Track using the GPT-OS® In-App Tracker at pinnacleblooms.org, the downloadable PDF tracking sheet, or a simple notebook. The method matters less than the consistency.

What If It Didn't Go as Planned?
Session challenges are not failures — they are data. Every difficult session teaches you something precise about your child's sensory profile and readiness window. Here are the 7 most common challenges and their evidence-based solutions.
Child refused to participate at all
Why: Child wasn't in a regulated state, or the invitation felt like a demand.
Fix: Make NO demands tomorrow. Just use the material yourself nearby. Let curiosity bring them. It may take 3–5 sessions before initial engagement.
Fix: Make NO demands tomorrow. Just use the material yourself nearby. Let curiosity bring them. It may take 3–5 sessions before initial engagement.
Engaged with material but wouldn't come near me
Why: The material is great — you are the unpredictable variable. This is actually progress!
Fix: The material is regulating their sensory system. Proximity to you will follow. Don't rush it.
Fix: The material is regulating their sensory system. Proximity to you will follow. Don't rush it.
Tolerated contact briefly then pushed away
Why: Their nervous system hit its real, physiological limit.
Fix: That brief tolerance IS today's session. Celebrate it. Match that duration tomorrow — don't exceed it until they naturally extend it themselves.
Fix: That brief tolerance IS today's session. Celebrate it. Match that duration tomorrow — don't exceed it until they naturally extend it themselves.
Child became distressed during the session
Why: Went too far, too fast, or child wasn't ready today.
Fix: Back up 2 steps. Return to what was comfortable. Distress creates negative associations with touch — never push through it.
Fix: Back up 2 steps. Return to what was comfortable. Distress creates negative associations with touch — never push through it.
Went well with me, but child still avoids grandparents
Why: Generalization takes time. Each person is a new sensory experience for the child's nervous system.
Fix: Teach grandparents the alternative ritual. Start them at your child's current level, not where you are now.
Fix: Teach grandparents the alternative ritual. Start them at your child's current level, not where you are now.
Light touch (my instinct) makes it worse
Why: Light touch activates the alarm system. Deep pressure activates the calming system.
Fix: Practice firm, consistent pressure. A quick firm squeeze is therapeutically superior to a soft long embrace for this child.
Fix: Practice firm, consistent pressure. A quick firm squeeze is therapeutically superior to a soft long embrace for this child.
Child hugs the dog but not me
Why: Objects are sensorially predictable — consistent temperature, no movement, no social expectations.
Fix: This is NOT rejection. Your job is to gradually become as predictable as the stuffed animal: firm, consistent, brief, expected.
Fix: This is NOT rejection. Your job is to gradually become as predictable as the stuffed animal: firm, consistent, brief, expected.

Adapt and Personalize
No two children are the same. This protocol has three difficulty tiers and age-specific modifications so you can meet your child exactly where they are — on their best days and their hardest ones.
Easier Version
For bad days or initial sessions
• Use only one material
• Stay side-by-side with no contact goal
• Keep session to 5 minutes
• Focus only on the alternative affection ritual
• Accept "same room" as success today
• Use only one material
• Stay side-by-side with no contact goal
• Keep session to 5 minutes
• Focus only on the alternative affection ritual
• Accept "same room" as success today
Standard Version
Core protocol
• 2–3 materials available as options
• Aim for side-by-side contact with shared material
• 10–15 minute session
• Practice 2–3 alternative rituals
• Brief contact attempts if child is willing
• 2–3 materials available as options
• Aim for side-by-side contact with shared material
• 10–15 minute session
• Practice 2–3 alternative rituals
• Brief contact attempts if child is willing
Advanced Version
For breakthrough sessions
• Introduce brief modified hugs with countdown
• Practice with different family members
• Try in different settings
• Increase contact duration gradually (+2–3 seconds per week)
• Work toward child-initiated hugs
• Introduce brief modified hugs with countdown
• Practice with different family members
• Try in different settings
• Increase contact duration gradually (+2–3 seconds per week)
• Work toward child-initiated hugs
For Sensory Seekers
Children who crash into things and seek heavy input often WANT the pressure of hugs but can't process the other elements (heat, unpredictability). Focus on high-pressure activities: tight squeezes with countdown, bear hugs on request, wrestling play. These children may progress faster.
Age Modifications
- Ages 2–4: Play-based approaches. Blanket peek-a-boo. Stuffed animal stories. Parallel play with proximity.
- Ages 5–8: Involve child in creating rituals. Give them ownership. "What should OUR special greeting be?"
- Ages 9–12: Discuss the neuroscience (see Card 3). Let them drive the pace. Help with social strategies for peers.
Progress Arc — Week 1–2
Weeks 1–2: Establishing the Foundation
Managing expectations honestly in the early weeks is as important as executing the technique correctly. Progress at this stage is real but subtle — and it matters enormously.
What Progress Actually Looks Like
• Child accepts the material without resistance
• Child sits on the same surface as you (even at the far end)
• Child participates in alternative affection rituals without reluctance
• Child shows curiosity about new materials (touching the body sock, feeling the vest)
• Child sits on the same surface as you (even at the far end)
• Child participates in alternative affection rituals without reluctance
• Child shows curiosity about new materials (touching the body sock, feeling the vest)
What Is Not Progress Yet
• Child will likely NOT be accepting full hugs yet
• Contact tolerance may fluctuate day to day — this is normal and expected
• Extended family may not see obvious changes
• Some days will feel like backward steps — this is part of the pattern, not a problem
• Contact tolerance may fluctuate day to day — this is normal and expected
• Extended family may not see obvious changes
• Some days will feel like backward steps — this is part of the pattern, not a problem
If your child tolerates being near you with a shared material for 3 seconds longer than last week — that is real, measurable, neurological progress. Measure in seconds, not hugs.
Parent Emotional Preparation: The grief of not being able to hug your child is real and valid. Allow yourself to feel it while also noticing the small connections that ARE happening. Your special handshake IS affection. Your child leaning against the same couch cushion IS closeness.

Progress Arc — Week 3–4
Weeks 3–4: Neural Pathways Forming
By weeks three and four, something remarkable begins to happen: connection starts to feel expected. That expectation — that anticipation — is the sound of new neural pathways forming.
Consolidation Indicators
Child begins to expect the activity — "Are we doing blanket time?" Anticipation signals neural pathway formation. Child moves closer to you voluntarily during shared material time. Alternative affection rituals become smoother, faster, more natural.
Behavioral Changes That Signal Progress
Less pulling away when you sit close • Offering the blanket to you ("Here, you get under too") • Smiling during connection activities • Child initiates the ritual — running up with fist extended for a bump • Reduced stiffness when brief contact occurs
Generalization Seeds — Watch For
Child uses the alternative ritual with someone new (teacher, friend) • Child hugs the stuffed animal in front of family • Child sits closer to siblings during other activities • These spontaneous transfers are the strongest evidence of progress.
When to Increase Difficulty
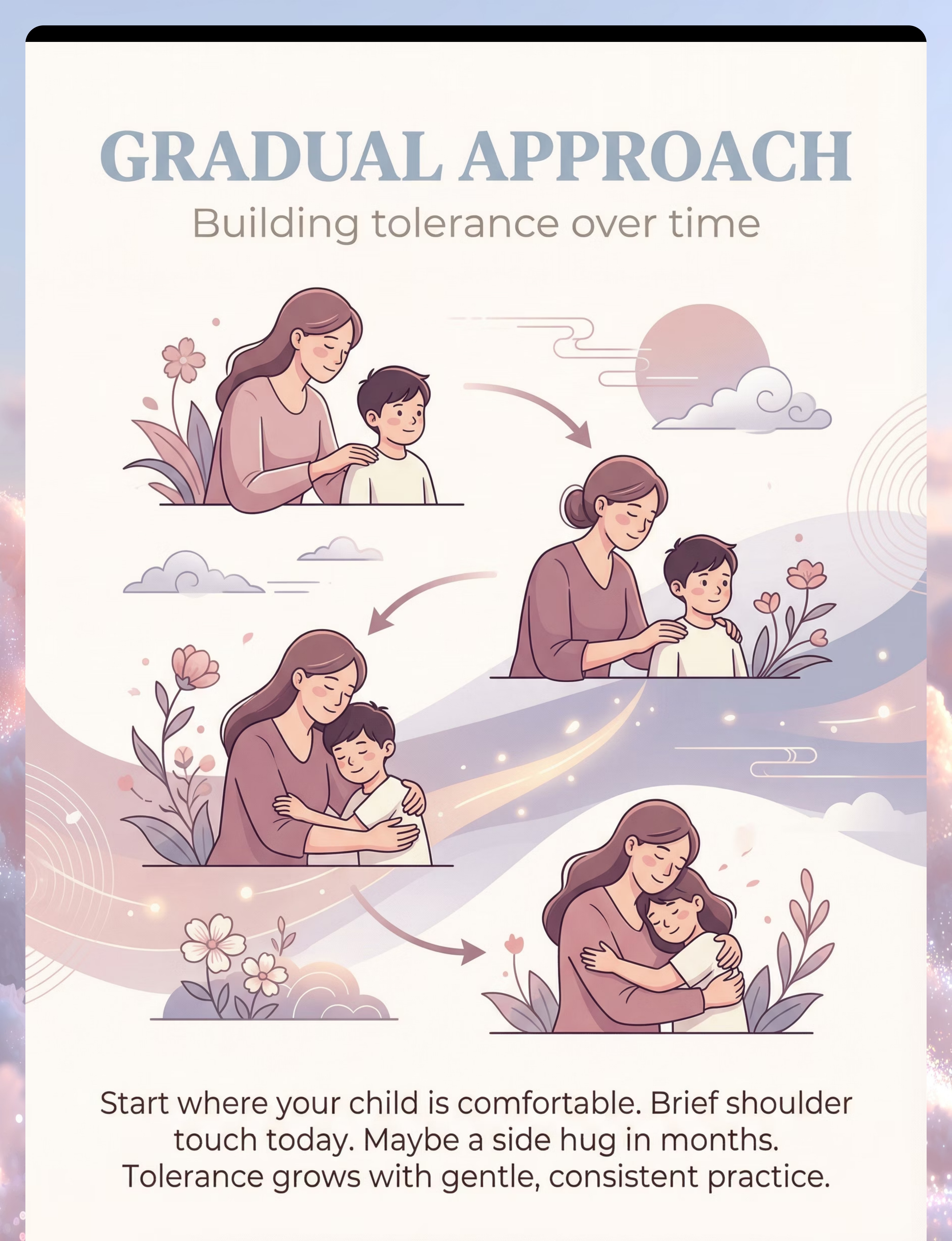
If the child is consistently tolerating the current level for 5+ sessions without distress, try the next step — one element only at a time: slightly more duration OR slightly closer proximity OR a new person. Never all three simultaneously.
Progress Arc — Week 5–8
Weeks 5–8: Connection, Redefined
By weeks five through eight, the goal shifts from building tolerance to consolidating a new, authentic way of connecting. Some children will progress toward modified hugs; others will master rich alternative affection — both represent full success.
Mastery Criteria (Observable and Measurable)
- Child has a reliable alternative affection ritual used with 2+ people
- Child tolerates side-by-side sitting with shoulder or arm contact for 2+ minutes without distress
- Child initiates some form of physical contact at least once per day
- Extended family can use the alternative ritual successfully
- Child shows comfort with brief modified hugs from at least one caregiver
Generalization Indicators
- Affection rituals used across settings (home, grandparents' house, school)
- Child adapts rituals for different people (special handshake with Dad, fist bump with teacher)
- Touch tolerance improving in non-affection contexts too (haircuts, clothing, grooming routines)
Defining Success
Some children will plateau at alternative affection rituals and modified contact — and this IS a successful outcome. The goal is meaningful connection, not a specific physical form of connection. A child with a rich repertoire of alternative affection who connects deeply through their own methods has MASTERED this intervention.

Celebrate This Win
You did this. You arrived at this page worried that your child didn't love you — or that they'd never tolerate being held. You learned the neuroscience. You set up the space. You offered materials with patience. You created rituals that became your family's language of love.
"Your child grew because of your commitment. Your child connects because you learned THEIR way."
What You Achieved
You learned that love and touch tolerance are separate neurological systems. You taught your family alternative ways to show affection. You gave your child the gift of being understood, not forced to conform.
What Your Child Gained
You built neural pathways, one patient session at a time. Your child now has a way to say "I love you" that their body can actually handle. That is not a consolation prize — it is extraordinary.
Your Family Milestone
Take a photo or video of your special affection ritual — your handshake, your fist bump, your blanket time. Save it. This is your family's love language. It's not lesser. It's yours. And it's beautiful.
A special handshake is just as meaningful as a hug. A child who runs to fist bump you when you come home loves you as much as any child who runs to hug. You gave them a way to show it that their body can handle. That is extraordinary parenting.

Red Flags — When to Pause and Seek Help
Trust your instincts — if something feels wrong, pause and ask. These specific warning signs indicate when home-based intervention should be complemented or paused in favor of professional evaluation.
🔴 Pause — Seek Professional Guidance
- Touch avoidance that is new or sudden (not a lifelong pattern) — may indicate trauma or medical issue
- Touch avoidance specific to certain people — professional evaluation essential
- Complete absence of any desire for connection or proximity — developmental evaluation needed
- Regression: touch tolerance that was improving suddenly reverses without clear cause
- Signs of physical pain with any touch — medical evaluation needed
- Extreme anxiety (not sensory discomfort) about touch — may need anxiety-specific intervention
📍 Pinnacle Center Locator
Find your nearest center at pinnacleblooms.org/centers
70+ centers across India operating under GPT-OS® clinical standards.
70+ centers across India operating under GPT-OS® clinical standards.
📞 FREE National Autism Helpline
9100 181 181
Available in 16+ languages. Guidance, center referral, and initial consultation at zero cost.
Available in 16+ languages. Guidance, center referral, and initial consultation at zero cost.
The Progression Pathway
This technique exists within a larger developmental map. Understanding where you are — and where you're headed — gives every session purpose and direction beyond the immediate goal.
← Prerequisite Techniques
- A-001: Touch Sensitivity — General Tactile Defensiveness
- A-020: Lotion/Moisturizer Resistance (related tactile tolerance building)
★ You Are Here
A-021 — Materials That Help When Child Avoids Hugs
→ Next-Level Options
- If deep pressure materials worked well → Deep Pressure Desensitization Protocol
- If alternative rituals worked well → Social Communication — Physical Greeting Strategies
- If co-occurring challenges → A-022 (Noise) or A-025 (Clothing)
- Lateral alternative → Floortime/DIR-based connection strategies
Browse: techniques.pinnacleblooms.org/sensory/tactile
Related Techniques in This Domain
If you purchased a weighted blanket or compression vest for A-021, those same materials are used across multiple related techniques — your investment works harder than you think.
A-001: Touch Sensitivity — General Tactile Defensiveness
Difficulty: Introductory | Materials: Tactile Sensory Kit
techniques.pinnacleblooms.org/sensory/touch-sensitivity-general
techniques.pinnacleblooms.org/sensory/touch-sensitivity-general
A-009: Sand Play Avoidance
Difficulty: Introductory | Materials: Texture Exploration Kit
techniques.pinnacleblooms.org/sensory/sand-play-avoidance
techniques.pinnacleblooms.org/sensory/sand-play-avoidance
A-019: Sunscreen Application Resistance
Difficulty: Core | Materials: Tactile Sensory Kit
techniques.pinnacleblooms.org/sensory/sunscreen-application-resistance
techniques.pinnacleblooms.org/sensory/sunscreen-application-resistance
A-020: Lotion / Moisturizer Resistance
Difficulty: Core | Materials: Tactile Tools
techniques.pinnacleblooms.org/sensory/lotion-moisturizer-resistance
techniques.pinnacleblooms.org/sensory/lotion-moisturizer-resistance
A-022: Overwhelmed by Noise
Difficulty: Introductory | Materials: Noise-Reducing Headphones
techniques.pinnacleblooms.org/sensory/overwhelmed-by-noise
techniques.pinnacleblooms.org/sensory/overwhelmed-by-noise
A-025: Avoids Certain Clothing Textures
Difficulty: Core | Materials: Compression Clothing
techniques.pinnacleblooms.org/sensory/clothing-texture-avoidance
techniques.pinnacleblooms.org/sensory/clothing-texture-avoidance
Your Child's Full Developmental Map
This technique is one focused piece of a larger developmental picture. Your child's journey spans all 12 domains simultaneously — and understanding how they interconnect reveals the full opportunity for growth.
Domain A: Sensory Processing ★ Current Focus
This technique directly addresses tactile over-responsivity — a core sensory processing challenge that ripples through every domain of your child's development.
Connected Domains Impacted
- Domain B: Social-Emotional Development — touch tolerance directly impacts bonding and social connection
- Domain C: Communication — expressing sensory needs, requesting/declining touch
- Domain D: Behavioral Regulation — sensory regulation is the foundation of behavioral regulation
- Domain E: Daily Living Skills — personal care, grooming, and dressing all involve touch
See Your Child's Full Profile
GPT-OS® maps all 12 domains simultaneously and identifies which techniques, across which domains, create maximum developmental momentum for YOUR child specifically.
Request an AbilityScore® assessment to understand your child's complete developmental picture.
📍 pinnacleblooms.org
📞 9100 181 181
📞 9100 181 181

Families Who've Been Here
Progress isn't always a hug. Sometimes it's a fist bump, a three-squeeze hand hold, or a child running across the room toward you with their fist extended. These are real families who found their way. Note: Illustrative cases; outcomes vary by child profile.
1
Family Story 1 — The Fist Bump That Changed Everything
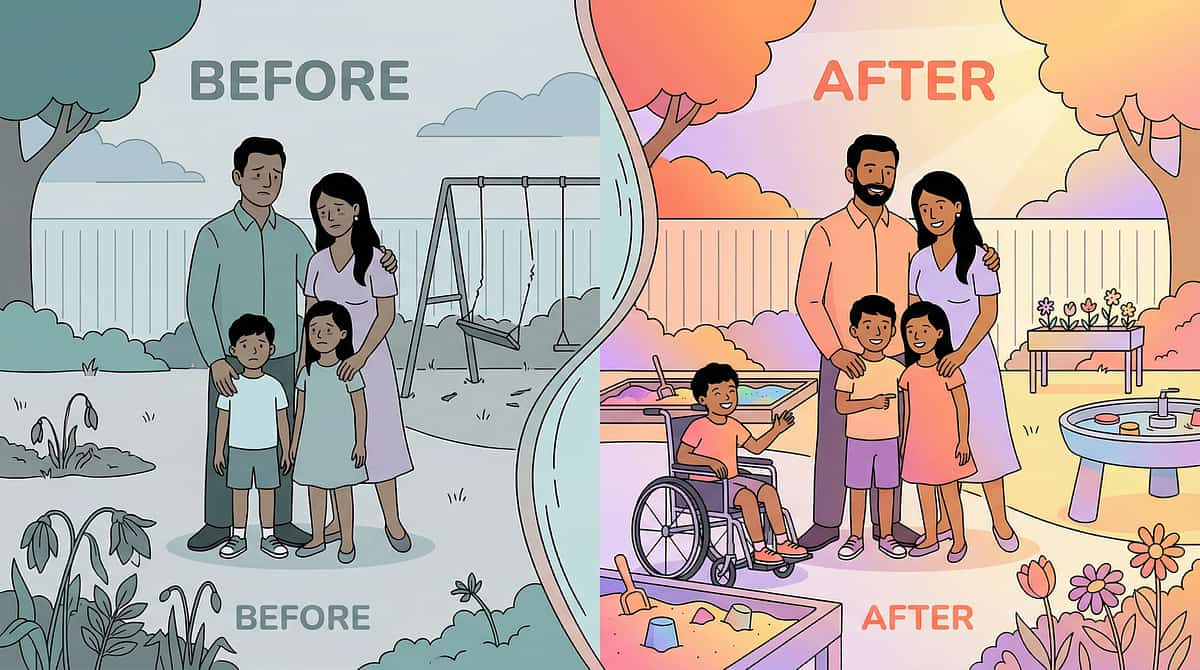
Before (Week 0): 4-year-old who would scream and arch when family members tried to hug. Grandparents believed the child didn't love them. Parents felt heartbroken. Every family gathering became a source of stress and shame.
After (Week 10): Family created a special "fist bump explosion" greeting. Child now RUNS to do it with grandparents. Gradually accepted sitting under a weighted blanket with mom. After 8 weeks, initiated a brief side hug with dad — the first in over a year.
After (Week 10): Family created a special "fist bump explosion" greeting. Child now RUNS to do it with grandparents. Gradually accepted sitting under a weighted blanket with mom. After 8 weeks, initiated a brief side hug with dad — the first in over a year.
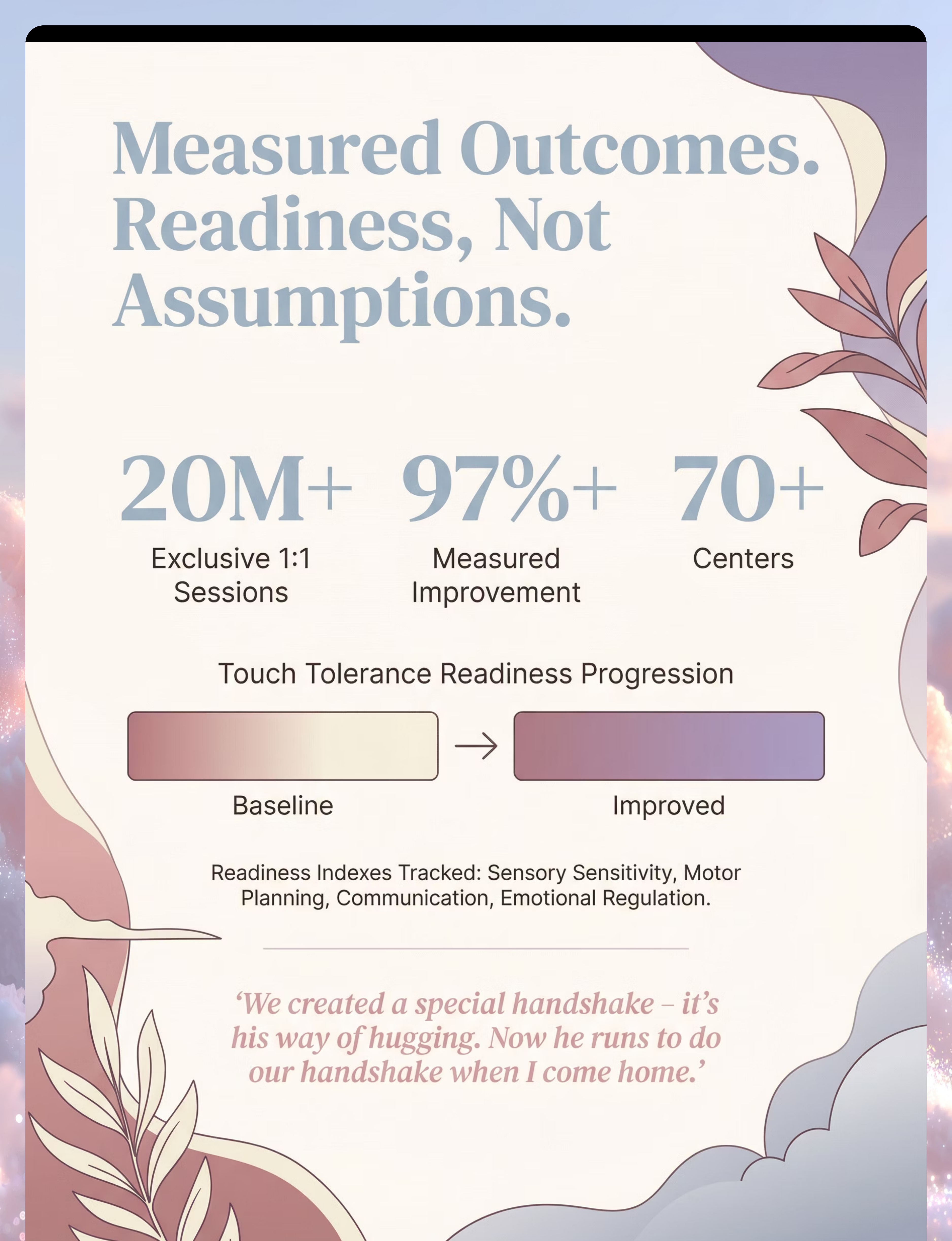
"We created a special handshake — it's his way of hugging. Now he runs to do our handshake when I come home. Grandma learned it too. It's connection, just different." — Parent, Pinnacle Blooms Network
2
Family Story 2 — Three Squeezes
Before (Week 0): 7-year-old who hugged stuffed animals enthusiastically but went rigid when family tried to hold her. Felt different from classmates who hugged friends easily. Mom grieved the cuddles she imagined.
After (Week 12): Compression vest under school uniform improved overall touch tolerance. Created a "butterfly kiss" ritual with mom. Began accepting brief firm hugs from dad. Taught her best friend a special handshake.
After (Week 12): Compression vest under school uniform improved overall touch tolerance. Created a "butterfly kiss" ritual with mom. Began accepting brief firm hugs from dad. Taught her best friend a special handshake.
"The breakthrough wasn't when she accepted a hug. It was when she created her own way to say 'I love you' — a three-squeeze hand hold. That was HER hug." — Pinnacle Blooms Therapist Notes
Connect With Other Parents
You are not alone in this journey. Connecting with other families navigating the same challenge accelerates your learning, lifts your spirits on hard days, and reminds you that there is always a path forward. Consistency across caregivers multiplies the impact of everything you do at home.
Sensory Solutions Parent Group
WhatsApp community for parents navigating tactile sensitivity challenges. Daily peer support, technique tips, and celebration of small wins. Join via pinnacleblooms.org/community
Touch and Connection Support Circle
Monthly virtual meetup for families working specifically on physical affection tolerance. Hosted by a Pinnacle OT specialist. Register at pinnacleblooms.org/events
Pinnacle Parent Forum
Online community with technique-specific discussion threads. Search by technique number, child age, or challenge type. pinnacleblooms.org/forum
Peer Mentoring Program
Connect with a parent who has already navigated this journey. Pinnacle's Peer Parent Program matches families by challenge type and child age. Once you've found what works, consider sharing your story — every family that learns from you is one less family navigating alone.

Your Professional Support Team
Home practice is powerful. Clinical support makes it even more powerful. The combination of consistent home implementation and professional clinical guidance produces the strongest outcomes in the research literature.
Find Your Nearest Pinnacle Blooms Center
Interactive map and center locator available at pinnacleblooms.org/centers
70+ centers across India, all operating under GPT-OS® clinical standards and consortium protocols.
70+ centers across India, all operating under GPT-OS® clinical standards and consortium protocols.
Therapist Matching for A-021
Primary match: Occupational Therapist — Sensory Integration Specialist
Supported by: BCBA for behavior strategies | SLP for communication support | NeuroDev Pediatrician for complex cases
Supported by: BCBA for behavior strategies | SLP for communication support | NeuroDev Pediatrician for complex cases
Teleconsultation
Can't visit a center? Book a virtual consultation with a Pinnacle specialist from anywhere. Available for parents who need guidance on technique implementation, troubleshooting, or deciding whether in-clinic assessment is needed.
pinnacleblooms.org/teleconsult
pinnacleblooms.org/teleconsult
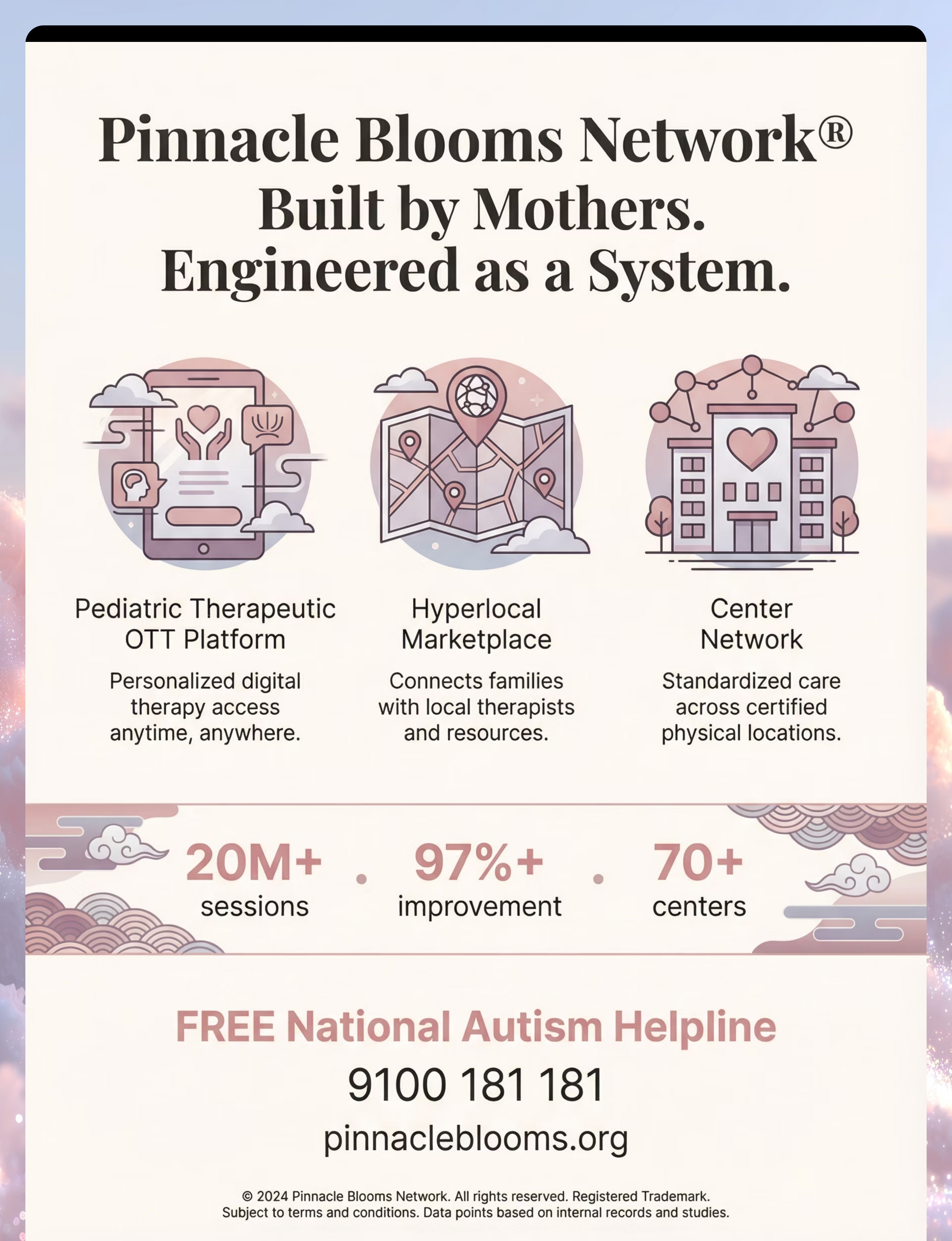
FREE National Autism Helpline
📞9100 181 181
Available in 16+ languages. Guidance, center referral, and initial consultation at zero cost to every family in India.
📧 care@pinnacleblooms.org
🌐 pinnacleblooms.org
Available in 16+ languages. Guidance, center referral, and initial consultation at zero cost to every family in India.
📧 care@pinnacleblooms.org
🌐 pinnacleblooms.org

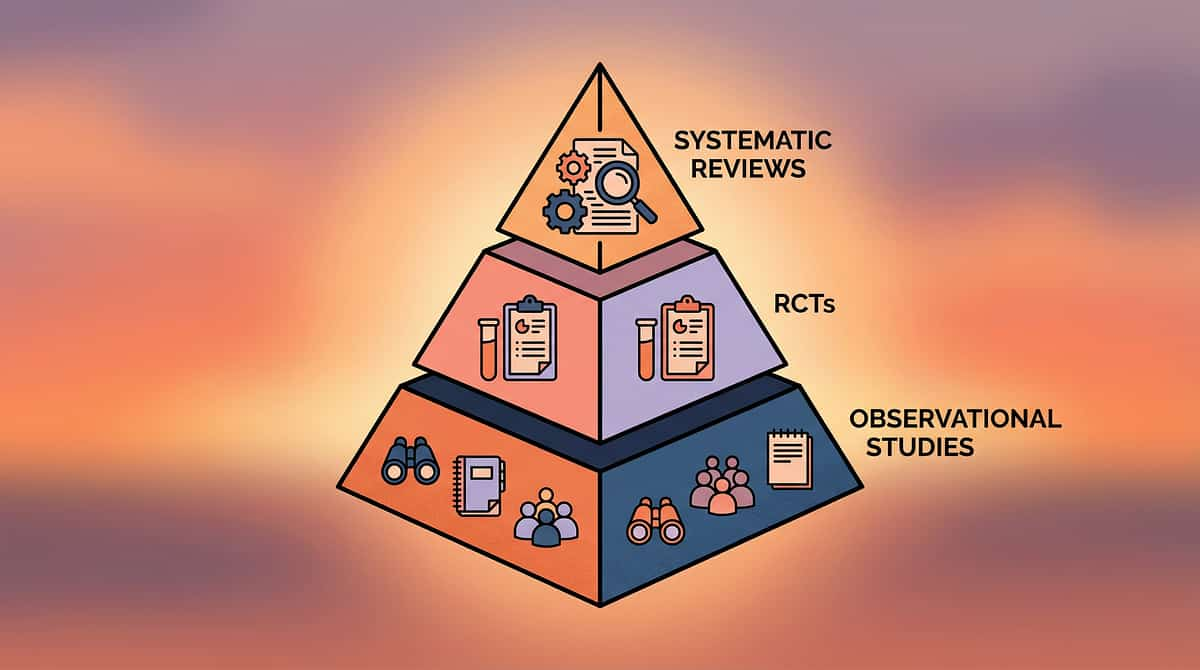
The Research Library
Every recommendation on this page is grounded in peer-reviewed, published evidence. Below is the complete reference set — organized by evidence level — so parents and clinicians alike can verify every claim.
Study | Key Finding | Reference | |
PRISMA Systematic Review (2024) | 16 articles confirm sensory integration meets evidence-based practice criteria for ASD | PMC11506176 | |
Meta-analysis (World J Clin Cases, 2024) | Significant improvement in social skills, adaptive behavior, sensory processing across 24 studies | PMC10955541 | |
Indian RCT (Padmanabha et al., 2019) | Home-based sensory interventions with significant outcomes in Indian pediatric population | DOI: 10.1007/s12098-018-2747-4 | |
WHO Nurturing Care Framework (2018) | CCD Package implemented across 54 countries; caregiver awareness directly impacts outcomes | PMC9978394 | |
Frontiers in Integrative Neuroscience (2020) | Neurological basis for sensory-based interventions in ASD established | DOI: 10.3389/fnint.2020.556660 | |
NCAEP Evidence Base (2020) | Sensory integration and visual supports classified as evidence-based practices | NCAEP 2020 Report | |
Multi-Disciplinary SLP Framework (2022) | Adapted UNICEF/WHO Nurturing Care Framework for multi-discipline integration | DOI: 10.1080/17549507.2022.2141327 |
Additional sources: SPD Foundation | AOTA Clinical Guidelines | Dunn, W.: Sensory Profile 2 | Kranowitz, C.S.: The Out-of-Sync Child | nurturing-care.org
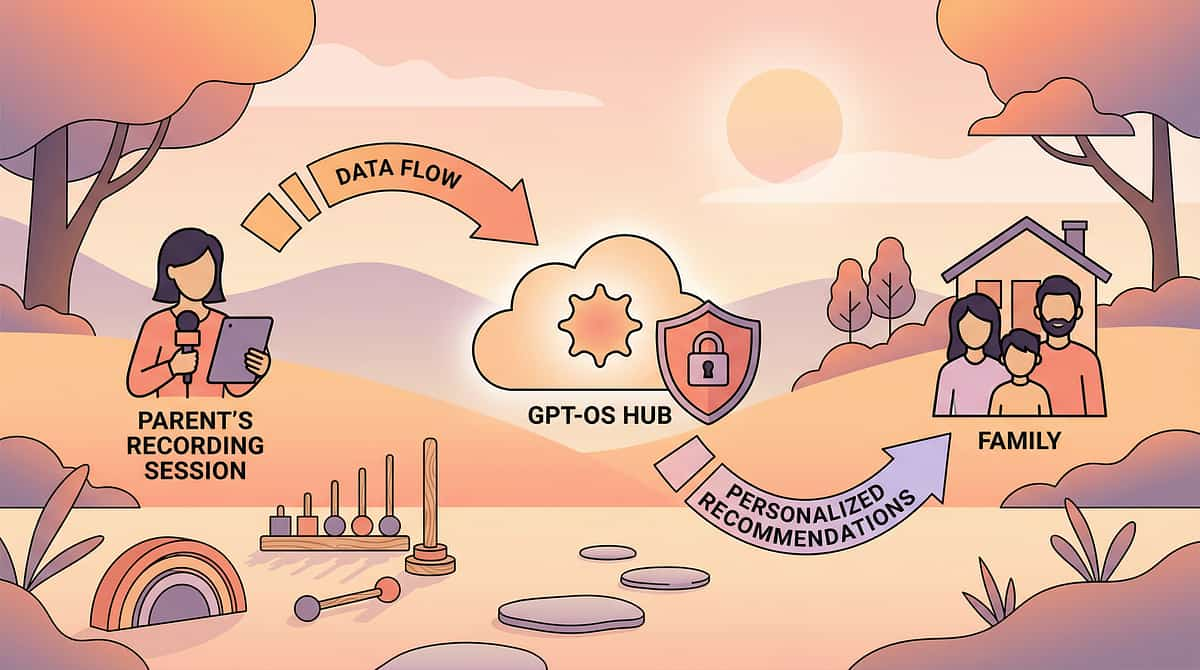
How GPT-OS® Uses Your Data
Your data powers better outcomes — for your child and every child like yours. Every session you track makes GPT-OS® smarter, and makes the next family's journey easier and faster.
What GPT-OS® Learns From This Technique's Data
- Which materials produce fastest touch tolerance gains for which sensory profiles
- Optimal session frequency and duration for tactile desensitization
- Which alternative affection rituals have highest adoption rates by age group
- Progression timelines: how long from alternative rituals → modified hugs → comfortable contact
Privacy and Data Protection
- Data is encrypted, anonymized, and protected under international standards
- Individual data is NEVER shared, sold, or used beyond improving your child's outcomes
- Request data access, modification, or deletion at any time
- Compliant with India's Digital Personal Data Protection Act and international privacy frameworks
Watch the Reel — A-021 in Action
Seeing is believing. This short reel demonstrates each of the 9 materials in action — filmed with real families by Pinnacle Blooms Consortium therapists. Watch the difference between light touch and deep pressure. See alternative affection rituals in real homes with real children.
🎬 Reel A-021 — Sensory Solutions Series Episode 21
Domain: Sensory Processing → Tactile Over-Responsivity → Social-Emotional Connection
Duration: ~75 seconds
Presented by: Pinnacle Blooms Network® Consortium — Occupational Therapy Lead
Watch at: techniques.pinnacleblooms.org/sensory/child-avoids-hugs-tactile-sensitivity
Duration: ~75 seconds
Presented by: Pinnacle Blooms Network® Consortium — Occupational Therapy Lead
Watch at: techniques.pinnacleblooms.org/sensory/child-avoids-hugs-tactile-sensitivity
This Reel shows each of the 9 materials in action — the weighted blanket shared between parent and child, the body sock in play, the difference between light touch and deep pressure hugs, and alternative affection rituals in real family settings. Series continues with A-022: 9 Materials That Help When Child Is Overwhelmed by Noise.

Share This With Your Family
Consistency across caregivers multiplies impact. If only you execute this technique, its impact is limited to your sessions. When your spouse, grandparents, school teachers, and other caregivers all understand AND use your child's alternative affection strategies — every interaction becomes therapeutic.
Share This Page
📱 Share via WhatsApp
📧 Send via Email
🔗 Copy Link: techniques.pinnacleblooms.org/sensory/child-avoids-hugs-tactile-sensitivity
📧 Send via Email
🔗 Copy Link: techniques.pinnacleblooms.org/sensory/child-avoids-hugs-tactile-sensitivity
Download Family Guide (1-Page PDF)
A simplified one-page guide including what hug avoidance means (NOT rejection), your child's specific alternative affection rituals, and clear do's and don'ts for family members.
"Explain to Grandparents" Version
A warm, simple explanation for extended family: Your grandchild loves you deeply. Their brain processes touch differently. Here is THEIR special greeting — learn it, use it, treasure it. What NOT to do (no forced hugs, no guilt).
Teacher / School Communication Template
A professional letter template explaining your child's touch preferences for school settings — designed for teachers, aides, and school counselors who interact with your child daily.
WHO CCD Package emphasizes multi-caregiver training as critical for intervention generalization and maintenance. Reference: PMC9978394
Frequently Asked Questions
The questions every parent asks — answered with evidence, empathy, and honesty. If you don't find your answer here, ask GPT-OS® at pinnacleblooms.org/ask or book a teleconsultation at pinnacleblooms.org/teleconsult.
Q: Does hug avoidance mean my child doesn't love me?
A: No. Attachment (love) and sensory tolerance (touch processing) are independent neurological systems. Your child can love you with their whole heart while their nervous system finds hugging overwhelming. The love is real. The sensory barrier is real. Both exist simultaneously. (See Card 3 for the neuroscience.)
Q: Will my child ever be able to hug normally?
A: Many children significantly improve their touch tolerance with consistent intervention. Some reach full typical hugging. Others develop rich alternative affection repertoires that are equally meaningful. Both outcomes represent complete success. The goal is connection, not a specific physical form of it.
Q: My mother-in-law says I'm spoiling my child by not making them hug. What do I do?
A: Share the Family Guide from Card 37 with her. Explain that forced hugging creates trauma and increases avoidance — the opposite of the goal. Teach her your child's alternative greeting. Grandparents who learn the alternative ritual often become the child's favorite person.
Q: Is this just autism, or can other children have this too?
A: Tactile over-responsivity affects children with autism, sensory processing disorder, anxiety, and some neurotypical children with sensory sensitivity. The intervention principles are the same regardless of diagnosis.
Q: How long before I see results?
A: Typically 2–4 weeks for initial tolerance changes, 5–8 weeks for consolidated progress, and 8–12 weeks for meaningful behavioral shifts. Progress is measured in seconds of additional tolerance, not dramatic overnight changes. (See Cards 23–25 for detailed timelines.)
Q: My child hugs the dog but not me. Why?
A: Animals are sensorially predictable — consistent body temperature, fur texture, no social expectations, no varying pressure. Your child CAN hug when sensory variables are controlled. Your job is to gradually become as predictable as the dog: firm, consistent, brief, expected.
Q: Should I stop trying to hug my child entirely?
A: No. Continue offering — but offer, don't force. "Would you like a squeeze?" Give them the choice. And build your alternative affection rituals so that connection flows through channels they can handle.
Q: Can I use these materials for other sensory challenges too?
A: Yes. Weighted blankets, body socks, and compression vests support sensory regulation across many challenges — not just hug avoidance. See Card 29 for related techniques using the same materials.

Your Next Step
You Have the Knowledge. You Have the Materials. You Have the Plan.
Start today. The path forward is clear, evidence-based, and waiting for you right now. Every day you delay is a day of connection your child doesn't have to wait for.
🟢 Start This Technique Today
Launch a guided GPT-OS® session with step-by-step prompts. The system walks you through every card in real time, adapted to your child's current profile.
pinnacleblooms.org/start/A-021
pinnacleblooms.org/start/A-021
📞 Book a Consultation
Speak directly with a Pinnacle sensory integration specialist. Free guidance available now.
FREE National Autism Helpline: 9100 181 181
Or book online: pinnacleblooms.org/consult
FREE National Autism Helpline: 9100 181 181
Or book online: pinnacleblooms.org/consult
🔄 Explore the Next Technique
A-022: 9 Materials That Help When Child Is Overwhelmed by Noise — the natural companion to this technique for children with co-occurring sensory challenges.
techniques.pinnacleblooms.org/sensory
techniques.pinnacleblooms.org/sensory
Validated by the Pinnacle Blooms Consortium. Disciplines: OT • SLP • ABA • SpEd • NeuroDev • CRO. 20M+ sessions. 97%+ measured improvement. 70+ centers.
Preview of 9 materials that help when child avoids hugs Therapy Material
Below is a visual preview of 9 materials that help when child avoids hugs therapy material. The pages shown help educators, therapists, and caregivers understand the structure and content of the resource before use. Materials should be used under appropriate professional guidance.








Link copied!

The Pinnacle Promise
Built by Mothers. Engineered as a System.
From fear to mastery. One technique at a time.
The Pinnacle Blooms Consortium
Clinical Research Organization | Speech-Language Pathologists | Occupational Therapists | Board Certified Behavior Analysts | Special Educators | NeuroDevelopmental Pediatricians | WHO/UNICEF Aligned Practices
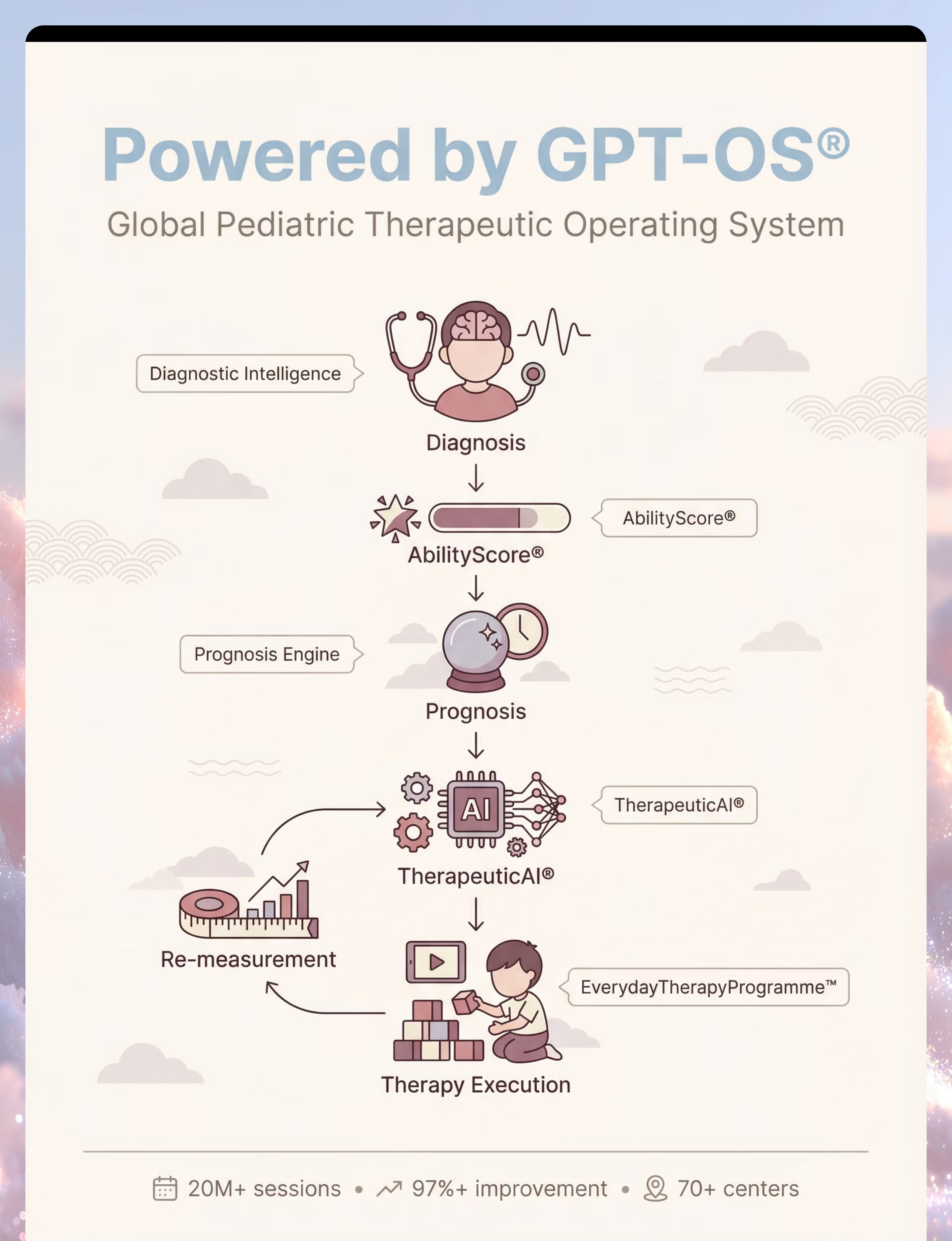
Powered by GPT-OS®
Global Pediatric Therapeutic Operating System
20M+ exclusive 1:1 sessions • 97%+ measured improvement • 70+ centers • Patents filed across 160+ countries
20M+ exclusive 1:1 sessions • 97%+ measured improvement • 70+ centers • Patents filed across 160+ countries
Reach Us
📞 FREE Helpline: 9100 181 181 (16+ languages)
🌐 pinnacleblooms.org
📧care@pinnacleblooms.org
📚 techniques.pinnacleblooms.org
🌐 pinnacleblooms.org
📧care@pinnacleblooms.org
📚 techniques.pinnacleblooms.org
Medical Disclaimer: This content is educational and informational. It does not replace assessment, diagnosis, or treatment by a licensed occupational therapist, developmental pediatrician, or other qualified healthcare professional. Touch avoidance can reflect tactile processing differences, anxiety, trauma history, or other factors requiring professional evaluation. Individual results vary. Statistics represent aggregate outcomes across Pinnacle Blooms Network. Always consult with your child's healthcare team before beginning any intervention protocol.
© 2025 Pinnacle Blooms Network®, unit of Bharath Healthcare Laboratories Pvt. Ltd. All rights reserved. GPT-OS®, AbilityScore®, TherapeuticAI®, EverydayTherapyProgramme™, and FusionModule™ are registered trademarks of Bharath Healthcare Laboratories Pvt. Ltd. CIN: U74999TG2016PTC113063 | DPIIT: DIPP8651 | MSME: TS20F0009606 | GSTIN: 36AAGCB9722P1Z2