
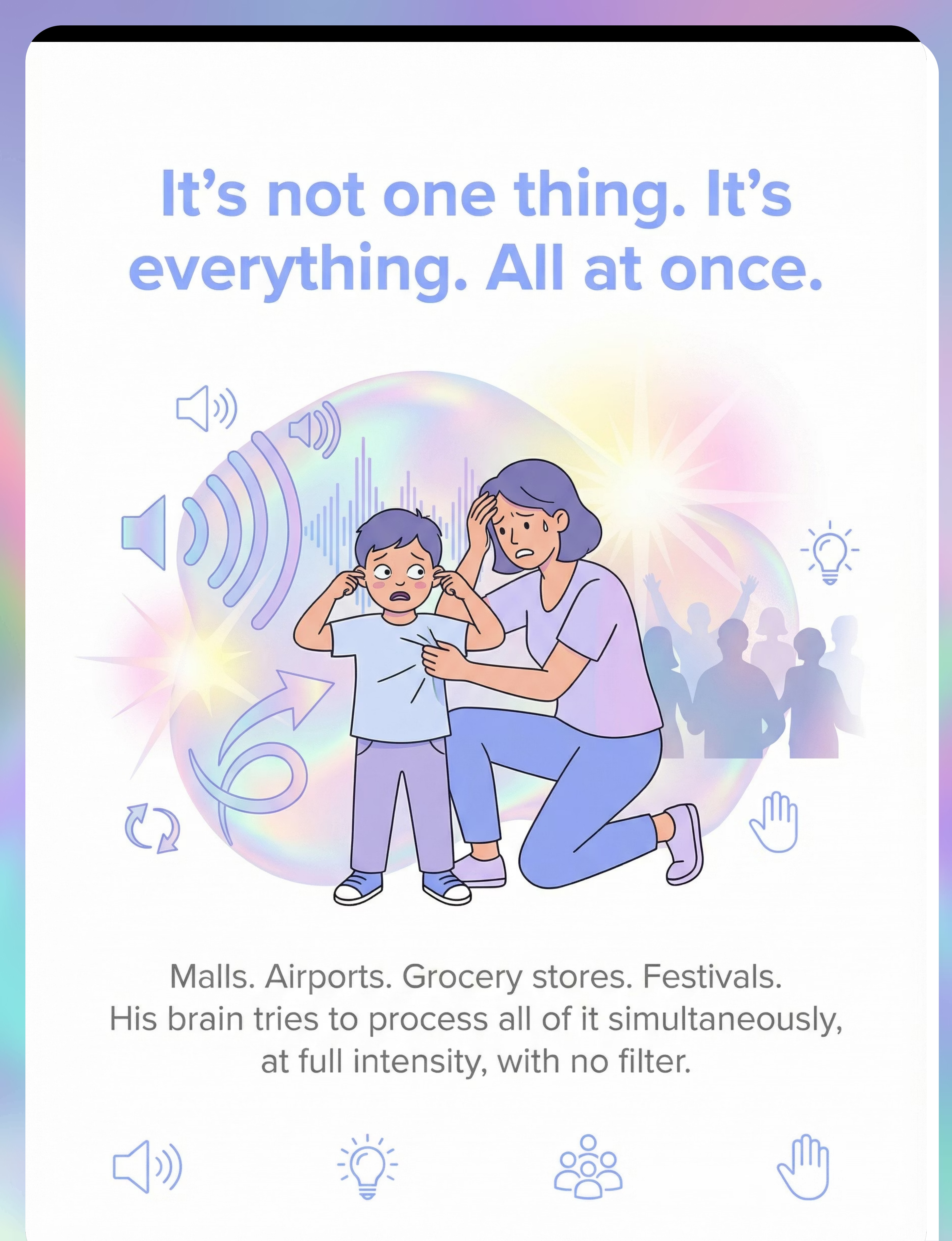
"We've Stopped Going Places. Our World Keeps Getting Smaller."
Malls. Airports. Grocery stores. Festivals. Even a cousin's birthday party. The noise hits like a wall — announcements layering over music layering over conversations layering over carts rattling. The lights are too bright, too much, everywhere. You watch it happen: the eyes darting, the hands over ears, the grabbing your hand too tight. Then shutdown — or meltdown. People say "he needs to get used to it." They don't understand: his brain is processing everything at maximum volume, all at once, with no filter.
You are not failing. Your child's nervous system is speaking. And there are 9 materials that can help you both go places again.
Pinnacle Blooms Consortium — OT • SLP • ABA • SpEd • NeuroDev
Sensory Solutions Series — Episode 39
Age: 2–12 years

You Are Not Alone — The Numbers
Every family that has abandoned a shopping cart, left a restaurant before the food arrived, or watched their child curl into a ball at a festival — you are among millions navigating this exact challenge. Multi-sensory overload in complex environments is one of the most commonly reported challenges across the global autism community. This is not rare. This is not unusual. This is not a failure of parenting. This is neurology — and neurology responds to the right interventions.
80%+
Children with Autism
Experience sensory processing difficulties (PRISMA Systematic Review, 2024 — PMC11506176)
69–95%
ASD Hyper-Sensitivity
Of individuals with ASD report hyper-sensitivity to environmental sensory stimuli — auditory and visual channels most affected (World J Clin Cases, 2024)
1 in 36
Children Identified with ASD
In the US (CDC, 2023). In India, an estimated 18 million+ children on the spectrum face crowded-environment challenges daily.
"You are among millions of families navigating this exact challenge. The science is clear. The solutions exist."

What's Happening in Your Child's Brain
The Brain Under Sensory Overload
In a crowded environment, sensory input floods through multiple channels simultaneously: the Auditory Cortex receives hundreds of sounds at once; the Visual Cortex tracks movement, light, and color; the Somatosensory Cortex registers every touch and bump; and the Amygdala flags threat after threat.
The critical structure is the Thalamus — the brain's relay station and gating mechanism. In a typical brain, it sorts "important" from "background." In your child's brain, this filter is calibrated differently: it processes EVERYTHING at high priority, all channels, all at once, all at maximum intensity.
The Neuroscience — In Your Words
In a crowded mall, a typical thalamus lets through the announcement that your flight is boarding, while filtering out the 200 conversations, the refrigerator hum, the fluorescent flicker, and the child crying three gates away. Your child's thalamus does not filter. There is no "background." Everything is foreground.
This isn't a behavior choice. This is a wiring difference. The technical term is Sensory Modulation Disorder — specifically, multi-sensory over-responsivity. The meltdowns and shutdowns you see are not tantrums. They are the nervous system's emergency response when processing capacity is exceeded. Like a circuit breaker tripping.
"This is neurology, not behavior. And neurology responds to intervention."

Where This Sits in Development
Multi-sensory environmental overwhelm emerges and evolves at different stages of childhood. Understanding where your child sits on this timeline helps calibrate expectations — and clarifies why now is exactly the right time to intervene.
0–24 Months
Emerging sensory responses. Early sensitivity signs may appear. First crowded outings reveal difficulties.
2–4 Years ★ Critical Window
Most families first identify crowded-environment overwhelm. The world "gets bigger" — preschool, outings, shopping, travel — and the child's system is tested.
4–7 Years
Without intervention, avoidance patterns solidify. With intervention, the tolerance-building window is optimal.
7–12 Years
Social implications increase — birthday parties, school trips, family events. Intervention expands community access significantly.
Multi-sensory environmental overwhelm commonly co-occurs with auditory sensitivity, visual over-responsivity, tactile defensiveness, anxiety, and transition difficulties. Addressing the environment as a whole — not one channel at a time — is critical.
The Evidence Behind This Technique
Evidence Grade: Level I–II — Systematic Reviews + RCTs
The materials and strategies on this page are grounded in three converging, peer-reviewed evidence streams — validated by clinicians who have delivered 20 million+ therapy sessions.
Stream 1 — Sensory Integration Therapy
PRISMA Systematic Review (2024): 16 articles from 2013–2023 confirm sensory integration interventions meet criteria as evidence-based practice for ASD. Improvements documented across sensory processing, adaptive behavior, social skills, and motor function. Reference: PMC11506176
Stream 2 — Home-Based Sensory Intervention
Indian Journal of Pediatrics RCT (Padmanabha et al., 2019): Home-based sensory interventions administered by trained parents demonstrated significant outcomes, establishing safety and efficacy for parent-delivered strategies. Reference: DOI: 10.1007/s12098-018-2747-4
Stream 3 — Environmental Modification
AOTA guidelines and sensory modulation research (Miller, Dunn) establish that environmental modification — reducing sensory load through protective tools and strategic planning — enables functional participation. Meta-analysis of 24 studies (PMC10955541) confirms improvements across all key domains.
"Clinically validated. Home-applicable. Parent-proven."

The Technique — What It Is
Formal Name
Multi-Sensory Environmental Protection Protocol
Parent-Friendly Name
"The Outing Survival Kit — 9 Materials That Help in Crowded, Noisy Places"
Age Range
2–12 years
Setting
Community environments — every outing
Definition
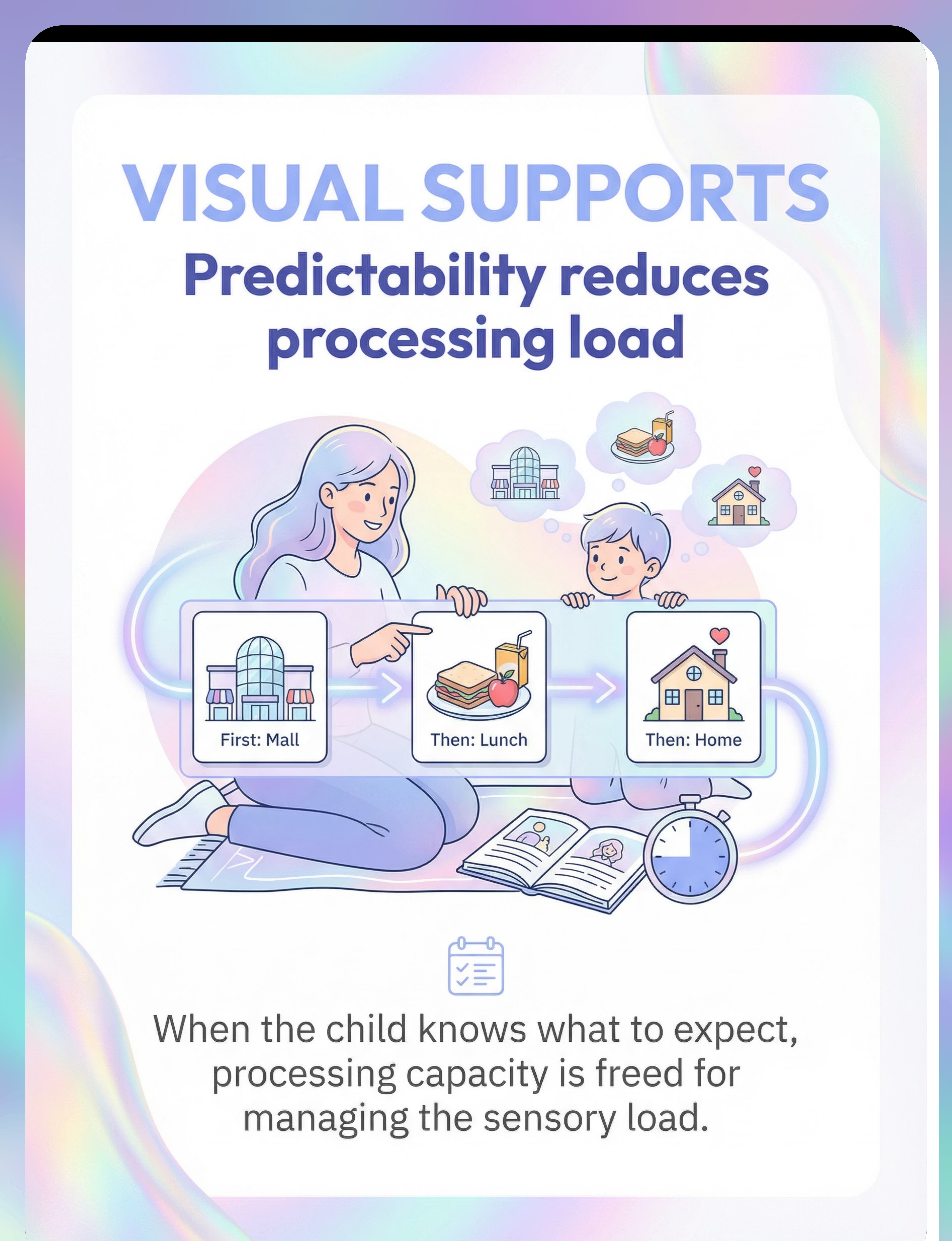
A structured, multi-material sensory protection and regulation strategy designed to reduce environmental sensory load across auditory, visual, tactile, proprioceptive, and oral channels simultaneously — enabling children with sensory over-responsivity to access and participate in crowded, noisy community environments that would otherwise be overwhelming or impossible.
The protocol combines sensory protection tools (headphones, glasses, weighted wearables), emotional anchoring (comfort objects, visual supports), environmental engineering (escape routes, timing, safe bases), and self-regulation supports (oral sensory tools) into a customizable "outing kit" that travels with the child and family.
Domain: Sensory Processing (A)
Sub-Domain: Multi-Sensory Overload / Environmental Overwhelm
Canon Categories: Sensory Regulation, Visual Supports, Oral Motor Tools

Who Uses This Technique
Crowded environments challenge EVERYTHING at once — and the response must be equally integrated. This technique crosses therapy boundaries because the brain doesn't organize by therapy type.
Occupational Therapist (Primary Lead)
OTs design the comprehensive sensory profile, identify specific channel sensitivities, recommend appropriate protection levels, create individualized sensory diets, and train parents in graded exposure protocols. The OT is the architect of the environmental protection plan.
Speech-Language Pathologist
SLPs address communication strategies for overwhelming environments — teaching the child to signal distress ("too loud," "need break"), use communication boards in community settings, and maintain social communication skills despite sensory load.
Board Certified Behavior Analyst (BCBA)
BCBAs develop behavior support plans for community outings, create reinforcement schedules for tolerance-building, analyze function of meltdown behaviors, and design data collection systems to track progress across environments.
Special Educator
SpEds prepare the child for community experiences through social stories, visual schedules, and generalization of coping strategies across settings, bridging therapy goals to real-world functioning.
Neurodevelopmental Pediatrician
NeuroDev physicians evaluate whether sensory over-responsivity is part of a broader neurodevelopmental profile, assess for co-occurring conditions, and determine if pharmacological support is warranted alongside behavioral strategies.
What This Technique Targets
🎯 Primary Target
Multi-sensory modulation in complex environments. Observable: tolerates crowded places for increasing durations; uses protection tools independently; signals distress before meltdown threshold.
🎯 Secondary Targets
Community participation, self-regulation, communication under stress, and transition tolerance between sensory environments with reduced distress.
🎯 Tertiary (Long-Term)
Environmental adaptability, social participation in birthday parties and school outings, progressive independence, and full family quality of life restored.

What You Need — The 9 Materials Overview
The Multi-Sensory Environmental Protection Kit combines sensory protection, emotional anchoring, and environmental engineering into one portable, customizable system. Below are all 9 materials — each targeting a specific sensory channel or coping mechanism.
1. Noise-Reducing Headphones / Ear Defenders
Canon: #003 — Sensory Regulation Tools | ₹1,500–8,000
Options: Active noise-canceling (kid-sized), passive ear defenders, Loop earplugs for older children.
Options: Active noise-canceling (kid-sized), passive ear defenders, Loop earplugs for older children.
2. Tinted Glasses / Sunglasses
Canon: #005 — Sensory Regulation Tools | ₹500–3,000
Options: Child-sized sunglasses, FL-41 tinted lenses for fluorescent sensitivity, wraparound styles.
Options: Child-sized sunglasses, FL-41 tinted lenses for fluorescent sensitivity, wraparound styles.
3. Weighted Wearable
Canon: #001 + #002 — Sensory Regulation Tools | ₹1,500–5,000
Options: Weighted vest, weighted lap pad, compression vest/shirt, compression athletic wear.
Options: Weighted vest, weighted lap pad, compression vest/shirt, compression athletic wear.
4. Portable Comfort Object / Sensory Toy
Canon: #060 + #004 — Behavioral + Sensory Regulation | ₹200–1,500
Options: Child's existing comfort item, quiet fidgets, squishy/stress ball, textured toys, therapy putty.
Options: Child's existing comfort item, quiet fidgets, squishy/stress ball, textured toys, therapy putty.
5. Visual Supports
Canon: #014 — Visual Supports & Scheduling | ₹0–500
Options: Laminated visual schedule cards, social stories, visual timer, first-then board.
Options: Laminated visual schedule cards, social stories, visual timer, first-then board.

Materials 6–9 + Zero-Cost Alternatives
"Not every family can order from Amazon. Not every village has same-day delivery. Every parent, regardless of economic status, can protect their child in crowded environments TODAY."
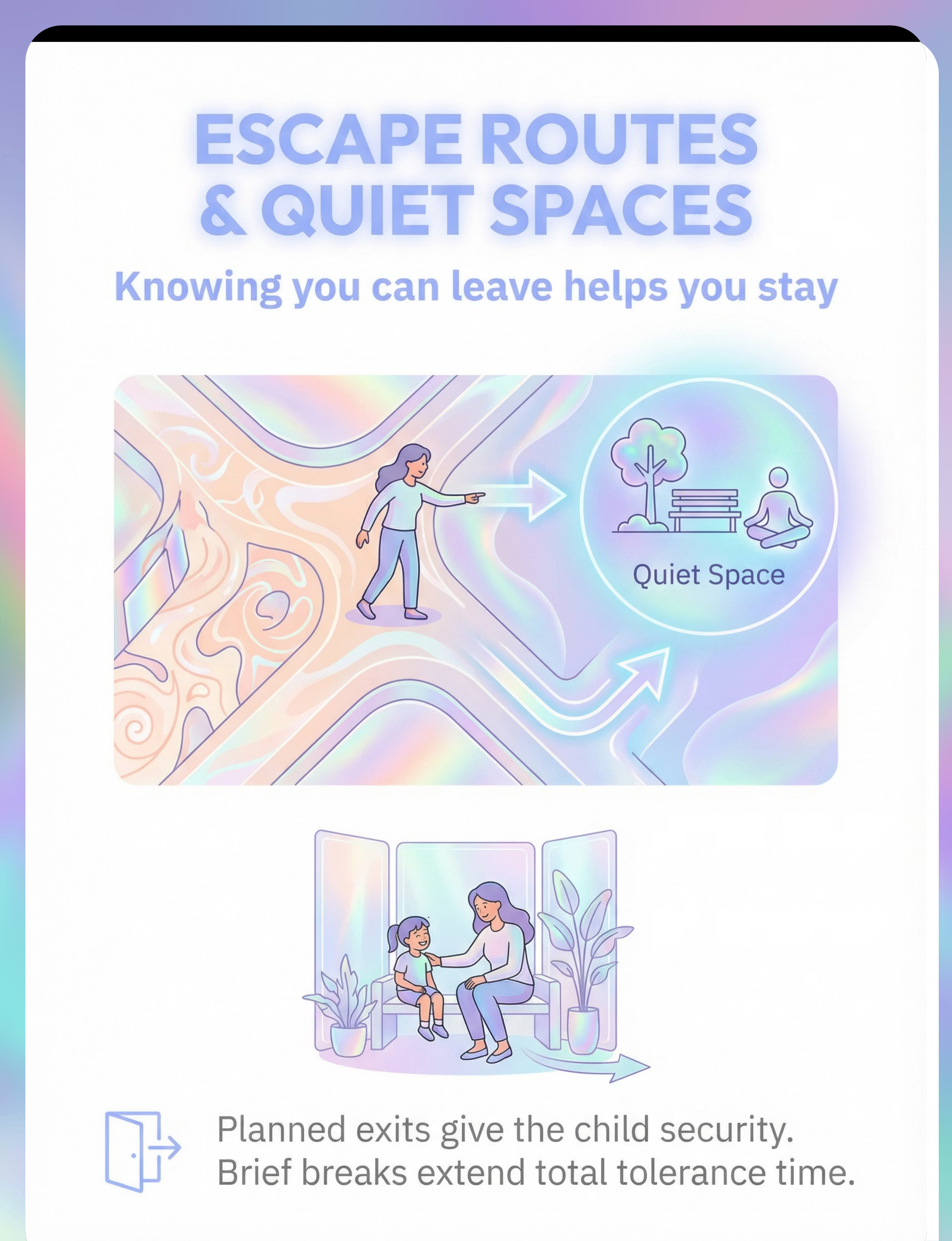
6. Planned Escape Routes & Quiet Spaces
Price: ₹0 (Strategy, not product)
Walk the venue before bringing the child. Identify family restrooms, quiet corners, and the car. Take photos to show the child: "If you need a break, we go here."
Walk the venue before bringing the child. Identify family restrooms, quiet corners, and the car. Take photos to show the child: "If you need a break, we go here."
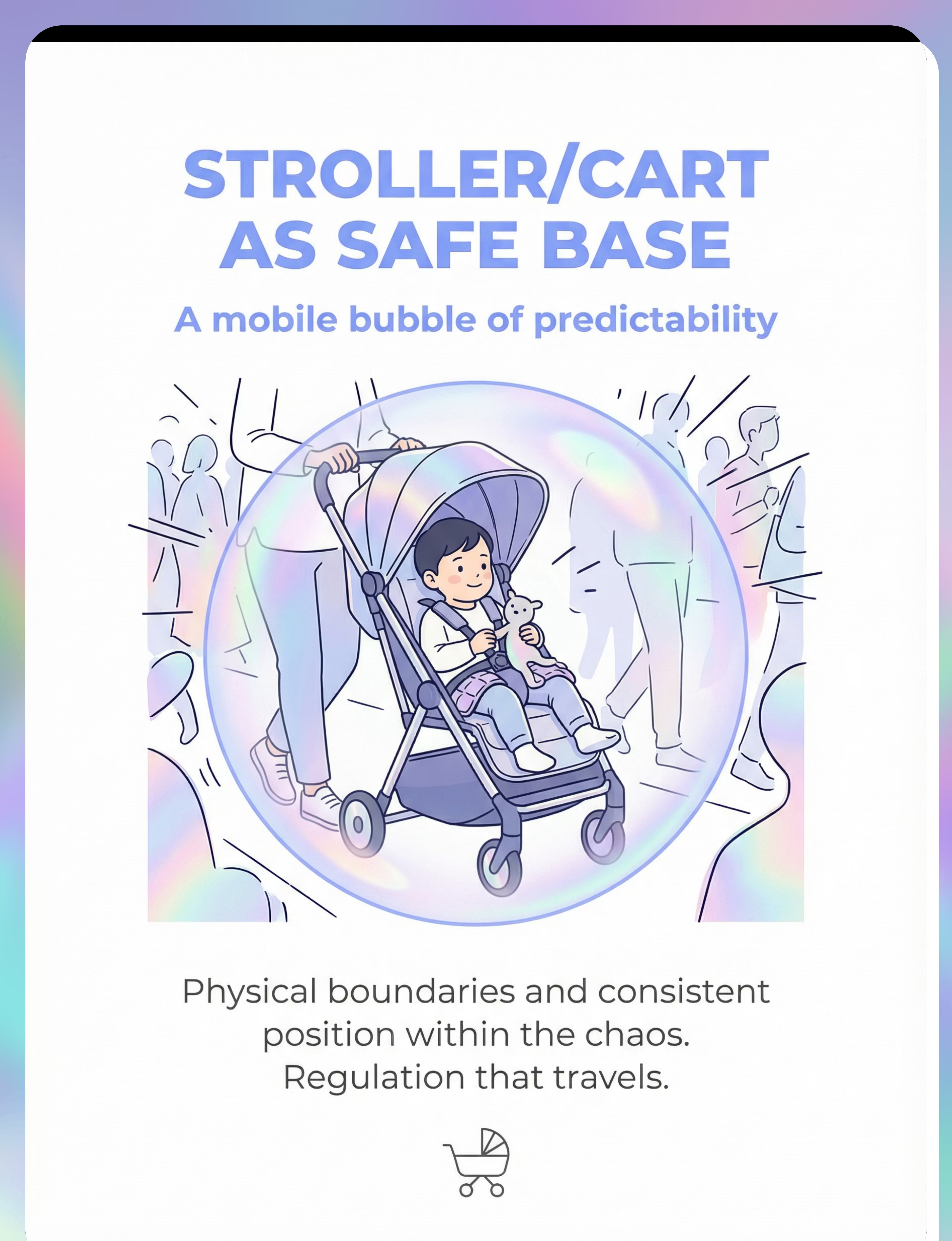
7. Stroller / Cart as Safe Base
Price: ₹0 (using existing stroller) – ₹5,000+ for accessories. Best for ages 2–5.
Add a canopy for visual reduction, a weighted lap pad, familiar blanket, and snack/fidget storage to any existing stroller.
Add a canopy for visual reduction, a weighted lap pad, familiar blanket, and snack/fidget storage to any existing stroller.
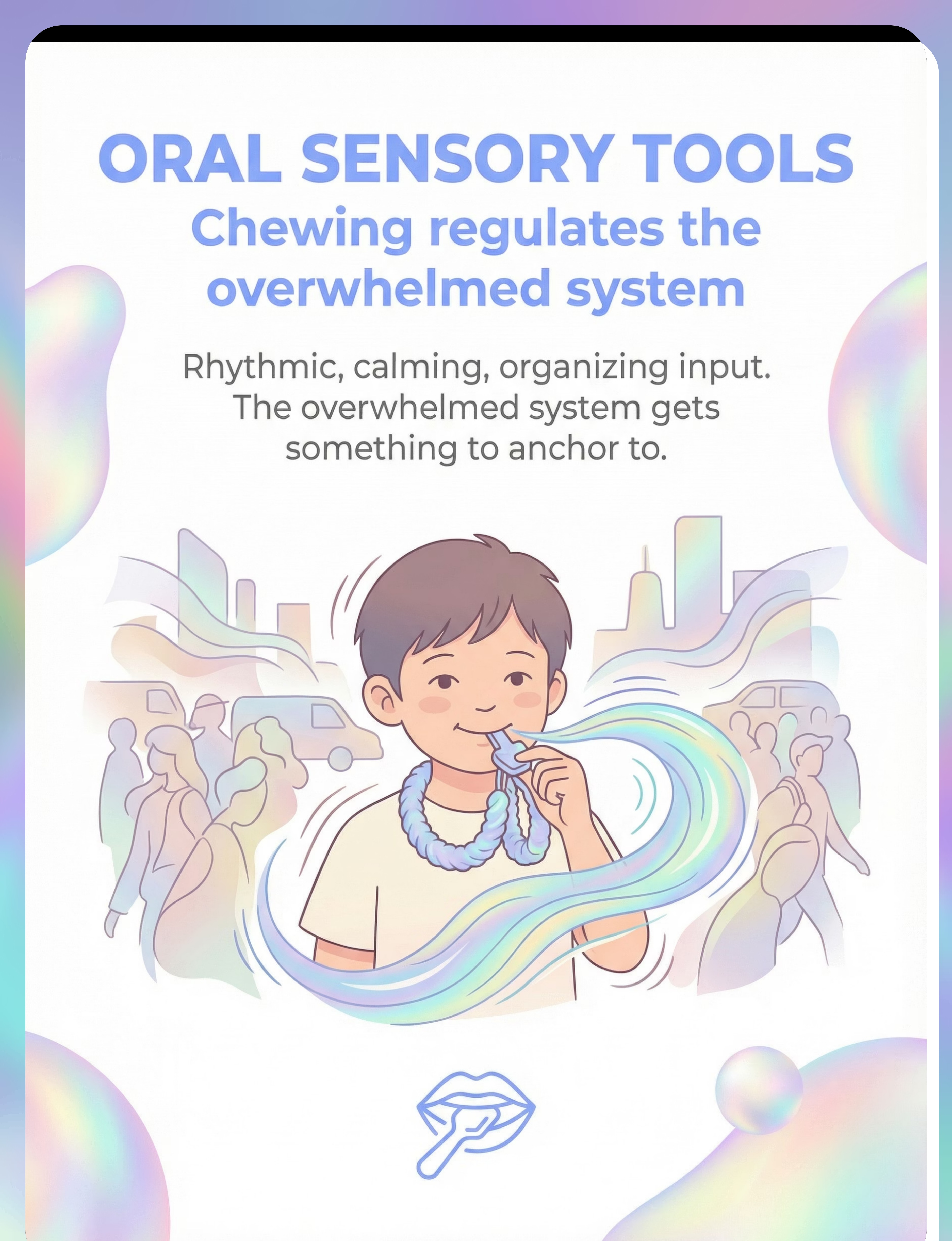
8. Chewy / Oral Sensory Tools
Canon: #041 — Oral Motor Tools | ₹300–1,500
Options: Chewable jewelry (necklace, bracelet), silicone chew tubes, crunchy/chewy snacks. Same oral sensory input, zero cost when using food alternatives.
Options: Chewable jewelry (necklace, bracelet), silicone chew tubes, crunchy/chewy snacks. Same oral sensory input, zero cost when using food alternatives.
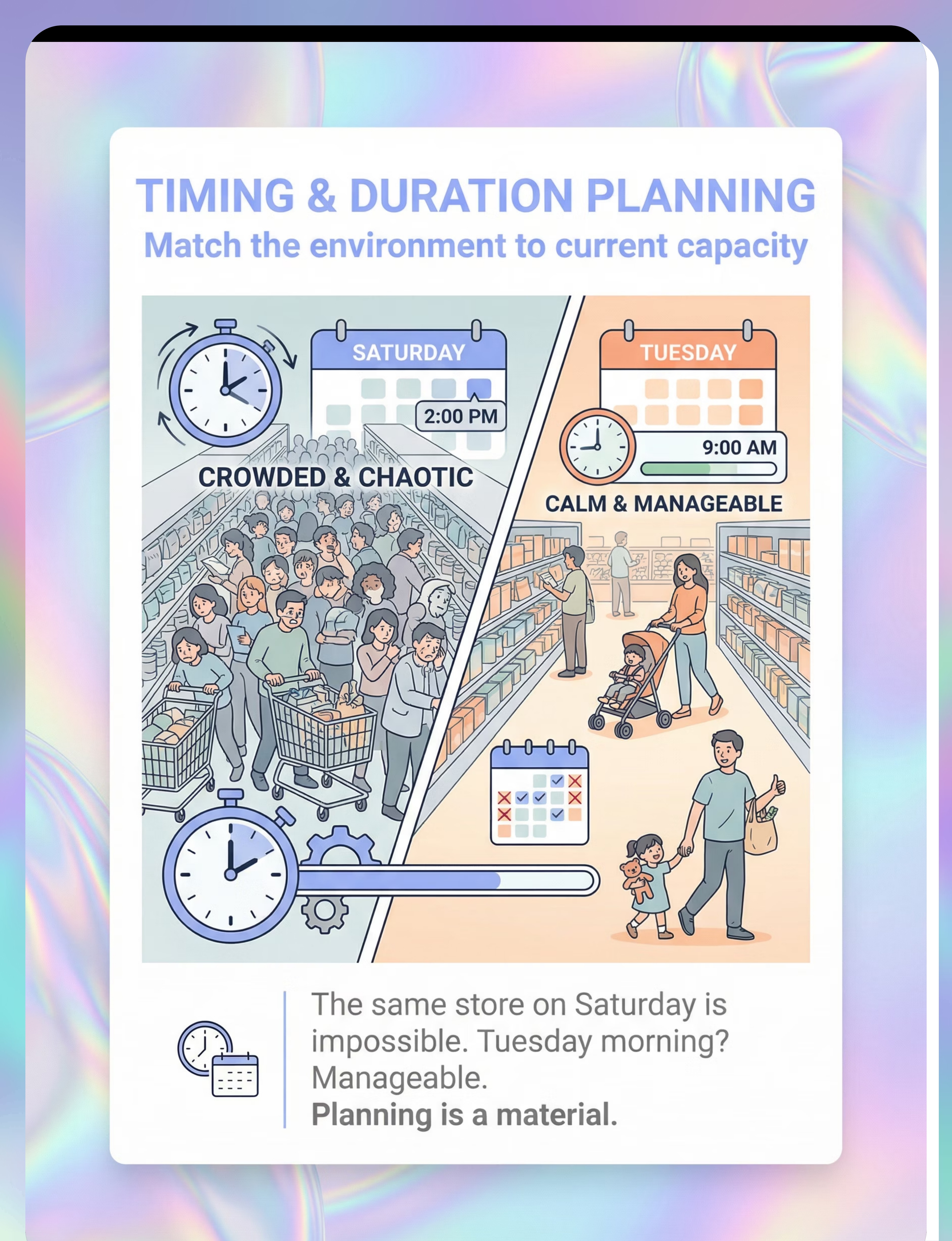
9. Strategic Timing & Duration Planning
Price: ₹0 (Strategy, not product)
Ask store staff when it's least crowded. Early morning weekdays are typically quietest. Plan 20 minutes maximum. Leave on schedule — before meltdown, not because of one.
Ask store staff when it's least crowded. Early morning weekdays are typically quietest. Plan 20 minutes maximum. Leave on schedule — before meltdown, not because of one.
The Zero-Cost Outing Kit: Sunglasses (₹200) + tight athletic shirt + child's comfort toy + hand-drawn schedule + crunchy snacks + timing plan = Under ₹500 total. Total estimated full kit: ₹0–8,000+ depending on selections. Essential starters: Headphones + Sunglasses + Comfort Object + Visual Schedule + Strategic Timing = ₹2,000–12,000.

Safety First — Before You Begin
🔴 STOP — Do Not Proceed If:
• Child is already in distress, fatigued, or ill before the outing
• Child has had a meltdown or shutdown in the past 2 hours
• You do not have an exit plan
• You are rushing and cannot commit to leaving on schedule
• Weighted items exceed 10% of child's body weight
• Chewable items show signs of wear, cracking, or degradation
• Child has had a meltdown or shutdown in the past 2 hours
• You do not have an exit plan
• You are rushing and cannot commit to leaving on schedule
• Weighted items exceed 10% of child's body weight
• Chewable items show signs of wear, cracking, or degradation
🟡 CAUTION — Proceed with Awareness:
• Ensure headphones still allow child to hear your voice and safety-relevant sounds
• Medium-tint sunglasses recommended indoors — very dark may affect depth perception
• Monitor for overheating when using weighted vests, especially in Indian summer
• Never leave weighted items on sleeping or unsupervised children
• Some children resist headphones — practice at home in a calm setting first
• Medium-tint sunglasses recommended indoors — very dark may affect depth perception
• Monitor for overheating when using weighted vests, especially in Indian summer
• Never leave weighted items on sleeping or unsupervised children
• Some children resist headphones — practice at home in a calm setting first
🟢 GO — Ready When:
• Child is rested, fed, and in a regulated baseline state
• Outing kit is packed and accessible (not buried in a bag)
• Visual schedule reviewed WITH the child before departure
• You know your quiet spaces and escape routes
• Planned duration is set and you are committed to leaving on schedule
• Communication signal agreed with child for "I need a break"
• Outing kit is packed and accessible (not buried in a bag)
• Visual schedule reviewed WITH the child before departure
• You know your quiet spaces and escape routes
• Planned duration is set and you are committed to leaving on schedule
• Communication signal agreed with child for "I need a break"
Red Line: Stop immediately and seek professional guidance if your child shows self-injurious behavior during overwhelm, prolonged shutdowns (unresponsive for more than 15 minutes), physical aggression causing injury, or meltdowns increasing in frequency and severity despite consistent use of these strategies.

Setting Up Your Outing Kit
The "outing kit" is not assembled each time — it lives in a dedicated backpack or tote that is always packed and ready to grab. The routine of the kit becomes its own cue for regulation.
Inside the Kit
✓ Noise-reducing headphones (charged if active NC) ✓ Tinted glasses or sunglasses ✓ Weighted lap pad or compression shirt ✓ Comfort object / favorite fidgets (child-selected) ✓ Laminated visual schedule OR phone with photo schedule ✓ Oral sensory tools + crunchy snacks in container ✓ Water bottle ✓ One preferred calming activity (small book, sticker sheet, preferred app)
Parent Preparation
Accept that you may need to leave earlier than planned — that's a success, not a failure. Prepare responses for strangers: "He wears headphones because loud environments are hard for his brain. Thank you for understanding." And bring your own regulation: you cannot regulate your child if you are dysregulated. Breathe.

Readiness Check — Is Your Child Ready?
Before every outing, run through this four-area readiness check. A single amber or red flag is a signal to adjust the plan — not push through.
Physical State
☐ Slept adequately — not overtired
☐ Eaten recently — hunger increases sensitivity
☐ Not ill or recovering from illness
☐ Had some movement/proprioceptive input today (jumping, swinging, rough play)
☐ Eaten recently — hunger increases sensitivity
☐ Not ill or recovering from illness
☐ Had some movement/proprioceptive input today (jumping, swinging, rough play)
Emotional State
☐ Calm or regulated baseline — not mid-tantrum or post-meltdown
☐ No major stressors today (new environment anxiety, schedule changes, family conflict)
☐ Not already at sensory threshold from earlier activities
☐ No major stressors today (new environment anxiety, schedule changes, family conflict)
☐ Not already at sensory threshold from earlier activities
Environmental Match
☐ Destination strategically timed for low-traffic period
☐ Duration planned is LESS than child's current maximum tolerance
☐ Quiet spaces/escape routes identified at destination
☐ Weather appropriate for weighted/compression wear
☐ Duration planned is LESS than child's current maximum tolerance
☐ Quiet spaces/escape routes identified at destination
☐ Weather appropriate for weighted/compression wear
Kit Status
☐ Outing kit packed and accessible
☐ Headphones charged
☐ Visual schedule reviewed with child
☐ Snacks and oral tools fresh and available
☐ Distress signal confirmed with child
☐ Headphones charged
☐ Visual schedule reviewed with child
☐ Snacks and oral tools fresh and available
☐ Distress signal confirmed with child
"GREEN on all sections? Let's go. AMBER on any? Consider adjusting the plan. RED on any? Today may not be the day — and that's okay."
The Invitation — Framing the Outing
This is an invitation, not a command. The child who participates in the plan owns the plan — and ownership reduces anxiety. The conversation before leaving home should feel empowering, not instructional.
Ages 2–4 (Pre-Verbal or Early Verbal)
Show the visual schedule. Point to each step. Use simple language: "First store [point to picture]. Then park [point to picture]. Then home [point to picture]." Put headphones on the child's favorite stuffed animal first: "Bear is wearing his headphones for the store. Want yours?" Offer the comfort object. Let the child hold the schedule.
Ages 4–7 (Verbal)
"We're going to [place] today. Remember, it can be noisy and busy there. What do we bring?" Let the child name the tools. "Right — headphones, your glasses, [comfort object]. We'll be there for [duration]. If it gets too much, what do we do?" Let the child answer. Review the visual schedule together. Empower: "You have your tools. You've got this."
Ages 7–12 (Self-Aware)
"We're heading to [place]. Want to talk through the plan?" Review the schedule. Let the child choose which tools to bring — they may have preferences you didn't expect. Discuss the escape plan: "If you need a break, just [signal]. No questions asked." And for older children: "Some people might look at your headphones. That's their problem, not yours. Your comfort matters more than anyone's opinion."

Engagement — Entering the Environment
"The first 3 minutes determine everything. Protect the entry." Protection goes on BEFORE the sensory assault begins — not after the child is already overwhelmed. Every step of the entry protocol exists to give the nervous system the best possible chance of successful regulation.
The Action — During the Outing
What to Do
MAINTAIN PROTECTION: Keep all tools active throughout. Don't remove headphones "to see if he's okay now." If the child removes them voluntarily — that's their choice and their progress. Offer oral sensory input proactively: "Want your chewy?" Don't wait for escalation. Check the timer regularly. Stick to the plan.
STAY CONNECTED: Maintain physical contact if the child wants it. Narrate the plan: "We're almost done here. Two more things, then we go." Validate: "I know it's loud. Your headphones are helping. You're doing great."
MANAGE TRANSITIONS WITHIN THE SPACE: Moving between sections is its own transition. Pause briefly. Reorient. If moving from quiet to loud zone: warn the child. "This part is noisier. Ready?"
What to Watch For
EARLY WARNING SIGNS (ACT NOW):
• Eyes darting or tracking multiple stimuli
• Increased fidgeting or restlessness
• Pulling at clothing
• Seeking more physical contact with you
• Verbal complaints: "too loud," "too bright"
• Covering ears even with headphones on
• Eyes darting or tracking multiple stimuli
• Increased fidgeting or restlessness
• Pulling at clothing
• Seeking more physical contact with you
• Verbal complaints: "too loud," "too bright"
• Covering ears even with headphones on
→ Move to quieter area immediately. Offer break. Do NOT say "just a few more minutes" — the child's nervous system doesn't negotiate.
ESCALATION SIGNS (LEAVE NOW):
• Crying, screaming, inconsolable distress
• Physical aggression or self-injury
• Flight response (trying to run)
• Shutdown: going silent, vacant, unreachable
• Crying, screaming, inconsolable distress
• Physical aggression or self-injury
• Flight response (trying to run)
• Shutdown: going silent, vacant, unreachable
Leave now. No exceptions. Staying "to finish" creates trauma, not tolerance.

Reinforce — Celebrate the Success
During the Outing
Use specific praise: "You're using your headphones in this noisy place. That's so smart." Acknowledge effort, not just outcome: "I can see this is hard. You're doing it." Small, in-the-moment reinforcers: preferred snack, quick phone game in quiet spot, verbal praise that lands at exactly the right moment.
Leaving on Schedule — The Most Important Reinforcement
When the timer goes off: LEAVE. Even if the child is doing well. Especially if the child is doing well. Leaving on a success builds trust. The child learns: "The plan was followed. It ended before it got terrible. I can do this again."
On the Way Home + At Home
"You went to [place] today. You used your headphones and your glasses and your schedule. You did the whole 20 minutes. That's incredible." At home: a preferred activity, rest time, a progress chart with stickers or stamps, and telling the other parent/caregiver — "He went to the mall today for 20 minutes with his kit. He did it."
"Every successful outing — even 10 minutes — is a deposit in the tolerance bank. Meltdowns are withdrawals. Build the balance."

Cool-Down and Recovery
Even successful outings tax the nervous system. Your child's brain has been working overtime to process input through protective filters. Recovery is NOT optional — it's part of the protocol.
1
Immediate (First 30 Minutes Home)
Low-stimulation environment: dim lights, minimal sound, no screens if possible. Let the child decompress in their preferred way. Offer water and a light snack. Do NOT immediately launch into the next activity. Remove weighted vest/compression garment — the protective "armor" comes off in the safe base.
2
Short-Term (1–3 Hours)
Expect lower tolerance for other sensory input (siblings may seem "too loud"). Expect lower frustration tolerance. This is NOT regression — this is a tired nervous system recovering from hard work. Allow self-directed sensory regulation: swinging, bouncing, quiet play, preferred stims.
3
If Outing Ended in Meltdown
Extended recovery may be needed (2–4 hours or remainder of day). Do not discuss what happened until the child is fully regulated. Do not punish or "teach a lesson" about the meltdown. Analyze privately: What signs did you miss? What was different — timing, duration, or environment?
"Recovery is not a luxury. It's the second half of the intervention."

Data Capture — Track What Matters
Every data point feeds into GPT-OS® — which tracks your child's Community Participation Index, Environmental Adaptability Index, and Sensory Modulation Index. Over time, patterns emerge: which environments at which times with which tools produce the best outcomes. This is personalized care — powered by your observations.
What to Record After Every Outing
Logistics: Date · Destination · Time of day · Crowd level (1–5) · Duration planned vs. achieved
Tools Used: ☐ Headphones ☐ Glasses ☐ Weighted vest ☐ Comfort object ☐ Visual schedule ☐ Escape route ☐ Stroller ☐ Oral tools ☐ Timing plan
Which tool helped MOST? ___ Which was LEAST used? ___
Which tool helped MOST? ___ Which was LEAST used? ___
Child State: Before outing (1–5): ___ During outing peak (1–5): ___ After outing (1–5): ___ Recovery time needed: ___
Outcome: ☐ Completed as planned ☐ Left early (planned) ☐ Left early (overwhelm) ☐ Meltdown ☐ Shutdown
Why This Data Matters
Patterns emerge across weeks of data — revealing which environments at which times with which tools produce the best outcomes for your specific child.
GPT-OS® uses your records alongside anonymized data from 20M+ sessions to generate personalized next-step recommendations — when to try a harder environment, when to reduce supports, when to seek professional input.

Troubleshooting — When It's Not Working
Every family hits obstacles. The following are the most common challenges — and exactly what to do about each one.
"My child refuses to wear headphones."
Start at home in a calm environment. Let the child explore the headphones without wearing them. Put them on yourself, on a stuffed animal, on a sibling. Play preferred music through them. Never force them on. Try different styles: over-ear vs. headband vs. earplugs. If all headphones are refused, focus on other tools — this channel is not the priority right now.
"We tried glasses and she rips them off."
Start with the child's own choice of sunglasses — let them pick from a selection. Practice wearing them in easy environments first (sunny park). Some children tolerate clip-on shades on existing glasses better. If glasses are strongly refused, consider a hat with a brim as partial visual reduction.
"He had a meltdown anyway — the tools didn't work."
Ask: Was the environment harder than planned? Was the child at baseline? Were tools applied BEFORE entry? Was duration too long? Was there an unprepared transition? One meltdown doesn't mean the approach failed — analyze the specific variable. Adjust the plan, not the strategy.
"She's fine for 10 minutes then suddenly falls apart."
This is cumulative load. Ten minutes may be her current ceiling. Plan 8-minute outings. Leave at 8 minutes — before the fall. Build from there: 10 minutes next time, 12 the time after. The ceiling rises with repeated successful exposures that end BEFORE overload.
"Other people stare or make comments."
Prepare your response: "He wears headphones because his brain processes sound differently. It helps him be here with us." You do not owe anyone an explanation. Your child's comfort outranks anyone's curiosity.
"My child is too old for a stroller but still overwhelmed."
Replace the stroller function: weighted backpack, compression clothing, a "home base" bench within the venue, more frequent breaks, shorter total duration. Older children often respond well to personal agency: "You carry the headphones. You decide when to put them on."
Adapt — Personalize to Your Child
Adapting by Age
Toddlers (2–3 years): Stroller as primary safe base. Maximum 10–15 minute outings. Comfort object is essential; child may not accept other tools yet. Parent is the primary regulation tool — hold, carry, be close.
Preschoolers (3–5 years): Full kit becomes feasible. Visual schedule with photos or drawings. Practice wearing tools at home first. Introduce the "break" concept: model taking breaks yourself.
School-Age (6–9 years): Child can participate in kit selection. Social stories about why they use tools. Gradual independence: child puts on own headphones, checks own schedule. Prepare for questions from peers.
Pre-Teens (10–12 years): Discreet tools preferred — earplugs over headphones, light tint over dark sunglasses, compression shirt under regular clothes. Maximum agency: child leads the plan. Self-advocacy: child explains their own needs.
Adapting by Sensory Profile
Primarily auditory sensitive: Prioritize headphones; other tools secondary.
Primarily visual sensitive: Prioritize glasses + hat; avoid direct fluorescent light positioning.
Primarily tactile sensitive: Prioritize compression clothing + stroller; avoid peak crowds.
Oral sensory seeker: Prioritize chewables + crunchy snacks — these may be the child's most effective tool.
Multi-channel overwhelm: Full kit deployed; shortest duration; most strategic timing. Every variable matters.

Session Complete — You're Equipped
✅ The Understanding
Your child's brain processes sensory input differently. Crowded environments overwhelm because ALL channels are at maximum simultaneously. This is neurology, not behavior.
✅ The Tools
9 materials — each targeting a specific channel or coping mechanism. From ₹0 (timing/planning) to ₹8,000 (full commercial kit). DIY alternatives for every budget.
✅ The Protocol
Equip before entry. Pause at threshold. Gradual entry. Monitor continuously. Leave on schedule. Recover fully. Every step serves the nervous system.
✅ The Data + Mindset
Track every outing. Every successful outing — even 10 minutes — builds tolerance. Meltdowns erode it. Protect the wins. GPT-OS® will personalize as data accumulates.
Next Session Goal: Plan ONE outing this week using at least 3 tools. Choose a low-challenge environment at a low-traffic time. Plan for a duration LESS than your child's current ceiling. Document the outcome.
"From fear to mastery. One outing at a time."

Weeks 1–2: Establishing the Foundation
The first two weeks are about building the routine, not pushing the limits. The goal is simple: outings that end before meltdown, a kit that is always packed, and at least two data points recorded.
1
Week 1 — First Outings
1–2 outings using the full protection kit. Target LOW-challenge environments — quiet grocery store, uncrowded park, familiar restaurant at off-peak. Duration: 10–20 minutes maximum. The child may resist some tools. Offer, don't force. Focus entirely on establishing the routine: pack kit → review schedule → equip → enter → timer → leave on time → recover.
2
Week 2 — Building the Pattern
2–3 outings at the same or similar environments. You may notice: the child reaches for headphones independently, shows less resistance to the routine, begins to associate the kit with "we're going out" rather than "something hard is happening." If Week 1 outings resulted in meltdowns — reduce the challenge. Lower-stimulation environment, shorter duration, more strategic timing.
What Success LOOKS Like
You completed outings that ended before meltdown. The kit is packed and ready. You have data from at least 2 outings.
What Success Does NOT Look Like
Your child suddenly loves crowded malls. That's a months-long goal, not a Week 1 outcome. Manage your own expectations alongside your child's nervous system.

Weeks 3–4: Building Tolerance
In weeks 3–4, you begin to gradually expand — but with a critical rule: increase either duration OR environment challenge — never both simultaneously.
How to Progress
If a 15-minute grocery trip is stable → try 20 minutes at the same store, same time. OR: keep 15 minutes but try a slightly busier time slot. The child may begin self-managing some tools (putting on own headphones, requesting breaks verbally). You may notice the visual schedule becomes less critical as the routine becomes familiar.
Positive Progression Indicators
• Duration extending without signs of overload
• Child requesting outings or not resisting them
• Recovery time decreasing after outings
• Fewer early warning signs during outings
• Child using distress signal BEFORE meltdown (communication improving)
• Child requesting outings or not resisting them
• Recovery time decreasing after outings
• Fewer early warning signs during outings
• Child using distress signal BEFORE meltdown (communication improving)
Plateau or Concern Indicators
• No change in tolerance duration after 3–4 weeks
• Meltdowns at the same time and intensity as Week 1
• Child refusing to participate despite gentle, consistent approach
→ Consider OT consultation for comprehensive sensory profile. If worsening: illness, anxiety, sleep changes, or schedule disruption may be contributing.
• Meltdowns at the same time and intensity as Week 1
• Child refusing to participate despite gentle, consistent approach
→ Consider OT consultation for comprehensive sensory profile. If worsening: illness, anxiety, sleep changes, or schedule disruption may be contributing.
Weeks 5–8: Expanding the World
By weeks 5–8, if progression is on track, the world that was once defined by avoidance begins to genuinely expand. Duration stretches. New environments become accessible. The child may surprise you — "Can we go to [place]?"
Low Challenge
Quiet grocery store (Tuesday morning) → Moderately busy store (Saturday morning)
Moderate Challenge
Familiar restaurant off-peak → Busier restaurant → Mall food court with short duration + break plan
Higher Challenge
Mall at moderate traffic → Festival/event with planned duration and escape route → Airport/travel with comprehensive preparation
By Week 5–8: Duration 30–60 minutes in moderate-challenge environments with full kit. Variety: 3–4 different environment types successfully navigated. Independence: child managing 1–2 tools independently. Some tools may no longer be needed for lower-challenge environments.
"Each successful experience is a brick in the foundation. The world doesn't have to keep shrinking. It can expand — one protected outing at a time."

Celebrate — Every Milestone Matters
"We couldn't go anywhere. Now we bring his outing bag — headphones, his squishy, his visual schedule. We go to the store Tuesday mornings. We did a mall trip last month — 40 minutes. He needed his headphones the whole time and we took one break, but he did it. We're not avoiding life anymore. We're managing it." — Mother, Pinnacle Blooms Network, Hyderabad
(Illustrative case; individual outcomes vary.)
First Wins
🌟 First outing completed without meltdown
🌟 First time the child put on headphones independently
🌟 First time the child used the distress signal BEFORE meltdown
🌟 First time the child put on headphones independently
🌟 First time the child used the distress signal BEFORE meltdown
Growing Wins
🌟 First outing lasting longer than the previous record
🌟 First new environment successfully navigated
🌟 First outing where a tool was no longer needed
🌟 First new environment successfully navigated
🌟 First outing where a tool was no longer needed
Life-Changing Wins
🌟 First time the child ASKED to go somewhere
🌟 First family event attended and completed
🌟 First time a stranger commented positively on the tools and strategies
🌟 First family event attended and completed
🌟 First time a stranger commented positively on the tools and strategies

Red Flags — When to Get Professional Help
These strategies are designed for parent-led implementation — but some situations require professional evaluation. Use the following as your guide for when to escalate.
⚠️ Occupational Therapist
• Child needs comprehensive sensory processing evaluation
• You need an individualized sensory diet beyond outing tools
• School is requesting accommodation letters or sensory support plans
• Progress has plateaued despite 4+ weeks of consistent implementation
• You need an individualized sensory diet beyond outing tools
• School is requesting accommodation letters or sensory support plans
• Progress has plateaued despite 4+ weeks of consistent implementation
⚠️ Neurodevelopmental Pediatrician
• Sensory issues are part of a broader developmental profile
• You are questioning whether autism or another condition may be present
• Medication assessment for co-occurring anxiety is being considered
• You are questioning whether autism or another condition may be present
• Medication assessment for co-occurring anxiety is being considered
⚠️ Psychologist
• Significant anxiety component beyond sensory processing
• Child has developed phobic avoidance of all environments
• Family is significantly impacted and needs support
• Trauma history related to past sensory overload experiences
• Child has developed phobic avoidance of all environments
• Family is significantly impacted and needs support
• Trauma history related to past sensory overload experiences
⚠️ Board Certified Behavior Analyst
• Meltdowns involve safety concerns (running into traffic, self-injury)
• School requires a formal behavior support plan with community data
• Need a structured desensitization protocol beyond what this guide provides
• School requires a formal behavior support plan with community data
• Need a structured desensitization protocol beyond what this guide provides
Immediate Professional Contact: Self-injurious behavior during or after overwhelm · Prolonged shutdowns (unresponsive >15 minutes) · Regression in other developmental areas · Your child expresses they "don't want to be alive" or similar distress.

Progression Pathway — What Comes Next
GPT-OS® tracks your child's progress through six defined stages — from complete avoidance to functional community access. Understanding the full arc helps you see every small win in context.
Stage 1 — Severe Avoidance
Cannot enter complex environments. Immediate meltdown/shutdown. Family isolation. → This technique starts here.
Stage 2 — Brief Protected Exposure
10–15 minutes with maximum supports (all 9 materials). Specific low-challenge environments only.
Stage 3 — Extended Protected Exposure
30–60 minutes with full supports. Variety of environments. Recovery time shortening.
Stage 4 — Moderate Supported Exposure
Longer durations. Some supports reduced. Most environments accessible with the kit.
Stage 5–6 — Light Supported → Functional Access
Minimal supports for most environments. Child self-manages tools. Participates in family and community life. World is no longer shrinking — it's expanding.
Related Techniques — The Sensory Cluster
Multi-sensory environmental overwhelm rarely exists in isolation. The following techniques form the complete environmental sensory cluster — and are the most common co-occurring challenges families in A-039 also navigate.
Same Cluster — Environmental Sensory Challenges
→ A-036: Hand Dryer Fear
→ A-037: Sensitivity to Sudden Sounds
→ A-038: Visual Over-Responsivity
→ A-039: Crowded Noisy Places (YOU ARE HERE) ★
→ A-040: Multiple Sensory Sensitivities Overview
→ A-037: Sensitivity to Sudden Sounds
→ A-038: Visual Over-Responsivity
→ A-039: Crowded Noisy Places (YOU ARE HERE) ★
→ A-040: Multiple Sensory Sensitivities Overview
Parent Knowledge Support
→ K-910: Understanding Multi-Sensory Overload
→ K-912: Planning Successful Family Outings
→ K-915: When to Push and When to Protect
→ K-912: Planning Successful Family Outings
→ K-915: When to Push and When to Protect
Deep Dives (Coming Soon)
→ "Creating an Outing Survival Kit: The Complete Guide" (A-039-DD-01)
→ "Strategic Timing for Different Environments" (A-039-DD-02)
→ "Strategic Timing for Different Environments" (A-039-DD-02)
The Full Developmental Map
Sensory processing challenges rarely exist in isolation. A-039 connects to motor development, communication, social-emotional development, behavioral regulation, and community participation. The brain doesn't organize by therapy domain — and neither should the intervention.
A-039 Connects to: Motor (proprioceptive processing affects motor planning) · Communication (overwhelm suppresses expressive language) · Social-Emotional (avoidance reduces social participation) · Behavioral Regulation (meltdowns are a regulation challenge) · Community Participation (the direct impact of this technique).

Family Stories — You're Not Alone in This
Hyderabad
"We hadn't been to a mall in two years. Two years. Not because we didn't want to — because we couldn't. After working with Pinnacle and building his outing kit, we went back. Twenty minutes. He wore his headphones, held his bear, and I followed his schedule. He asked for a break once. We sat by the fountain for 3 minutes. Then he said, 'Okay, let's go.' We finished the trip. I cried in the car — but happy tears." — Mother, Pinnacle Blooms Network
Bangalore
"The airport was our nightmare. Travelling to see grandparents meant hours of distress. Now we prepare: visual schedule of the airport, headphones from the parking lot, compression shirt under his clothes, his fidget collection in his backpack. Security still stresses him, but he makes it through. Our family is connected again." — Father, Pinnacle Blooms Network
Chennai
"I thought we'd never go to a restaurant again. Now we go Tuesday evenings — early, before the rush. He sits with his weighted lap pad, chews his necklace, and we eat dinner together. It's not perfect. But it's dinner. Together. As a family." — Mother, Pinnacle Blooms Network
Illustrative cases; individual outcomes vary by child profile.

Connect — Join the Community
Pinnacle Parent Community
Join thousands of families navigating sensory challenges together — sharing strategies, celebrating milestones, and supporting each other through hard days.
Find a Center Near You
Pinnacle Blooms Network operates 70+ centers across India.
Parent Training Programs
EverydayTherapyProgramme™: Daily home-executable micro-interventions designed to build into your existing routine.
Parent Sensory Training: Learn to read your child's sensory signals before they reach the meltdown threshold.
Outing Success Workshop: Hands-on training for community access strategies — from kit assembly to graded exposure protocols.
Online Resources
Professional Access — Pinnacle Centers
Services for This Technique
✓ Occupational Therapy — Sensory Integration (Ayres SI® based)
✓ Comprehensive Sensory Processing Evaluation
✓ Individualized Sensory Diet Development
✓ Parent Training for Sensory Support Strategies
✓ EverydayTherapyProgramme™ — Home extension
✓ School Consultation and Accommodation Support
✓ FusionModule™ — Coordinated multi-disciplinary approach
✓ Comprehensive Sensory Processing Evaluation
✓ Individualized Sensory Diet Development
✓ Parent Training for Sensory Support Strategies
✓ EverydayTherapyProgramme™ — Home extension
✓ School Consultation and Accommodation Support
✓ FusionModule™ — Coordinated multi-disciplinary approach
Your Assessment Path
1. Call FREE National Autism Helpline: 9100 181 181 (24x7, 16+ languages)
2. AbilityScore® Assessment — comprehensive developmental baseline
3. Comprehensive Sensory Processing Evaluation
4. Individualized intervention plan generated by GPT-OS®
5. Track progress through Community Participation Index + Environmental Adaptability Index + Sensory Modulation Index
2. AbilityScore® Assessment — comprehensive developmental baseline
3. Comprehensive Sensory Processing Evaluation
4. Individualized intervention plan generated by GPT-OS®
5. Track progress through Community Participation Index + Environmental Adaptability Index + Sensory Modulation Index

The Research — Deep Dive
Every material on this page is grounded in peer-reviewed evidence. Every strategy has been validated by the Pinnacle Blooms Consortium — clinicians who have delivered 20M+ therapy sessions across 70+ centers.
Study 1 — PRISMA Systematic Review (2024)
"Sensory Integration Intervention for Children with Autism Spectrum Disorder." 16 articles reviewed (2013–2023). Conclusion: Sensory integration therapy meets criteria as evidence-based practice for ASD. Improvements across sensory processing, adaptive behavior, social skills, and motor function. Published: Frontiers in Pediatrics. Reference: PMC11506176
Study 2 — Meta-Analysis, World J Clin Cases (2024)
"Efficacy of Sensory Integration Therapy in Children with ASD." 24 studies analyzed. Outcomes: Significant improvements in social skills, adaptive behavior, sensory processing, and motor skills. Reference: PMC10955541
Study 3 — Indian RCT, Padmanabha et al. (2019)
"Home-Based Sensory Interventions in Children with ASD." Randomized controlled trial in Indian pediatric population. Demonstrated significant outcomes for parent-administered sensory interventions. Published: Indian Journal of Pediatrics. Reference: DOI: 10.1007/s12098-018-2747-4
Study 4 — WHO Care for Child Development (CCD) Package
Implemented across 54 low- and middle-income countries. Establishes evidence for caregiver-delivered developmental interventions. Reference: PMC9978394
Study 5 — Frontiers in Integrative Neuroscience (2020)
"Framework for Sensory Integration/Sensory Processing Treatment in ASD." Establishes neurological basis for sensory-based interventions. Reference: DOI: 10.3389/fnint.2020.556660
Additional Sources: SPD Foundation · AOTA Position Statement on Sensory Integration · Miller, L.J.: Sensory Modulation Disorder Research · Dunn, W.: Sensory Profile Research · NCAEP (2020): Evidence-Based Practices Report · CDC MMWR (2023): Autism Prevalence Data · WHO/UNICEF Nurturing Care Framework
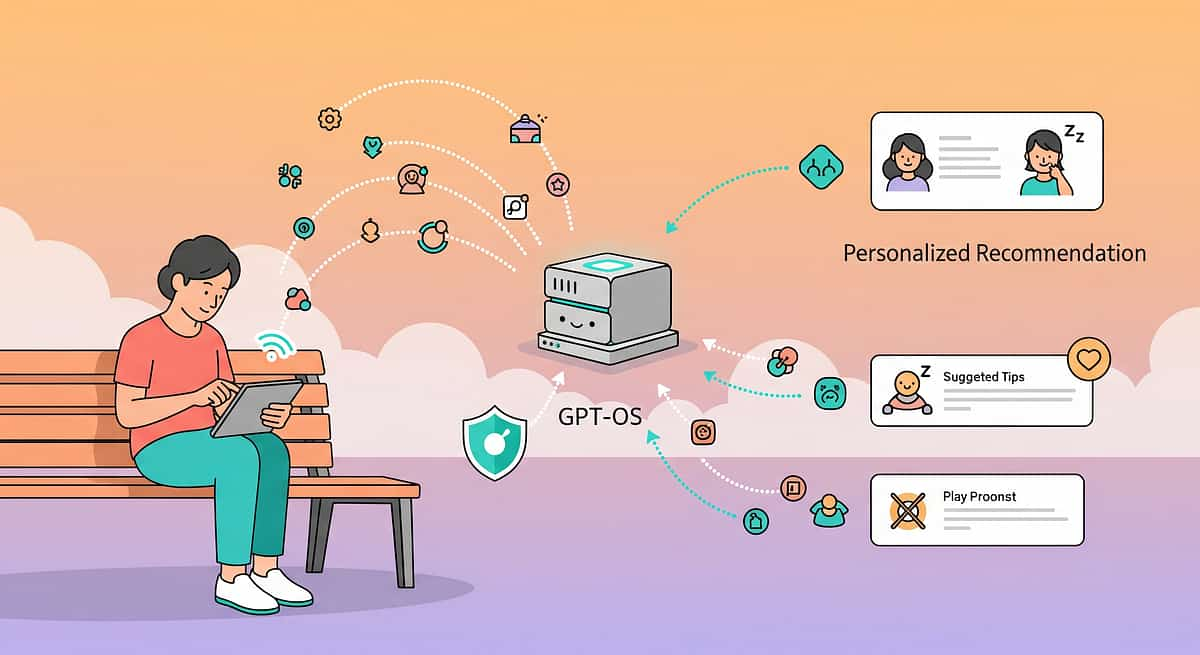
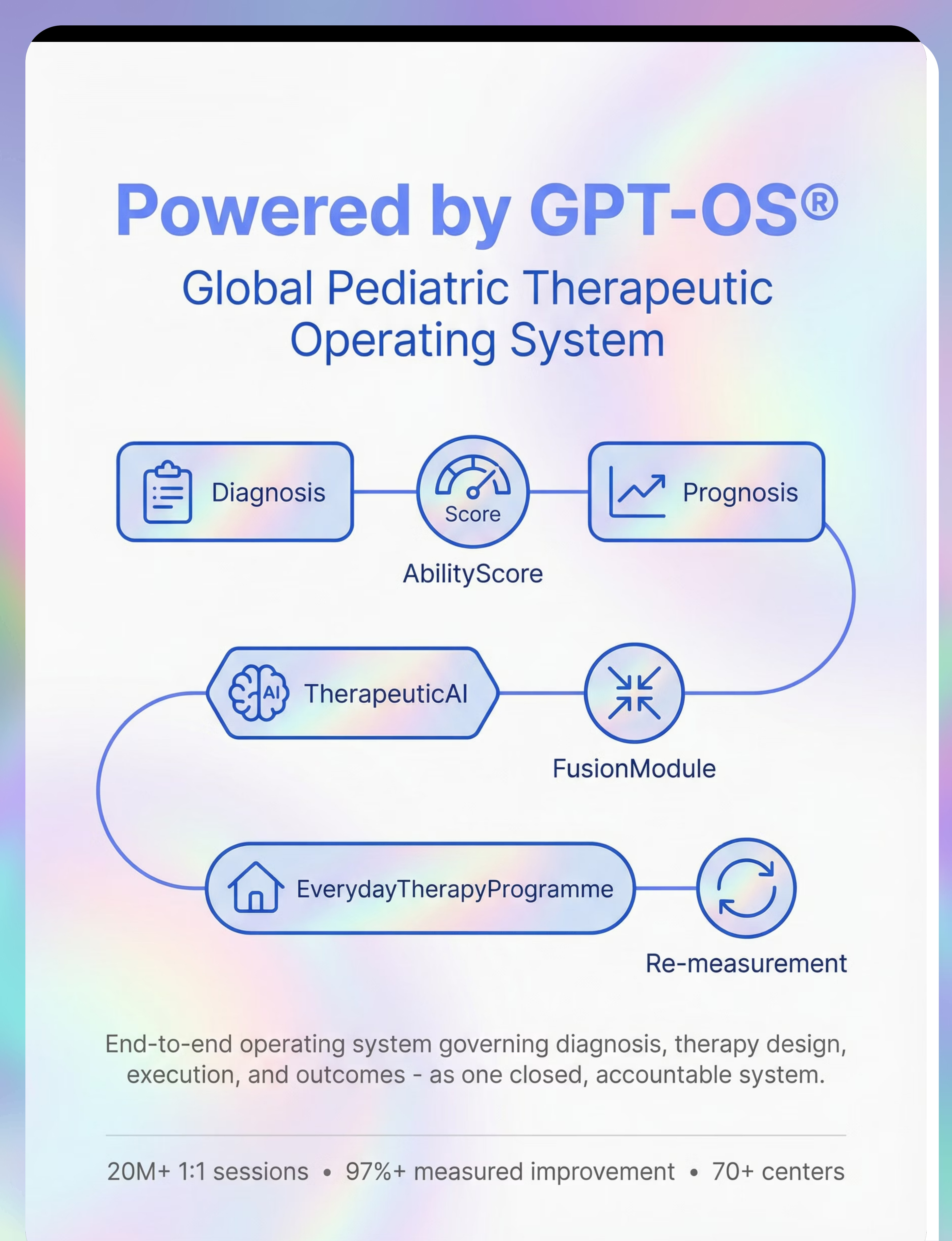
How GPT-OS® Uses Your Data
What GPT-OS® Learns from A-039
• Which combination of sensory protection tools yields the best outcomes for children with your child's profile
• Optimal duration thresholds for different environment types
• Which environments serve as effective stepping stones
• When to recommend OT evaluation vs. continued parent-led intervention
• Population-level insights: "Children with similar profiles typically reach Stage 3 within 6–8 weeks"
• Optimal duration thresholds for different environment types
• Which environments serve as effective stepping stones
• When to recommend OT evaluation vs. continued parent-led intervention
• Population-level insights: "Children with similar profiles typically reach Stage 3 within 6–8 weeks"
Privacy Assurance
Your child's data is protected under Pinnacle's ISO/IEC 27001 information security framework. Data is used only for your child's personalized recommendations and anonymized population insights. You control your data at all times. No personal information is shared with third parties.
"Your data helps your child. And anonymized, it helps every child like yours."
Watch the Reel — A-039
Reel A-039 — Sensory Solutions Series, Episode 39
Domain: Sensory Processing
Duration: 75–85 seconds
9 Materials That Help in Crowded, Noisy Places
A Pinnacle Blooms OT Specialist walks you through all 9 materials — demonstrating each one in real environments. See the headphones going on before a mall entry. Watch a child navigate a store with tinted glasses and a weighted vest. See the visual schedule in action. Experience the transformation from overwhelm to access.
Video modeling is classified as an evidence-based practice for autism (NCAEP, 2020). Multi-modal learning — visual + text + demonstration — improves parent skill acquisition and implementation fidelity.
Share This With Your Family
Consistency across caregivers multiplies impact. If only one parent knows the outing protocol, it's limited. Share this with everyone who takes your child to crowded environments — grandparents, teachers, extended family.
Explain to Grandparents — Simplified Version
Your grandchild's brain processes sensory information differently. Crowded, noisy places feel overwhelming — not because they're difficult, but because their brain hears, sees, and feels EVERYTHING at once with no filter. When we go out, we use special tools: headphones to reduce noise, glasses to soften lights, a weighted vest for calming, and a plan for how long we'll stay. These aren't crutches — they're like wearing glasses for blurry vision. Please support the outing plan, use the distress signal, and leave when the timer goes off — even if everything seems fine. Leaving on a success builds tolerance.
Share & Download
Teacher/School Template: "Dear [Teacher], [Child's name] has sensory processing differences that make crowded/noisy environments challenging. During school events, assemblies, and outings, the following supports are recommended: [list from IEP/plan]. An occupational therapy evaluation has confirmed these needs. We appreciate your partnership."

Frequently Asked Questions
The eight most common questions from families implementing the Multi-Sensory Environmental Protection Protocol — answered with clinical clarity and parental warmth.
Q1: Will my child always need headphones and glasses to go anywhere?
Not necessarily. These are protective tools that enable access NOW while the nervous system builds tolerance. Many children gradually need fewer supports as tolerance increases through repeated successful exposures. Some children continue using select tools (like headphones) by preference — and that's perfectly okay. The goal is functional access, not tool elimination.
Q2: Isn't using all these tools just "avoiding" the problem?
No. Avoidance is staying home. Protection is going out with supports. A person who needs glasses to see doesn't "avoid" the problem of blurry vision — they enable functional access. These sensory tools do the same thing. Protected exposure builds tolerance; unprotected exposure creates trauma.
Q3: What if other parents judge my child for wearing headphones or sunglasses indoors?
Your child's neurological comfort is more important than any stranger's opinion. If asked: "His brain processes sound differently — headphones help." Many parents report that the tools actually reduce judgment because the child is calm and participating rather than melting down. Sensory tools are increasingly normalized.
Q4: My child is 10 — isn't he too old for a comfort object?
Comfort objects are emotional regulation tools, not age-limited items. Many adults carry objects that ground them (jewelry, worry stones, phone). For a child whose nervous system is genuinely overwhelmed, a comfort object provides legitimate neurological regulation. If social concerns arise, transition to discreet comfort items: textured stone in pocket, bracelet, keychain.
Q5: How long until we see improvement?
Most families report noticeable improvement within 2–4 weeks of consistent implementation — slightly longer durations before distress, child reaching for tools independently, faster recovery. Significant functional gains typically take 6–12 weeks. Every child's timeline is different.
Q6: Can I use these strategies without an OT evaluation?
Yes. The materials and strategies on this page are safe for parent implementation without professional guidance. However, an OT provides: specific sensory profile data, individualized tool recommendations, and a graded exposure plan. If progress plateaus after 4–6 weeks, professional evaluation is strongly recommended.
Q7: My child had a meltdown even with all the tools. Should I give up?
One meltdown doesn't invalidate the approach. Analyze: Was the environment harder than expected? Was the child at baseline before the outing? Were tools applied before entry? Was the duration too long? Adjust the specific variable that failed. The strategy works — but each variable must be calibrated to your specific child.
Q8: What about school environments — assemblies, field trips, cafeteria?
The same principles apply. Work with your child's school to implement sensory accommodations: preferential seating, headphones during assemblies, early dismissal from cafeteria if needed, access to a quiet space. An OT can write an accommodation letter. Pinnacle centers provide school consultation support.
Preview of 9 materials that help in crowded noisy places Therapy Material
Below is a visual preview of 9 materials that help in crowded noisy places therapy material. The pages shown help educators, therapists, and caregivers understand the structure and content of the resource before use. Materials should be used under appropriate professional guidance.



Link copied!

The Pinnacle Promise
OT • SLP • BCBA • SpEd • NeuroDev Pediatrician
Pinnacle Blooms Consortium
"From fear to mastery. One technique at a time."
You arrived on this page scared, exhausted, with a world that keeps shrinking. Now you understand the neuroscience. You have 9 evidence-based tools. You have a protocol. You have a community of millions of families walking this same path. Your child's brain is not broken. It processes differently. And with the right supports, the world opens up again.
20M+
1:1 Therapy Sessions
Delivered by the Pinnacle Blooms Network across 70+ centers
97%+
Measured Improvement
Across families served by the Pinnacle Blooms clinical consortium
70+
Centers in India
Serving families from 70+ countries worldwide
Medical Disclaimer: This content is educational. It does not replace assessment by a licensed occupational therapist or healthcare provider. Significant sensory processing difficulties may require comprehensive evaluation and professional-guided intervention. Persistent meltdowns, self-injury, or significant functional impairment warrant professional consultation. Individual results may vary. Statistics represent aggregate outcomes across the Pinnacle Blooms Network. Sensory tolerance timelines vary significantly between children.
© 2026 Pinnacle Blooms Network®, unit of Bharath Healthcare Laboratories Pvt. Ltd. All rights reserved. CIN: U74999TG2016PTC113063 | DPIIT: DIPP8651 (Govt. of India) | MSME Udyog Aadhaar: TS20F0009606 | GSTIN: 36AAGCB9722P1Z2