
When Words Disappear
He used to say "mama," "ball," "more" — and then he just… stopped. The words disappeared. You don't know what happened. He still understands you, but the words are gone. You lie awake replaying every day, searching for the moment it changed. Every silent morning feels heavier than the last.
You are not failing. Your child's brain is reorganizing — and there are bridges you can build right now.
9 Evidence-Based Materials That Support Communication After Word Regression
Regression & Developmental Concerns · Episode B-129
Age Band: 12–36 months · Home & Therapy
🏛️Drafted by the Pinnacle Blooms Consortium: SLP • OT • BCBA • Special Educator • NeuroDevelopmental Pediatrician
🔬Powered by GPT-OS® Therapeutic Intelligence
🔬Powered by GPT-OS® Therapeutic Intelligence

You Are Among Millions
Language regression — the loss of words a child once used — is far more common than most parents realize. You are not alone in this experience. The silence feels isolating, but the science is clear, the pathways are mapped, and the support exists.
25–30%
Children with ASD
Of children later diagnosed with autism experience language regression
15–24mo
Peak Window
The most common age window for regression to occur
18M+
Children in India
Children in India alone who require developmental therapy services
"You are among millions of families worldwide navigating this exact moment. The silence feels isolating — but the science is clear, the pathways are mapped, and the support exists."
The World Health Organization identifies early identification and responsive caregiving as the two most powerful determinants of developmental outcomes. Pinnacle Blooms Network operates 70+ centers across India, delivering 21 million+ therapy sessions with 97%+ measured improvement. Families from 70+ countries access this evidence base. You are here, seeking answers — that is the first and most important step.
📎 References: WHO Nurturing Care Framework (2018) | Barger et al. (2013) | UNICEF MICS developmental monitoring indicators
What's Happening Inside: The Neuroscience of Language Regression
The Brain During Regression
Language regression occurs when the neural pathways supporting word production become disrupted or reorganized. Broca's area — responsible for speech production — may lose connectivity with the motor planning systems that coordinate mouth, tongue, and breath for words.
The critical insight: Your child's comprehension (Wernicke's area) often remains intact. They still know what "mama" means — they've lost the route to say it.
This is why your child may still respond to their name, follow simple directions, or show recognition — even while producing no words.
This is a wiring difference — not a behavior choice.
The 9 materials in this guide target alternative routes — through pictures, gesture, music, and connection — that bypass the disrupted speech production pathway while supporting its reconstruction.
What remains intact:
- Comprehension and understanding (Wernicke's area)
- Response to name and familiar voices
- Music-based pathways (often preserved)
- Motor cortex for gesture
- Visual processing and recognition
This is not "starting over" — it's building bridges around a temporary roadblock.
📎 References: Frontiers in Integrative Neuroscience (2020) DOI: 10.3389/fnint.2020.556660
Where This Sits in Your Child's Development
Understanding the developmental context of regression helps families recognize the window they're in — and where they're headed.
6–9 Months
Babbling, consonant sounds emerging
9–12 Months
First words emerging — mama, dada. Pointing begins.
12–15 Months
3–10 words, pointing, gestures. ⚠️ Early regression window opens.
15–24 Months 🔴
PEAK REGRESSION WINDOW. Word combinations, vocabulary explosion — and the most common time for regression to appear.
24–36 Months
Sentences, questions, storytelling. ⚠️ Late regression can still occur.
Regression rarely happens in isolation. Many families also notice changes in eye contact, social engagement, play patterns, or sensory responses. This is why comprehensive evaluation across all developmental domains is essential — and why the Pinnacle Consortium brings five disciplines together.
📎 References: WHO Care for Child Development (CCD) Package | PMC9978394 | UNICEF MICS developmental indicators

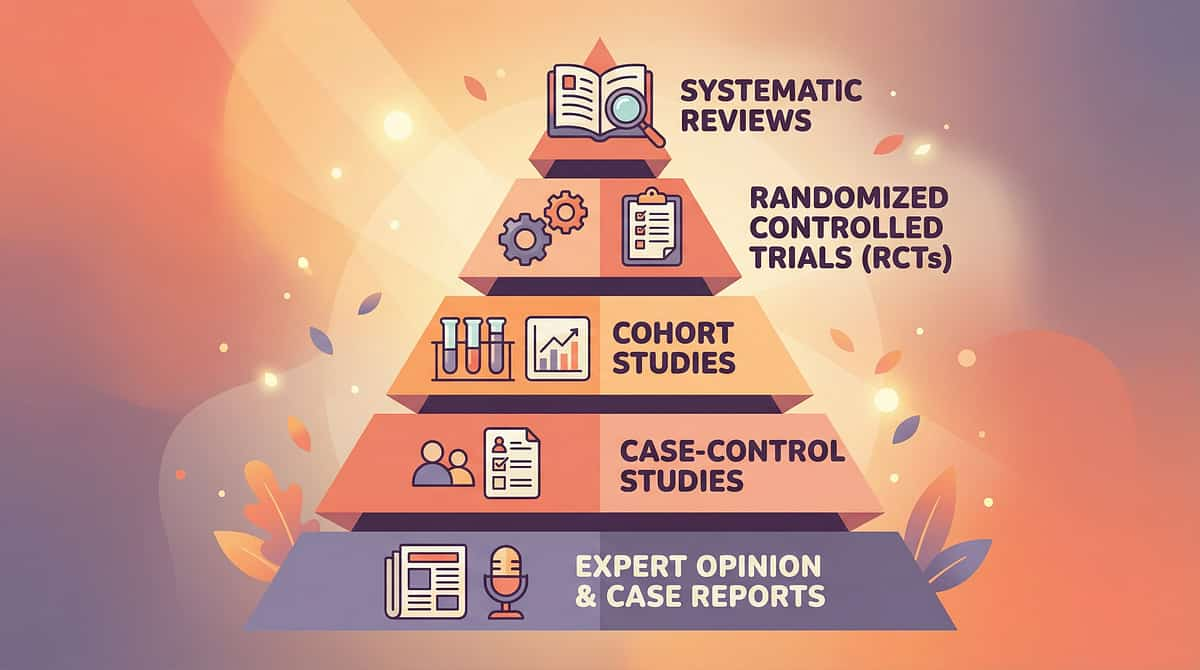
The Evidence Behind These Materials
Level II — Strong Clinical Evidence
The 9 materials recommended in this guide are drawn from multiple converging evidence bases spanning speech-language pathology, occupational therapy, applied behavior analysis, and developmental pediatrics.
🔬 AAC and Language Development
Romski & Sevcik (2005) — AAC supports, never hinders, verbal language return. Multiple RCTs confirm that providing alternative communication increases spoken word production.
🔬 Music and Language Pathways
Neuroimaging studies demonstrate that music engages language-adjacent brain regions. Children who have lost spoken words sometimes retain the ability to sing familiar melodies — a key finding behind Material #3.
🔬 Sensory Regulation and Communication
PRISMA systematic review (2024, PMC11506176): 16 studies confirm sensory integration interventions effectively support developmental outcomes in children with ASD.
🔬 Parent-Mediated Intervention
WHO CCD Package (PMC9978394): Home-based, caregiver-delivered interventions demonstrate comparable or superior outcomes to clinic-only delivery across 54 countries.
"These materials aren't guesses. Each one is backed by published research, validated in clinical practice across thousands of children, and refined through 21 million therapy sessions at Pinnacle Blooms Network."
Clinically validated. Home-applicable. Parent-proven.
📎 References: PMC11506176 | PMC10955541 | PMC9978394 | Romski & Sevcik (2005) | NCAEP Evidence-Based Practices Report (2020)
📎 References: PMC11506176 | PMC10955541 | PMC9978394 | Romski & Sevcik (2005) | NCAEP Evidence-Based Practices Report (2020)
Multimodal Communication Support After Language Regression
Formal Name: Post-Regression Multimodal Communication Scaffolding
Parent-Friendly Name:"Rebuilding Bridges — 9 Materials That Keep Connection Alive When Words Disappear"
Parent-Friendly Name:"Rebuilding Bridges — 9 Materials That Keep Connection Alive When Words Disappear"
A structured approach using 9 evidence-based therapeutic materials to maintain and rebuild communication during and after language regression. Rather than waiting for words to return — which creates a communication vacuum and mounting frustration — this technique provides alternative pathways through pictures, gestures, music, sensory regulation, and relational connection. These keep your child communicating while verbal production recovers.
What It Does
Reduces communication frustration, maintains parent-child connection, supports alternative pathways, and creates conditions for verbal language to re-emerge
Who It's For
Families with children aged 12–36 months experiencing confirmed or suspected language regression — loss of previously acquired words
Frequency
5–15 minutes per material, multiple times daily. Daily integration into natural routines is the goal.
Domain: Speech-Language / Developmental
Age: 12–36 months
Setting: Home & Therapy

Your Consortium Team — Who Uses These Materials and How
"This technique crosses therapy boundaries because the brain doesn't organize by therapy type."
Speech-Language Pathologist (SLP) — PRIMARY LEAD
Drives AAC implementation, communication board design, music-based language elicitation, and verbal production monitoring. The SLP maps which words were lost, which communicative functions remain, and designs the multimodal communication plan.
Occupational Therapist (OT)
Addresses sensory regulation as the foundation for communication readiness. Designs individualized sensory diets and ensures the child's nervous system is organized enough for communication to emerge.
Board Certified Behavior Analyst (BCBA)
Structures reinforcement for communicative attempts across all modalities — whether pointing, gesturing, vocalizing, or producing a word. Designs data collection systems and troubleshoots communication breakdowns.
Special Educator
Integrates communication materials into play-based learning routines and supports generalization across home, school, and community settings.
NeuroDevelopmental Pediatrician
Leads the medical evaluation that MUST accompany any communication support. Rules out treatable medical causes — Landau-Kleffner syndrome, metabolic disorders — and coordinates with neurology and audiology.
📎 References: DOI: 10.1080/17549507.2022.2141327 (Adapted UNICEF/WHO Nurturing Care Framework for SLPs, 2022)

What These 9 Materials Target
Every material in this guide is mapped to a specific communication target. Understanding what you're aiming for helps you recognize progress — even when it doesn't look like spoken words.
What you'll observe if these materials are working: Your child points to pictures on the AAC board to get juice. Your child waves bye-bye when someone leaves. Your child sings part of a familiar song. Your child brings you a toy to play together. These are all communication — and they are all progress.
📎 References: PMC10955541 (Meta-analysis: intervention targets across sensory, social, adaptive, and motor domains)

Your 9 Materials — What to Get
⚠️CRITICAL: These materials support communication while you pursue medical evaluation. They do NOT replace evaluation. If your child is experiencing language regression, contact a developmental pediatrician immediately. FREE National Autism Helpline: 9100 181 181 (24/7, 16+ languages)
# | Material | Price Range (INR) | Canon Category | |
1 | AAC Communication Boards | ₹0–5,000 (DIY to app-based) | Communication & AAC | |
2 | Cause-and-Effect Toys | ₹300–1,500 | Interactive Learning | |
3 | Music and Singing Tools | ₹200–1,500 | Sensory & Music | |
4 | Sensory Regulation Tools | ₹300–3,000 | Sensory Regulation | |
5 | Gestural Communication Games | ₹0–500 | Communication & Social | |
6 | Photo Albums of Family/Favorites | ₹100–500 | Visual Supports | |
7 | Repetitive Interactive Books | ₹200–600 | Literacy & Language | |
8 | Recording/Playback Devices | ₹300–1,500 | Technology Aids | |
9 | Joint Activity Materials | ₹200–1,000 | Social Interaction |
💰Total Comprehensive Setup: ₹1,300–14,000
💡Essential Starter Kit (3 items): DIY AAC Board (free) + Photo Album + Familiar Music = Under ₹500
💡Essential Starter Kit (3 items): DIY AAC Board (free) + Photo Album + Familiar Music = Under ₹500

DIY Alternatives — Start Today With What You Have
Not every family can order online. Not every village has same-day delivery. Every parent, regardless of economic status, can support their child's communication TODAY.
Material | Buy This | Make This (Zero-Cost) | |
AAC Boards | PECS cards, TouchChat app | Print pictures of favorite items & family. Laminate. Put on a board. Point while naming. | |
Cause-Effect Toys | Musical button toys, busy boxes | Light switches, push-button lamps, any toy with a button or lever. Clear, predictable response to child's action. | |
Music Tools | Keyboard, xylophone, rhythm instruments | Pots and spoons as drums. Sing familiar songs from before regression. Pause before key words. | |
Sensory Tools | Therapy swing, weighted lap pad | Heavy blankets, rice-filled sock as lap weight, playground swing time, quiet corners. | |
Gesture Games | Baby sign language cards | Pat-a-cake, peek-a-boo, wave bye-bye. Simple signs for "more," "all done," "help." | |
Photo Albums | Personalized board books | Print photos of family, pets, favorite toys. Put in simple album or tape to cardboard. | |
Repetitive Books | Published board books | Any book with repetitive text. Read the same books many times. Pause before predictable words. | |
Recording Devices | Talk-back toys, echo mics | Voice memo on phone. Record and play back funny noises, animal sounds. | |
Joint Activity | Building blocks, Play-Doh sets | Ball to roll back and forth, stacking cups, bubbles to blow together. |
The principle behind every DIY option: Same neurological pathway, accessible materials. The communication happens through the interaction — not through the price tag.
📎 References: WHO Nurturing Care Framework (2018) — equity-focused interventions | PMC9978394 — CCD Package across 54 LMICs

⚠️ Safety First — Critical Information Before You Begin
🔴 ABSOLUTE REQUIREMENT
Language regression requires IMMEDIATE comprehensive medical evaluation. Contact: Developmental Pediatrician + Neurologist + Audiologist. Regression can indicate autism spectrum disorder, Landau-Kleffner syndrome, metabolic disorders, or other neurological conditions — some of which are TREATABLE.
📞FREE National Autism Helpline: 9100 181 181 (24/7 • 16+ languages). For regression, call immediately rather than waiting for online scheduling.
🟡 MATERIAL-SPECIFIC SAFETY
• Choking hazards: All materials for ages 12–36 months must pass the small parts test.
• AAC boards: Do NOT withhold AAC to "motivate" speech.
• Music tools: Don't force singing — some children may become distressed.
• Sensory tools: NEVER force sensory input the child resists. Consult OT for individualized sensory diet.
• Recording devices: Follow child's lead. Don't use to "test" whether child can say words.
• All interactions: Never turn any material into pressure, testing, or "work."
• AAC boards: Do NOT withhold AAC to "motivate" speech.
• Music tools: Don't force singing — some children may become distressed.
• Sensory tools: NEVER force sensory input the child resists. Consult OT for individualized sensory diet.
• Recording devices: Follow child's lead. Don't use to "test" whether child can say words.
• All interactions: Never turn any material into pressure, testing, or "work."
🟢 PROCEED WHEN
✅ Child has been seen by or referred to developmental pediatrician
✅ Materials are age-appropriate and hazard-free
✅ Child is in a calm, regulated state (fed, rested, healthy)
✅ Parent understands these are SUPPORT tools, not diagnostic or treatment tools
✅ Home environment is calm, with distractions minimized
✅ Materials are age-appropriate and hazard-free
✅ Child is in a calm, regulated state (fed, rested, healthy)
✅ Parent understands these are SUPPORT tools, not diagnostic or treatment tools
✅ Home environment is calm, with distractions minimized
🛑STOP IMMEDIATELY IF: Child shows signs of seizure activity | Acute distress or self-injury | NEW losses beyond language | Fever, lethargy, or sudden behavioral changes → SEEK IMMEDIATE MEDICAL ATTENTION
Set Up Your Communication Space
The environment matters. A calm, organized space creates the conditions for communication to emerge. Spatial precision prevents 80% of session failures.
Choose a consistent spot
Same location each time builds predictability. Floor-level is ideal for ages 12–36 months.
Position yourself face-to-face
At child's eye level — not behind, not above, directly across. Communication is a two-way street; your child needs to see your face.
Place materials within reach
AAC board visible and accessible at all times. Current material between you. Other materials nearby but not overwhelming.
Remove distractions
Turn off TV, silence phones, close doors to busy areas. Other toys out of sight. Siblings in another room if possible.
Optimize lighting, sound, and temperature
Natural light preferred. No background music unless that IS the session. Comfortable temperature — a cold or overheated child won't communicate.
Quick Setup (Under 2 Minutes): Clear a floor space → Place AAC board on left → Today's material in center → Sit face-to-face → Begin.

Is Your Child Ready Right Now?
"The best session is one that starts right."
Take 60 seconds before every session to check your child's readiness. Starting when a child is not ready wastes everyone's energy — and can set back trust in the materials.
Check | ✅ Go | ⚡ Modify | ⏸️ Postpone | |
Fed recently? | Yes, within last hour | Hungry but not distressed | Refusing food, very hungry | |
Rested? | Well-slept, alert | Slightly tired | Exhausted, just woke, overtired | |
Regulated? | Calm, organized | Slightly fussy but redirectable | Meltdown, crying, self-injury | |
Healthy? | No illness signs | Mild runny nose | Fever, pain, acute illness | |
Recent meltdown? | No, calm 15+ min | Minor fuss resolved | Major meltdown within 30 min | |
Interested in you? | Looking, approaching | Neutral, tolerating | Actively avoiding, withdrawing |
✅ Mostly "Go"
Full session with today's chosen material
⚡ Mix of "Go" and "Modify"
Shortened, simplified version — 3–5 minutes only
⏸️ Any "Postpone"
Skip the session. Offer calming sensory input instead. Try again later.
If you postpone — that is not failure. That is clinical judgment. You just read your child like a therapist.

Step 1: The Invitation
30–60 seconds
Every session begins with an invitation, not a command. Choose today's material and rotate through the 9 materials across the week. Don't try all 9 in one day.
Sit at child's level. Hold the material where they can see it. Say with warm enthusiasm: "Look what I have! Want to play with me?" Wait 5 full seconds. Watch for any response — eye glance, reach, lean, vocalization, smile.
What Acceptance Looks Like
Child looks at the material, reaches for it, moves toward you, vocalizes, or simply doesn't move away. Any of these signals readiness to begin.
What Resistance Looks Like
Child turns away, pushes material, cries, covers eyes, or leaves the area. Don't push. Place the material near the child where they can access it independently. Stay nearby. Try a different material.
"That's okay. It's here when you're ready."
"That's okay. It's here when you're ready."
Body Language Guidance: Relaxed shoulders, soft voice, warm facial expression. Open body posture — no hovering, no blocking escape. Mirror your child's pace — slow if they're slow, still if they're still.

Step 2: The Engagement
1–3 minutes
Use the material-specific engagement script that matches what you've chosen for today's session. Keep your energy warm and unhurried.
Material 1 — AAC Board
Point to a picture. Say the word. Wait. Point again. "Look — JUICE. You want JUICE? Point to JUICE." If child reaches for actual juice, guide their hand to the picture first, then give juice. Communication = reward.
Material 2 — Cause-Effect Toys
Press button together. Show delight at the response. Wait for child to press. "Push! You pushed it! MUSIC!" Celebrate any attempt.
Material 3 — Music
Sing a familiar song from before regression. Sing slowly. PAUSE before key words. Wait. "Twinkle twinkle little… [PAUSE 5 seconds]… STAR."
Material 4 — Sensory Tools
Offer the regulation tool. Let child settle. Communication comes AFTER regulation — never before.
Material 5 — Gesture Games
Model the gesture. Pat-a-cake, clap, wave. Pair gesture with word ALWAYS. "CLAP! [clap together] CLAP!"
Materials 6–9
Photos: Look together, name simply, no testing. "Look — MAMA!"
Books: Read, pause before predictable words, create space without pressure.
Recording: Record silly sounds together. Play back. Celebrate any vocalization.
Joint Play: Roll ball back and forth. "ROLL! My turn. Your turn. ROLL!"
Books: Read, pause before predictable words, create space without pressure.
Recording: Record silly sounds together. Play back. Celebrate any vocalization.
Joint Play: Roll ball back and forth. "ROLL! My turn. Your turn. ROLL!"

Step 3: The Therapeutic Action
3–7 minutes
The core principle: MAINTAIN COMMUNICATION THROUGH ANY CHANNEL. Across all 9 materials, the therapeutic action is identical — create a communicative loop where your child acts, you respond meaningfully, and communication is rewarded regardless of modality.
❌ Common Execution Errors
- Testing: "Can you say 'ball'? Say 'ball.'" — Creates pressure and shuts down communication.
- Withholding: Not giving the item until the child says the word.
- Overloading: Using all 9 materials in one session.
✅ What Works
- Modeling: "BALL! You want the BALL! Here's the BALL!" — Language input without demand.
- Honoring: Responding to ANY communicative attempt — point, reach, vocalization — immediately.
- Focusing: One material per session. Depth, not breadth.
Duration: 3–7 minutes of active engagement. Quality over quantity. End before the child wants to — leaving them wanting more.
📎 References: PMC10955541 | NCAEP Evidence-Based Practices Report (2020)
📎 References: PMC10955541 | NCAEP Evidence-Based Practices Report (2020)

Step 4: Repeat & Vary
3–5 minutes
"3 good reps > 10 forced reps."
Target: 3–5 meaningful communication exchanges per session. A communication exchange is any moment where: Child acts → You respond → Connection occurs — whether through pictures, gestures, sounds, or words.
Variation Within Each Material
AAC Board: different pictures each round. Music: same song, different pauses; or different song, same style. Gestures: wave → clap → high five → pat-a-cake. Books: different pages to pause on. Joint Play: different toys, same turn-taking structure.
Satiation Indicators
When you see these — STOP. The session was successful.
• Gaze shifts away consistently
• Body moves toward something else
• Engagement quality drops noticeably
• Mild fussiness emerging
• Simply stops responding
• Gaze shifts away consistently
• Body moves toward something else
• Engagement quality drops noticeably
• Mild fussiness emerging
• Simply stops responding

Step 5: Reinforce & Celebrate
"Celebrate the attempt, not just the success."
Use reinforcement within 3 seconds of any communicative act. Your face, voice, and body all need to say "that was AMAZING."
"YES! You pointed! You TOLD me! Good communicating!"
"You made a sound! I heard you! That was wonderful!"
"You showed me! I understand! Great job!"
The Reinforcement Rules
- Immediate — within 3 seconds of the communicative act
- Specific — name WHAT they did: "You pointed to juice"
- Enthusiastic — your face, voice, and body all respond
- Modality-neutral — a pointed picture is celebrated equally to a spoken word
Natural Reinforcement (Most Powerful)
When child points to juice on AAC board → GIVE THEM JUICE. The natural consequence of communication is the most powerful reinforcer that exists. Don't save reinforcement only for spoken words. Don't use food as the sole reinforcer — the communication itself should be primary.
📎 References: BACB ethical guidelines for reinforcement | ABA reinforcement scheduling literature

Step 6: The Cool-Down
1–2 minutes
No session ends abruptly. Every child needs a clear, predictable signal that the session is wrapping up. Consistency with transitions builds trust and reduces end-of-session meltdowns.
Give a transition warning
"Two more, then all done!" → Do two more exchanges. → "One more, then all done!" → Final exchange. → "All done! Great playing together!"
Offer calming sensory input
Gentle rocking, soft music, favorite blanket, quiet looking at photos — 1–2 minutes of regulation before moving to the next activity.
Material Put-Away Ritual
If child can participate: "Help me put it away. Bye-bye [material]!" — This is itself a communication opportunity.
If child resists ending
This is GOOD — it means they were engaged. But consistency matters. "I know, it was so fun! We'll play again soon. Now it's time for [next activity]." Use a visual timer for the next session to build the expectation.
📎 References: NCAEP Evidence-Based Practices Report (2020) — Visual supports as evidence-based practice

Capture the Data — Within 60 Seconds
"60 seconds of data now saves hours of guessing later."
Record these 3 things immediately after every session. Your data feeds into the Communication Readiness Index tracked through GPT-OS®. Over weeks, patterns emerge — which materials work best, which times of day, which environments. Your clinical team uses this to refine the intervention plan.
Data Point | How to Record | Example | |
Which material used | Name or number | "Material 3 — Music" | |
Communication attempts | Tally count (any modality) | "5 attempts (3 points, 1 vocalization, 1 reach)" | |
Child's state | 😊 Engaged / 😐 Neutral / 😢 Distressed | "😊 Engaged for 4 min, then neutral" |
Optional (if time allows): Any new sounds or vocalizations (write them phonetically) | Which material generated most engagement | Any word approximations or recognizable sounds
📥 Download Tracking Sheet
Printable PDF — one page for 4 weeks of data
📱 Log in GPT-OS® Tracker
Digital tracking through your Pinnacle account at pinnacleblooms.org
📎 References: BACB Guidelines + Cooper, Heron & Heward (Applied Behavior Analysis)
What If It Didn't Go as Planned?
"Session abandonment is not failure — it's data."
Child refused all materials today
That's okay. Sit near your child. Narrate what they ARE doing: "You're spinning the wheel. Spin, spin, spin!" You just provided language input without any materials. That counts.
Child engaged but produced zero communication attempts
Were YOU communicating? If you modeled language, pointed, sang, gestured — your child received language input even without producing it. Receptive comes before expressive. Keep going.
Child became distressed
Stop the session immediately. Offer comfort. This tells you something important: the material, the timing, or the environment needs adjustment. Try a different material tomorrow, at a different time, in a calmer space.
Child only wants one material
Use that one material. If your child will ONLY engage with music, use music every day. Preference is data — it tells you which neural pathway is most accessible.
You feel like nothing is working after a week
One week is too soon to see change. Measurable change typically emerges at 4–8 weeks. Document everything — the patterns reveal themselves over time.
You noticed NEW skill losses beyond language
Contact your developmental pediatrician IMMEDIATELY. New regression beyond the initial language loss requires urgent medical re-evaluation. 📞9100 181 181
Adapt & Personalize — No Two Children Are the Same
Easier Version
1 material/day. 2–3 min max. Zero verbal demands — only modeling. Focus on Material #4 (Sensory Regulation) first. Goal: co-regulation and connection, not communication.
Standard Version
1–2 materials/day. 5–10 min. Gentle pauses inviting communication. Respond to any communicative attempt. Goal: maintaining communication through alternative modalities.
Advanced Version
2–3 materials/day. 10–15 min. Create communication opportunities through play sabotage. Begin expanding from single words to word combinations on AAC. Goal: expanding communicative functions and increasing verbal approximations.
Sensory Profile Adjustments:
• Sensory Seeker: Increase movement-based materials (#2, #5, #9), more animated music (#3), bigger gestures
• Sensory Avoider: Start with calm materials (#6 photos, #7 books), quiet environment, softer voice
• Mixed Profile: Alternate between alerting and calming materials. Use sensory regulation (#4) as a bridge between activities.
• Sensory Seeker: Increase movement-based materials (#2, #5, #9), more animated music (#3), bigger gestures
• Sensory Avoider: Start with calm materials (#6 photos, #7 books), quiet environment, softer voice
• Mixed Profile: Alternate between alerting and calming materials. Use sensory regulation (#4) as a bridge between activities.
Week 1–2: What Real Progress Looks Like
Progress: ~15%
✅ What You MAY See — This IS Progress
- Child tolerates the materials being present (even without engaging)
- Fleeting eye contact during music or photo albums
- Brief engagement moments (3–5 seconds) with one material
- Less distress when materials are offered compared to day 1
- One or two accidental communicative acts (reaching toward a desired item)
⏳ What You Will Likely NOT See Yet
- Spoken words returning
- Consistent use of AAC board
- Extended engagement with materials
- Clear preference patterns
"If your child tolerates the material for 3 seconds longer than last week — that's real progress. Neural pathways are forming. You can't see them, but they're building."
Parent Emotional Preparation: Weeks 1–2 are the hardest. You may feel like nothing is working. This is normal. The research is clear: measurable change in communication intervention typically emerges at 4–8 weeks. Your consistency NOW is building the foundation for change LATER.
⚠️What is NOT progress: If the child shows INCREASING distress, NEW skill losses, or medical symptoms — contact your medical team immediately.

Week 3–4: Consolidation Signs
Progress: ~40%
Neural pathways are actively forming. What you see now is the result of weeks of patient, consistent work.
Consolidation Indicators
- Child anticipates the session — may approach the materials area
- Clear preference for 1–2 materials emerging
- Engagement duration increasing (from seconds to 1–2 minutes)
- Communicative attempts appearing more intentionally (pointing more, reaching more)
- Less resistance to structured interaction
- May begin to tolerate AAC board even if not yet using it purposefully
Spontaneous Generalization Seeds
- Pointing at things outside of sessions
- Bringing items to you (requesting through action)
- Vocalizing more during play (not words yet, but sounds)
- Seeking out music or familiar books independently
When to increase frequency or intensity: If your child shows anticipation and preference — add one more session per day. If engagement exceeds 5 minutes consistently — introduce a second material into the same session.
"You may notice you're more confident too. That parental self-efficacy is the single strongest predictor of your child's continued progress."

Week 5–8: Mastery Indicators
Progress: ~75%
Mastery Criteria
- Purposeful use of AAC board to make requests (points to juice picture when thirsty)
- Consistent gestural communication (signs for "more," "all done," waving)
- Vocalization during music (humming, vowel sounds, word approximations)
- Spontaneous engagement with materials without adult initiation
- Communication frustration DECREASING — child has a working communication system
Generalization Signs
- Using gestures or pointing at the store, at grandparents' house, in the car
- Communicative attempts with other family members, not just primary caregiver
- Showing pictures to unfamiliar people
- Seeking out communication tools (AAC board, photo album) independently
The big question: Are words returning? For some children: yes. Verbal approximations may begin emerging between weeks 6–12, especially through music and repetitive books. For others: alternative communication becomes the primary system while verbal recovery continues on a longer timeline. Both pathways are valid. Both represent functional communication.
🏆"Mastery Unlocked" when: Child independently initiates communication through ANY modality at least 10 times per day in natural routines.

You Did This.
"Your child lost words — and you didn't give up. You didn't wait. You didn't freeze. You built bridges."
In a moment of fear, you sought evidence. You learned 9 therapeutic materials. You set up your space. You showed up, session after session, even when it felt like nothing was happening. You celebrated sounds and gestures and pointed fingers with the same joy you once celebrated first words.
That is world-class parenting. That is therapy.
Your child grew because of your commitment: from communication lost or severely impacted → to alternative communication emerging → to multimodal communication established.
📸 Document This Milestone
Take a photo or video of your child communicating today — whatever modality they're using. Compare it to where you started. That delta is your evidence.
💛 Celebrate as a Family
This isn't just your child's achievement — it's yours, your partner's, your family's. Acknowledge what this took.
"From fear to mastery. One technique at a time."

🚩 Red Flags — When to Pause and Seek Immediate Help
PAUSE the materials and CONTACT your medical team if you observe any of the following.
🔴 Stop & Call Now
- New regression: Additional skills disappearing beyond the initial language loss
- Seizure signs: Staring spells, unusual eye movements, repetitive involuntary body movements (Landau-Kleffner must be ruled out)
- Medical symptoms: New fever, lethargy, vomiting, or sudden behavioral changes
- Complete withdrawal: Child stops all communication — no gestures, no eye contact, no response to name
- Self-injury: Head banging, biting, scratching that is new or increasing
🟡 Consult Your Team
- Increasing distress: Sessions are causing MORE dysregulation, not less, after 3+ weeks
- Persistent difficulty with any specific material after multiple modified attempts
- Regression in skills that had appeared to be returning
📞FREE National Autism Helpline: 9100 181 181 (24/7 • 16+ languages)
The Progression Pathway — Where This Leads
This technique is one node in a larger clinical pathway. Understanding where B-129 sits helps you and your team plan what comes next.
Related Techniques in Language & Communication
Many techniques in this domain use the same 9 materials in different configurations. You may already own everything you need.
Technique | Level | Difficulty | Materials Overlap | |
B-128: No Words by 18 Months | Intro | ⭐⭐⭐ | High | |
B-130: Social Skill Regression | Core | ⭐⭐ | Moderate | |
B-131: Play Skill Regression | Core | ⭐⭐ | Moderate | |
K-881: Parents After Diagnosis | Support | — | — | |
K-890: Coping with Regression | Support | — | — | |
K-960: Supporting Communication at Home | Core | ⭐⭐⭐ | High |
"You already own materials for these" — many techniques in this domain use the same 9 materials in different configurations.
Your Child's Full Developmental Map
This technique addresses one domain in your child's developmental landscape. Language doesn't develop in isolation — it connects to everything.
Communication Readiness Index
Currently tracking on GPT-OS® — verbal + AAC + gesture integration
Cross-Domain Interaction Map
How speech-language connects to sensory, motor, social, and emotional regulation
Full Profile on GPT-OS®
AbilityScore® across all 12 domains. 591+ structured observations.
📎 References: WHO/UNICEF Nurturing Care Framework — five components of nurturing care | UNICEF 2025 Country Profiles
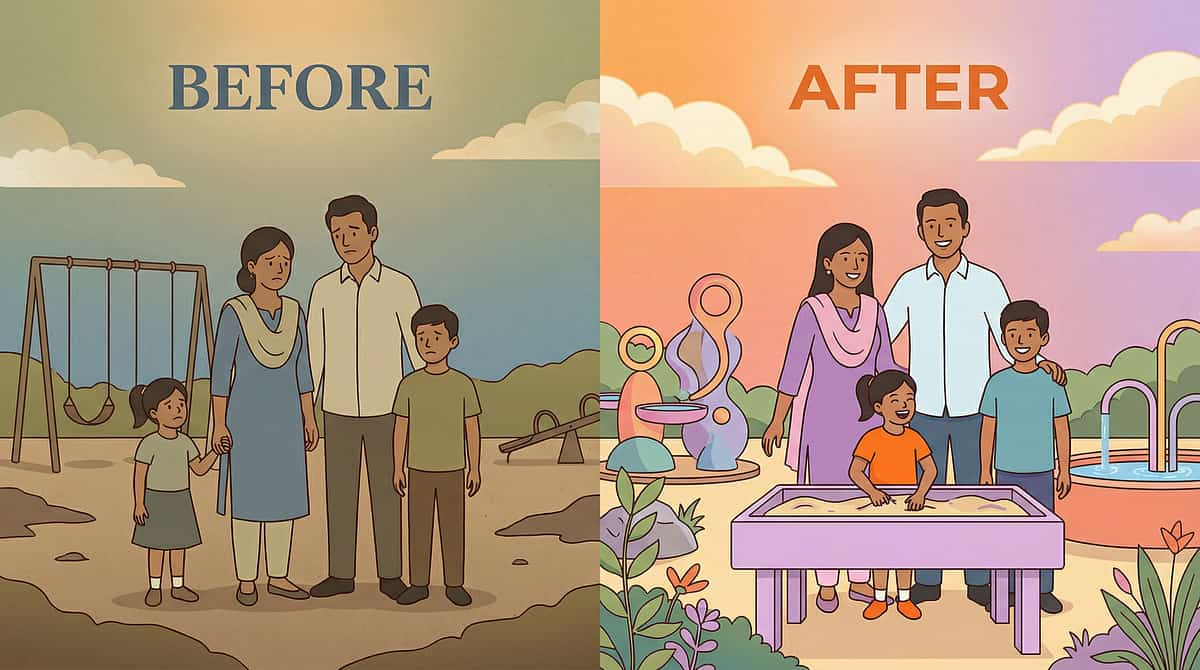
Families Who've Been Here
Family A — Chennai
"When our son lost his words at 20 months, we were devastated. He had said 'mama,' 'papa,' 'ball,' and then everything went silent. The team at Pinnacle helped us start with a simple AAC board — just photos of our family members. Within two weeks, he was pointing to my photo and making a sound. It wasn't 'mama' yet, but it was HIM communicating. Six months later, words started coming back."
Family B — Hyderabad
"My daughter lost about 15 words between 18 and 20 months. Music was our bridge. She wouldn't look at AAC boards initially, but she would sing along to 'Twinkle Twinkle' — the melody was still there even when the words weren't. Her SLP used that as the entry point, and gradually the melodies became words again."
Family C — Remote Village, Telangana
"We couldn't afford therapy toys. The Pinnacle team showed us over phone — use your family photos, use your cooking pots as drums, use the swing at the park. We did everything DIY. My grandson is now pointing at things and making sounds. We are traveling to the city for proper evaluation next month."
Illustrative cases; outcomes vary significantly. Medical evaluation is essential for all children experiencing language regression.

Connect With Other Parents
"Isolation is the enemy of adherence. You don't have to do this alone."
Language Regression Parent Support Group (WhatsApp)
Connect with other families navigating word regression. Share what's working, ask questions, find hope in real-time peer support from parents who understand exactly where you are.
Pinnacle Parent Community Forum
Moderated by clinical staff. Topic-specific threads. Evidence-checked responses. A safe space to ask your most vulnerable questions.
Peer Mentoring
Connect with an experienced parent who has navigated language regression and come out the other side — someone who has been exactly where you are right now.
Local Pinnacle Parent Meetups
Monthly gatherings at your nearest Pinnacle center. Bring your child — integrated play sessions while parents connect and share strategies.
"Your experience helps others — consider sharing your journey when you're ready."
Your Professional Support Team
"Home + Clinic = Maximum Impact"
🏥 Find Your Nearest Pinnacle Blooms Center
70+ centers across India. Each staffed with SLP, OT, BCBA, Special Educator, and NeuroDevelopmental Pediatrician working as an integrated consortium.
Center Locator →
Center Locator →
📱 Teleconsultation
Remote? Rural? International? Book a video consultation with a Pinnacle specialist from anywhere in the world.
Book Teleconsult →
Book Teleconsult →
📞 FREE National Autism Helpline
9100 181 181 — 24/7 • 16+ Languages
For regression: CALL IMMEDIATELY. Don't wait for online scheduling.
For regression: CALL IMMEDIATELY. Don't wait for online scheduling.
Relevant Pinnacle Services for Language Regression: Comprehensive Developmental Evaluation | Speech-Language Evaluation | Neurological Referral Coordination | AAC Evaluation and Training | ABA Therapy | Speech Therapy | Occupational Therapy | Parent Support Services
The Research Behind These Recommendations
Deeper reading for the curious parent and the clinical professional.
📄 PRISMA Systematic Review (2024) — PMC11506176
16 articles confirm sensory integration intervention meets evidence-based practice criteria for children with ASD. Strong methodological rigor across included studies.
📄 Meta-Analysis (World J Clin Cases, 2024) — PMC10955541
Sensory integration therapy effectively promoted social skills, adaptive behavior, sensory processing, and motor skills across 24 studies.
📄 WHO Care for Child Development Package (2023) — PMC9978394
Age-specific, evidence-based recommendations for caregivers. Implemented in 54 LMICs. Home-based caregiver-delivered interventions demonstrate comparable or superior outcomes to clinic-only delivery.
📄 Romski & Sevcik (2005)
AAC supports language development. Does NOT prevent verbal speech return. Foundational evidence for the AAC-first approach used in Material #1.
📄 NCAEP Evidence-Based Practices Report (2020)
National Clearinghouse classifying evidence-based practices for autism, including visual supports, video modeling, AAC, and naturalistic developmental behavioral interventions.
📄 Adapted WHO/UNICEF Nurturing Care Framework for SLPs (2022)
DOI: 10.1080/17549507.2022.2141327 — Framework for applying nurturing care principles in speech-language pathology practice.
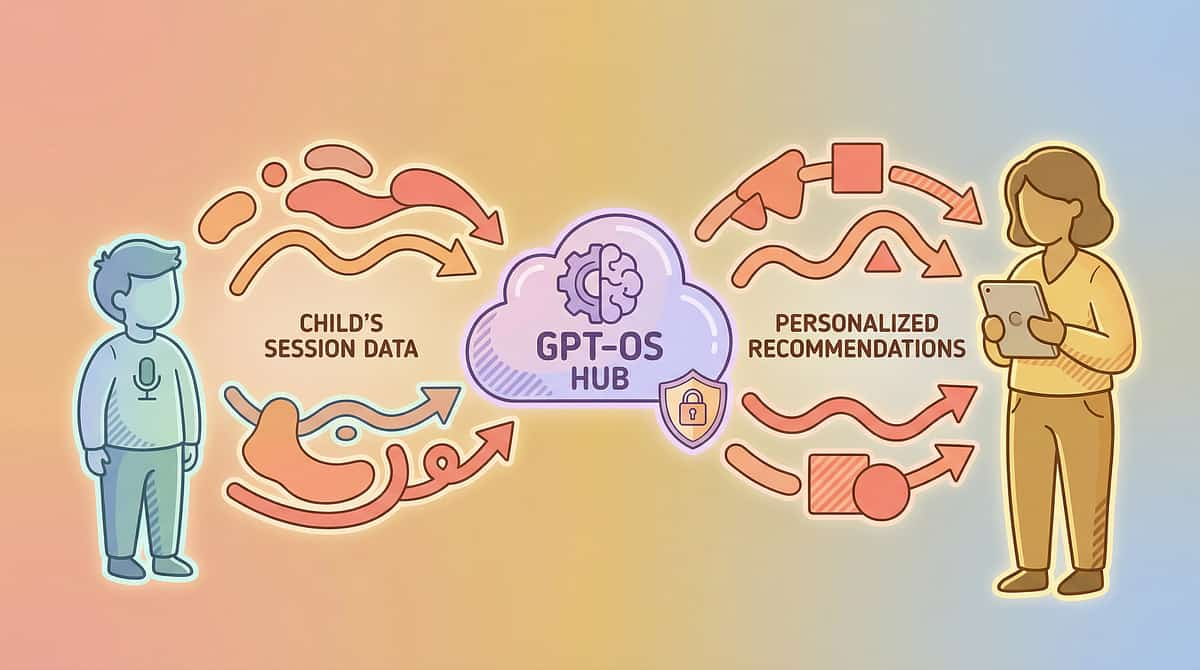
How GPT-OS® Uses Your Data
01
Diagnostic Intelligence Layer
591+ structured observations across 349 skills. AbilityScore® — Universal developmental score (0–1000).
02
Prognosis Engine
Predicts trajectories from 21M+ real therapy sessions. TherapeuticAI® determines therapy focus, intensity, and sequencing.
03
EverydayTherapyProgramme™
Translates clinical plans into daily home activities. FusionModule™ coordinates speech, OT, behavior, and special education inputs.
04
Closed-Loop Control
Observe → Score → Plan → Execute → Re-measure → Adapt. For language regression: tracks Communication Readiness Index, Caregiver Dependence Reduction Index, and Multimodal Communication sub-index.
Privacy: Your child's data is encrypted, HIPAA-compliant, and used only to improve YOUR child's care and the collective evidence base. You control your data. "Your data helps every child like yours."
Watch the Reel — B-129
Episode B-129
Regression and Developmental Concerns Series
Duration: 75 seconds
📺 "9 Materials That Help After Word Regression"
Pinnacle Blooms Network — Therapeutic Reels Series. A Pinnacle therapist walks through each of the 9 materials, demonstrating how to use them with a child experiencing language regression.
What you'll see: Watch how the therapist reads the child's cues, how materials are presented without pressure, and how every communicative attempt is celebrated. See how session flow moves from invitation through cool-down in real time.
"9 Materials That Help After Word Regression — watch, learn, and feel empowered to start today."
📎 References: NCAEP (2020) — Video modeling classified as evidence-based practice for autism. Multi-modal learning (visual + text + demonstration) improves parent skill acquisition.
Share This With Your Family
"Consistency across caregivers multiplies impact."
Share This Page
Send via WhatsApp, email, or copy the link. Every caregiver who reads this can support your child's communication with the same evidence-based approach you're using.
📄 Downloadable Family Guide (1-page PDF)
Everything on this page distilled into a single printable sheet. Put it on the fridge so every caregiver in your home can reference it at a glance.
👴👵 "Explain to Grandparents" Version
Core message: "Your grandchild has lost some words. We are working to rebuild communication. Use these pictures, sing familiar songs, play simple games together — and don't pressure them to 'say it.' Every point, every gesture, every sound is progress. Celebrate those."
👩🏫 Teacher/School Communication Template
Letter to share with daycare, preschool, or school explaining what language regression means, what the child needs, and how staff can support communication using the same 9 materials.
📎 References: PMC9978394 — WHO CCD Package emphasizes multi-caregiver training for intervention generalization

Frequently Asked Questions
Will my child's words come back?
Many children do regain verbal language, particularly with early intervention, appropriate medical treatment, and consistent communication support. The timeline varies significantly. Regardless, your child CAN communicate effectively through multiple modalities while verbal recovery proceeds.
Does using AAC prevent speech from returning?
No. Research conclusively shows that AAC supports and often accelerates verbal language development. Do NOT withhold AAC in hopes of "motivating" speech.
Should I stop talking to my child if they've lost words?
Absolutely not. Continue talking, narrating, singing. Your child's comprehension often remains intact. Your language input builds the foundation for verbal return.
Is this my fault? Did I cause regression?
No. Language regression has neurological, not parenting, causes. There is nothing you did or didn't do. The causes are biological, and the research is unambiguous on this.
How urgent is the medical evaluation?
Very urgent. Regression can indicate treatable conditions. Do not delay medical evaluation while using these materials. These materials are SUPPORT while you pursue answers — not a substitute.
Can I use these materials alongside formal therapy?
Yes, absolutely. These materials are designed to extend therapy into your home. Share your data with your Pinnacle therapy team to ensure alignment and avoid conflicting approaches.

Your Next Step — Start Now
"You arrived scared. You leave empowered. Now act."
📞 PRIMARY ACTION — Call the FREE Helpline NOW
9100 181 181 — 24/7 • 16+ Languages
For regression: immediate evaluation is essential. Don't wait for online scheduling.
For regression: immediate evaluation is essential. Don't wait for online scheduling.
📋 Book a Comprehensive Developmental Evaluation
Schedule at your nearest Pinnacle Center — in-person or via teleconsultation. The consortium team will map your child's full profile and design an integrated intervention plan.
➡️ Explore the Next Technique
B-130: Supporting Social Skill Regression — the natural next step for many families navigating this journey.
🏛️Validated by the Pinnacle Blooms Consortium
SLP • OT • BCBA • Special Educator • NeuroDevelopmental Pediatrician
Standardized. Personalized. Evidence-Based.
SLP • OT • BCBA • Special Educator • NeuroDevelopmental Pediatrician
Standardized. Personalized. Evidence-Based.
Preview of 9 materials that help after word regression Therapy Material
Below is a visual preview of 9 materials that help after word regression therapy material. The pages shown help educators, therapists, and caregivers understand the structure and content of the resource before use. Materials should be used under appropriate professional guidance.




















Link copied!
The Pinnacle Promise
Pinnacle Blooms Consortium
Speech-Language Pathology • Occupational Therapy • Applied Behavior Analysis • Special Education • NeuroDevelopmental Pediatrics
"From fear to mastery. One technique at a time."
⚕️IMPORTANT MEDICAL DISCLAIMER: Language regression requires comprehensive medical and developmental evaluation. This content is for educational purposes and does NOT replace professional assessment, diagnosis, or treatment. Regression may indicate neurological, metabolic, or developmental conditions requiring medical attention. Please consult a developmental pediatrician, neurologist, and other specialists immediately if your child is experiencing language regression. These materials support communication while evaluation proceeds — they are not a substitute for diagnosis and treatment. Individual outcomes vary. All clinical claims are based on published research and Pinnacle Blooms Network aggregate data; individual results depend on multiple factors including medical diagnosis, intervention intensity, and biological factors.
© 2026 Pinnacle Blooms Network®. All Rights Reserved. Powered by GPT-OS® — Global Pediatric Therapeutic Operating System
Technique ID: B-129 | Domain: SLP-REG-CR | Version: 1.0 | Patents filed across 160+ countries.
Technique ID: B-129 | Domain: SLP-REG-CR | Version: 1.0 | Patents filed across 160+ countries.
Explore Techniques
Pinnacle Ecosystem
Legal
Built by Mothers. Engineered as a System. Powered by GPT-OS®.
techniques.pinnacleblooms.org
techniques.pinnacleblooms.org