
The fire alarm went off. He dropped his device and ran. For 23 minutes, my nonverbal son could not tell anyone his name.
You are not failing. Your child's communication system has a single point of failure that no one warned you about.
Pinnacle Blooms Network® Consortium
SLP · OT · ABA · SpEd · NeuroDev
Communication Access & AAC Series — Episode B-230
📞 FREE National Autism Helpline: 9100 181 181 | 16+ languages | 24×7
WHO NCF 2018 · PMC11506176 · 20M+ therapy sessions · 97%+ measured improvement
Every AAC User Is One Dead Battery Away from Silence
You are among millions of families navigating this exact vulnerability. Emergency communication failure is not a rare edge case — it is the default state for most AAC-using families. The gap between technology-dependent communication and disaster-proof communication is where this page lives.
1 in 54
Children with Autism
Diagnosed with autism in India (2023). Source: NIMHANS National ASD Survey
30%
Minimally Verbal
Of autistic children remain minimally verbal or nonverbal. Source: JAMA Pediatrics, 2021
0
Emergency Backups
Emergency AAC backup systems most families currently have. Source: Pinnacle Clinical Audit, 2024
Systematic review (Children, 2024 — PMC11506176): 80% of children with ASD display communication difficulties. Emergency communication access gaps are documented across all AAC user populations. ISAAC position statement (2021) identifies emergency AAC preparedness as a critical unmet need.
Emergency Communication Readiness Is a Developmental Milestone
Emergency communication readiness typically becomes clinically relevant between ages 6–10, as children begin entering higher-risk environments: public schools, community outings, extracurricular programs. This is the window when the gap between primary AAC fluency and emergency backup capability becomes most dangerous.
1
Early AAC
18m–3yr: First symbols, device introduction, foundational communication
2
Device Fluency
3–6yr: Navigation, vocabulary expansion, routine communication
3
Emergency Awareness
6–10yr: ← This page addresses this window. Backup systems become critical.
4
Crisis Independence
10–14yr: Self-directed emergency communication, community scenarios
5
Community Safety
14–18yr+: Fully self-advocating, system maintenance, autonomy
Children who benefit most also commonly present with: sensory processing differences, epilepsy/seizure disorders, elopement history, and reduced verbal output under stress. Goal: From communication-vulnerable → communication-capable across all scenarios.
WHO Care for Child Development Package (2023) | UNICEF MICS 2025 | PMC9978394

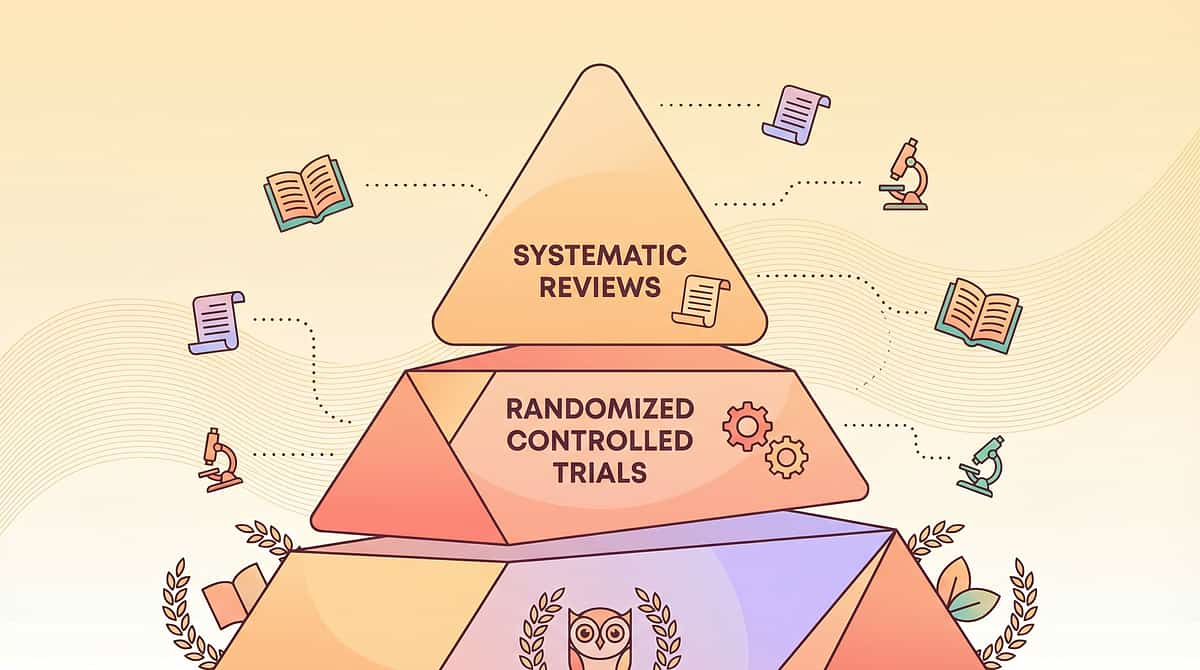
This Is Not Cautious Parenting. This Is Evidence-Based Practice.
LEVEL II EVIDENCE
Systematic Reviews + Expert Consensus + RCT-Supported Principles
NCAEP 2020
National Clearinghouse on Autism Evidence and Practice classifies visual supports and low-tech AAC backup systems as evidence-based practices for autism. Emergency AAC falls within this classification.
ISAAC 2021
The International Society for AAC explicitly identifies emergency preparedness as a critical AAC service delivery component, insufficient in current practice globally.
PMC11506176 (2024)
16 studies confirm AAC intervention as evidence-based practice. Low-tech backup systems are included in comprehensive AAC service delivery models.
WHO NCF + UNICEF
Communication access during emergencies is identified as a right, not a preference. Emergency preparedness is embedded in the Nurturing Care Framework's safety and security component.
"Clinically validated. Home-applicable. Parent-proven. Emergency communication cannot have a single point of failure."
Emergency AAC Preparation: The Complete Definition
Domain B: Communication
AAC-EMERG
Safety Communication
Formal Name
Emergency Augmentative and Alternative Communication Preparedness System
Parent-Friendly Alias
"Communication that can't fail" · "The backup voice system"
Definition
Emergency AAC preparation is the clinical practice of building redundant, durable, pre-positioned communication systems that function when a child's primary AAC device is unavailable, damaged, or inaccessible. It encompasses low-tech backups, wearable identification, medical communication, first responder interfaces, and systematic practice — all designed to ensure communication access across every possible emergency scenario.
Specifications: Age 2–18+ years · Ongoing system · Review every 6 months · All environments
Canon Material Badges
Laminated Communication Cards
Medical ID Systems
Wearable Communication
Body Map Tools
Hospital Communication Boards
Five Disciplines. One Mission: Your Child's Voice Cannot Fail.
Speech-Language Pathology ⭐ PRIMARY
Primary authority on AAC system design, emergency vocabulary selection, and backup system specification. The SLP leads design of every layer of the emergency communication system.
Occupational Therapy
Wearable communication design, fine motor accessibility under stress, and sensory-safe material selection for all wearable and low-tech components.
ABA / BCBA
Behavioral emergency protocols, practice schedule design, and reinforcement strategies for emergency AAC use across all scenarios.
Special Education
School emergency protocol integration, staff training, and IEP emergency communication goals that give the system legal standing in school environments.
NeuroDev Pediatrics
Medical emergency communication coordination, hospital board specifications, and seizure/allergy protocol design for children with complex medical needs.
"This technique crosses therapy boundaries because emergencies don't respect therapy schedules. When a child is in crisis, the SLP's vocabulary, the OT's material design, the BCBA's practice protocols, and the NeuroDev doctor's medical specifications must all function simultaneously — in a laminated card the size of a credit card." — Pinnacle Blooms Network® Consortium

9 Materials. Zero Tolerance for Communication Failure.
When the device fails — and eventually, it will — these 9 materials ensure your child's voice remains intact. Each material serves a specific emergency function. Together, they form a redundant, layered communication safety system that no battery or broken screen can defeat.
# | Material | Function | Price | |
1 | Emergency ID Cards + Medical Alert Jewelry | Identity in 30 seconds | ₹500–3,000 | |
2 | Waterproof Low-Tech Communication Cards | Words that survive water + chaos | ₹200–1,000 | |
3 | Wearable Communication Strips + Bands | Vocabulary that can't be dropped | ₹300–1,500 | |
4 | Body Map Pain Communication Boards | Tell them where it hurts | ₹100–500 | |
5 | Emergency Vocabulary Programmed into AAC Device | One touch to crisis words | ₹0 | |
6 | Car + Go-Bag Communication Kits | Pre-positioned where emergencies happen | ₹500–2,000 | |
7 | First Responder Communication Cards | Instructions for police, fire, EMTs | ₹100–500 | |
8 | Hospital + Medical Procedure Communication Boards | Communication in healthcare settings | ₹200–1,000 | |
9 | Emergency Scenario Practice Materials | Train before it's real | ₹200–1,000 |

Material 1 of 9
Emergency ID Cards + Medical Alert Jewelry
What It Is
Physical identification that stays with the child regardless of device status — engraved bracelets, laminated cards, QR-coded tags — carrying name, emergency contacts, medical conditions, allergies, medications, and the critical statement: "I use AAC to communicate."
Why the Science Supports It
When an AAC user is found alone, separated, or unresponsive, first responders need three answers within 30 seconds: Who is this person? What do they need medically? How do I communicate with them? Medical alert systems are the only reliable answer when devices are absent, locked, or damaged.
The Outcome
A stranger finds your child alone, crying, unable to speak. They look at the wrist: ARJUN · I use AAC · Mom: 9876543210. They know what to do. They make the call. Your child is safe in under 2 minutes.
What · Why · Where · When · How
- WHAT: Engraved silicone/stainless ID bracelet + laminated emergency profile card
- WHY: Devices can be dropped, stolen, or dead. Wearable ID cannot be separated from the child
- WHERE: Always on child — wrist, backpack clip, shoe tag
- WHEN: 100% of the time when outside the home
- HOW: Engrave: Name · "I use AAC" · Emergency contact · Diagnosis. Link QR code to detailed profile.
💡DIY Version (₹0): Print card: Name + Photo + Emergency contact + "I communicate using AAC — please be patient and show me options." Laminate with packing tape (3 layers). Attach to backpack with zip tie. Update monthly.
⚠️Safety Note: Balance information access with privacy. Include what a stranger needs to help — not private behavioral data. QR codes can link to password-protected profiles for authorized responders.
Price: ₹500–3,000 | Search Amazon.in →
ASHA AAC Emergency Guidelines · NCAEP 2020 · PMC11506176

Material 2 of 9
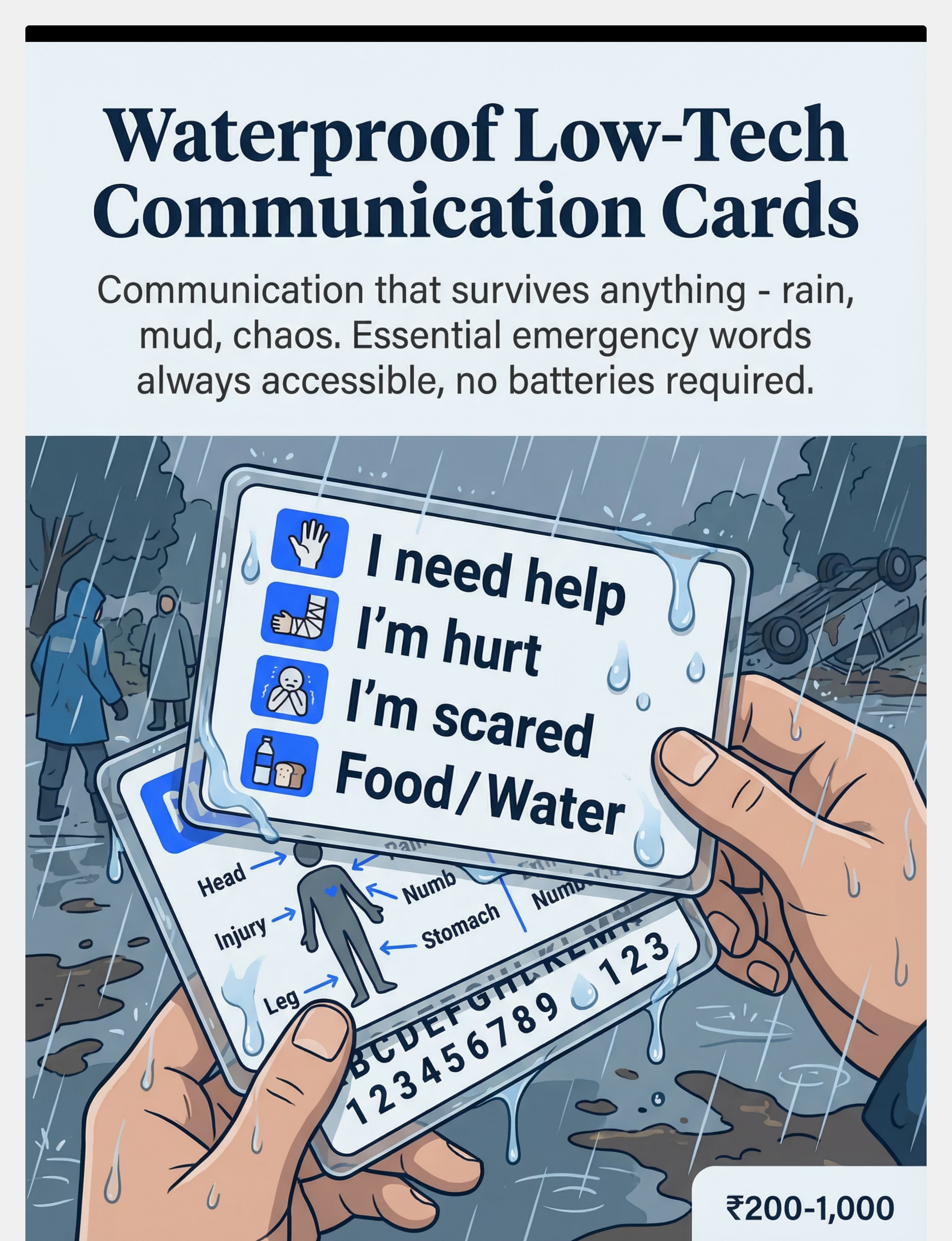
Waterproof Low-Tech Communication Cards
What It Is
Laminated or waterproof-material cards containing essential emergency vocabulary — "I need help," "I'm hurt," "I'm scared," "I can't breathe," "Call my parent" — along with body maps, yes/no, and basic needs. Functional in rain, mud, flood, and physical trauma scenarios.
Why the Science Supports It
High-tech AAC fails in water, extreme temperatures, and physical trauma — precisely the conditions defining most emergencies. Waterproof low-tech cards operate on zero power, require no boot time, and function under the degraded fine motor control that stress produces.
The Outcome
Flood evacuation. Device shorted out in the water. Your child holds up the waterproof card: I NEED HELP + body map pointing to leg. Rescuers respond immediately. The card worked when nothing else could.
What · Why · Where · When · How
- WHAT: Heavy laminated symbols + words for 12–20 critical emergency messages
- WHY: Devices are destroyed by water/heat/impact. Cards survive the conditions that cause emergencies
- WHERE: Attached to child (belt clip), go-bag, car kit, school locker
- WHEN: Activated when primary device is inaccessible, damaged, or dead
- HOW: Child points to symbol + word. No navigation. No power. Immediate.
Core vocabulary to include: Help · Hurt · Scared · Safe · Yes · No · Call Mom/Dad · I can't breathe · I need medicine · Body map
💡DIY Version (₹50): Print core vocabulary on A4 paper. Laminate with 5+ layers of packing tape OR place inside zipper freezer bag heat-sealed at edges. Test: submerge in water for 5 minutes. If readable, it works.
⚠️Safety Note: Test durability before trusting in emergencies. Submerge, bend, expose to heat. Weak points now prevent failures when it matters.
Price: ₹200–1,000 | Search Amazon.in →
NCAEP 2020 | ASHA Low-Tech AAC Guidelines | PMC9978394

Material 3 of 9
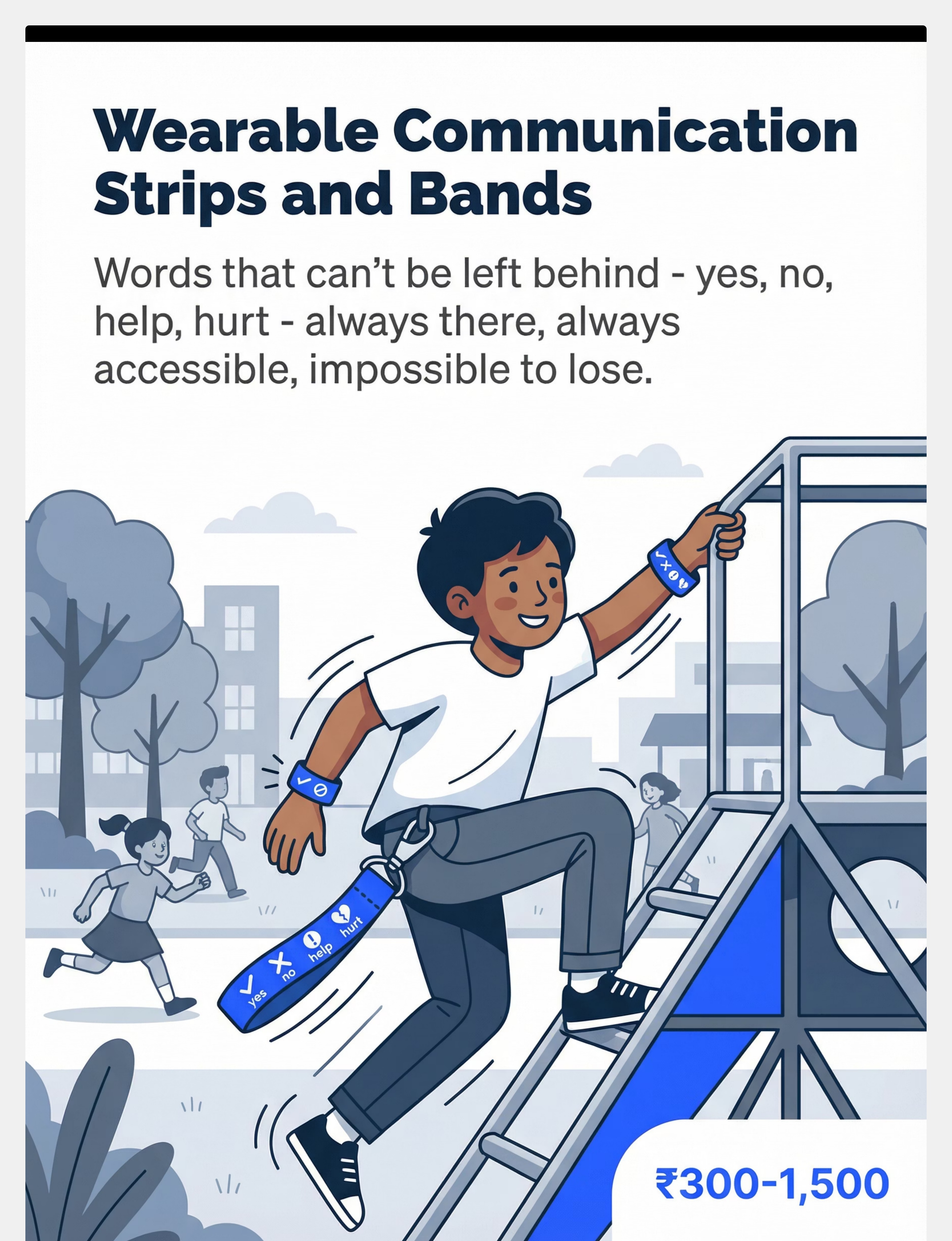
Wearable Communication Strips and Bands
What It Is
Fabric or silicone bands with printed core symbols, attached communication card strips, or custom-engraved wristbands — ensuring that essential vocabulary (yes, no, help, hurt, scared) is literally attached to the child's body and moves with them through running, falling, evacuation, and separation.
Why the Science Supports It
Communication that must be carried will be dropped. Communication that must be found will be lost. Communication that is worn stays with the person through every physical scenario. Wearable communication is the only format that guarantees vocabulary access when hands are covering ears, gripping railings, or being held by rescuers.
The Outcome
Fire drill chaos. Device on desk inside. Child outside, covering ears, stimming. Teacher approaches. Child raises wrist. Band shows: SCARED · HELP · NAME: PRIYA. Teacher knows who she is and what she feels. Priya was not alone.
What · Why · Where · When · How
- WHAT: Silicone/fabric wristband with symbols + words for 5–8 critical messages
- WHY: Under stress, children drop objects, leave bags, run without belongings. The body is the only reliable carrier
- WHERE: On wrist (non-dominant hand) at all times outside home
- WHEN: Full-time wearable during school, community, travel
- HOW: Child touches/points to symbol on band. Parent/responder reads aloud to confirm.
💡DIY Version (₹0): Write core vocabulary on surgical tape or fabric bandage. For more durable: sew symbols onto elastic band. Custom silicone wristband services widely available at ₹50–200.
⚠️Safety Note: Use breakaway attachments for anything near the neck. Wristbands must be comfortable for all-day wear — if uncomfortable, child will remove.
Price: ₹300–1,500 | Search Amazon.in →
OT wearable AAC literature | ASHA low-tech AAC | NCAEP 2020

Material 4 of 9
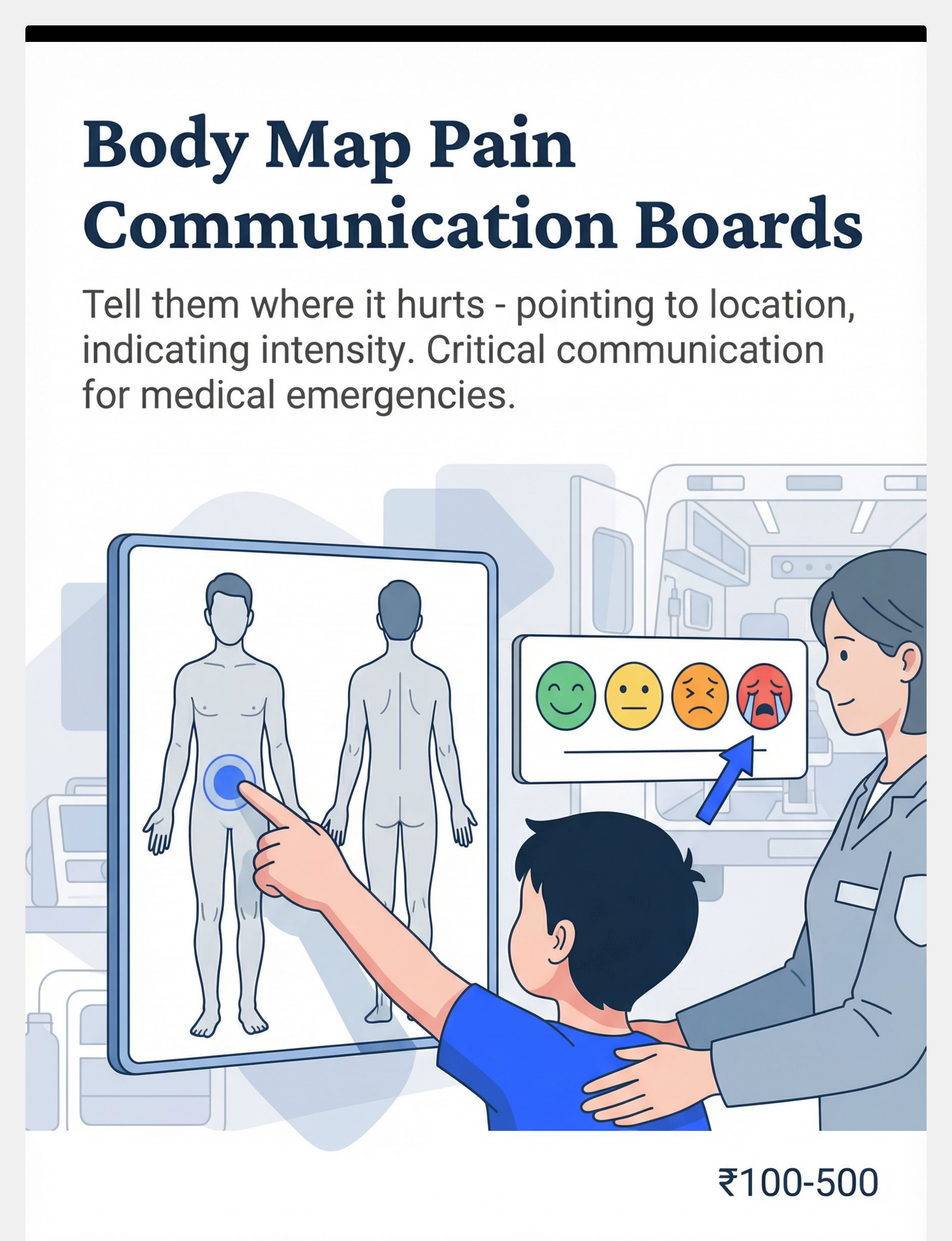
Body Map Pain Communication Boards
What It Is
Laminated boards showing front and back body outlines where the child points to indicate pain location, combined with pain intensity scales (faces 0–10) and pain type symbols. Essential for medical emergencies where accurate symptom communication determines treatment speed and accuracy.
Why the Science Supports It
AAC users who cannot verbally describe pain location experience delayed or incorrect medical treatment — a documented patient safety risk. Body maps convert the complex language requirement of pain description into a simple pointing task accessible even under significant cognitive and physical stress.
The Outcome
Your child has a fever at school, doubled over in pain but cannot speak. The nurse shows the body map. Child points: lower right abdomen. Intensity: maximum (crying face). The nurse calls you immediately: "possible appendicitis." The body map may have saved your child's appendix — or more.
What · Why · Where · When · How
- WHAT: A4 laminated body diagram (front + back) + pain scale (faces) + pain type symbols
- WHY: "Where does it hurt?" is an impossible question without this tool. A pointed finger answers in 2 seconds
- WHERE: Go-bag, medical bag, car kit, school health office
- WHEN: Any medical interaction — clinic visit, hospital, emergency, illness at school
- HOW: "Show me where it hurts." Child points. "Show me how bad." Child points to face scale.
💡DIY Version (₹0): Print free body outline images (search "body map pain scale children printable"). Add Wong-Baker FACES pain scale (freely available). Laminate with packing tape. Keep one copy in every relevant location.
⚠️Safety Note: Practice using body maps before emergencies. Children who have never used a body map in practice cannot reliably use one in crisis.
Price: ₹100–500 | Search Amazon.in →
PMC10955541 | Medical AAC literature | ASHA clinical guidelines
Material 5 of 9
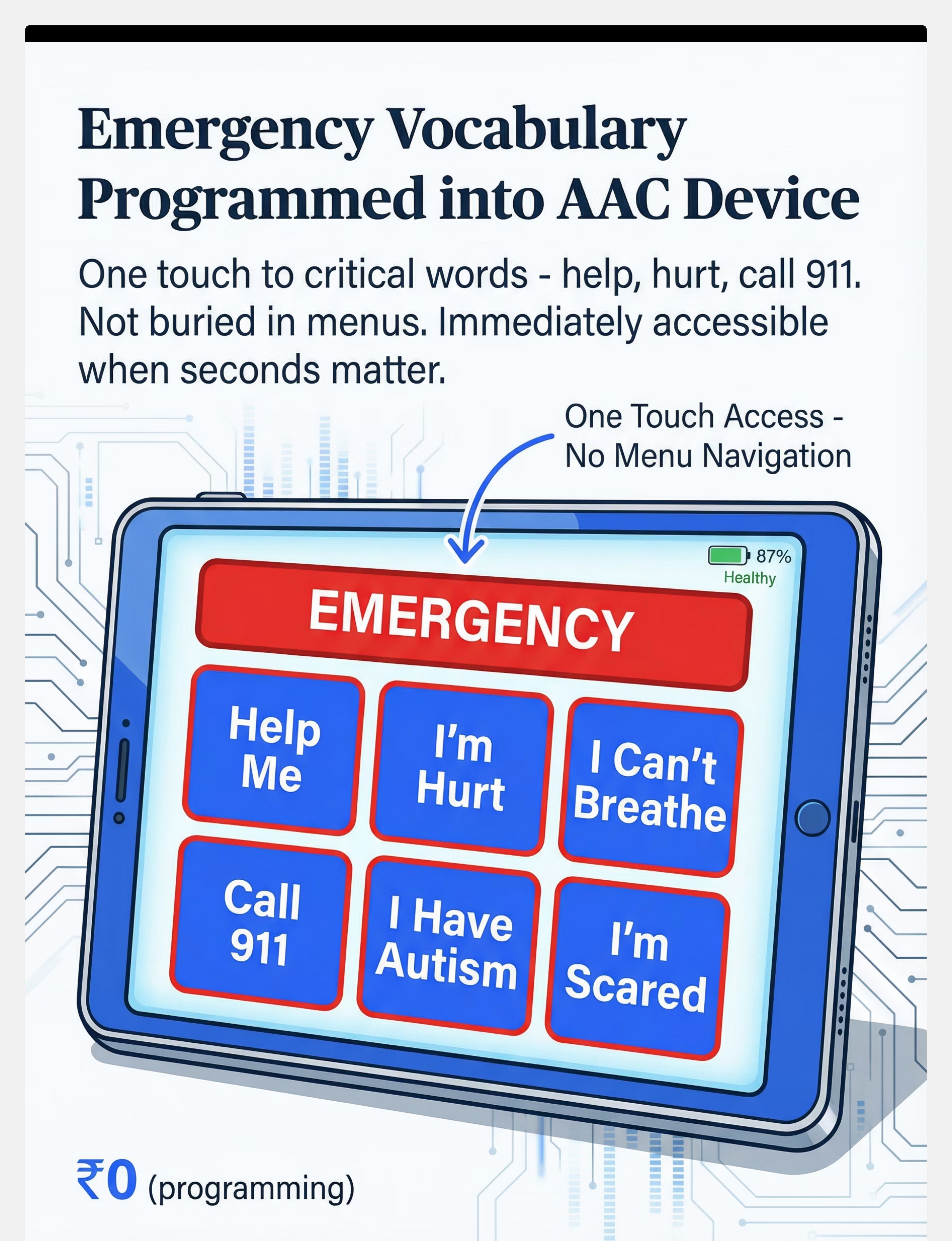
Emergency Vocabulary Programmed into AAC Device
What It Is
A dedicated emergency page or home-screen shortcut on the primary AAC device providing immediate, single-touch access to critical messages: "Help me," "I'm hurt," "I can't breathe," "I'm scared," "Call emergency," "I have autism," "I'm allergic to ____," "I take ____ medication" — without menu navigation.
Why the Science Supports It
When the AAC device is available, cognitive load under stress means the child cannot navigate complex menus. Emergency vocabulary buried 3 clicks deep is inaccessible vocabulary. Dedicated emergency pages eliminate navigation — one touch reaches the critical word.
The Outcome
Medical emergency at a mall. Child has their device. Panic prevents navigation. But the large red EMERGENCY button on the home screen is unmissable. One tap: "I NEED HELP. I HAVE EPILEPSY. CALL MY MOM: 9876543210." Mall security reads the screen and makes the call in 10 seconds.
What · Why · Where · When · How
- WHAT: Custom emergency page on AAC device with 6–8 critical messages + medical info
- WHY: Standard AAC navigation requires executive function that stress disables. One-touch emergency bypasses this
- WHERE: Home screen or dedicated physical button on device
- WHEN: When device is present but standard navigation is too complex under stress
- HOW: Large EMERGENCY button on home screen → Help / Hurt / Scared / Call Parent / I have autism / I need medicine
💡DIY Version (₹0 — programming time only): In Proloquo2Go, TouchChat, LAMP, Snap Core First, or LetMeTalk: Create page "EMERGENCY." Add large-format buttons: Help Me · I'm Hurt · I'm Scared · Call [parent] · I Have [diagnosis] · I'm Allergic to [allergen] · I Need My Medicine · I Use AAC To Talk. Set as home screen shortcut. Test monthly.
⚠️Safety Note: Device programming is ESSENTIAL but is a complement to low-tech backups, not a replacement. When the device is unavailable, this card is irrelevant.
Price: ₹0 (uses existing device) | ASHA AAC App Resources →
NCAEP 2020 | ASHA AAC Practice Portal | Digital health AAC systematic reviews (2024)

Material 6 of 9
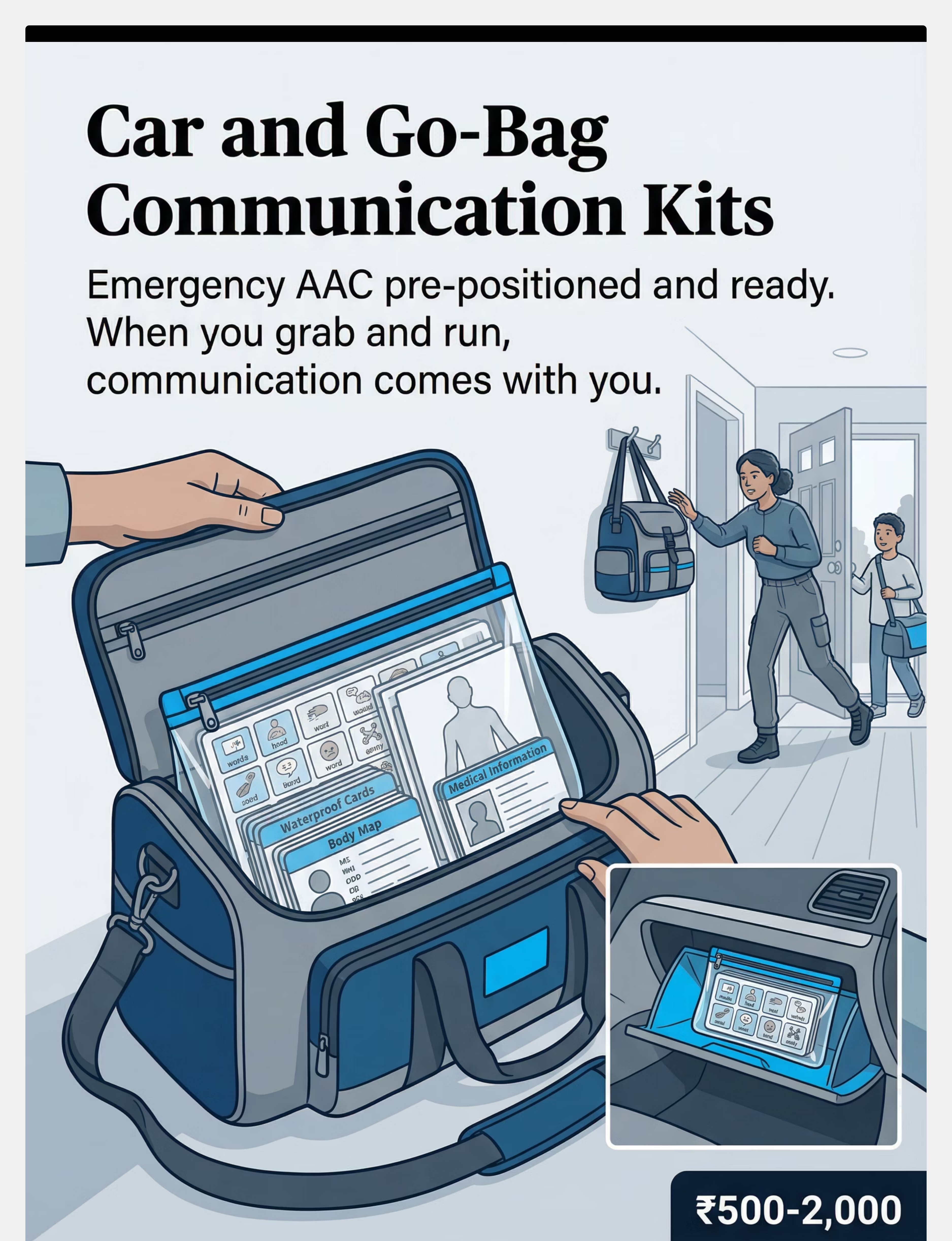
Car + Go-Bag Communication Kits
What It Is
Pre-assembled, waterproofed emergency AAC kits pre-positioned at exit points: one go-bag by the front door for evacuation, one car kit in the vehicle, one school backup. Each contains: duplicate low-tech communication boards, emergency ID copies, medical information card, body map, first responder instruction card, pen + paper, and a current photo of the child.
Why the Science Supports It
You cannot think clearly during emergencies. Pre-positioned kits remove the "what do I pack?" question from the crisis moment. Families who have experienced emergency communication failure uniformly identify pre-positioned kits as the single most effective preparation strategy.
The Outcome
2 AM: gas leak in the building. Evacuation in under 3 minutes. You grab the bag by the door. Inside: everything your child needs to communicate with any responder, any doctor, any stranger. Nothing was forgotten because nothing needed to be packed in the dark at 2 AM.
Kit Contents Checklist
- Duplicate low-tech communication cards
- Emergency ID card (copy)
- Medical information card (conditions, medications, allergies)
- Body map
- First responder instruction card
- Current photo of child
- Emergency contacts (handwritten)
- Pen + paper
- Small amount of cash (₹500)
Locations: Front door hook · Car glove compartment · School office/locker
💡DIY Version (₹100–200): Assemble all printed/laminated materials in a large zip-lock bag or small waterproof pouch. Store in visible location at door. Review biannually.
⚠️Safety Note: Check kits every 6 months. Outdated contacts and photos can cause dangerous confusion during emergencies.
Price: ₹500–2,000 | Search Amazon.in →

Material 7 of 9
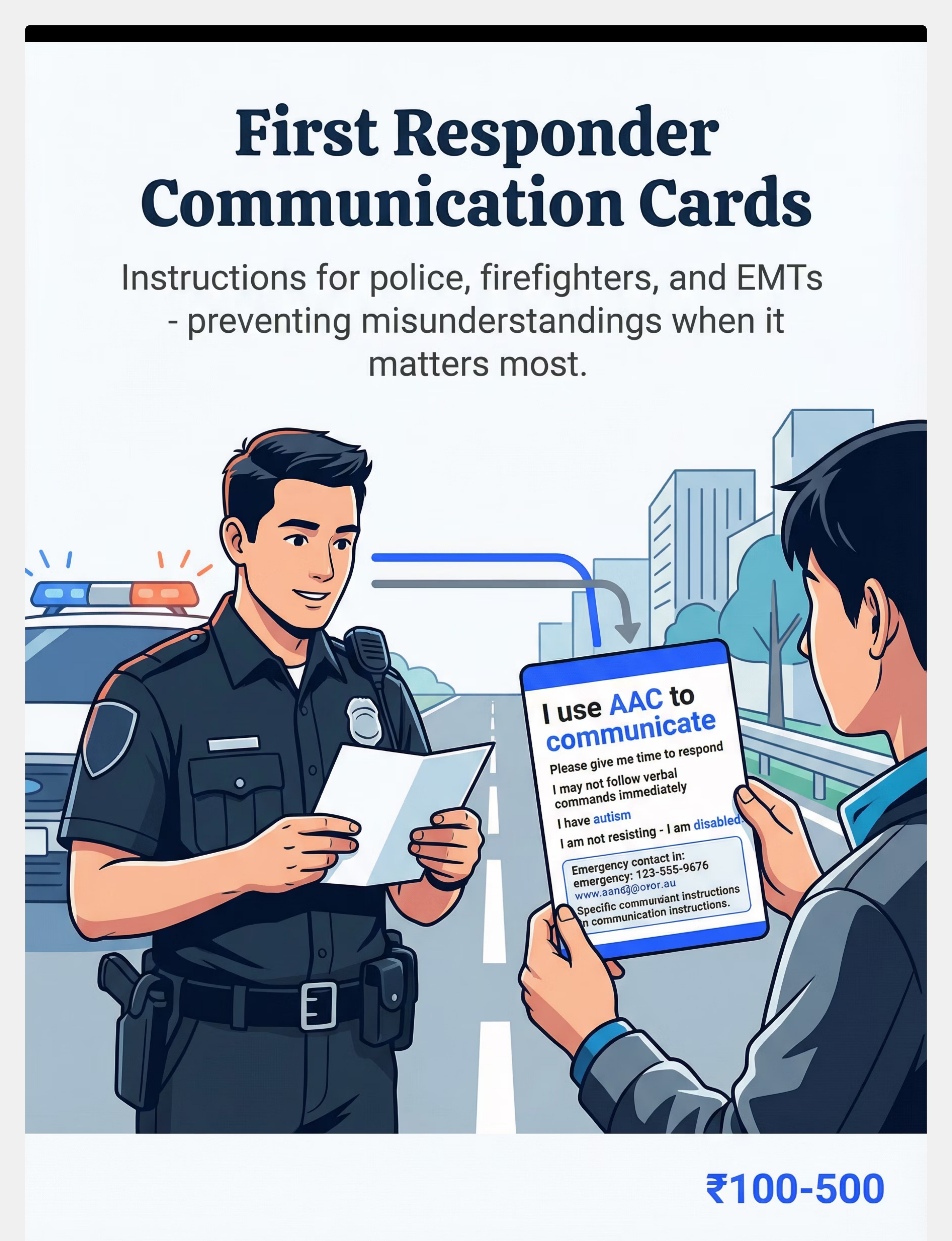
First Responder Communication Cards
What It Is
Professional-format cards designed specifically for police, firefighters, and EMTs that explain: "I use AAC to communicate. Please give me time to respond. I may not follow verbal commands. I have autism and may behave unexpectedly. I am not resisting — I am disabled. Here is how to communicate with me effectively."
Why the Science Supports It
First responders receive minimal training in disability communication and can misinterpret non-compliance, non-response, or atypical behavior as intoxication, aggression, or resistance — creating dangerous escalation. Responder cards prevent this misunderstanding by providing context before the interaction deteriorates.
The Outcome
Police encounter. Child bolts in a crowded market, found alone by officers. Child doesn't respond to "what's your name?" Officer sees card attached to backpack. Reads: "I use AAC. I have autism. Please call 9876543210." No escalation. No misunderstanding. Child protected.
Card Content Template
I USE AAC TO COMMUNICATE
Please give me TIME to respond
I may NOT follow verbal commands immediately
I am NOT resisting — I have AUTISM
I am NOT drunk or high — I am DISABLED
HOW TO COMMUNICATE WITH ME:
• Speak slowly · Use simple words · Show options
• Point to my communication card/device
• Wait 10 seconds for my response
EMERGENCY CONTACT: [Name] · [Phone]
DIAGNOSIS: [Autism Spectrum Disorder]
MEDICATIONS: [list] · ALLERGIES: [list]
COMMUNICATION METHOD: [AAC device / this card]💡DIY Version (₹10): Print template above. Laminate. Attach to backpack, school bag, and include in car kit and go-bag.
Price: ₹100–500 | Search Amazon.in →
ASHA first responder resources | Autism + law enforcement literature | NCAEP 2020

Material 8 of 9
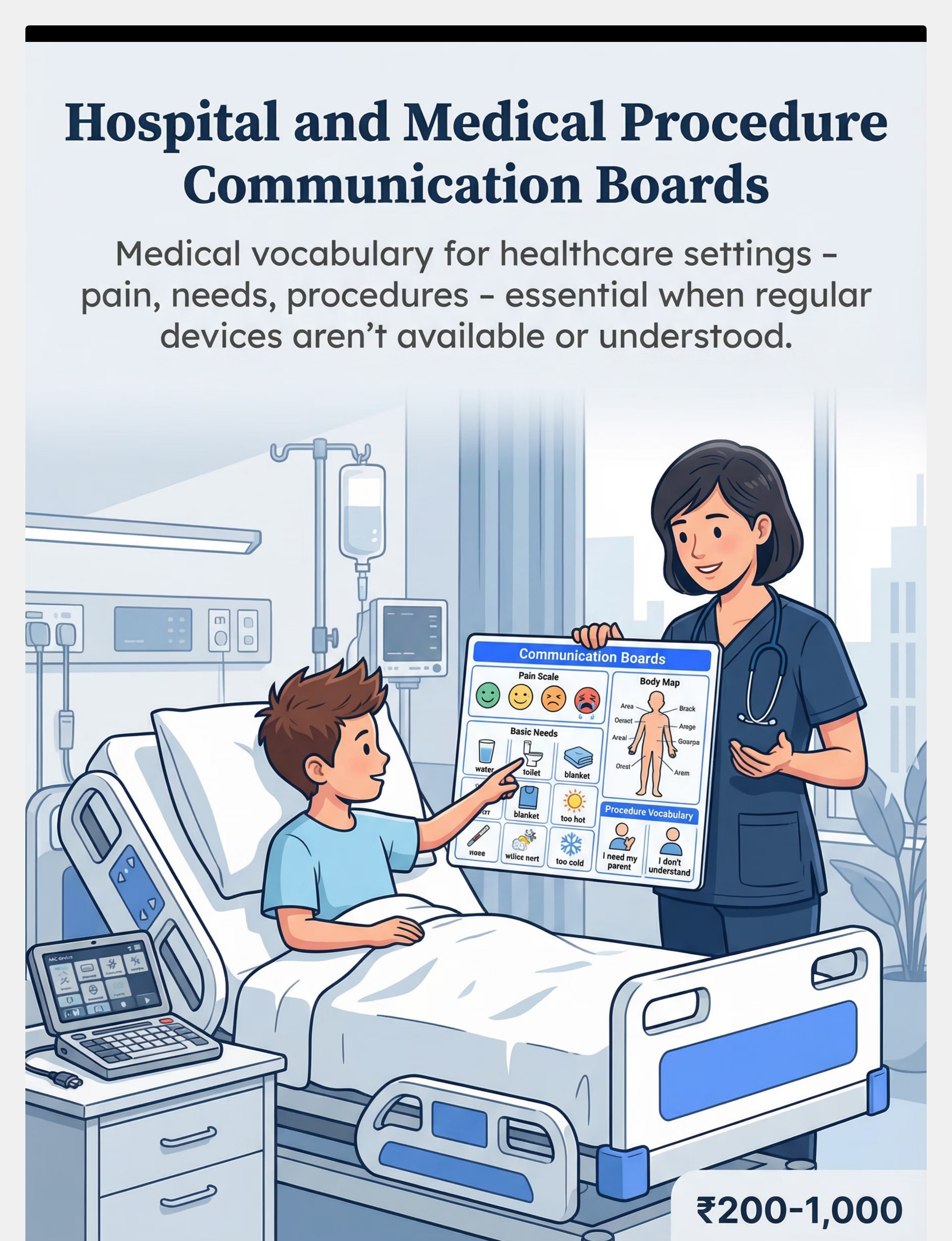
Hospital + Medical Procedure Communication Boards
What It Is
Specialized communication boards designed for medical settings — containing pain scales, procedure vocabulary, basic needs (water, bathroom, blanket, too hot, too cold), emotional states (scared, hurt, confused, I need my parent), and ways to indicate "I don't understand" or "stop." Designed to function with rotating medical staff who have no prior AAC knowledge.
Why the Science Supports It
Hospitals represent concentrated communication vulnerability: devices may not be allowed in sterile areas, may be lost during transfers, may not be charged during multi-day stays, and medical staff change each shift. Hospital boards ensure continuity of communication access regardless of staff familiarity.
Board Content
Pain Scale: 😊😐😣😢😭 (0–10) · Body Map: Front + Back · Basic Needs: Water · Bathroom · Blanket · Too Hot · Too Cold · Hungry · Tired · Emotions: Scared · Hurt · Confused · OK · I need my parent · I don't understand · STOP · Procedure: I don't want to · I need a break · I understand · Please explain
The Outcome
Emergency appendectomy. Child in pre-op, terrified, device left in locker. Different nurse every 30 minutes. Medical bag has the hospital board. Each nurse is shown the board on arrival. Child can indicate fear, pain, needs without a single word. Surgery proceeds safely.
What · Why · Where · When · How
- WHAT: A4 laminated board with pain scale · body map · basic needs grid · emotional states · procedure vocabulary
- WHY: Primary AAC may be unavailable. Hospital staff won't know your child's system. Board works immediately for all staff
- WHERE: Medical bag, go-bag — brought to EVERY medical appointment, procedure, hospital stay
- WHEN: Every clinical interaction where primary AAC may not be available
- HOW: "He uses this to communicate. Please use it with him." Present to each new staff member.
💡DIY Version (₹50): Print pain scale + body map + needs grid on A4 paper. Laminate with packing tape. Add to medical bag immediately.
⚠️Safety Note: Note AAC use prominently in medical records. Brief each incoming staff member — do not assume continuity of care.
Price: ₹200–1,000 | Search Amazon.in →
Medical AAC literature | ASHA hospital communication guidelines | PMC10955541

Material 9 of 9
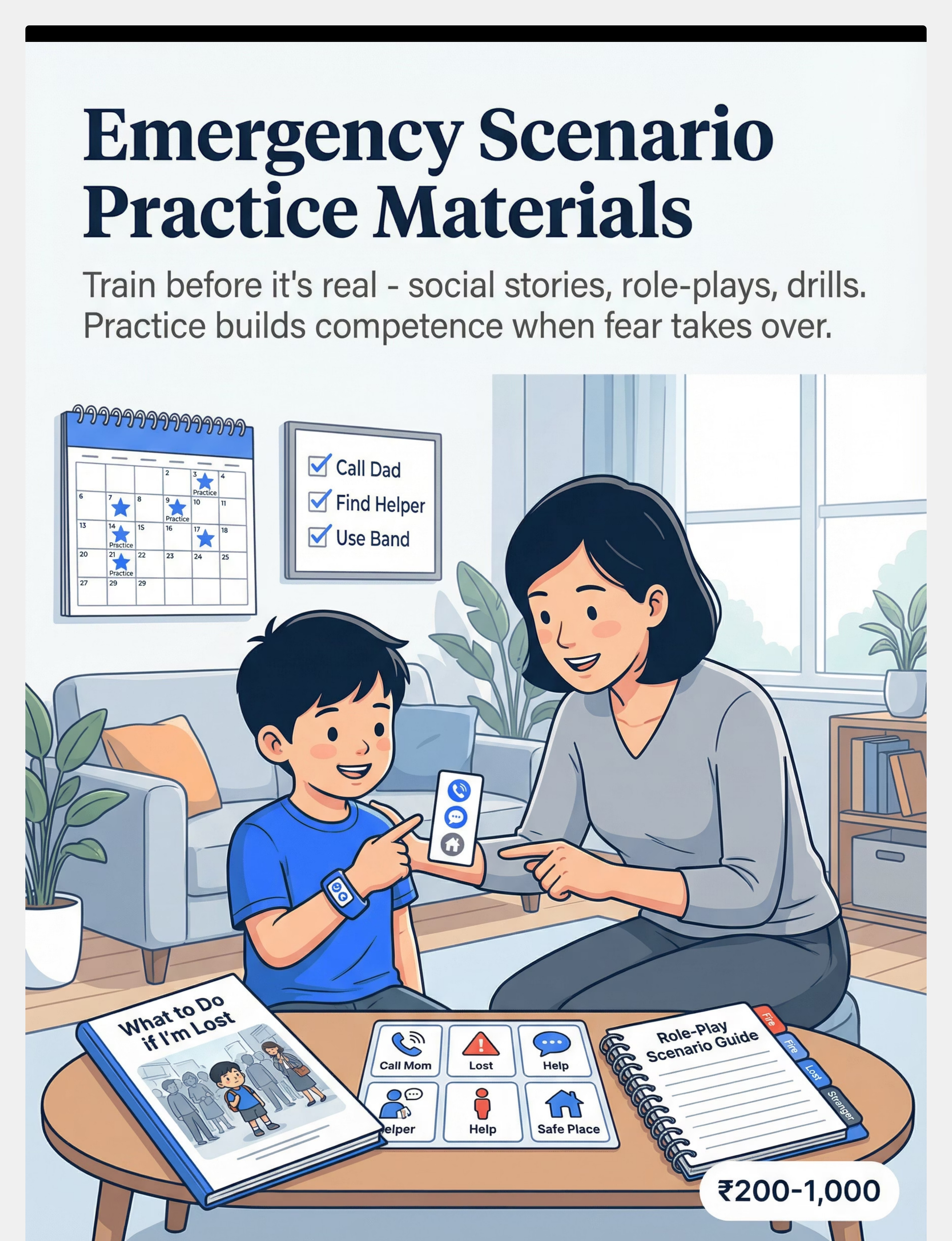
Emergency Scenario Practice Materials
What It Is
Social stories, role-play scripts, drill practice guides, and video models that train the child to use emergency AAC materials before emergencies occur. Includes scenario-specific stories: "What happens in a fire drill," "What to do if I'm lost," "What to do if I feel very sick," "How to show a police officer I need help."
Why the Science Supports It
Under stress, cognitive load increases and unfamiliar tasks become impossible. Skills practiced under calm, supported conditions transfer to crisis conditions. Children who have rehearsed emergency AAC use perform significantly better than those encountering materials for the first time in real emergencies.
Monthly Practice Schedule
- Week 1: "Fire Drill" — device-free evacuation with wearable communication
- Week 2: "Lost in Public" — using ID card with a 'stranger' (trusted adult)
- Week 3: "I Feel Sick" — body map use and first responder card
- Week 4: "Hospital Visit" — hospital board with parent as 'nurse'
The Outcome
Real fire at a shopping mall. Your child has practiced this monthly. They know: cover ears, stay near a wall, show the communication band. When found by security, they point to their wristband. Security reads the name and number. You receive the call within 4 minutes. The practice made it possible.
What · Why · Where · When · How
- WHAT: Social stories (print/digital) + role-play scripts + monthly practice schedule
- WHY: You don't learn during emergencies. You execute what you already practiced
- WHERE: Home, classroom, therapy session
- WHEN: Monthly minimum. Increase before high-risk periods (travel, public events)
- HOW: Read social story → Role-play scenario with positive reinforcement → Practice with actual emergency materials
💡DIY Version (₹0): Write simple social stories in first person: "My name is Kiran. If I am lost, I will find a person who looks safe. I will show them my wristband. My wristband has my name and my Amma's number." Practice monthly. Make it a game, not a threat.
⚠️Safety Note: Practice must be supportive, not frightening. Competence — not anxiety — is the goal. Adapt intensity to child's emotional capacity.
Price: ₹200–1,000 | Download free social story templates → | Search Amazon.in →
NCAEP 2020 (social narratives as EBP) | Video modeling literature | ABA practice principles

No Amazon Access Required. Every Material Can Be Made Today.
Per WHO/UNICEF Nurturing Care Framework, every intervention in this library has a ₹0 version. Emergency AAC preparation is too important to be gated by income.
Material | Commercial Version | DIY Version (₹0) | |
Emergency ID | Medical alert bracelet ₹500–3,000 | Laminated card + zip-tie to backpack strap | |
Waterproof Cards | Tyvek/synthetic cards ₹200–1,000 | Laminate with 5 layers packing tape. Test in water. | |
Wearable Band | Custom silicone wristband ₹300–1,500 | Write on surgical tape or fabric bandage | |
Body Map | Pre-printed laminated board ₹100–500 | Print from Google Images + laminate with tape | |
Device Emergency Page | ₹0 (programming time) | ₹0 — just needs programming time | |
Go-Bag Kit | Assembled kit ₹500–2,000 | Large zip-lock bag + printed materials | |
Responder Card | Professional laminated ₹100–500 | Print the template from Card 09-G | |
Hospital Board | Pre-printed board ₹200–1,000 | Print pain scale + body map + needs grid | |
Practice Materials | Commercial social stories ₹200–1,000 | Write your own. 1 paragraph. First person. |
The same emergency communication principle works whether the material costs ₹3,000 or ₹0. A laminated paper ID card saves lives. A ₹2,500 silicone bracelet also saves lives. Start with what you have. Build from there.

Read Before You Build. Safety Standards for Emergency AAC Materials.
🔴 STOP — Address These First
- Medical ID must be verified for accuracy — incorrect allergy/medication info is more dangerous than no ID
- Responder cards must NOT use confrontational language — cards that alarm responders create worse outcomes
- Wearable items must use breakaway mechanisms near the neck — strangulation risk is real
- Body maps must be practiced before emergency use — unpracticed tools fail under stress
🟡 CAUTION — Monitor and Manage
- Update all emergency materials every 6 months minimum (contacts, medications, photos change)
- Some children may find emergency practice scenarios distressing — calibrate intensity to emotional capacity
- QR codes on medical IDs must link to accurate, currently maintained profiles
🟢 PROCEED — Readiness Confirmed
- All materials contain accurate, current information ✓
- At least one wearable ID is on the child when outside the home ✓
- At least one low-tech backup is accessible at school ✓
- Emergency practice has been completed at least once ✓
- Family and school staff know the emergency AAC system exists ✓
🛑Stop Immediately if: Child shows extreme distress during emergency practice (adjust, do not push) · ID material contains outdated emergency contacts (update before next outing) · Device emergency page has not been tested recently (test today)
📞 9100 181 181 — Helpline for professional safety guidance | Indian Journal of Pediatrics RCT (2019) DOI: 10.1007/s12098-018-2747-4

Before Each Emergency Practice Session — The 5-Point Check
This card applies to emergency PRACTICE sessions — the scheduled drills and role-plays that build competence. Use this before intentional practice, not before actual emergencies (which don't wait for readiness).
Indicator | ✅ Go | ⚡ Modify | ❌ Postpone | |
Child is regulated (calm baseline) | Yes | Mildly elevated | Dysregulated | |
Child is rested | Yes | Somewhat tired | Exhausted | |
No recent meltdown (past 2 hours) | Clear | 2–4 hours ago | Within 2 hours | |
Child not hungry/thirsty | Fed | Slightly hungry | Very hungry | |
Child not showing illness signs | Healthy | Mild sniffles | Clearly unwell |
✅ If GO
Proceed with practice scenario as planned. Keep tone playful and supportive.
⚡ If MODIFY
Use a shorter, simpler version. Focus on just one material (e.g., just the ID card). Limit to 5 minutes.
❌ If POSTPONE
Do a positive activity instead. Reschedule practice. Note: actual emergencies don't wait — this check is ONLY for practice sessions.
"The best practice session is one that ends with the child feeling competent and safe. A shortened successful session is worth more than a full session that creates aversion."
Step 1 of 6
The Practice Session
Step 1: The Invitation
The Opening Script
"Hey [child's name], we're going to play our safety game today! Remember? It's where we practice the special cards/band that help you talk when things get crazy."
Body Language
- Get to child's eye level
- Relaxed posture — this is play, not a drill
- Material visible but not pushed toward child
- Warm, matter-of-fact tone (not dramatic)
Timing: 30–60 seconds to gauge acceptance.
Acceptance Cues to Look For
- Child looks at material ✓
- Child moves toward parent ✓
- Child shows interest (pointing, reaching) ✓
- Child uses AAC/speech to respond positively ✓
Resistance Cues + Modification
- Child turns away → reduce stakes: "Want to just look at the card together?"
- Child covers ears → today is not the right day. Try again tomorrow.
- Child uses "no" → honor it. Emergency preparedness must remain a positive context.
ABA pairing procedures | OT just-right challenge principle
Step 2 of 6
The Practice Session
Step 2: The Engagement
Material Introduction Script
"This is your special helper card. It has your name, my number, and it tells people how to talk with you. Let's practice: if someone came over and you couldn't tell them your name, you'd show them THIS."
How to Present
- Hold material at child's eye level
- Let child touch, hold, examine
- Point to each element: "This is your name. This is Amma's number."
- Use the actual emergency materials — not symbols or photos of them
Timing: 1–3 minutes
Engagement Indicators
- Child examines material ✓
- Child responds to questions about the material ✓
- Child demonstrates understanding (points to name, number) ✓
- Child holds material independently ✓
Reinforcement Cue
When child engages with material → immediate specific praise:
"Yes! That's YOUR name! Now a helper would know exactly who you are!"
PMC11506176 | ABA reinforcement principles
Step 3 of 6
The Practice Session
Step 3: The Therapeutic Action
Choose ONE scenario per session. Role-play it fully with real emergency materials. Duration: 3–5 minutes per scenario. Child success rate: 2 correct responses = session success. Do NOT repeat more than 3 times if child shows fatigue.
Scenario A — "The Lost Scenario"
Materials: ID Card + Wearable Band
Parent plays a "stranger/helper": "Hi, I found this child. What's your name?" Child shows wristband / ID card. Parent reads it and responds: "I can see! Your name is [name] and I'm calling [parent name] right now! You did it!" Reinforce immediately with celebration.
Scenario B — "The Pain Scenario"
Materials: Body Map
Parent plays a nurse: "Where does it hurt?" Child points to body map. Parent: "You showed me exactly where! I know what to tell the doctor!"
Scenario C — "The Fire Drill"
Materials: Wearable Communication Band
Parent simulates alarm (claps hands): "Fire drill! Everyone outside!" Child practices leaving without device, showing communication band when asked "Who are you?"
NCAEP 2020 | ABA behavior rehearsal | Video modeling evidence

Step 4 of 6
The Practice Session
Step 4: Repeat and Vary
Target Repetitions
2–3 successful scenario completions per session. Not more. Quality over quantity.
"3 good practice reps with full engagement > 10 rushed reps with checked-out compliance."
Satiation Indicators — End Session When:
- Child becomes disengaged or irritable
- Responses become perfunctory/automatic without comprehension
- Child actively tries to move on to next activity
Variation Options — Rotate Monthly
Month | Scenario | Material Focus | |
1 | Lost in mall | ID card + wristband | |
2 | Medical emergency | Body map + hospital board | |
3 | Police encounter | Responder card | |
4 | School fire drill | Device-free evacuation + wearable | |
5 | Hospital stay | Hospital communication board | |
6 | Device dead in public | Waterproof cards + go-bag |
Sensory integration dosage research | ABA data collection standards

Step 5 of 6
The Practice Session
Step 5: Reinforce and Celebrate
"You DID IT! You showed the card and the helper knew exactly who you were and how to help you! You are SO prepared!"
Timing: Within 3 seconds of successful emergency communication response.
Social Reinforcement
High five, hug, specific verbal praise about the exact skill demonstrated
Activity Reinforcement
5 minutes of preferred activity immediately after practice completion
Token Reinforcement
Stamp, sticker, or point toward a preferred reward system
Natural Reinforcement
"Because you practiced, you get to choose our next activity!"
What to Celebrate
- Showing the ID card (even without prompting who to show it to) ✓
- Pointing to body map correctly ✓
- Remaining calm during simulated alarm ✓
- Attempting any emergency communication behavior ✓
- Completing the scenario — even imperfectly ✓
"Celebrate the attempt. The brain rewards what it practices celebrating."
ABA reinforcement principles | BACB ethical guidelines

Step 6 of 6
The Practice Session
Step 6: The Cool-Down
Transition Warning
"One more time, then we're all done with our safety game!"
Cool-Down Sequence (2 minutes)
01
End Signal
"All done with safety practice! You were amazing today."
02
Materials Away
Child participates in putting materials in designated spot — builds ownership
03
Calming Input
2 minutes of preferred low-demand activity (reading, sensory bin, music)
04
Transition Cue
"Now we get to do [preferred activity]!"
If Child Resists Ending
- Offer one more short demonstration (not full scenario)
- Use visual timer: "When the timer beeps, we're done"
- Honor completion ritual: child puts the ID card/band "to bed" in its designated spot
What Happens Next
- Materials returned to designated locations (ID card on backpack, go-bag by door)
- Parent logs: what went well, which scenario, date
- Celebrate: this practice session may have just protected your child's life
This practice session may have just protected your child's life. That deserves a moment of recognition.
NCAEP 2020 (visual supports as EBP) | Transition support evidence
60 Seconds of Data Now. Clarity for the Next 6 Months.
Data Point | How to Record | |
Which scenario practiced | Lost / Medical / Police / Fire / Hospital / Device-dead | |
Child success rating | 1 (full prompts) → 5 (independent, correct) | |
Materials used | ID card / Wristband / Body map / Responder card / Hospital board / Go-bag | |
Any modifications needed | One sentence (or "none") |
The Principle
"Data from today's calm practice predicts performance in tomorrow's real emergency. 60 seconds of recording now is a life-safety investment."
Tracking which materials your child tolerates best, which scenarios produce the highest success rates, and where modifications are needed gives you a roadmap for the next 6 months of preparation — and gives your clinical team the data they need to support you precisely.
ABA data collection standards | BACB guidelines | GPT-OS® data dashboard
Most First Sessions Are Messy. That's Information, Not Failure.
Problem 1: Child refused to engage with emergency materials
Why: Materials may feel "scary" or unfamiliar. The emergency context signals threat.
Fix: Introduce materials during play with zero emergency framing first. Let child hold/examine ID card as a "special sticker" before using it in scenario.
Problem 2: Child used materials correctly in practice but panicked in a real drill
Why: Stress response overrides practiced behavior when emotional intensity is much higher than practice.
Fix: Gradually increase practice intensity. Introduce mild simulated stress (quiet alarm sound at low volume) and build tolerance over weeks.
Problem 3: Child keeps removing wearable communication band
Why: May be uncomfortable, a sensory irritant, or child doesn't understand its importance.
Fix: Try different materials (silicone vs. fabric), different placement (dominant vs. non-dominant wrist), shorter wearing periods with positive reinforcement for wearing.
Problem 4: Family couldn't build go-bag — felt overwhelming
Why: Comprehensive preparation feels insurmountable as a whole.
Fix: Start with ONE material. A single laminated ID card attached to the school bag. That's the minimum viable emergency AAC system. Build from there.
Problem 5: School refuses to participate in emergency AAC protocols
Why: Schools may not have existing frameworks for AAC-specific emergency planning.
Fix: Frame as IEP goal: "Emergency communication access" is a legitimate IEP objective. Request meeting with special education coordinator. 📞 9100 181 181
Problem 6: Child became distressed during emergency scenario practice
Why: Some children find emergency topics genuinely distressing — especially those with trauma history.
Fix: Immediately abandon scenario. Return to play. Consult SLP for adapted approach. Rushed preparation creates worse outcomes than careful, supported preparation.
"Session abandonment is not failure — it's data."
No Standard Emergency. No Standard Preparation. Your Child's Profile Determines the System.
EASIER
For younger children / early AAC users / high distress: Focus only on ID card · No role-play — just familiarity · Attach materials and build slowly
STANDARD
Ages 5–12, established AAC users: Full system (all 6 layers) · Monthly scenario rotation · Active practice with familiar adults
ADVANCED
Older children, community-independent: Practice with unfamiliar trusted adults · Independent use without parent prompting · Self-directed emergency communication check
Sensory Profile Variations
Profile | Adaptation | |
Sensory avoider | Thinner/lighter wristband. Avoid heavy lanyard. Increase acclimatization time before wearing. | |
Sensory seeker | Textured wristband. Weighted ID card pouch. Materials chosen for tactile engagement. | |
High anxiety | Practice without emergency framing. Introduce as "special helper tools" not "emergency." | |
Elopement risk | Prioritize wearable ID above all other layers. GPS tracker integration consideration. |
Age Modifications
Ages 2–5
Wearable ID + 1 low-tech card. No scenario practice. Materials familiarity only.
Ages 5–10
Full system. Scenario practice with parent. ID + wearable + go-bag.
Ages 10–18
Include child in system design. Self-advocacy focus. Community-scenario practice.
Progress Tracking
Week 1–2
Weeks 1–2: Foundation. Not Performance. Not Mastery.
What "Progress" Looks Like at This Stage
- Child allows ID card to remain on backpack without removing it ✓
- Child can identify their name on the emergency ID when shown ✓
- Child accepts wearable communication band for 15+ minutes without distress ✓
- Go-bag has been assembled and is positioned at door ✓
- Emergency page has been programmed on AAC device ✓
What Is Not Progress Yet (and that's completely fine)
- Child doesn't yet use emergency materials independently ✗
- Child hasn't practiced any scenario role-play ✗
- Materials aren't yet "tested" in any real-world context ✗
- School hasn't yet been briefed ✗
The Realistic Expectation
"In weeks 1–2, success is that the system EXISTS and the child tolerates its presence. If your child wears the ID band to school without meltdown — that is real, measurable, life-safety progress."
Parent Emotional Note: Building emergency AAC systems brings up fear. It makes the unthinkable feel thinkable. Acknowledge the discomfort — it means you love your child and you're thinking clearly about their safety.
📞 9100 181 181 — For personalized guidance on building your emergency AAC system
PMC11506176 | Intervention timeline literature
Progress Tracking
Weeks 3–4
Weeks 3–4: The System Is Becoming Real.
Consolidation Indicators
- Child retrieves ID card from backpack when asked "where's your helper card?" ✓
- Child can point to their name and a parent's contact on the ID ✓
- First scenario role-play completed (even with significant prompting) ✓
- Go-bag has been checked once for completeness ✓
- At least one family member/school staff briefed on system ✓
When to Increase
If child is tolerating all wearables comfortably and has completed one successful scenario → add second scenario (rotate per the 6-month variation table).
Behavioral Changes That Signal Consolidation
These are neural pathway formation indicators — the preparation is becoming internalized:
- Child spontaneously shows you the wristband
- Child refers to emergency materials by name ("my helper card")
- Child asks questions about emergency scenarios ("what if the alarm goes off?")
Parent Milestone
"You may notice you feel slightly less afraid thinking about emergencies. That's because you've built something real. That's the preparation working."
Neuroplasticity evidence | Clinical milestone literature
Progress Tracking
Weeks 5–8
Weeks 5–8: Your Child Can Be Found, Identified, and Helped — Without You Present.
Mastery Target | Observable Indicator | |
Identity communication | Child independently shows ID card when asked "who are you?" by unfamiliar adult in role-play | |
Pain communication | Child points to correct body map location independently when parent says "show me where it hurts" | |
Emergency vocabulary | Child navigates to emergency page on AAC device without prompting when "emergency" scenario is introduced | |
System maintenance | All materials are in designated locations (child can confirm) | |
Practice fluency | Child completes monthly scenario rotation with ≤1 prompt per scenario |
Generalization Indicators (skill appearing in real contexts)
- Child volunteers ID card when meeting unfamiliar healthcare provider
- Child points to body map when genuinely unwell without parent prompting
- Child asks for wristband before going to community events
🏆 EMERGENCY COMMUNICATION READY — Level 1
Pinnacle GPT-OS® Safety Communication Readiness Index
PMC10955541 | BACB mastery criteria standards

You Just Protected Your Child's Voice. That Is Not a Small Thing.
You did this. While other families hoped for the best, you built a system. Your child now has a layer of protection that most AAC-using children in the world don't have. The 23 minutes that haunts the parent in this page's opening story — you have made that scenario survivable.
An identity that survives device failure ✓
Pain communication that works in a hospital ✓
Emergency vocabulary a stranger can understand ✓
A family that practiced before the emergency arrived ✓
Family Milestone Ritual: Take a photo of your child wearing the communication wristband + ID card. This is not a medical photo. This is a milestone. This is the day your child's emergency communication system went live.
Journal Prompt:"Today we built [child's name]'s emergency voice. The system is: ___. The scenario we practiced was: ___. What I felt building this: ___."
Parental self-efficacy research | Intervention adherence literature
Even in the Celebration Zone — Know When to Call.
🚩 Red Flag 1: Child consistently removing emergency materials
Why it matters: A system the child removes is not a system. Wearable acceptance requires OT assessment.
Action: Consult occupational therapist for sensory-informed wearable materials design.
🚩 Red Flag 2: Child shows extreme distress at any emergency scenario mention
Why it matters: May indicate trauma response or anxiety disorder requiring clinical support.
Action: Pause all emergency scenario practice. Consult SLP + behavioral clinician.
🚩 Red Flag 3: Child cannot be identified by ANY method after 8+ weeks
Why it matters: Identification layer has not been successfully built. Life-safety gap remains open.
Action: Emergency consultation with Pinnacle SLP. This is a priority clinical goal.
🚩 Red Flag 4: Child has had a real emergency and the system failed
Why it matters: Real-world failure reveals specific system gaps that need immediate remediation.
Action: Document what failed. Call 9100 181 181 for emergency AAC system review.
WHO NCF Progress Report 2018–2023 | Pinnacle clinical escalation protocols
Where This Technique Sits in Your Child's Communication Journey
B-228
AAC in the Community
B-229
AAC for Teenagers and Transitions
B-230 ← YOU ARE HERE
AAC for Emergencies
B-231
AAC Users Report Pain and Illness
B-232
AAC for Social Relationships
Prerequisite Techniques
- B-220: Getting Started with AAC
- B-228: AAC in the Community
Next-Level Options
- Medical complexity → B-231: AAC Users Report Pain and Illness
- Community autonomy goals → B-232: AAC for Social Relationships
- School inclusion focus → Domain B School Communication Techniques
Lateral Alternatives
- Wearable acceptance barrier → OT Sensory Processing + Wearable Tolerance Techniques (Domain A)
- Practice scenarios too distressing → Emotional Regulation techniques (Domain C) before returning to emergency AAC
Long-Term Developmental Goal
Community-independent, crisis-competent communication across all environments — without caregiver mediation.
WHO developmental milestones | Domain B progression architecture
Explore Domain B: Communication — Techniques Adjacent to Emergency AAC
Technique | Code | Difficulty | Shared Materials | |
Getting Started with AAC | B-220 | 🟢 Intro | Communication boards | |
Core Vocabulary in AAC | B-222 | 🟢 Intro | Communication cards | |
AAC in the Community | B-228 | 🟡 Core | Wearable communication | |
AAC Users Report Pain + Illness | B-231 | 🟡 Core | Body map, hospital boards | |
AAC for Social Relationships | B-232 | 🟡 Core | Social communication cards | |
First Words + Core Vocabulary | B-150 | 🟢 Intro | Picture cards |
"You already own materials for these" — if you've built emergency AAC materials for B-230, the body map, communication cards, and wearable materials directly transfer to B-231 (Pain Reporting) and B-228 (Community AAC).
Pinnacle 128 Canon Materials | Domain B classification

Real Preparation. Real Emergencies. Real Outcomes.
Before — Arjun's Family
"We had never thought about what would happen if Arjun lost his device. His communication was device-only. No backup. We assumed the device would always be there."
After
"Seven months after building the emergency system, Arjun had a seizure at a community event. We were separated in the chaos. A stranger found him. He had his emergency wristband, his ID card, and his mini communication board clipped to his belt. By the time I reached him — 11 minutes later — the EMTs already knew his name, his diagnosis, his seizure protocol, and how to communicate with him. His preparation saved those 11 minutes. I think about what those 11 minutes could have been." — Parent, Pinnacle Hyderabad Network
(Illustrative case; outcomes vary by child profile)
Before — Priya's Family
"School fire drills were nightmares. The alarm would go off, Priya would drop everything and run, hands over ears, screaming. She'd end up separated from her class, alone, unable to tell anyone who she was. Every drill was terrifying."
After
"We practiced the fire drill scenario every month for 4 months. She learned: when alarm, walk to door, show wristband. At the next real drill, her teacher saw her wristband from 10 meters away, knew exactly who she was, and was able to guide her to her class group. First time she'd never been lost in a drill. First time I'd never been called to school after a drill." — Parent, Pinnacle Bangalore Network
(Illustrative case; outcomes vary by child profile)
"Emergency AAC preparation is not pessimism. It is the highest expression of clinical responsibility. We plan for the scenarios that break most communication systems, because the children we serve deserve communication that cannot break." — Speech-Language Pathology Lead, Pinnacle Blooms Consortium

70,000 Families. One Network. You Are Not Doing This Alone.
Pinnacle AAC Emergency Preparedness Parent Group (WhatsApp)
Parents who have built emergency AAC systems, sharing templates, real stories, and support. Join Group →
Online Forum: Emergency AAC & Safety Communication
Connect, ask questions, share progress. pinnacleblooms.org/community/aac-emergency →
Peer Mentoring
Connect with a parent who has navigated emergency AAC preparation for a child with a similar profile. Request Peer Mentor →
Local Pinnacle Parent Safety Workshops
Emergency AAC preparation workshops at Pinnacle centers near you. Find workshops →
"Your experience helps others." If you have built an emergency AAC system that worked in a real emergency — your story could protect another family's child. Consider sharing your journey with the Pinnacle community.
📞 9100 181 181 — National Autism Helpline (16+ languages, 24×7)

Home-Based Preparation + Professional Guidance = Maximum Safety.
🗺️ Find Your Nearest Pinnacle Center
70+ centers across India, staffed by SLPs, OTs, BCBAs, and NeuroDev specialists trained in emergency AAC assessment and system design.
📞 Teleconsultation
Book emergency AAC teleconsultation from anywhere in India — and internationally.
📞FREE National Autism Helpline: 9100 181 181 | 24×7 | 16+ languages
Specialist Services for Emergency AAC
Service | How to Access | |
Emergency AAC Assessment | Via SLP at any Pinnacle center | |
School Safety Planning Consultation | Via Special Education team | |
Medical Communication Assessment | Via NeuroDev + SLP collaboration | |
First Responder Training Coordination | Via Pinnacle community team | |
Emergency Practice Therapy Session | Via SLP/ABA team |
"The materials on this page can be built at home. The clinical precision of an SLP-designed emergency AAC system adds a layer that protects against the scenarios you haven't yet imagined."
WHO NCF Progress Report (2023) | PMC9978394

See It Done. Then Do It Yourself.
Reel ID: B-230
Domain B — Communication
~75–85 seconds
📹Reel Title: 9 Materials That Help AAC for Emergencies · Series: Communication Access & AAC Solutions — Episode 230
What You'll See
All 9 emergency AAC materials demonstrated in real contexts, with clinician voiceover explaining why each material works. Price indicators and DIY alternatives flagged on screen.
Why Video Modeling Matters
Video modeling is classified as an evidence-based practice for autism (NCAEP, 2020). Watching the technique reinforces the text through a different learning modality — increasing the likelihood you'll execute correctly.
Multi-Modal Learning
Text (this page) + Video (this reel) + Practice (the 6-step session) = Highest parent skill acquisition rate.
📞 9100 181 181
Preview of 9 materials that help aac for emergencies Therapy Material
Below is a visual preview of 9 materials that help aac for emergencies therapy material. The pages shown help educators, therapists, and caregivers understand the structure and content of the resource before use. Materials should be used under appropriate professional guidance.






Link copied!
The Pinnacle Promise
Pinnacle Blooms Network®
Built by Mothers. Engineered as a System.
🗣️ Pediatric SLP · 🤲 Pediatric OT · 📊 Pediatric ABA/BCBA · 📚 Pediatric SpEd · 🧠 NeuroDev Pediatrics · 🔬 CRO · 👨👩👧 Families
"From fear to mastery. One technique at a time." — The Pinnacle Blooms Consortium
What this page delivered: You arrived with a parent's fear — the 23 minutes of silence that haunts every family. You leave with a system: 9 materials, 6 implementation layers, a practice schedule, a professional support pathway, and a community. Your child's emergency voice now has a backup. And a backup's backup. And a backup for that.
Medical Disclaimer: This content is educational. It does not replace individualized safety planning with a licensed speech-language pathologist and emergency preparedness professionals. Emergency AAC needs vary significantly by individual, environment, communication profile, and risk factors. Individual results may vary.
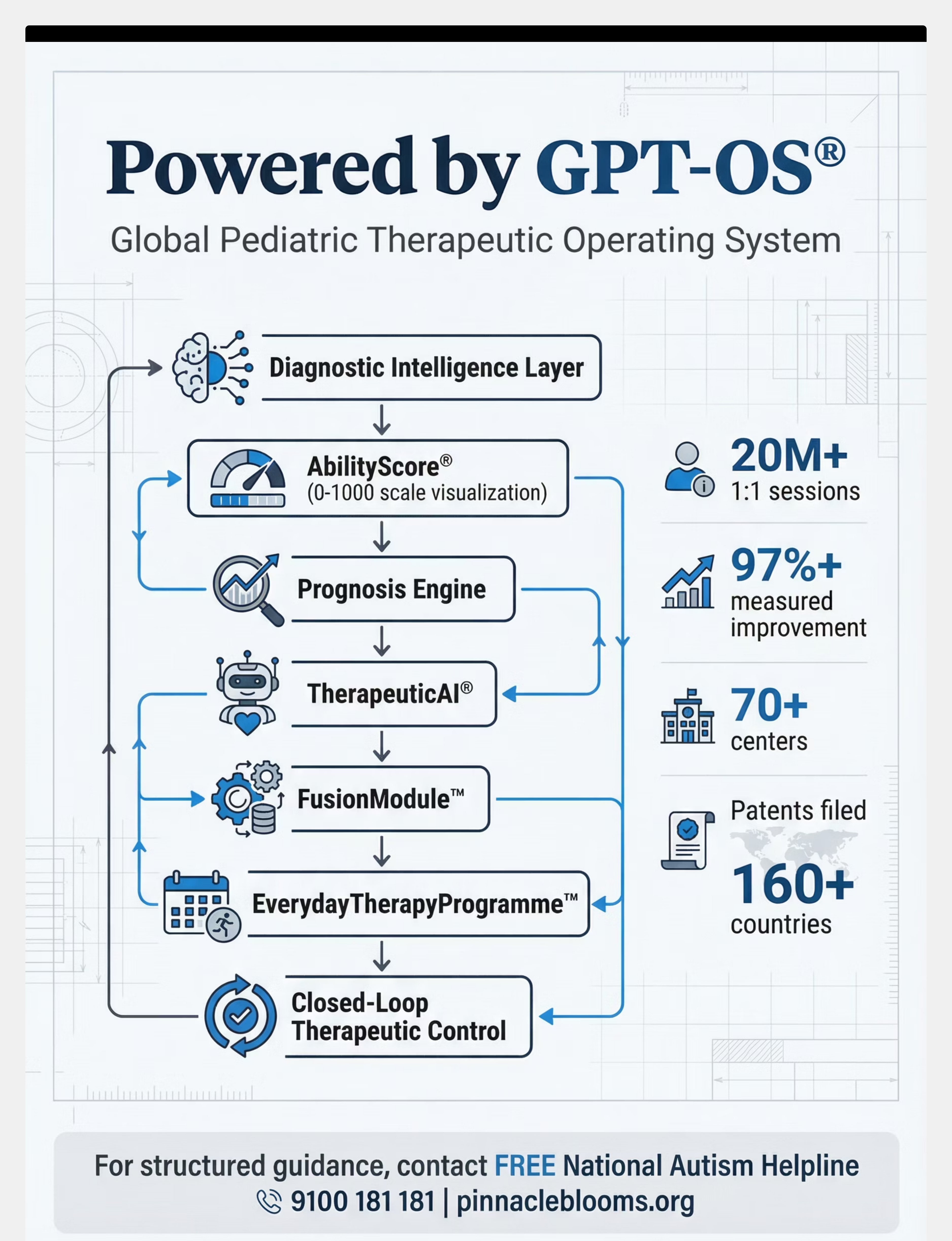
Pinnacle Blooms Network® is a unit of Bharath Healthcare Laboratories Pvt. Ltd. CIN: U74999TG2016PTC113063 | DPIIT: DIPP8651 | MSME: TS20F0009606 | GSTIN: 36AAGCB9722P1Z2 · © 2025 Pinnacle Blooms Network®. All rights reserved. Powered by GPT-OS® — Global Pediatric Therapeutic Operating System · techniques.pinnacleblooms.org | pinnacleblooms.org | care@pinnacleblooms.org · FREE National Autism Helpline: 9100 181 181 | 16+ languages | 24×7