
"The baby cries. Within seconds, I have two children in crisis."
When your older child melts down every time the baby cries — screaming, covering ears, begging you to make it stop, running from the room — it feels like your family is breaking. You expected some sibling adjustment. You did not expect this.

RECOGNITION
You Are Not Failing. Your Child Is Not Broken.
What You're Seeing
Your older child's nervous system is treating baby crying like an alarm that will not turn off. The pitch, the urgency, the unpredictability — sounds designed by evolution to be impossible to ignore — are flooding a sensory system that cannot filter them.
This is not jealousy. This is not sibling rivalry. This is not a behavior choice. This is neurology. And there are materials that help.
"A child who begs you to 'make the baby stop' is not rejecting their sibling. Their auditory system is genuinely overwhelmed by one of the most acoustically demanding sounds in human experience." — Pinnacle Blooms Consortium (OT, SLP, BCBA, NeuroDev, Pediatrics)
WHO Nurturing Care Framework (2018): Responsive caregiving requires understanding each child's unique sensory needs within the family system.

PREVALENCE & NORMALIZATION
This Happens in Millions of Homes. Every Day.
For children with auditory over-responsivity, baby crying is experienced at heightened intensity — as if the volume is permanently turned to maximum and there is no off switch. The distress is genuine. The reactions are proportional to what the child is experiencing, even when they appear disproportionate to adults with typical sensory filtering.
1 in 6
Sensory Differences
Children show signs of sensory processing differences (SPD Foundation)
80%+
ASD & Auditory
Children with ASD experience auditory processing difficulties (PRISMA Review, PMC11506176)
1 in 4
Auditory Defensiveness
Sensory-sensitive children show specific defensiveness to high-frequency sounds
18M+
Families in India
Navigating pediatric developmental differences (National estimates, Census + prevalence data)
You are not the only family living this. You are one of millions. And solutions exist.
Baby Crying Was Designed to Be Impossible to Ignore. Their Nervous System Can't Filter It.
Baby crying is not just any loud sound. Evolution engineered infant cries with specific acoustic properties designed to guarantee adult response. For a child with typical auditory processing, the brain's thalamic filter reduces the intensity to "unpleasant but tolerable." For a child with auditory over-responsivity, this filter malfunctions — the sound arrives at the cortex at full intensity, the amygdala reads it as threat, and fight-or-flight launches. Not once, not occasionally — every single time the baby cries.
Frequency
300–600 Hz with harmonics reaching the high-frequency range most distressing for auditory-sensitive children
Intensity
Can reach 100+ decibels — comparable to power tools or a motorcycle engine at close range
Onset
Sudden, unpredictable — the child never knows when it's coming and cannot prepare
Duration
Variable and uncontrollable — the child cannot stop it and cannot predict when it will end
Key Message: Your child's reaction isn't about understanding. No amount of explaining that "babies cry" changes how their nervous system processes the sound. This requires sensory tools, not logic.

DEVELOPMENTAL CONTEXT
When Crying Sensitivity Meets New Sibling Reality
This challenge sits at the intersection of two developmental realities: auditory over-responsivity (which may pre-exist or be newly revealed) and the arrival of a crying infant into the child's daily environment.
The older child may have been sensitive to other sounds previously — vacuum, blender, loud voices — and baby crying becomes the most intense and frequent trigger. Or the child appeared to have typical auditory processing until the constant, inescapable nature of baby crying exposed a vulnerability that quieter daily life never revealed.
Why this is a family-level challenge: Baby crying cannot be eliminated. The older child cannot leave the home. The parent is simultaneously needed by both children. The child may develop anticipatory anxiety — tensing every time the baby fusses, hypervigilant for the next cry.
Sleep Disrupted
Fear of being woken by nighttime crying
Mealtimes Derailed
Family routines compromised at every level
Comorbidity
Often co-occurs with tactile, visual, vestibular sensitivity and anxiety
WHO/UNICEF CCD
Family-level intervention is essential — each child's needs addressed within the family system
EVIDENCE BASE
Evidence Grade: Level I–II | Systematic Review + Meta-Analysis Supported
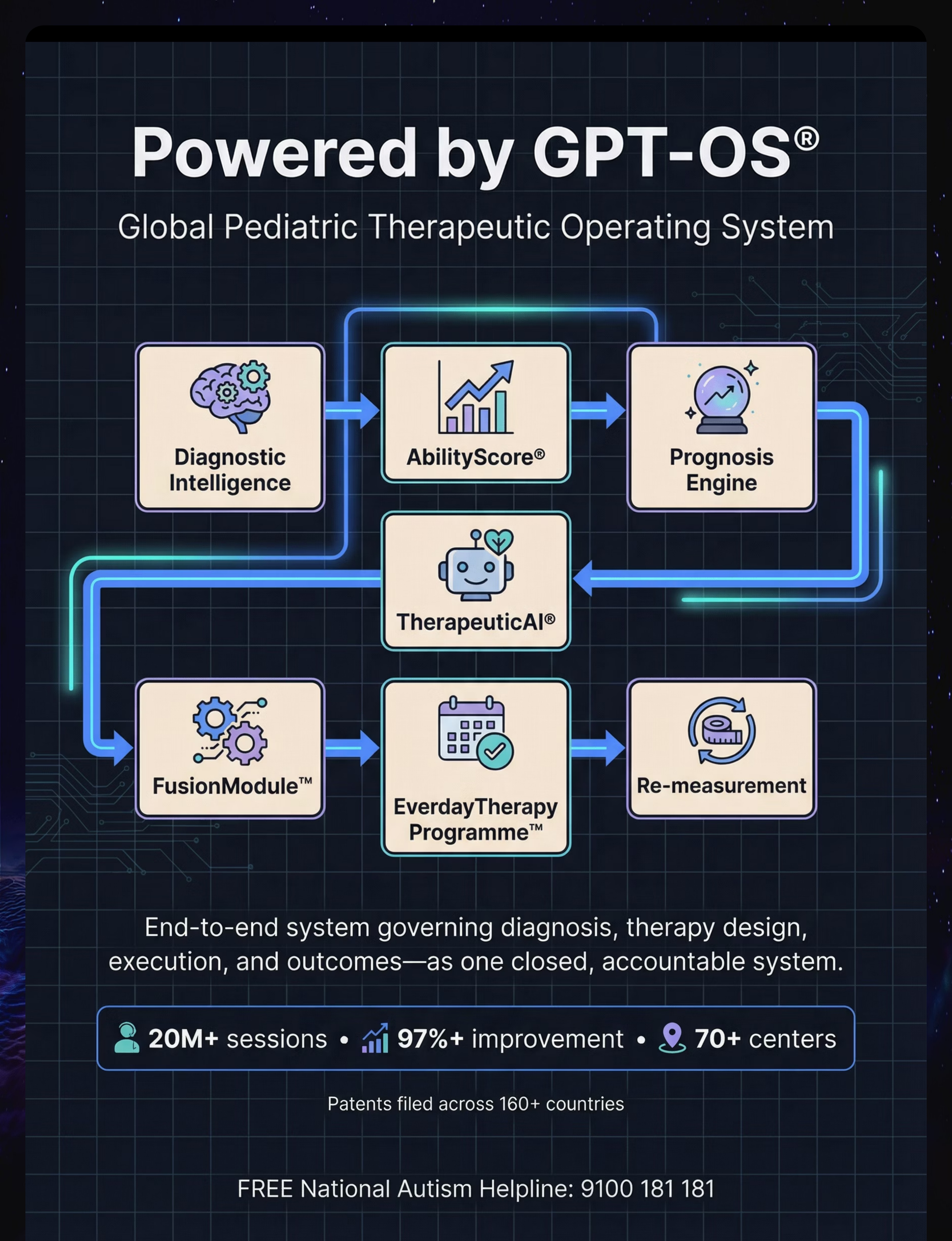
This technique page represents the integrated clinical perspective of the Pinnacle Blooms Consortium — Occupational Therapists, Speech-Language Pathologists, Board Certified Behavior Analysts, Special Educators, NeuroDevelopmental Pediatricians, and Family Systems Specialists — drawing on 21M+ therapy sessions and continuous population-level outcome data via GPT-OS®.
1
PRISMA Systematic Review (PMC11506176)
"Comprehensive review demonstrating 80%+ prevalence of sensory processing difficulties in ASD populations, with auditory over-responsivity as one of the most functionally impactful."
2
Meta-Analysis — World J Clin Cases 2024 (PMC10955541)
"24 studies analyzed. Sensory integration therapy effectively improved social skills, adaptive behavior, sensory processing, and motor skills."
3
Indian J Pediatrics RCT 2019
"Randomized controlled trial establishing efficacy and safety of parent-administered sensory interventions in Indian home settings." DOI: 10.1007/s12098-018-2747-4
4
WHO/UNICEF CCD Package (PMC9978394)
"Multi-country implementation across 54 LMICs demonstrating family-level intervention efficacy with household-available materials."
5
Porges Polyvagal Theory
"Auditory processing directly linked to autonomic nervous system regulation. Middle ear muscle function modulates sound sensitivity and social engagement."
Supporting frameworks: SPD Foundation (spdfoundation.net) · AOTA (aota.org) · NCAEP Evidence-Based Practices Report (2020) · OCEBM Levels of Evidence

TECHNIQUE DEFINED
Multi-Material Auditory Coping Protocol for Infant Crying Sensitivity
SEN-AUD-CRY
Ages 2–12
Home + Family
Daily Integration
A multi-layered intervention protocol that combines auditory protection, environmental modification, sensory regulation tools, cognitive preparation, and positive association building to enable sensory-sensitive children to coexist with a crying infant sibling. This technique addresses the auditory over-responsivity — not the baby's behavior. The goal is functional family life with manageable coping, not the elimination of all distress.
Layer 1: Auditory Protection
Reduce the intensity of sound reaching the child's ears — ear defenders, noise-canceling headphones, white noise
Layer 2: Environmental Modification
Create physical refuge from the sound — designated safe/quiet space
Layer 3: Sensory Regulation
Provide competing, calming input — fidgets, weighted and compression items
Layer 4: Cognitive Preparation
Build understanding and predictability — social stories, visual timers
Layer 5: Positive Association
Transform the experience — special activities that only happen during crying episodes
MULTI-DISCIPLINARY MAP
Four Disciplines. One Family. One Integrated Approach.
Occupational Therapist (Primary Lead)
Sensory processing evaluation, auditory modulation assessment, sensory diet design, environmental modification, ear protection selection, weighted/compression prescription, and desensitization planning. OTs specialize in how the nervous system processes sensory input.
Board Certified Behavior Analyst (BCBA)
Behavioral assessment of crying-triggered responses, positive association programming, systematic desensitization hierarchy, reinforcement strategies, and data collection protocols. BCBAs bring precision to the behavioral layer.
Speech-Language Pathologist (SLP)
Social story creation, communication supports for child to express distress, developing verbal coping scripts, and narrative comprehension — helping the child understand "babies cry → parents help → baby stops."
NeuroDevelopmental Pediatrician
Comprehensive developmental evaluation, differential diagnosis (hyperacusis vs. auditory over-responsivity vs. anxiety), ruling out ear pathology, and medical context for sensory profile.
GPT-OS® FusionModule™ coordinates all disciplines into a single converged therapeutic pathway. No silos. One plan. One child. One family.

THERAPEUTIC GOALS
Precision Targets: What This Technique Improves
Primary Targets (Core)
- Auditory tolerance to infant crying (measured: duration before distress onset)
- Distress severity during crying episodes (measured: behavioral indicators on 1–4 scale)
- Independent coping strategy use (measured: self-initiated use of ear protection, safe space, fidgets)
- Sibling coexistence (measured: time able to remain in same home space during crying)
Secondary Targets (Downstream)
- Anticipatory anxiety reduction — less hypervigilance about baby's state
- Sleep quality — reduced fear of being woken by crying
- Active coping repertoire — number and flexibility of strategies used
- Self-advocacy: "I need my ear helpers" instead of meltdown
- Recovery time after crying episodes
Tertiary Targets (Long-Term)
- Family functioning and quality of life
- Sibling relationship quality during non-crying times
- Emotional regulation generalization to other challenges
- Community participation — family events, visiting homes with babies

MATERIAL 1 OF 9
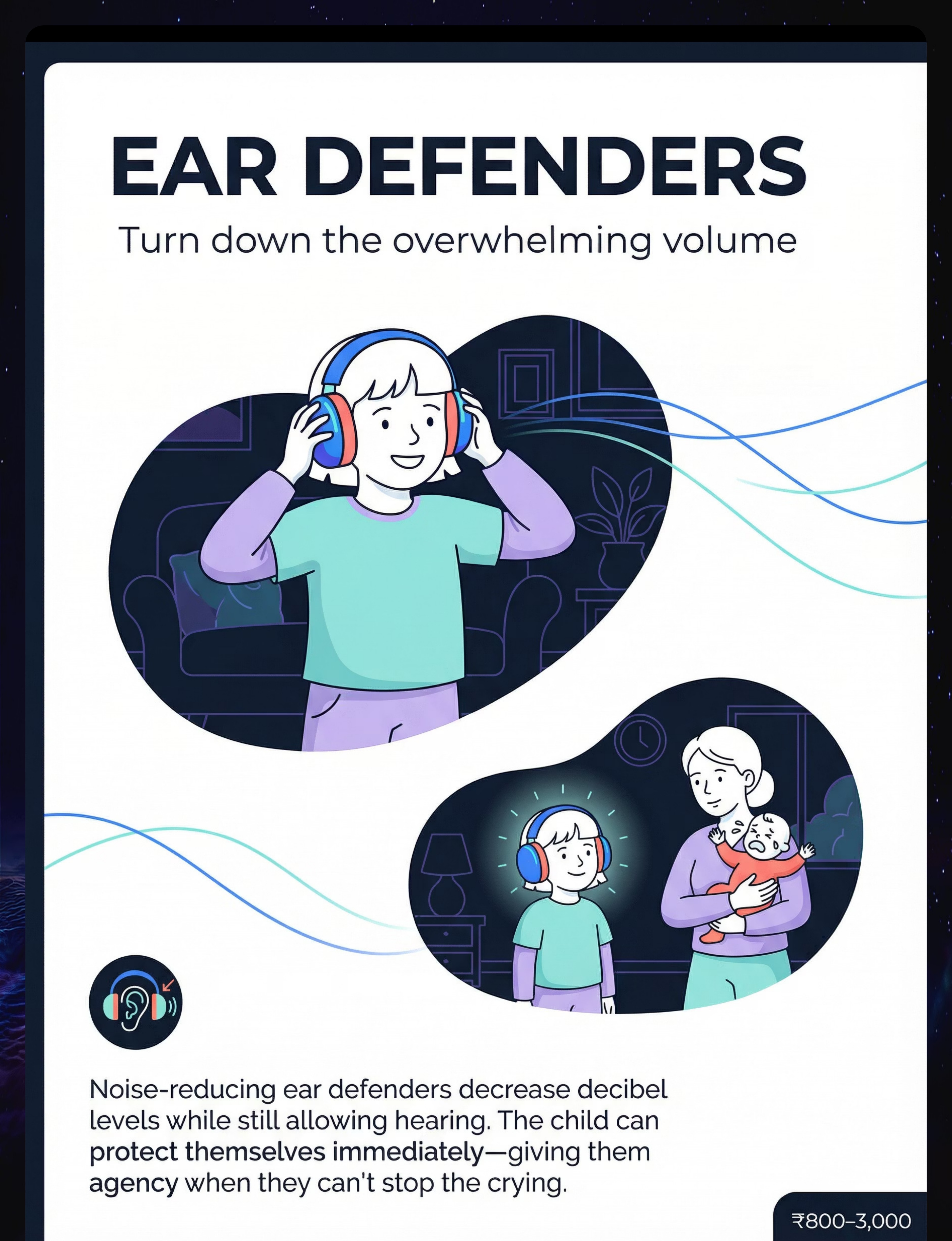
Noise-Reducing Ear Defenders

Canon #3
Sensory Regulation
₹800–3,000
The single most important tool in this protocol. Ear defenders reduce the decibel level reaching the child's auditory cortex, bringing the sound below the distress threshold. The child still hears the environment — they maintain full situational awareness — but the cry no longer arrives as an emergency signal.
Why it works: By reducing intensity, the thalamus can perform its filtering function. The amygdala does not activate. Fight-or-flight does not launch. The child stays regulated enough to use other coping tools.
- Place one pair in every room the child frequents
- Hang at child's height — accessible independently
- Introduce during calm, quiet times first — never first during active crying
- Let the child decorate them to build ownership and willingness
DIY Alternative: Industrial hearing protection from hardware store (₹200–500). Cotton balls or soft foam in a headband for very young children. Hands over ears is always the first line of defense.

MATERIAL 2 OF 9
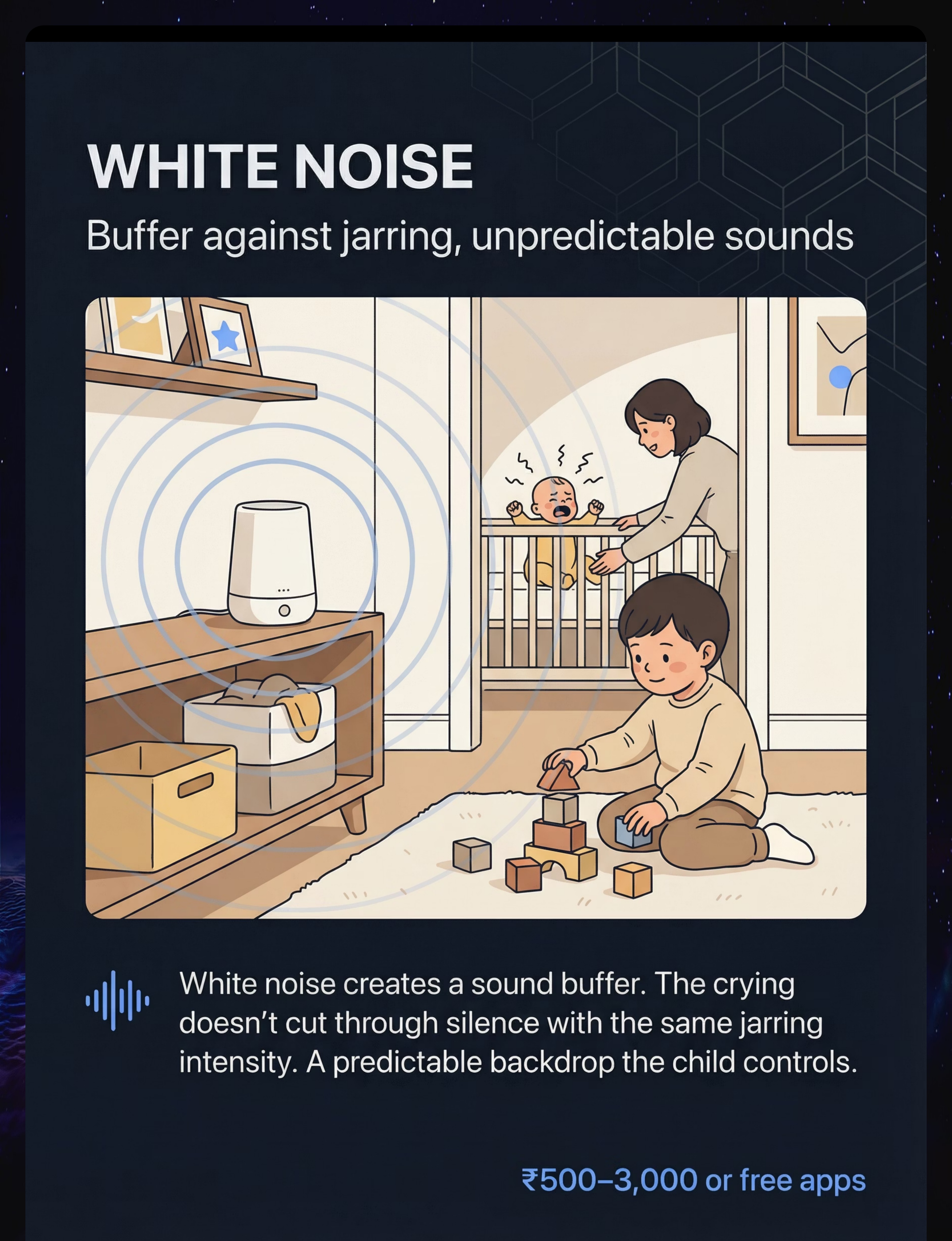
White Noise Machine or App
Canon #123
Sleep Supports
₹500–3,000 or Free
White noise works by masking the sharp onset of baby crying — the acoustic ambush that triggers the startle-to-overwhelm cascade. A continuous layer of sound in the background prevents the sudden contrast between silence and screaming that is itself a major component of the distress.
Why it works: The nervous system responds most intensely to sudden acoustic change. White noise reduces this contrast, giving the auditory system a gentler transition and reducing the startle element of the cry's onset.
- Run in child's bedroom all night — not just during crying episodes
- Let child choose preferred sound: rain, ocean, fan, brown noise
- Moderate volume — loud enough to mask, not loud enough to require shouting over
- Also useful in the calm space during daytime crying episodes
DIY: Box fan on low. Free apps: myNoise, Noisli. YouTube rain/ocean videos on phone or tablet. Running water in an adjacent room.

MATERIAL 3 OF 9
Designated Safe / Quiet Space
The safe space is the older child's refuge — a physical location in the home that belongs to them, is stocked with their tools, and carries the association of "this is where I go when sounds are too much." It is never a timeout location, never a punishment, never used for any purpose other than calm and regulation.
What to Stock
- Ear defenders on a hook at child's height
- Comfort items — weighted lap pad, favorite blanket, stuffed animal
- Fidget basket — 3–5 options
- Visual timer — in view, ready to start
- Special activity materials — tablet charged, activity box, preferred snack
- Social story — accessible for re-reading
Key Principles
- Set up in the room farthest from where baby typically cries or sleeps
- Let the child help design and stock it — ownership increases use
- The child CHOOSES to go — never sent there as consequence
- Practice visiting during calm, non-crisis times first
DIY: Large cardboard box with cushion inside. Blanket draped over a table. Child's bedroom with door closed. Closet converted with cushions. Budget: ₹0.
MATERIAL 4 OF 9
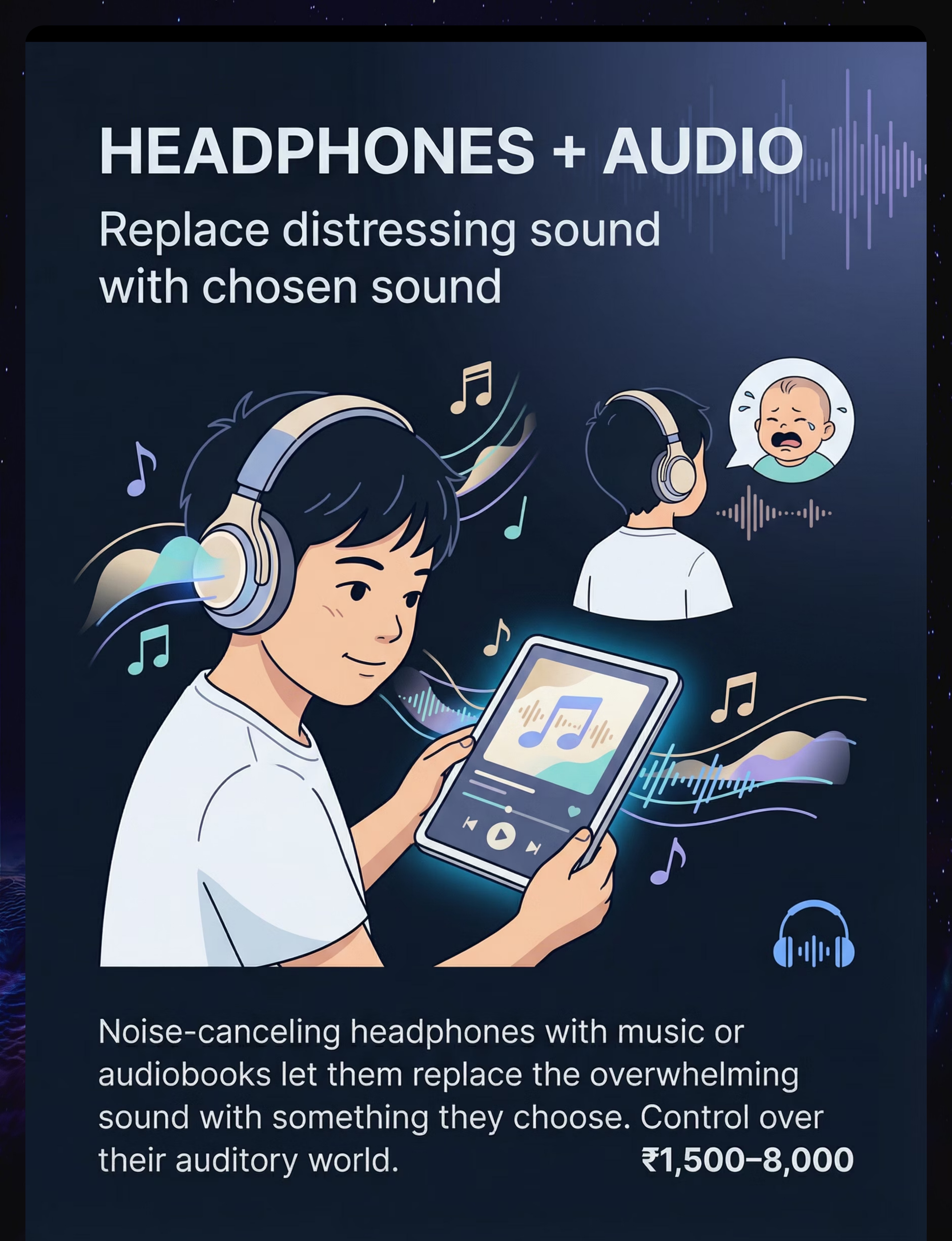
Noise-Canceling Headphones + Audio

Canon #3
Sensory Regulation
₹1,500–8,000
Headphones with audio add a second layer: not only do they reduce the intensity of baby crying, but they replace it with preferred auditory input — the child's favorite music, audiobooks, or calming sounds. This activates the positive association mechanism alongside the auditory protection function.
For older children (ages 7+) or those with tactile sensitivity to the hard shell of ear defenders, headphones with audio may be the preferred option. They are also more socially discreet — a consideration for school-age children who are aware of peer perceptions.
- Critical safety rule: Volume limits are essential — protect the child's hearing
- Child must be able to remove easily and independently
- Supervision required for young children using electronics
- Pre-load preferred playlist so child can start independently
DIY: Any over-ear headphones connected to phone playing the child's music. Budget earbuds with music. Even humming a tune with hands over ears provides measurable relief.

MATERIAL 5 OF 9
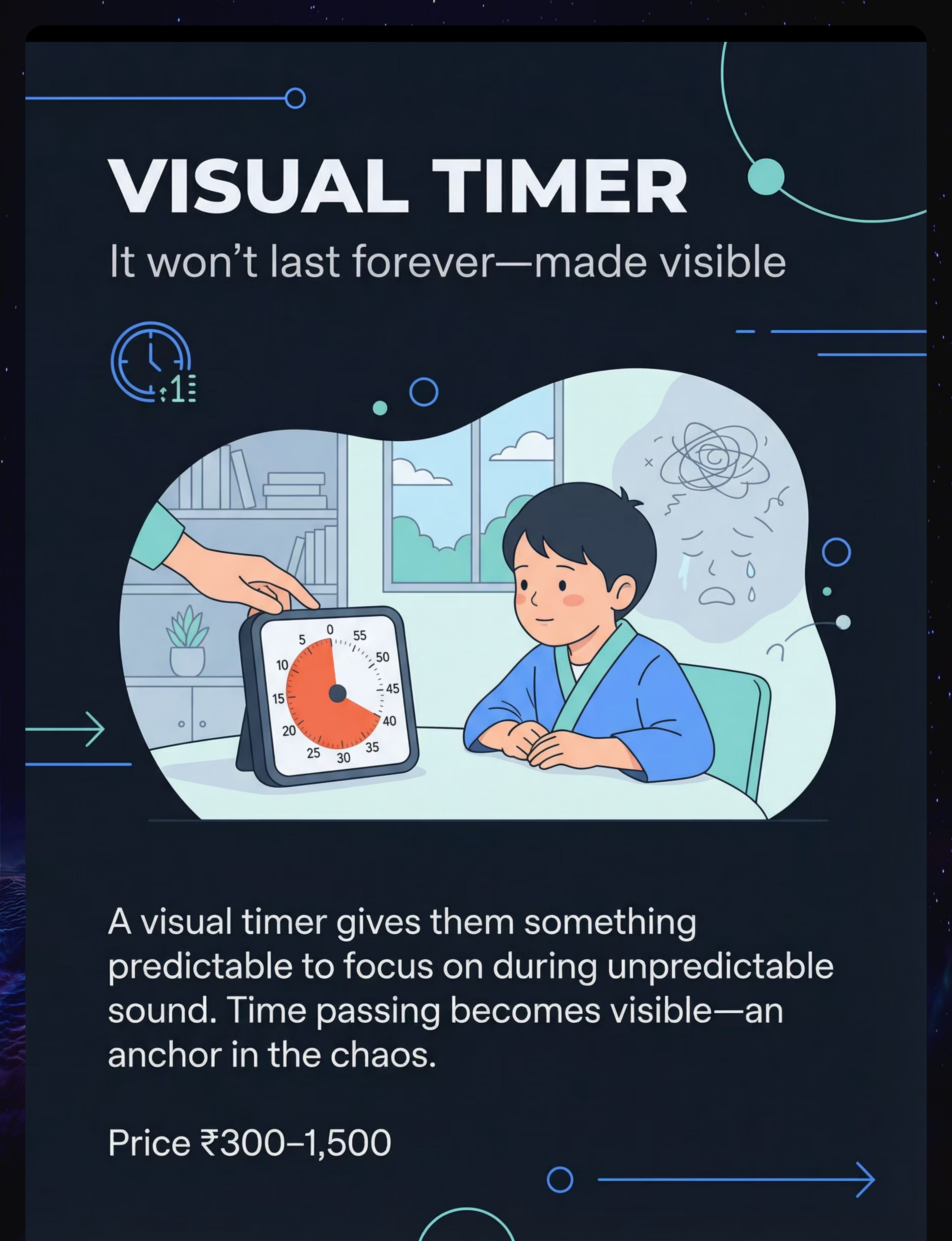
Visual Timer / Countdown
Canon #22
Visual Supports
₹300–1,500
One of the most distressing aspects of baby crying is its unpredictability — the child has no way to know when it will stop. The visual timer makes the abstract concept of "it won't last forever" concrete and visible. The child can see time passing. The unknown becomes bounded.
Why it works: Predictability is calming to the nervous system. The unknown is threatening. When the child can watch time elapse on a timer, the experience shifts from "endless suffering with no end" to "a defined period I can watch pass." This cognitive anchor reduces the secondary layer of panic that overlies the primary sensory overwhelm.
- Position in view from calm space and primary seating areas
- Start the timer as soon as crying begins
- Teach child to check the timer: "How much red is left?"
- Celebrate when the timer finishes — "You watched the whole time!"
DIY: Sand timer from toy store (₹50–100). Phone timer with visual countdown. Count backward together aloud. Sing a familiar song as a time marker.

MATERIAL 6 OF 9
Fidget Tools & Sensory Toys
Canon #4
Sensory Regulation
₹100–800
Fidget tools work by engaging the tactile and proprioceptive systems with competing, calming input — diluting the dominance of baby crying in the child's sensory experience. The nervous system has limited bandwidth. When the hands are occupied with squeezing, stretching, or manipulating a fidget, the brain is processing something other than the auditory threat.
Most Effective Types
- Squeeze balls — high proprioceptive input, simple, durable
- Textured objects — engages tactile system differentially
- Stretchy resistance toys — active hand engagement
- Smooth stones or polished objects — calming tactile input
- Playdough or putty — versatile, engaging, deeply regulating
Safety Notes
- Age-appropriate sizes only — no small parts for children under 3
- Some fidgets become projectiles during dysregulation — choose soft options for children prone to throwing
- Keep 3–5 options in the fidget basket — variety prevents habituation
DIY: Balloon filled with flour = stress ball. Chapati dough. Rubber bands. Textured fabric scraps. Ice cubes in a bag. Smooth stones from outside.

MATERIAL 7 OF 9
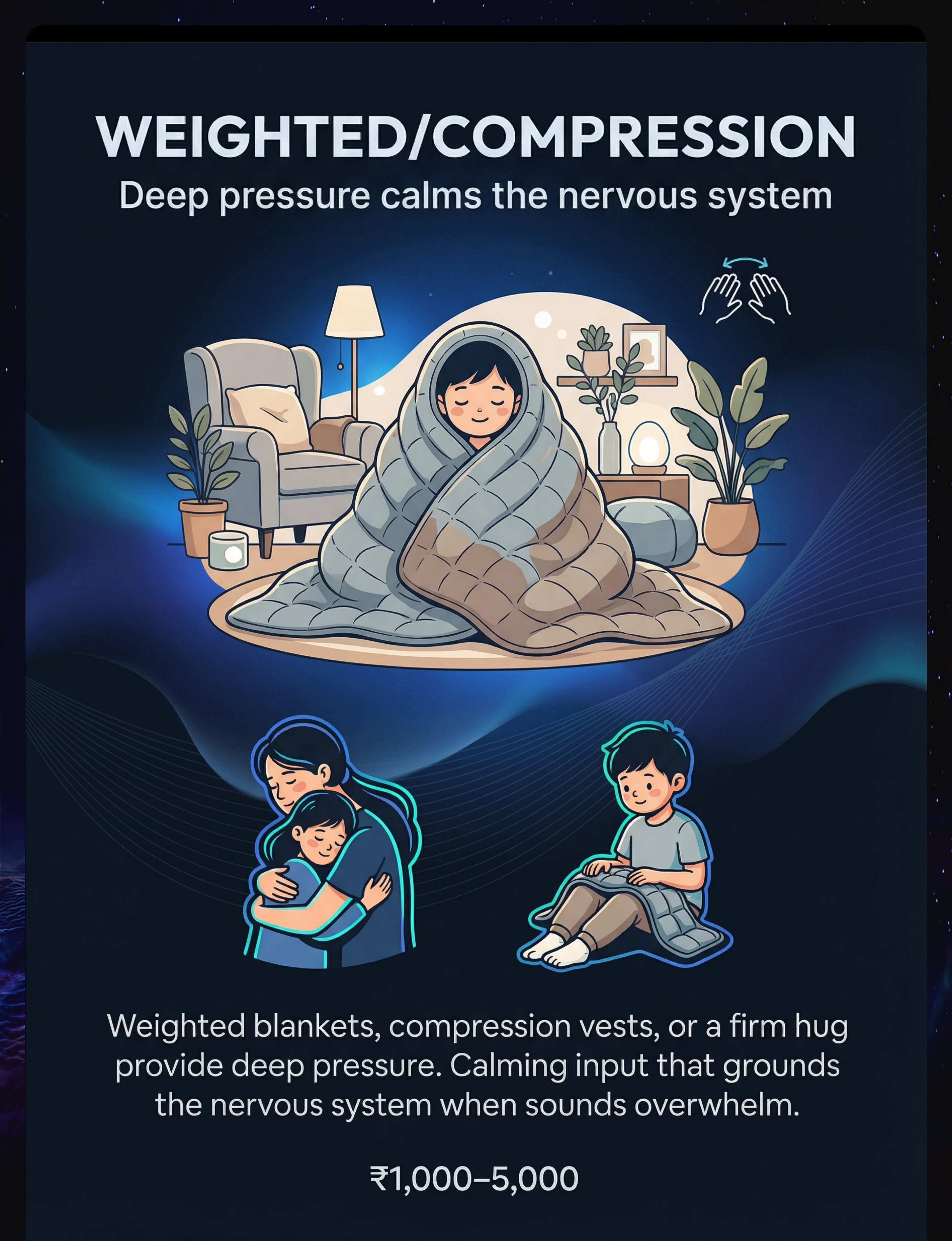
Weighted & Compression Items
Canon #1 & #2
Sensory Regulation
₹1,000–5,000
Deep pressure — delivered through weighted blankets, lap pads, or compression vests — is one of the most powerful nervous system regulation tools available. It activates the proprioceptive system and triggers a parasympathetic (calm-down) response, directly counteracting the sympathetic (fight-or-flight) state that baby crying induces in sensitive children.
- Weighted blanket or lap pad: Drape over child's legs or full body in calm space — 5–10% of child's body weight
- Compression vest/body sock: Provides all-over proprioceptive input — particularly useful for children who find weighted items on limbs uncomfortable
- Firm parent hug: Free, immediate, powerful — and validates the child simultaneously
Safety: Maximum 10% of child's body weight. Never on a child who cannot remove independently. Not for sleeping for children under 3. Weighted items are a regulated sensory tool — consult OT for prescription.
DIY: Heavy quilt or multiple blankets layered. Being wrapped snugly in a regular blanket. Bag of rice or lentils in a pillowcase as a lap weight.

MATERIAL 8 OF 9
Social Stories About Baby Crying
Canon #14
Emotional/Behavioral
₹0–500
Social stories address the cognitive-linguistic layer of the distress. A child who understands that "babies cry because they cannot talk yet, a parent always helps, and the crying always stops" has a narrative framework that contains the experience. Predictability and understanding are calming. Confusion and the unknown are threatening.
Read during calm, quiet times — not during active crying. Repeated readings (3+ per week) build the narrative into an accessible mental script. When crying starts, the child can recall: "The baby needs help. Mama/Papa is helping. It will stop."
Sample Script (Write Your Own)
"Sometimes Baby cries. Crying means she needs help. Mama/Papa helps her. Then she stops crying. I can use my ear helpers while she cries. The crying always stops."
DIY: Write 3–4 sentences with simple drawn pictures. Photograph your actual baby, your actual parent, your actual ear defenders. Personalized stories outperform generic ones.

MATERIAL 9 OF 9
Special Activity / Positive Association Builder
This is the most elegant mechanism in the protocol: classical conditioning, deliberately applied. A special activity — something the child loves but only has access to when the baby cries — gradually transforms the emotional valence of crying episodes from "pure suffering" to "suffering + something I love." Over repeated pairings, the anticipatory response shifts from dread to qualified acceptance.
How to Select the Special Activity
- Must be genuinely preferred — something the child would choose above most alternatives
- Must be exclusively reserved for crying times — not available any other time
- Must be immediately deployable — no setup delay when crying starts
- Age-appropriate: building sets, coloring books, playdough, favorite tablet content, special snack
The Conditioning Principle
When the child hears crying and says "Is it iPad time?" — the conditioning is working. The special activity does not eliminate the sensory discomfort. It provides a powerful competing experience that makes the episode endurable and builds a new, less terrible association with baby crying over time.
Cost: ₹0 — use any already-owned preferred item, reserved exclusively for crying times.
COMPLETE MATERIALS OVERVIEW
9 Materials That Help When Baby Crying Overwhelms
The full protocol at a glance — from essential-only to comprehensive. Your total investment for the essentials (ear defenders + calm space + social story) can be under ₹200 using DIY alternatives.
# | Material | Canon | Layer | Price (INR) | Priority | |
1 | Noise-Reducing Ear Defenders | #3 | Auditory Protection | ₹800–3,000 | 🏆 Start Here | |
2 | White Noise Machine or App | #123 | Auditory Protection | ₹500–3,000 / Free | 🏆 Start Here | |
3 | Designated Safe/Quiet Space | #12 | Environmental | ₹0–2,000 | 🏆 Start Here | |
4 | Noise-Canceling Headphones + Audio | #3 | Auditory Protection | ₹1,500–8,000 | Recommended | |
5 | Visual Timer / Countdown | #22 | Cognitive Prep | ₹300–1,500 | Recommended | |
6 | Fidget Tools & Sensory Toys | #4 | Sensory Regulation | ₹100–800 | Recommended | |
7 | Weighted / Compression Items | #1, #2 | Sensory Regulation | ₹1,000–5,000 | Recommended | |
8 | Social Stories (Baby Crying) | #14 | Cognitive Prep | ₹0–500 | Recommended | |
9 | Special Activity / Distraction | — | Positive Association | ₹0–varies | Recommended |
Essentials Only (₹0–3,000): Ear defenders + safe space + social story = a complete foundation. Add other materials as resources allow.

SAFETY GATE
Safety Gate: Read This Before Starting
🔴 DO NOT PROCEED IF:
- The older child has a current ear infection, surgery, or ear pain
- The child is in acute crisis — active meltdown, self-injury in progress
- The child has shown aggression toward the baby — implement safety barriers first
- The baby is in medical distress — attend to baby's safety first
🟡 PROCEED WITH CAUTION IF:
- Child resists or is distressed by headphones/ear defenders — introduce gradually
- Distress appears to have BOTH sensory AND behavioral/jealousy components
- Child shows significant anxiety beyond the immediate sound
- Child has hearing concerns or has not had a recent hearing assessment
🟢 PROCEED WHEN:
- Child is currently regulated — not mid-meltdown
- Materials have been introduced during calm times first
- Child understands tools are to help, not to punish or banish
- Parent is calm and prepared — not in crisis mode
- Safe space is genuinely safe with easy exit
🔴 RED LINE — Stop and seek professional help if: Self-injury is escalating · Aggression toward baby has occurred · Fear is spreading beyond crying episodes · Sleep disruption is severe and worsening · Child shows signs of depression or withdrawal · Parent burnout is compromising safety for any family member.

ENVIRONMENT SETUP
Two Zones That Transform Your Home During Crying
Zone 1: The Calm Space (Older Child's Refuge)
Set up in the room farthest from where baby typically cries or sleeps. Stock completely before the next crying episode.
- Position 1: Ear defenders on hook at child's height
- Position 2: Comfort items — weighted lap pad, favorite blanket, stuffed animal
- Position 3: Fidget basket — 3–5 options
- Position 4: Visual timer — in view, ready to start
- Position 5: Special activity materials — tablet charged, activity box, preferred snack
- Position 6: Social story — accessible for re-reading
- Position 7: Visual boundary — tent, curtain, or blanket draped over furniture
Zone 2: Immediate Access Stations (Every Room)
In every room the child frequents — ear defenders within arm's reach, always.
- Ear defenders hung at child's height (hook by door, basket by couch, nightstand)
- A single fidget item per room
- A visual cue card: "I can use my ear helpers. I can go to my calm space. I can do my special activity."
Nighttime Setup (Critical)
- White noise machine running at moderate volume in child's bedroom
- Ear defenders on nightstand within arm's reach
- Comfort items in bed
- Night light for orientation
- Increase physical distance between child's room and nursery if possible

READINESS CHECK
The Pre-Session Checklist (60 Seconds)
Check every box before the protocol is live. A child pushed into a sensory experience when unready learns to dread the tools, not use them. The best session is one that starts right.
1
Fed and Hydrated?
Hunger amplifies sensory sensitivity. Ensure the child has eaten recently.
2
Rested?
Fatigue drastically reduces tolerance. Not after a bad night's sleep or missed nap.
3
Currently Regulated?
No active distress. Recent meltdown recovery complete. Calm baseline.
4
Tools Introduced During Calm Time?
Child has seen, touched, and understands tools BEFORE they're needed during crying.
5
Tools Accessible?
Ear defenders within arm's reach. Calm space stocked. Special activity ready.
6
Parent Calm and Prepared?
Parent regulation matters. If parent is dysregulated, the child reads it and amplifies.
ALL GREEN → GO. Proceed with protocol as designed.
1–2 AMBER → MODIFY. Use maximum protection immediately rather than graded approach.
ANY RED → POSTPONE. Address the red flag first. Return to protocol when resolved. No harm in waiting — harm in forcing.
INTRODUCING TOOLS
Introducing the Tools: Scripts That Work
Critical Timing: Introduce ALL tools during calm, quiet moments — NOT during active crying. The first exposure to ear defenders should never be when the baby is screaming.
For Ear Defenders (All Ages)
"These are your ear helpers. When sounds are too loud, you can put them on and the sound gets quieter. Want to try? See? You can still hear me, but the loud sounds get smaller. These are yours. You decide when to use them."
For Safe Space (Ages 3+)
"This is your special calm spot. When you need a break from loud sounds, you can come here. What should we put in it? Let's practice — pretend the sounds are loud — you walk here, sit down, and look — your favorite things are here."
For Social Story (Ages 2+)
"Let's read this story about Baby. See? Babies cry because they can't talk yet. Then Mama/Papa helps, and the baby stops. It always stops."
For Special Activity (Ages 3+)
"When Baby cries and the sounds are hard, you get to do [special thing]. It's just for those times. Only when Baby cries."
If resistance occurs: Don't force. Leave tools visible and accessible. Model use yourself. Try again tomorrow. Some children need several days to accept new objects near their head. Resistance is information — not failure.

ACTIVE ENGAGEMENT
When the Baby Starts to Cry: Your Action Sequence
Step 1: Signal (0–3 seconds)
"I hear the baby. Your ear helpers are right there." Point to accessible ear defenders. Voice: calm, matter-of-fact, not urgent. The parent's tone sets the child's alarm level.
Step 2: Equip (3–10 seconds)
If child reaches for defenders → "Good. You've got your helpers." If child freezes → calmly hand them. If child runs → let them. "Your calm space is ready for you."
Step 3: Anchor (10–30 seconds)
"You're okay. The sound is quieter now." Offer fidget or special activity. Start visual timer if helpful.
Step 4: Monitor (Ongoing)
While attending to baby: briefly check on older child. "The baby is getting help. She'll stop soon." Do NOT require the child to watch you soothe the baby or participate in any way.
Step 5: Reconnect (After Crying Stops)
"The baby stopped. You did a great job using your tools." Physical connection: hug, sit together, shared activity. "That was hard. You coped. I'm here now."

THERAPEUTIC MECHANISM
How These Materials Actually Work in the Brain
Volume Reduction (Ear Defenders / Headphones / White Noise)
By bringing decibels below the child's distress threshold, the auditory cortex processes "unpleasant but manageable" instead of "emergency." The amygdala doesn't trigger. Fight-or-flight doesn't launch. The child stays regulated.
Agency and Control (All Tools)
A child who can reach for ear defenders, walk to a calm space, start a timer, or choose an activity has AGENCY. The shift from "helpless victim of sound" to "person with tools" is itself regulating. Perceived control activates the prefrontal cortex, which modulates amygdala reactivity.
Competing Sensory Input (Fidgets / Weighted Items / Music)
The nervous system has limited bandwidth. Deep pressure, fidgets, and preferred music give the brain something else to process, diluting the dominance of baby crying.
Cognitive Framework (Social Stories / Visual Timer)
Understanding "babies cry → parent helps → baby stops" creates a narrative that contains the experience. The timer makes the abstract concrete and visible. Predictability is calming.
Positive Reconditioning (Special Activity)
Classical conditioning: if the child's experience shifts from "pure suffering" to "suffering + something I love," the emotional valence gradually changes. Over time, the anticipatory dread may soften into qualified acceptance.

BUILDING TOLERANCE
Building Tolerance: The Gradual Staircase
Core Progression Principles
- Maximum protection first. Start with ALL tools available. Reduce supports only as tolerance builds.
- 5 successful coping episodes before any change. Don't rush. 5 consecutive "I coped" before reducing any support.
- The child leads the reduction. If the child spontaneously removes ear defenders during crying, that's the signal.
- Different crying = different challenge. Brief whimpers are easier than sustained screaming. Nighttime is harder. Adjust expectations.
- Regression is normal. Bad days happen. Return to maximum protection without guilt.
Variation Ideas to Build Tolerance
- Different locations in the home (kitchen during feeding, living room during awake time)
- Different times of day — morning vs. evening energy levels differ significantly
- Different activities paired with coping — drawing, building, eating, watching
- Gradually reducing physical distance from crying baby while maintaining protection
- Brief periods without ear defenders during mild fussing only — never full crying — only when child is ready
Satiation Indicator: "When the child says 'The baby's crying again' with mild annoyance rather than desperate terror, your protocol is working."

REINFORCEMENT
Catch Them Coping. Celebrate Immediately.
Reinforcement must be delivered within 3 seconds of observed coping behavior. Immediate. Specific. Enthusiastic. Celebrate the ATTEMPT, not just the success — a child who reached for ear defenders but still cried is coping.

"You grabbed your ear helpers all by yourself!"
When: Child reaches for ear defenders independently.
"That's so smart. You knew exactly what to do."
"That's so smart. You knew exactly what to do."

"You went to your calm spot. I'm proud of you."
When: Child goes to calm space without being told.
"You knew exactly what to do. You went to your calm spot."
"You knew exactly what to do. You went to your calm spot."

"Look at you using your squeeze ball."
When: Child uses fidget during crying.
"That's you taking care of yourself."
"That's you taking care of yourself."

"You said the baby needs help. That's being a wonderful sibling."
When: Child shows empathy toward baby.
"That's understanding. That's love, even when it's hard."
"That's understanding. That's love, even when it's hard."
Do NOT praise the absence of emotion ("Good, you didn't even react"). This invalidates the sensory experience. Always praise the coping action — never the suppression of feeling.
COOL-DOWN PROTOCOL
When the Baby Stops: The Critical Reconnection
Acknowledge Immediately
Go to the older child. Make eye contact. "The baby stopped. You did it." Physical presence is more important than words. Sit with them. Touch their shoulder.
Remove Pressure (1–2 minutes)
Let the child remove ear defenders when ready — don't remove for them. Let them stay in the calm space as long as they need. If they're mid-activity, let them finish. "Take your time."
Reconnect (2–5 minutes)
This is the parent-older child time that crying episodes steal. Use it. Read together, go outside, give a hug. One-on-one attention restores the balance disrupted by baby care.
Normalize (Brief)
"Babies cry a lot when they're little. It gets easier as she grows. And you have your tools." Brief, reassuring, factual. No lectures.
Prepare for Next Episode
"She might cry again when she wakes up. Your ear helpers are on the hook. Your calm space is ready." Preparation reduces shock. Predictability is calming.
DATA CAPTURE
60-Second Post-Episode Tracker
Tracking reveals patterns invisible to daily experience, shows progress over time, provides data for professional consultations, and validates parent effort. Record after each significant crying episode.
Field | Options | |
Date/Time | [date] [morning / afternoon / evening / night] | |
Crying duration | <5 min / 5–15 min / 15–30 min / 30+ min | |
Crying intensity | 1-Fussing / 2-Moderate / 3-Intense / 4-Screaming | |
Tools used | ☐ Ear defenders ☐ Calm space ☐ White noise ☐ Headphones ☐ Fidgets ☐ Weighted item ☐ Timer ☐ Special activity ☐ None | |
Self-initiated? | Yes, child chose / Parent offered / Parent had to assist / Child refused tools | |
Child's distress level | 1-Calm/coped / 2-Mild upset but functional / 3-Significant distress no meltdown / 4-Full meltdown despite tools | |
Recovery time | <1 min / 1–5 min / 5–15 min / 15+ min | |
Notes | Anything notable — new behavior, regression, breakthrough, concern |
Data feeds into GPT-OS® EverydayTherapyProgramme™ for personalized recommendations and population-level learning that improves outcomes for all families. Available as downloadable PDF tracker or in-app tracker.
TROUBLESHOOTING
Seven Scenarios. Seven Solutions.
Scenario 1: Child refuses to wear ear defenders
Why: Tactile sensitivity on head/ears, unfamiliarity, or negative association.
Solution: Try different types. Introduce gradually. Let child decorate them. Model wearing them yourself. Try headphones with music instead. If all ear-based tools are rejected, emphasize distance (calm space) and competing input (fidgets, weighted items).
Solution: Try different types. Introduce gradually. Let child decorate them. Model wearing them yourself. Try headphones with music instead. If all ear-based tools are rejected, emphasize distance (calm space) and competing input (fidgets, weighted items).
Scenario 2: Fine at home, still melts down at night
Why: Nighttime crying cuts through silence, disrupts sleep, child is disoriented and fatigued.
Solution: White noise machine running all night. Ear defenders at bedside. Increase physical distance between bedrooms. Prepare child before bed: "If the baby cries tonight, your ear helpers are right here."
Solution: White noise machine running all night. Ear defenders at bedside. Increase physical distance between bedrooms. Prepare child before bed: "If the baby cries tonight, your ear helpers are right here."
Scenario 3: Two children in crisis — I can't help both
Why: One parent, two distressed children, competing needs — the fundamental challenge.
Solution: Pre-position ALL tools so the older child can self-help while parent attends to baby. Prioritize safety: if baby is safe, briefly help older child equip (10 seconds) then attend to baby. Tag-team with partner when available. Accept imperfection.
Solution: Pre-position ALL tools so the older child can self-help while parent attends to baby. Prioritize safety: if baby is safe, briefly help older child equip (10 seconds) then attend to baby. Tag-team with partner when available. Accept imperfection.
Scenario 4: Child says "I hate the baby" or "Give the baby back"
Why: The child is expressing sensory suffering, not genuine hatred.
Solution: Validate: "The sounds are really hard for you. I understand." Do NOT lecture about loving siblings. Increase positive sibling interaction during QUIET times. Over time, as coping improves, the negative association weakens.
Solution: Validate: "The sounds are really hard for you. I understand." Do NOT lecture about loving siblings. Increase positive sibling interaction during QUIET times. Over time, as coping improves, the negative association weakens.
Scenario 5: Child hits the baby or themselves during episodes
Why: Fight response when overwhelmed with no available escape. This is a RED LINE situation.
Solution: Immediate safety protocol. Never leave children unsupervised during crying. Physical barriers. Seek professional behavioral support. This signals current tools are insufficient — not that the child is "bad."
Solution: Immediate safety protocol. Never leave children unsupervised during crying. Physical barriers. Seek professional behavioral support. This signals current tools are insufficient — not that the child is "bad."
Scenario 6: Getting easier, then suddenly worse again
Why: Regression triggered by illness, fatigue, developmental growth spurt, teething spike, or routine change.
Solution: Return to maximum protection. Identify trigger if possible. Tolerance will return to previous level, usually faster than the first time. "You've done this before. Your tools still work."
Solution: Return to maximum protection. Identify trigger if possible. Tolerance will return to previous level, usually faster than the first time. "You've done this before. Your tools still work."
Scenario 7: I'm exhausted. I can't keep doing this.
Why: Caregiver burnout from managing two dysregulated children simultaneously is real, expected, and not a failure.
Solution: Seek support. One hour per day of someone else holding the baby can break the cycle. Connect with parent community. Book a teleconsult. Babies cry less as they age. Your exhaustion is valid. It will get easier.
Solution: Seek support. One hour per day of someone else holding the baby can break the cycle. Connect with parent community. Book a teleconsult. Babies cry less as they age. Your exhaustion is valid. It will get easier.
Fallback Principle: If nothing resolves within 2–3 weeks of consistent effort, this is your signal to seek professional support. Not because you failed — because this child needs more than home strategies alone can provide.
ADAPTATION
One Protocol. Infinite Versions. Matched to Your Child.
◀ Easier (Start Here If Needed)
Use ALL tools simultaneously — maximum protection stack. Older child in calm space with door closed. Ear defenders + headphones + weighted blanket + special activity. No expectation to tolerate ANY crying without full protection.
■ Standard (Protocol As Written)
Tools accessible, child self-selects. Child remains in home — not necessarily same room — during crying. Uses 2–3 tools per episode. Gradually building tolerance over weeks.
Harder ▶ (Only When Child Leads)
Reduced tool use — child chooses whether to use ear defenders. Remains in same room during mild fussing. Brief exposure to crying without any tools — only if child is willing and regulated. Child participates in baby care.
Ages 2–3
- All tools parent-directed
- Simpler social story — 3–4 sentences with pictures
- Ear defenders introduced as a game during quiet times
- May need parent present in calm space
- Extra physical comfort: holding, carrying, weighted items
Ages 4–6
- Child begins to self-select tools with prompting
- Can understand visual timer concept
- Can choose items for calm space
- Verbal scripts: "I need my ear helpers"
Ages 7–12
- Child co-creates the protocol
- Understands the neuroscience: "Your brain turns the volume up"
- Self-manages timer, headphones, and calm space independently
- May prefer discreet earbuds over visible ear defenders
- Can learn about their own sensory profile
Sensory Profile Variations
- Auditory-Only: Ear protection is primary; other tools supplementary
- Multi-Sensory: Add dim lighting and soft textures to calm space
- Anxiety-Dominant: Add breathing techniques and professional anxiety support
- Empathy-Dominant: Social stories and safe-distance soothing involvement are especially important

PROGRESS: WEEKS 1–2
Weeks 1–2: Building the Foundation
15%
Foundation Phase
Tools introduced, familiarity building, first use emerging
What Real Progress Looks Like
- Child accepts ear defenders during calm times — tries them on, keeps them briefly
- Child has visited the calm space at least once during a non-crisis moment
- Social story has been read 3+ times during quiet periods
- At least one crying episode where child used ANY tool, even briefly
- White noise machine running in child's room at night
- Parent has tools accessible in 2+ locations
- Child knows where the ear defenders are and can reach them
What Is NOT Yet Expected
- Child calmly coping through entire crying episode
- Child remaining in same room as crying baby
- Reduced meltdown intensity
- Improved sleep — nighttime tolerance takes longer
"These two weeks may feel like nothing is changing. You are positioning materials, building familiarity, establishing routine. Neural pathways are forming beneath the surface. The tools need to become familiar before they become functional. Trust the process."
PROGRESS: WEEKS 3–4
Weeks 3–4: The Tools Start Working
40%
Consolidation Phase
Independent tool use emerging, distress reducing, recovery faster
Indicators of Consolidation
- Child reaches for ear defenders independently when crying starts — not prompted
- Goes to calm space on own initiative at least some of the time
- Distress intensity during protected episodes is reduced (from 4/4 to 2–3/4)
- Recovery time after crying episodes is shorter
- Anticipatory anxiety may be reducing — less tensing when baby fusses
🌟 Spontaneous Celebration Moments
- Child says "I need my ear helpers" — self-advocacy!
- Child walks to calm space while saying "I'm going to my spot"
- Child watches timer and comments "Almost done"
- Child references social story: "The baby needs help. She'll stop."
- Child touches or looks at the baby during quiet moments
When to Increase Challenge
Only after 5+ consecutive successfully coped episodes at current level. If in doubt, maintain current support. There is no deadline. The child's readiness is the only clock that matters.

PROGRESS: WEEKS 5–8
Weeks 5–8: From Coping to Living
75%
Emerging Mastery
Functional family life with manageable coping — the achievable, realistic goal
Mastery Criteria
- Child copes through most crying episodes using 1–2 tools (down from all tools)
- Can remain in the same general area as baby during moderate crying with ear defenders
- Distress level typically 1–2/4 during protected episodes
- Recovery time under 2 minutes for most episodes
- Self-initiates tool use without prompting in 80%+ of episodes
- Spontaneous positive sibling interaction increasing — holding, reading to, watching baby
- Can attend family gatherings where babies may cry (with tools in bag)
What Mastery IS and IS NOT
Mastery IS: Functional family life with manageable coping. The child has tools, knows how to use them, uses them independently, and can coexist with a crying sibling. Not zero distress — manageable distress.
Mastery IS NOT: The child loves baby crying. The child never needs ear defenders. The child can tolerate screaming at close range indefinitely. These are unrealistic goals.
Generalization Indicators
- Other sound sensitivities may be improving alongside
- Coping skills transferring to other challenging situations
- Overall family stress decreasing measurably
CELEBRATION
You Did This. Your Commitment Built This.
Before
"Make it stop! Please make it stop!" Running from the room in terror. Cannot be in the same house as crying. "Can we give the baby back?" Home as a crisis zone. Parent failing both children.
After
"I'm getting my ear helpers." Walking to the calm space with purpose. Can be in the same room with tools. Holding the baby. Reading to the baby. Home as home again. Parent supporting both children with a system.
What the Child Gained
Self-advocacy. Self-regulation tools. Agency over their sensory experience. A relationship with their sibling that isn't defined by suffering. The knowledge that hard things can be managed with the right tools.
What the Parent Gained
A system that works. Proof that their child's distress was neurological, not behavioral. Tools that free them to attend to the baby. A family that functions. Breathing room.
Celebrate: Take a photo of the child wearing ear defenders and playing near the baby. It's evidence of transformation. Share it (Card 37) — another parent needs to hear that this gets better.
RED FLAGS
Watch for These. Act Immediately.
🚩 Red Flag 1: Fear Spreading, Not Shrinking
Child now fears the baby at ALL times — won't be near even when calm, fears baby-related objects.
Action: Pause all exposure. Consult OT and child psychologist. Possible phobia component developing.
Action: Pause all exposure. Consult OT and child psychologist. Possible phobia component developing.
🚩 Red Flag 2: Nighttime Worsening
Nightmares about crying, refusing to sleep, new bedwetting, requiring parent for sleep onset — and getting worse despite supports.
Action: Reduce daytime exposure intensity. Maximize nighttime sound insulation. Consult pediatrician.
Action: Reduce daytime exposure intensity. Maximize nighttime sound insulation. Consult pediatrician.
🚩 Red Flag 3: Self-Injury Escalating
Hitting self, banging head, biting, pulling hair — increasing in frequency or severity during episodes.
Action: Immediate professional intervention. OT + behavioral specialist. Current tools are insufficient.
Action: Immediate professional intervention. OT + behavioral specialist. Current tools are insufficient.
🚩 Red Flag 4: Aggression Toward Baby
Child has attempted to hit, push, cover, or harm the baby during or after crying episodes.
Action: IMMEDIATE safety protocol. Never leave children unsupervised. Physical barriers during all crying. Professional behavioral support urgently.
Action: IMMEDIATE safety protocol. Never leave children unsupervised. Physical barriers during all crying. Professional behavioral support urgently.
🚩 Red Flag 5: Complete Regression
After weeks of progress, child returns to Week 1 levels with no identifiable trigger, persisting 2+ weeks.
Action: Return to maximum protection. If no identifiable trigger, consult OT.
Action: Return to maximum protection. If no identifiable trigger, consult OT.
🚩 Red Flag 6: Parent Burnout
Crying daily, losing your temper, unable to respond to either child, feeling hopeless.
Action: Seek support immediately. One hour of help per day can break the cycle. Your mental health is foundational to both children's wellbeing. Call: 9100 181 181.
Action: Seek support immediately. One hour of help per day can break the cycle. Your mental health is foundational to both children's wellbeing. Call: 9100 181 181.
Escalation Pathway: Self-resolve with tools (Cards 13–22) → Teleconsult → Clinic visit → Comprehensive evaluation

PROGRESSION PATHWAY
Where This Technique Sits in Your Child's Journey
Prerequisites
- General awareness of child's sensory sensitivities
- Understanding that the reaction is neurological, not behavioral
- Willingness to invest in tools and environmental modification
Branch A — Other Household Sounds
A-042: Vacuum Cleaner Fear · A-043: Blender and Kitchen Sounds · A-037: Sensitivity to Sudden Sounds. Same tools, different triggers — your materials transfer.
Branch B — Deeper Auditory Work
Therapeutic Listening Program · Comprehensive Auditory Processing Evaluation · Auditory Integration Therapy (professional-guided)
Branch C — Anxiety Dominant
CBT for specific sound anxiety · Parent-Child Interaction Therapy · Systematic desensitization with professional guidance
Branch D — Family Systems
Sibling adjustment counseling · Family therapy · Parent stress management — for when impact on family functioning is severe and persistent despite sensory tools
Long-Term Goal
Functional family integration — the child coexists with a sibling, participates in family life, has tools for auditory challenges, and the family system is healthy.

FAMILY STORIES
From Two Children in Crisis to a Family Again
Parent, Pinnacle Network
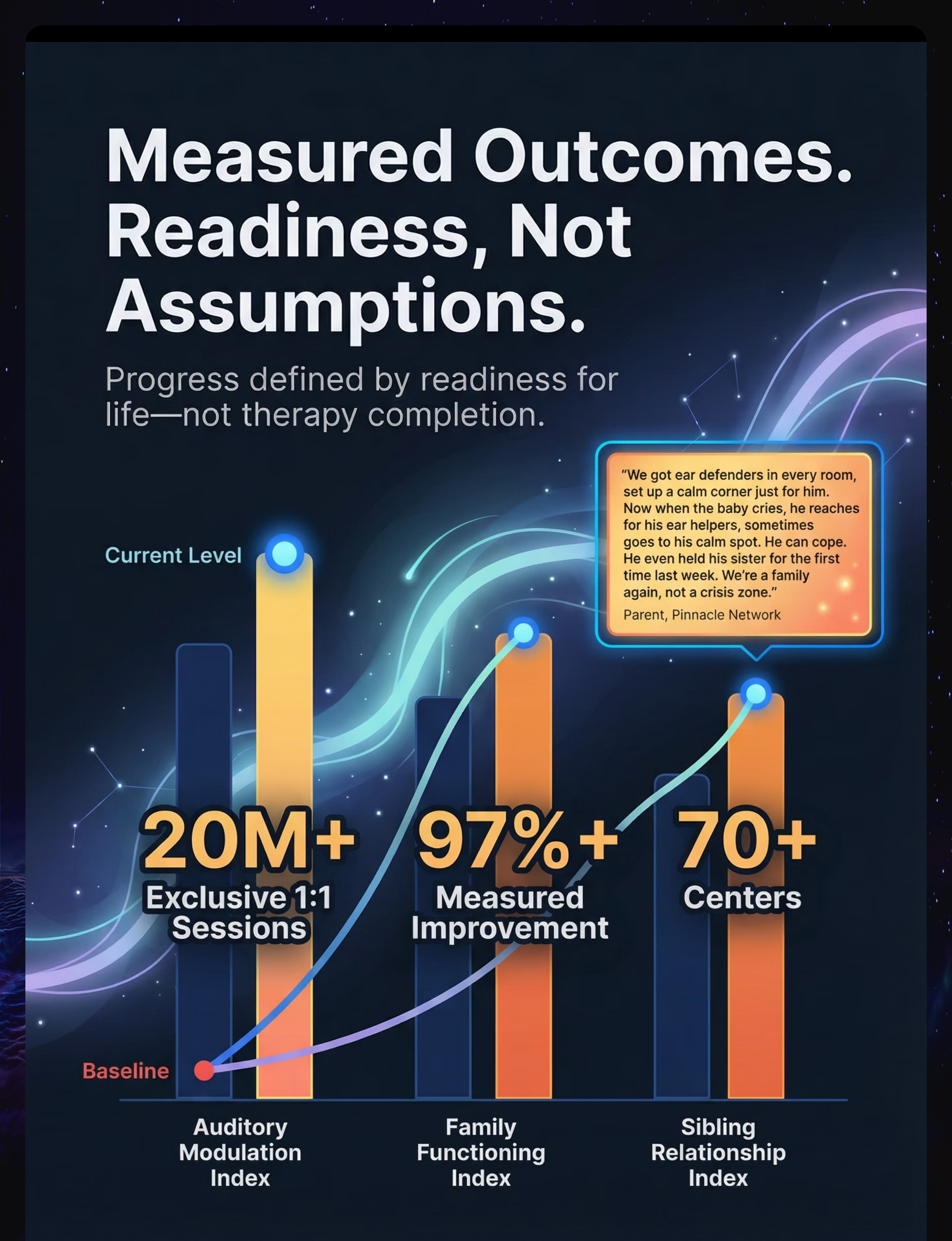
"When my daughter was born, my 4-year-old son started screaming every time she cried. He asked me, 'Why did you bring her here?' It broke my heart. Our OT explained his auditory system was genuinely overwhelmed — not jealousy. We got ear defenders for every room and wrote a simple story about why babies cry. By week three, he was putting them on himself. By week six, he stayed in the same room while I fed the baby. Last month — he held her for the first time while wearing his ear defenders. He said, 'She's actually kind of soft.' We're a family now. A real family."
Parent, Pinnacle Network (ASD, Age 7)
"Twelve weeks of screaming, no sleep, hitting his head against the wall. Our BCBA helped us set up a special activity station — his favorite tablet shows are ONLY available when the baby cried. Within days, he'd hear the baby and say 'Is it iPad time?' It didn't fix the sound — he still doesn't love it — but he could cope. And coping is everything."
"Auditory over-responsivity to infant crying is one of the most stressful presentations for families — constant, inescapable, and involving two children needing simultaneous care. Once families shift from 'behavioral problem' to 'sensory support,' outcomes improve rapidly. Multi-material approaches — especially the combination of auditory protection and positive association — show the strongest results in our clinical data." — Pinnacle Blooms Senior OT, Sensory Integration Specialist

FREQUENTLY ASKED QUESTIONS
Your Questions, Answered
Will my child always need ear defenders when the baby cries?
Not necessarily. Ear defenders are a bridge to tolerance. As the child's auditory system matures and coping skills strengthen, many children naturally reduce their reliance on protection. Some continue using them selectively — and that's fine. A child who uses tools is a child who copes.
How long until this gets better?
Most families see initial improvement within 2–4 weeks of consistent use. Significant tolerance gains emerge at 4–8 weeks. Full functional integration may take 2–6 months. Babies also cry less as they age, which compounds improvement.
Is this sibling rivalry or sensory?
It can be both. Key signs this is primarily sensory: child reacts immediately to the SOUND (not to parent attention), shows physical distress (body tension, fight-or-flight), is calm when the baby is quiet. Address both components if you see both.
My child won't wear anything on their head. Now what?
Try headband-style protectors, in-ear earplugs (older children), cotton balls, or simply hands over ears. Shift emphasis to distance (calm space), white noise, and positive association. Not all children use ear defenders — the protocol still works.
Does this mean my child is autistic?
Auditory over-responsivity occurs in children with and without autism. It is one data point, not a diagnosis. If you have broader developmental concerns, a comprehensive evaluation is warranted. Either way, the tools help.
Will this affect their sibling relationship long-term?
Most sibling relationships recover fully — especially when the sensory need is addressed early. Children given tools to cope develop positive associations with the sibling during quiet times. Address the sensory need. The relationship follows.
Didn't find your answer? → Ask GPT-OS® · Book a Teleconsultation · Call FREE: 9100 181 181 — 16+ languages, 24/7
Preview of 9 materials that help when baby crying overwhelms Therapy Material
Below is a visual preview of 9 materials that help when baby crying overwhelms therapy material. The pages shown help educators, therapists, and caregivers understand the structure and content of the resource before use. Materials should be used under appropriate professional guidance.











Link copied!

THE PINNACLE PROMISE
"From Fear to Mastery. One Technique at a Time."
You arrived wondering how to survive the next time the baby cries. You now have 9 materials, a complete protocol, tracking tools, troubleshooting for every scenario, a community of parents who've walked this path, professional support on call, and the knowledge — backed by systematic reviews, meta-analyses, and 21 million therapy sessions — that this works. Your older child's distress is real. Your exhaustion is valid. And your family can coexist. Not someday. Starting today.
Your Next Step
FREE National Autism Helpline: ☎ 9100 181 181
16+ languages · 24/7 availability
16+ languages · 24/7 availability
Medical Disclaimer
This content is educational and informational. It does not replace assessment by a licensed occupational therapist, healthcare provider, or developmental specialist. Severe or persistent auditory sensitivity may require comprehensive sensory processing evaluation and professional intervention. If distress includes self-injury, seek professional support immediately.
Individual results may vary. Statistics represent aggregate outcomes across the Pinnacle Blooms Network.
© 2026 Pinnacle Blooms Network®, unit of Bharath Healthcare Laboratories Pvt. Ltd.
CIN: U74999TG2016PTC113063 · DPIIT DIPP8651 · GSTIN 36AAGCB9722P1Z2
CIN: U74999TG2016PTC113063 · DPIIT DIPP8651 · GSTIN 36AAGCB9722P1Z2